
Abstract
Objective:
Childhood is a period of extensive socioemotional development, which can be impacted by the presence of a congenital craniofacial anomaly (CFA). Complex multidisciplinary treatment and long-term follow-up are normally required, yet understanding of children’s treatment experiences is limited. The objective of this study was to investigate children’s experiences of multidisciplinary team (MDT) consultations from the perspective of their parents.
Design:
Thirty-eight parents of children with a rare CFA were interviewed in person or over the telephone. Interviews were transcribed verbatim, translated into English, and explored using thematic analysis.
Results:
Background factors influencing the child’s experience of the consultation included age, developmental stage, personality, and prior treatment experiences. Participants tried to prepare their child for meeting the MDT, but did not fully understand what to expect themselves. During consultations, participants were acutely focused on their child’s emotional state, making it difficult to balance their desire to protect the child from potentially negative experiences, and the need to engage in a constructive dialogue with health professionals. Participants believed that health professionals’ conduct could considerably influence the child’s well-being and subsequent treatment decisions. Finally, participants highlighted the need to debrief their child to help them adjust positively.
Conclusions:
The ultimate goal of craniofacial care is to help children develop into confident adults who are able to cope with the challenges associated with their condition. Multidisciplinary teams play a vital role in creating a safe and supportive environment in which children feel genuinely informed and involved in key aspects of their care.
Keywords
Introduction
Childhood is a period of emotional and social development with the potential to impact future development and psychological well-being in adulthood. The understanding of risk and protective factors during childhood is therefore of crucial importance in order to maximize future quality of life (Rutter, 2013). Growing up with a congenital craniofacial anomaly (CFA) creates additional challenges for affected children, including living with a different appearance, and the burden of long-term treatment (Nelson and Kirk, 2013; Feragen and Stock, 2017). For the family, the birth of a child with a CFA can be an emotionally demanding experience, and parents will have to cope with their child undergoing multiple treatments (Nelson et al., 2012).
Craniofacial anomalies comprise a wide range of conditions affecting the form and function of the head and face. Prevalence rates and characteristics vary widely (Buchanan et al., 2014), but typically affected areas include the jaws, midface, cheekbones, eyes, ears, and respiratory tract, resulting in difficulties with breathing, chewing, sleeping, eating, vision, and speech. In addition to surgical treatment to address function and appearance, CFAs usually require complex multidisciplinary treatment and long-term follow-up. Care for individuals affected by CFAs and their families is usually provided by a multidisciplinary team (MDT). Although variations in the organization of MDTs are specific to the institution, teams may comprise surgical, orthodontic, genetic, orthoptic, audiologic, speech and language, nursing, and psychological expertise. The overall aim of the MDT is to present a coordinated voice in the patient’s complex treatment plan and to facilitate rapid and efficient patient-centered assessment and treatment (Holmbeck and Aspinall, 2015; Buchanan et al., 2014; Heineman et al., 2017).
Recommendations state that the views and experiences of patients and families should be considered during MDT consultations and when making treatment decisions (World Health Organization, 2008). Although decisions in acute care settings are often urgent, long-term conditions offer a prolonged opportunity to discuss preferences and revisit the risks and benefits of various procedures and management options (Jordan et al., 2018). Patient involvement in MDT consultations have been shown to influence patient satisfaction, health outcomes, and treatment adherence, while also reducing the incidence of unwarranted and expensive elective surgeries (Klifto et al., 2017).
Yet, many challenges exist for craniofacial teams with the desire to implement patient-centered care. During MDT consultations where patients and parents are present, teams are restricted by the need to see several patients in one day. In addition, clinicians from many different disciplines need to assess the child and discuss progress and treatment options (Heineman et al., 2017). Hence, the multidisciplinary setting may be experienced as emotionally demanding by parents and patients (Roberts and Shute, 2011; Pidgeon et al., 2017). Additional constraints, when the patient is a child, may include the child’s age and developmental stage, and the challenge of discussing difficult or complex issues with parents when the child is present (Grootens-Wiegers et al., 2017). Despite the known complexity and variability of CFA treatment, the potential psychological impact of the condition and its ongoing management, and the growing recognition of the importance of the patient perspective in health-care settings, few studies have investigated patients’ treatment–related experiences in the context of rare CFAs (Feragen and Stock, 2017). Fewer still have explored the potential impact of these experiences on children and adolescents. There are reasons to believe that a setting experienced as demanding by parents and adult patients (Roberts and Shute, 2011; Pidgeon et al., 2017) could be perceived as even more intimidating or confusing by the child. The aim of the current study was therefore to investigate how children and adolescents with CFAs may experience the MDT consultations, as presented from the perspectives of their parents.
Methods
Design
A semistructured interview schedule was created by the first 2 authors, in collaboration with the third author, by drawing upon current knowledge from the craniofacial and broader health fields. The interview guide explored parents’ perceptions of the information provided about their child’s condition and its treatment, shared treatment decision-making, and the quality of communication with health professionals. Individual semistructured interviews were conducted in person or over the telephone. Participants were asked open-ended questions and were prompted to provide more details where appropriate.
Multidisciplinary Care
Centralized and multidisciplinary care has been implemented for the treatment and follow-up of all patients born with a CFA in (Norway). The National Unit for Craniofacial Surgery consists of representatives with specialized expertise from different medical specialties, such as plastic and neurosurgeons, geneticists, otolaryngologists, ophthalmologist, radiologists, speech and language therapists, and orthodontists. A total of 15 to 20 health professionals may be present in the consultation room, and approximately 15 patients are seen on one consultation day. All specialists are not involved in the treatment of all patients, but in order to minimize movement in and out of the consultation room, and because the exact need for a specific discipline is not always clear in advance, most health professionals stay in the room during all consultations. Patients receive regular invitations to attend a MDT, the frequency of which depends on the complexity of the condition, and the individual need for follow-up. Topics of discussion may come from the patient and/or the family, and/or stem from the health professionals in charge of treatment. The team usually has 5 to 10 minutes to prepare for the next patient, and health professionals do usually not have any information in advance about which topics the patient and/or family could need to discuss. At the time of the study, each family or patient were given 15 to 20 minutes, more if possible and needed. The patient is brought into the room and sits on a chair facing the specialists. Parents or other accompanying persons are seated next to the child. Young children are often seated on their parents’ lap. One of the specialists, often a plastic surgeon or a neuro surgeon, sits close to the patients and leads the conversation with the patient/family. When needed, other specialists will come to the front and assess the patient. A nurse secretary is making notes of all decisions during the meeting, and treatment recommendations are summarized by the physician in charge of the patients’ treatment and communicated in writing to the families after the meeting, in addition to the patient’s general practitioner and other local or specialized health professionals in charge of the patient.
Procedure
All parents attending a MDT consultation with the craniofacial team during the study period (September 2016-October 2017) were approached to participate in this study. Information about the study was sent to parents by post prior to the MDT consultation. This information contained details about what participation in the study would entail, and key ethical information such as confidentiality and participants’ right to withdraw, in addition to a consent form. Some participants returned the consent form by post, and an appointment for the interview was made over the telephone. Those who did not contact the researchers prior to their MDT consultation were approached in person at the clinic. Among the 81 parents who received information about the study, 6.5% (n = 5) chose not to participate. Fourteen (17%) parents responded positively but were subsequently not reached when contacted for an interview appointment. Another 25% did not respond, which could indicate a lack of available time, a lack of felt relevance, or the absence of up-to-date contact information.
A total of 48 parents consented in participating and were reached for an interview. Interviews were conducted face-to-face (n = 14) or over the telephone (n = 34) by the second author, who is a qualified clinical psychologist, trained in qualitative methods, and not a member of the centralized treatment team. All interviews were audio-recorded with participants’ permission, and lasted on average, approximately 60 minutes.
Participants
The main focus of the interviews was on parents’ experiences of their child’s health care and the issue of how they believed their child experienced the MDT consultations. Among the 48 consenting participants, 10 interviews did not yield information about the child’s perspective for various reasons. In some cases, the parents had been through particularly demanding treatment experiences that impacted their own emotional well-being, and the interviewer therefore chose to focus solely on the parents’ experiences (n = 7), in order to minimize the potential emotional burden of the interview, and in order to let the parents talk about what seemed most difficult and important to them. In other cases, parents perceived their child to be too young to engage meaningfully in the MDT consultation (n = 3). Data from the remaining 38 interviews are included in the present article (mothers = 31; fathers = 7). Children’s ages ranged from 4 to 25 years (mean age = 10.4 years; males = 24; females = 14). Only one of the children was older than 18 years. This participant had a severe developmental disorder and consequently remained in the full custody of his/her parents. Therefore, these parents were included in the sample. Children’s conditions included single craniosynostosis (n = 4), and syndromes such as Treacher Collins, Crouzon, Goldenhar, Muenke, and Apert (n = 21), in addition to some other very rare genetic conditions that will not be named in order to protect participants’ anonymity (n = 23). Some children also had an additional diagnosis of autism spectrum disorder or cognitive difficulties. In 3 cases, one of the parents had the same condition as the child. A total of 70% were married or lived in partnership with the child’s mother/father, while 12 (26%) parents were divorced or had left their partner. Marital status was missing for 2 (4%) of the participants. Most families consisted of 2 (38%) or 3 (27%) children, including the child with a CFA.
Analysis
Interviews were transcribed verbatim and translated into English. Thematic analysis was carried out by all 3 authors following the guidance provided by Braun and Clarke (2006): (1) becoming familiar with the data, (2) identifying interesting features of the data, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes, and (6) producing the report. Analysis was seen as a recursive process, and detailed notes were written throughout. Themes were subsequently chosen for their prevalence and/or their apparent importance in relation to the research question. Themes were discussed until full agreement was reached.
Ethical Considerations
The Data Protection Office at (Oslo) University Hospital granted ethical approval for the study (2016/14088). Relevant referrals or a subsequent follow-up could be arranged by the trained clinical psychologist performing the interviews if needed.
Results
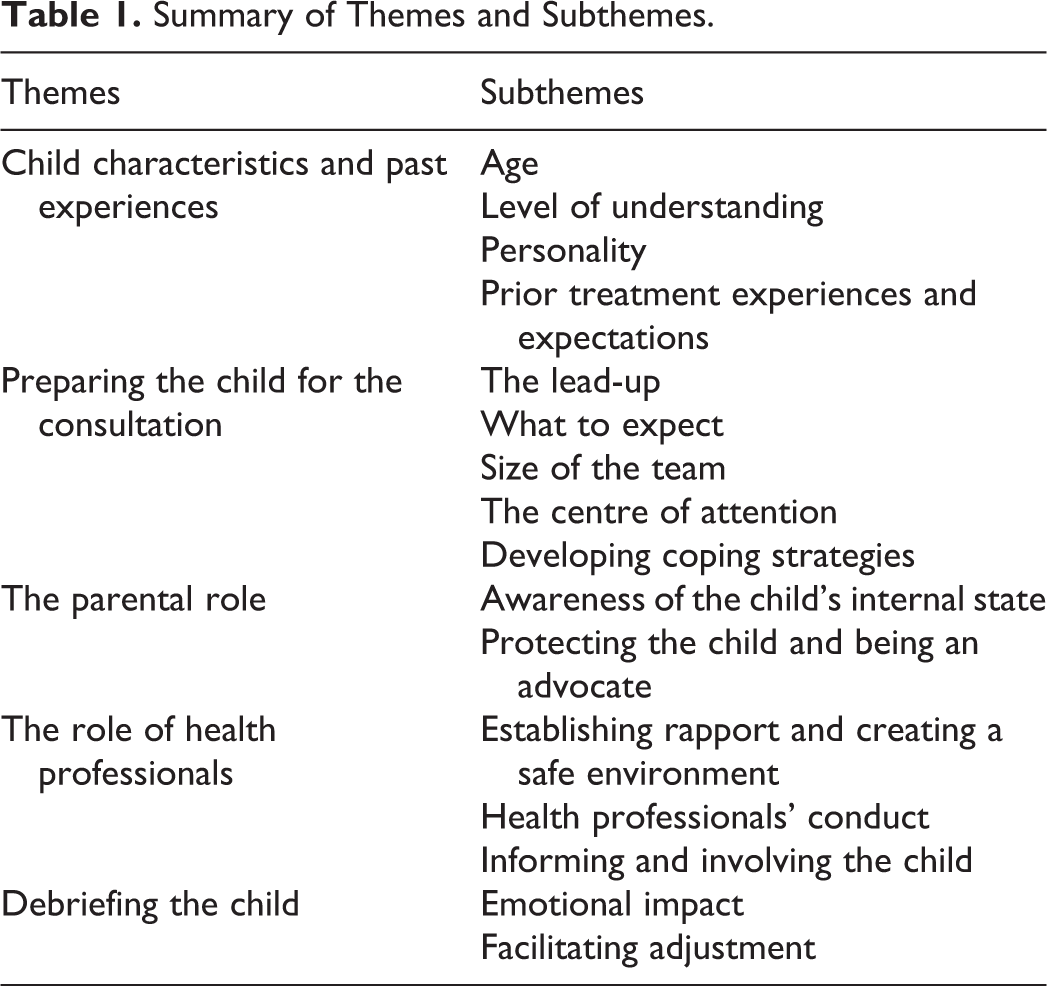
Five core themes with corresponding subthemes were identified (see Table 1 for an overview). Main themes were “Child Characteristics and Past Experiences,” “Preparing the Child for the Consultation,” “The Parental Role,” “The Role of Health Professionals,” and “Debriefing the Child.” Each of the identified themes and subthemes are outlined below and are illustrated using exemplar quotes. All participants have been given pseudonyms to preserve anonymity.
Summary of Themes and Subthemes.
Theme 1: Child Characteristics and Past Experiences
The analysis pointed to child characteristics and generalized past experiences that could be expected to influence the child’s experience of future MDT consultations.
Age
Participants stated that their child’s level of awareness during MDT consultations had increased with age, and some parents mentioned that their child had become more involved in the MDT consultations as they grew older. She was 4 or 5 last time, it didn’t look like she cared about them talking about her (…). Now that she is 6, she is much more aware of what is going on around her, so I am a little bit worried. (Sophie, daughter aged 6) I noticed he was more thoughtful than last time, wondering what this was. When he was younger, he did not understand at all. (Amelia, son aged 4) She is old enough to have her own questions now, and she understands what they talk about. (Rebecca, daughter aged 15) Today was the worst, worse than the previous [MDT consultations]. When he was younger, perhaps they asked him fewer direct questions. (Jack, son aged 15)
Level of understanding
Some participants indicated that their child did not completely understand the purpose of the MDT consultations. In some cases, parents reported their child to have a developmental impairment that limited their child’s awareness of the situation: [She finds it] very strange (…). She understands that it is all about her ear. (Hayley, daughter aged 8) She has a developmental disorder, so I am not sure what she understands. (Charlotte, daughter aged 5) Children understand things. Even when there are lots of things they do not understand, they understand when something is not as it should be. (Samantha, son aged 5)
Personality
Some participants believed their child possessed personality characteristics which could be protective against difficult treatment experiences. She is the kind of child that is OK with most situations (…). I do not believe this is traumatic for her. (Elizabeth, daughter aged 9) He is an intelligent and good boy (…), and very confident, so this is ok for him. (Katy, son aged 10)
Prior treatment experiences and expectations
A few participants believed that their child’s prior experiences of MDT consultations had been positive. He loves it! He receives lots of attention, they ask him questions about his new teeth or about kindergarten, and he loves receiving small treats. (Claire, son aged 6) She finds it really horrible (…). She has not wanted to go back. She dreads it every time (…), and she cries when she knows there is a whole team there. I don’t know if it is about being reminded about her condition. (Hannah, daughter aged 5) I know she dreads meeting the team, because there are so many people there and she (…) doesn’t like being the center of attention. (Thomas, daughter aged 10) He is aware of his speech problems, and is very sad about this. So when he knows people will ask questions, he is really nervous (…). He is so very vulnerable and exposed sitting there. (Natalie, son aged 10) We explain it all to him (…), but he has reached an age where he asks more questions about “Why do I have to be like this?” (…). But he is used to doctors looking at him and into his mouth. He grew up with this, so for him, this is normal. (Jemma, son aged 10)
Theme 2: Preparing the Child for the Consultation
Some participants described engaging in a dialogue with their child prior to their next MDT consultation in order to prepare the child for what they might expect.
The lead-up
Some participants described how they prepared their child for the MDT consultation in advance. As soon as we receive the information with a date, we tell her (…) that she will meet the team again. She asks “how long is it now?” and we say “a month.” Then she asks again “how long is it now?” and we answer “two weeks” or “next week.” I believe this helps her to prepare herself psychologically to sitting there in front of the team. (Thomas, daughter aged 10)
What to expect
Participants felt it was important to prepare their child for what to expect from the MDT consultation. [With increasing age] my daughter is more aware of (…) herself, her body, and her feelings (…), so this time we prepared her for (…) what she was going to do. (Isabelle, daughter aged 6) I wished we had prepared her for (…) them standing there, and measuring her head, and looking at her teeth (…). I hadn’t prepared my daughter, and I wish I had been given the possibility to do that. (Rebecca, daughter aged 15) [My son] sat on my lap and asked “mummy, what are they doing?” and I had to answer, “I don’t know what they are doing.” We have to be able to explain, he can’t just be a figurine (…), but sometimes it is hard to prepare the child, because we don’t know in advance what the team is going to address. (Samantha, son aged 5)
Size of the team
Participants also felt it was essential to prepare their child for the number of people who would be present in the room during the MDT consultations. We received a letter with information about the number of people present during the consultation, so we knew (…). This is madness really, having a meeting like this with a 7-year-old, but it gave us the possibility to talk to her about it in advance (…). So when we came into the room, she knew there would be many people there (…), and that they would perhaps ask her questions. (Mia, daughter aged 7)
The center of attention
Finally, participants discussed the need to prepare their child for being the focus of the team’s attention. We have always been open about it, talking about it with him, so that it becomes something natural (…). He has commented “they just sit there and look at me,” which he thought was weird in the beginning. He dreaded coming the first few times. (Victoria, son aged 8)
Developing coping strategies
Participants described a variety of strategies that their child used to cope with emotional challenges and to be more involved in the consultation. She had counted the number of people in the room (…), and could tell us afterwards that there were 16 people there. So she found something to focus on (…), and I also believe that she felt special with all those people being there for her. (Mia, daughter aged 7) She behaved like a clown when meeting the team (…). Like a protective strategy to ease the pressure off herself. (Thomas, daughter aged 10) We talked about what was going to happen and we wrote a list of questions. I feel she was more present than ever during this consultation. (Hayley, daughter aged 8)
Theme 3: The Parental Role
The third theme describes how participants experience their role as parents during the MDT consultations.
Awareness of the child’s internal state
Participants described being acutely focused on their child’s internal state during MDT consultations, often guessing how their child might be feeling in that situation. It must be difficult to sit there, being stared at, and with gloves in your mouth, but actually (…) I think she feels ok about it. (Thomas, daughter aged 10) I believe the setting is scary for him. But I also believe that he feels cared for. (Ingrid, son aged 11) I wonder whether she has more questions than she asks. (Isabelle, daughter aged 6) If I was to guess, I believe he finds it awful. (Jack, son aged 15) I believe she was surprised about the whole setting. She became very still (…). Her face became very pale (…). [Normally] she talks all the time. (Rebecca, daughter aged 15) I don’t believe he likes being there (…). He is a very joyful and happy boy in all other settings, but when meeting the team, he goes into himself. (Sarah, son aged 15)
Protecting the child and being an advocate
In order to comfort or protect their child during MDT consultations, participants described the need to advocate on their child’s behalf. We have learned (…) how to set boundaries (…). To be clearer about his boundaries, and to tell [the team] about them on his behalf, in order to protect him. (Harry, son aged 6) My son started crying (…) so I asked for a break. (Olivia, son aged 12) It is challenging for us as parents, when you notice that your child feels discomfort but you are also trying to have a constructive dialogue with the professionals. (Harry, son aged 6) I had so many thoughts in my head at the same time. I tried to observe him, but at the same time, I observed myself. “How can I handle this in the best possible way?” (…) It was demanding. (George, son aged 16) I miss the possibility to discuss things without my daughter being present. I have many questions that I do not ask because I am with [my child] (…), such as whether the operations are risky, and what if something happens? (Hannah, daughter aged 5) I wish they would discuss the things she needs to be involved in with her, and then discuss other issues with the parents by telephone. (Thomas, daughter aged 10) [The team] said we should discuss surgical options (…), but my son doesn’t want this surgery and we don’t feel it is necessary (…). They should have discussed this with us first. (Emily, son aged 12)
Theme 4: The Role of Health Professionals
During the consultation, health professionals have the challenge of combining medical expertise while actively involving the patient and the family.
Establishing rapport and creating a safe environment
Participants discussed the need for health professionals to establish rapport with the child, to help the child to feel safe in the hospital environment. They are good at capturing her attention by talking about (…) the last time they saw her, and telling her how much she has grown (…). She likes hearing that. (Thomas, daughter aged 10) We feel they care about the patient and his family (…). The doctors are his buddies. When they meet at the team, they fist-bump (…). It is so important that he sees the same faces. It makes him feel safe (…). I see he feels as he does at home. (Rachel, son aged 14) One of the nurses is good at finding a toy she can play with on my lap. (Sophie, daughter aged 6) They could have a small corner with some child chairs and a table, some drawing material and some toys (…). Or a nurse that could sit with the child. (Harry, son aged 6) She isn’t usually as shy as she was [at the consultation]. If they had given her more time, she would probably have become more communicative. (Charlie, daughter aged 7)
Health professionals’ conduct
Participants reported feeling anxious that comments made in MDT consultations could prompt their child to feel concerned about their appearance. Thoughtless comments such as “your forehead is a little bumpy” (…). If he hasn’t thought about this before, he certainly feels it is a problem now. (Sarah, son aged 15) They held his chin and said “we will have to do something about this”, and this in front of my 12-year-old son. In full puberty, he is told that he needs plastic surgery. (Emily, son aged 12) She does not experience her face as different, so I am a little bit worried about the next consultation (…) because of what might be said. (Sophie, daughter aged 6) They ask him if it is ok to touch his head (…). We have been very clear about this with them, that (…) this is a whole person with boundaries, and they should imagine how they would feel if somebody suddenly touched them, before asking if it is OK to do so. (Harry, son aged 6)
Informing and involving the child
Participants discussed the importance of speaking directly to the child. In a way, they talk about her but not to her. (Rebecca, daughter aged 15) Sometimes [the team] talk over the child’s head (…) and they whisper [to each other], and I believe that can be scary, because children are afraid of what is unknown (…). And if you point at the child as well, it will affect the child. This is about taking the child’s perspective. (Thomas, daughter aged 10) They ask him questions directly, how he feels and what he thinks, and I feel they take their time, so this is exactly what he needs. (Claire, son aged 6) They kind of expect her to want a new ear, but they have not asked her about this. (Hayley, daughter aged 8) They should talk to her before talking to the parents (…). Especially older children and adolescents. If not, you disempower the child. As adults and parents, we are supposed to support the child through a change or treatment, but it is still the child who is the one to go through it. (Thomas, daughter aged 10) It is important to me that they talk to him (…), that he is given an opportunity to have his say, so he doesn’t just feel like a game piece. He told me afterwards that he was happy (…). He felt cared for, and felt he could choose if he wanted the surgery or not. (Laura)
Theme 5: Debriefing the Child
When parents had sensed their child’s distress or discomfort during the MDT consultation, talking the experience through with the child afterward became a priority.
Emotional impact
Participants described the emotional impact that MDT consultations could have on their child. I believe he did not care really, but I don’t think he felt it was OK or uplifting either (…). He was very quiet afterwards. (Emily, son aged 12) The next day, the school called and said that [my daughter] had been emotional (…), and I wonder whether she might have been emotionally weary (…), that the experience was demanding for her. (Isabelle, daughter aged 6)
Facilitating adjustment
As a consequence of the potential impact of the consultation, participants felt it important to debrief their child, in order to help them adjust positively. My son asked me “mummy, is everything wrong with me?” (…) I told him “if you have a very nice car, and you take it for a service (…), the mechanic will not talk about how nice your car is, he will talk about what needs to be repaired. That’s why you are there. This is the same. (Olivia, son aged 12) We need to talk about how it felt after she has seen the team. If anything was upsetting or difficult. And we talk about what will happen in the future. Dentist, operations. She (…) does not like to be surprised. (Thomas, daughter aged 10)
Discussion
The current qualitative study investigated children’s experience of MDT consultations in craniofacial care, as seen through their parents’ eyes. Results confirm that several aspects of a MDT consultation can complicate the matter of attending to the child’s holistic needs. Although parents reported some positive experiences, largely due to the skill of the MDT, almost all felt the MDT consultations were exposing in nature, and expressed concern for the potential vulnerability of their children in the situation. Several parents believed their child had developed a generalized experience of MDT consultations, which were likely based on previous experiences, as well as child characteristics such as age and personality. The remaining themes explored some parents’ attempts to prepare their child for the consultation and/or to debrief their child after the consultation, if needed. The consultation itself proved to be challenging for most children, which had repercussions for the parents. The present study therefore illustrates the demanding balance which health professionals in MDTs face: combining complex treatment–related assessments with positive communication skills, and establishing a strong rapport with both the parents and the child, despite a nonchild-friendly environment. Suggestions for clinical care can be found in Table 2.
Suggestions for Clinical Care.
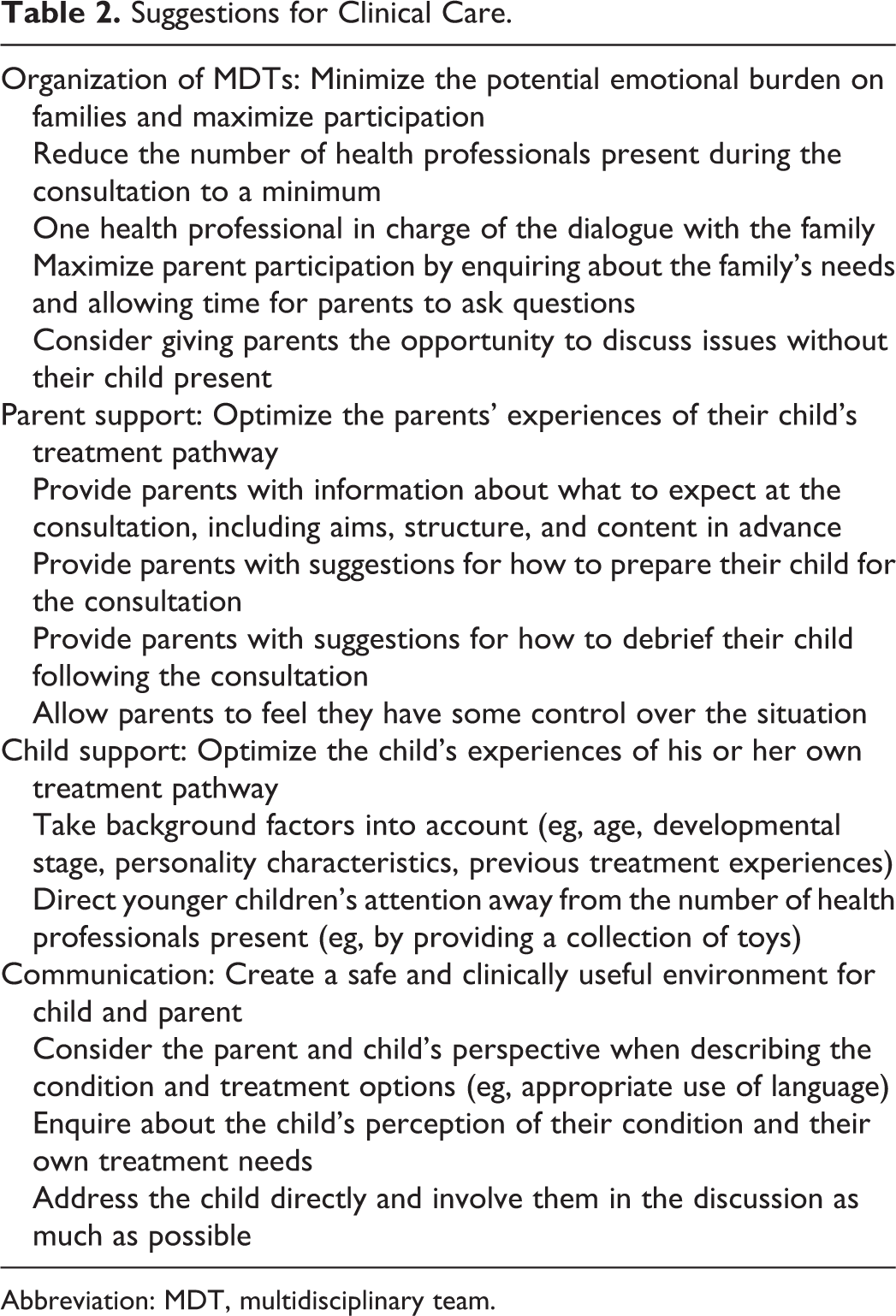
Abbreviation: MDT, multidisciplinary team.
Challenges of MDT Consultations
The aim of a MDT is to facilitate efficient patient-centered assessment and treatment (Heineman et al., 2017). The advantages of multidisciplinary consultations (including the size and broad representation of the team), combined with a short time frame for each patient, create a challenging environment for parents, patients, and health professionals. One recent qualitative investigation reported parents and adults affected by CFAs to be satisfied with the overall level of care they had received (Myhre et al., 2019). Nonetheless, the same participants reported feeling intimidated by the number of health professionals present during MDT consultations, and raised the issues of health professionals’ communication style and challenges related to decision-making (Myhre et al., 2019) . Nonetheless, patients have been shown to appreciate MDTs’ multidisciplinary nature, such as avoiding going from one specialist to another, and knowing that all aspects of treatment could be answered during the same consultation (Heineman et al., 2017). Still, the present study suggests that MDT consultations can be experienced by the child as intimidating, frightening, or confusing. This adds pressure to the parents’ difficult role of mediating between the emotional needs of the child and the need to engage with the health professionals in relation to important medical issues and places responsibility on clinicians to organize MDT consultations in a way that minimizes the potential emotional burden on patients and their families.
The ultimate goal of general, as well as craniofacial health care, is to help children develop into confident adults who are able to cope with the many challenges associated with their condition. The consequences of CFAs and their treatment place the child at risk of psychological distress in a number of areas of life (Feragen and Stock, 2017). A child with a complex and rare CFA will often have to undergo extensive and long-term treatment throughout childhood and into adulthood, and the child’s experiences of the MDT consultations may therefore become a core aspect of the adult patient’s narrative. Clinical experience and recent research demonstrate how treatment experiences can create deep scars (Beaune et al., 2004; Stock et al., 2018), potentially affecting future emotional adjustment, psychological well-being, and identity formation. Optimizing the child’s experience of his or her treatment pathway and experience with MDTs should therefore be a major priority in craniofacial care.
Supporting Parents
Participants in the current study provided examples of how they had tried to prepare their child for meeting the MDT. Preparation strategies reported by parents included a dialogue about what to expect, such as the number of people they would meet. Preparation was considered to be an important factor in minimizing distress and facilitating a positive experience for the child. However, some parents described finding it difficult to prepare their child when their own understanding of the consultation was limited. Parents therefore need to be informed in advance about the specific aims and content of upcoming MDT consultations in order to feel prepared themselves and to prepare their child in turn. Given that centralized follow-up of children born with a CFA is expected to start in infancy with many of the same providers, the continuity of care provides the opportunity to educate and prepare parents for the content and structure of the consultation face-to-face. Equally, parents may find suggestions for how to debrief their child after the consultation helpful, as indicated by the current study. The development and implementation of parental guidelines should therefore be a priority in craniofacial care. A recent study demonstrated how a purpose-built leaflet successfully provided parents with information about the MDT consultation, lowering anxiety during the consultation (Pidgeon et al., 2017). Guidelines could be distributed with the appointment letter, helping parents prepare themselves and the child in advance of the consultation.
The present study also illustrated the difficult role adopted by parents in MDT consultations, whereby parents attempted to protect their child from any negative experiences and advocate for their child when necessary, while also trying to actively participate in a constructive dialogue with health professionals regarding their child’s medical needs. Findings indicate that parents may find this experience emotionally demanding, and that important questions may go unanswered if the parent chooses not to discuss a particular issue while their child is present, for fear of upsetting them. Previous research with parents of children with craniofacial microsomia reported participants’ appreciation for health professionals who were willing to invest additional time to address important issues and to allow for the parent to retain some control over the situation (Johns et al., 2018). Similarly, participants in the current study suggested that the opportunity to speak with health professionals alone, before and/or after the MDT consultation could be beneficial for parents, and ease their anxiety for their child’s emotional well-being.
Supporting the Child
The findings demonstrate the need for health professionals to take various background factors into account when developing a long-term treatment-related relationship with the child. These include the child’s level of understanding (related to age and developmental stage), personality characteristics, and previous treatment experiences. Parents are ideally positioned to provide information about these issues to health professionals, in addition to their child’s current internal state and expectations of the consultation process. An awareness of these factors among health professionals may help to ensure a safe and child-friendly environment, by helping health professionals to better understand the perspective of the child and build rapport. In the case of young children, the presence of a nurse and/or a collection of toys may help the child to feel relaxed while the assessment is taking place. The impact of background factors, including those identified in the current study, as well as additional factors such as the child’s gender, parents’ educational level, and parents’ knowledge of the condition and its treatment, should also be taken into account in future quantitative work.
Health professionals have the challenging role of balancing complex treatment assessments with the provision of succinct and understandable treatment-related information. A crucial factor in creating a positive environment identified in the present study was the language used by health professionals. This suggests that health professionals may need to reconsider the way in which they describe the child’s condition and treatment options during MDT consultations. Using medical or appearance-focused terminology, such as “your forehead is a little bumpy” or “we will have to do something about this,” may increase the risk of the child feeling that there is something “wrong” with them that needs to be “fixed” (Myhre et al., 2019). Using neutral or descriptive language instead, and remembering to ask the patient what their treatment needs are and how they perceive the features of their condition, is therefore preferable. This is especially important when discussing issues related to appearance and/or appearance-altering surgery, as some patients may not yet be aware that their appearance is “different,” or may be particularly sensitive to appearance-related comments. In addition, health professionals should directly address and involve the child in the meeting where possible, to avoid the child feeling insecure or objectified. Small gestures, such as asking the child’s permission to touch their face and explaining why this is necessary may make a significant difference to the child’s and parents’ experience.
Strengths and Limitations of the Current Study
The main strength of the present study was its relatively large sample, recruited from a pool of parents that are expected to be broadly representative of the (Norwegian) population. In-depth qualitative interviews facilitated the collection of parents’ individual and personal perceptions of their child’s experience of MDT consultations. The sample remained dominated by mothers. Nevertheless, another strength was that fathers, who’s views and experiences are largely missing from the craniofacial literature (Nelson et al., 2012), were represented in the study. Finally, the same author performed all of the interviews, reducing the possibility for differences in interviewer technique and characteristics.
The study also had some limitations that need to be taken into account. First, the child’s perception of MDT consultations were based on parent reports, and future studies should therefore include children’s firsthand perspectives. Second, the present study provided important information about the child’s experience of care that could probably be generalized to other countries, teams, and treatment settings; however, cultural and institutional characteristics could be present and should be investigated in future studies. Third, interviews were performed either face-to-face or by telephone. It has been argued that telephone interviews produce findings that are of poorer quality than traditional face-to-face interviews. The psychologist in charge of the interviews did not experience any differences in the quality of the conversation between the 2 methods, and when asked, participants expressed satisfaction irrespective of the chosen approach. A more central factor could therefore be giving the participant a choice, especially when the study is investigating topics that are sensitive (Heath et al., 2018).
Conclusions
Participants in the current study identified several factors that may influence the child’s experience of MDT consultations. Treatment experiences are of central importance to patients’ psychological development, and MDTs therefore play a vital role in creating a safe and supportive environment in which children feel genuinely informed and involved in key aspects of their care.
Footnotes
Authors’ Note
For access to any resources associated with this manuscript, please contact the corresponding author.
Acknowledgments
The authors thank all parents who took part in the study by sharing their stories and experiences.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by the Norwegian ExtraFoundation for Health and Rehabilitation. Grant number: 2018/FO203158.