
Abstract
Objective:
The present study investigated how adults with congenital craniofacial anomalies (CFAs) and parents experience the long-term and complex treatment offered by a multidisciplinary team (MDT).
Design:
Exploratory-descriptive qualitative study based on individual semistructured interviews.
Setting:
Centralized national follow-up and treatment of CFAs by a multidisciplinary craniofacial team from which participants were systematically recruited.
Participants:
The sample included 48 parents of children with CFAs and 16 adults with CFAs (N = 64).
Results:
In general, participants reported to be satisfied with the follow-up and treatment they received from the MDT. Still, some aspects of treatment were experienced as demanding such as the large number of health professionals present during the consultation and being the object of their scrutinizing attention. Health professionals’ communication skills were described as central for participants’ involvement in, and satisfaction with, treatment. Participants also expressed a need for more treatment-related information regarding future treatment.
Conclusions:
Findings could have implications for the organization of care for parents and patients with rare CFAs. The many advantages of MDTs also create unique challenges for patients and parents that need to be addressed. Patients and families should be prepared for the first consultation with the MDT. Health professionals should be aware of their communication style when interacting with patients and be aware of individual differences and needs regarding treatment-related experiences and expectations.
Keywords
Introduction
A Congenital craniofacial anomaly (CFA) is a term used to describe a range of conditions affecting the form and function of the neck and head. Prevalence rates and characteristics vary widely, typically affecting the skull, middle face, jaws, cheekbones, eyes, respiratory or feeding tract, and/or ears (Holmbeck and Aspinall, 2015). Depending on the condition and associated features, early surgical intervention may be necessary, ranging from a single operation early in life to repeated surgical interventions throughout childhood and into adulthood for the more severe CFAs (Feragen and Stock, 2017). Due to the many areas involved and their interconnected functions, multidisciplinary and long-term treatment will be required.
The treatment of CFAs worldwide is often organized through multidisciplinary teams (MDTs). At its foundation, the overall aim of an MDT is to present a unified voice in the patient’s treatment plan by increasing multidisciplinary communication and cooperation and deal with the complexity of treatment processes (Buchanan et al., 2017). The organizations of MDTs are institutional specific, but the goals are the same and as follows: optimal; rapid; and efficient patient-centered evaluation, diagnosis, and treatment (Holmbeck and Aspinall, 2015; Heineman et al., 2017).
A central aspect of patients’ and parents’ treatment-related experiences is the quality of the communication with health professionals. Research on satisfaction with treatment and the relationship between the physician and patients has been extensively studied, both in the general population and within specific medical conditions (Klifto et al., 2017; Jordan et al., 2018; Truglio-Londrigan and Slyer, 2018). This topic has not, however, been investigated in-depth in craniofacial research.
The treatment pathway, defined here as all consultations and interventions a patient will go through, may represent a significant psychological burden for the patient and/or the patient’s family (Nelson et al., 2012; Feragen and Stock, 2017). Nevertheless, existing studies tend to measure satisfaction with treatment results rather than the treatment process itself (Feragen and Stock, 2017), with the exception of a few studies. As an example, Beaune et al. (2004) confirms the assumption that treatment may be a significant burden for affected patients and highlights the need to focus on communication skills and include patients’ views when discussing treatment options (Beaune et al., 2004). Treatment-related discussions with health professionals have also been described as demanding, especially if there was disagreement about recommended treatment or when a consultation involved many health professionals (Roberts and Shute, 2011). Last, adults with CFAs highlight the need of psychological support from health professionals and friends or family during the treatment process (Stavropoulos et al., 2011).
Despite the growing recognition of the importance of the patient perspective in health-care settings, and the known complexity and variability of CFA treatment, few studies have investigated patients’ and parents’ treatment-related experiences and satisfaction with MDTs in the context of CFAs (Nelson et al., 2012; Feragen and Stock, 2017). A qualitative methodology is ideally suited for an investigation of this topic, given the rare nature of CFAs, and the current lack of knowledge (Braun and Clarke, 2006). The aim of the present study was therefore to qualitatively investigate how patients and parents experienced the care and treatment they received from an MDT in charge of treatment and follow-up of CFAs.
Methods
Setting
In Norway, centralized and multidisciplinary care has been implemented for the treatment planning and follow-up of CFAs. The National Unit for Craniofacial Surgery is in charge of the coordination of all follow-up of patients. Patients can therefore easily be reached and invited to participate in research, and studies can be conducted with large and representative samples. The MDT consists of representatives with specialized expertise from different medical specialties, such as neurosurgeons, plastic surgeons, and other surgical specialties, geneticists, otolaryngologists, ophthalmologists, radiologists, speech and language therapists, and orthodontists, among others. Patients receive regular invitations to attend an MDT, the frequency of which depends of the complexity of the condition and the individual need for follow-up. A total of approximately 15 patients are seen by the team on 1 consultation day. At the time of the study, each family was given approximately 20 minutes with the team, and as many as 20 to 25 specialists could be present in the room during the consultation. All specialists who are present are not involved in all patients, but in order to minimize traffic in and out of the consultation room, and because the exact need for a specific discipline is not always clear in advance, most professionals stay in the room. The patient is brought into the room and seated facing the specialist. Parents or other accompanying persons are seated next to the child. One of the specialists, often a plastic surgeon or a neuro surgeon, leads the conversation with the patient/family. When needed, other specialists will come up and assess the patient. Notes of all decisions are made by a nurse during the meeting, and treatment recommendations are summarized by the physician in charge of the patients’ treatment and communicated in writing to the families, in addition to the patient’s general practitioner and other local or specialized health professionals in charge of the patient, after the meeting.
Design
An inductive qualitative approach was chosen to explore how the participants experienced the multidisciplinary consultations, treatment, and follow-up. Thematic analysis is deemed advantageous when existing research on a given phenomenon is limited, and when the aim of a study is to summarize a large body of qualitative data (Braun and Clarke, 2006). A semistructured interview schedule was created by the first and fourth author and discussed between all coauthors. The interview guide explored participants’ perceptions of diagnostic and treatment-related issues, their experiences of shared decision-making, and the quality of communication with health professionals. Participants were asked open-ended questions and were prompted to provide more details where appropriate.
Procedure
Ten participants were recruited during the first phase of the study (September to December 2016). Subsequently, all parents attending the MDT from January to August 2017, and adult patients attending between January 2017 and January 2018, were informed about the study and invited to participate. Some participants were also recruited through the Norwegian Patient Association. Potential participants who did not speak Norwegian, had cognitive disabilities, or a diagnosis other than a congenital CFA were excluded. In total, information about the study was sent to 81 parents and 19 adults (For an overview of the recruitment process, see Table 1).
Overview of Included and Excluded Participants During the Recruitment Process.
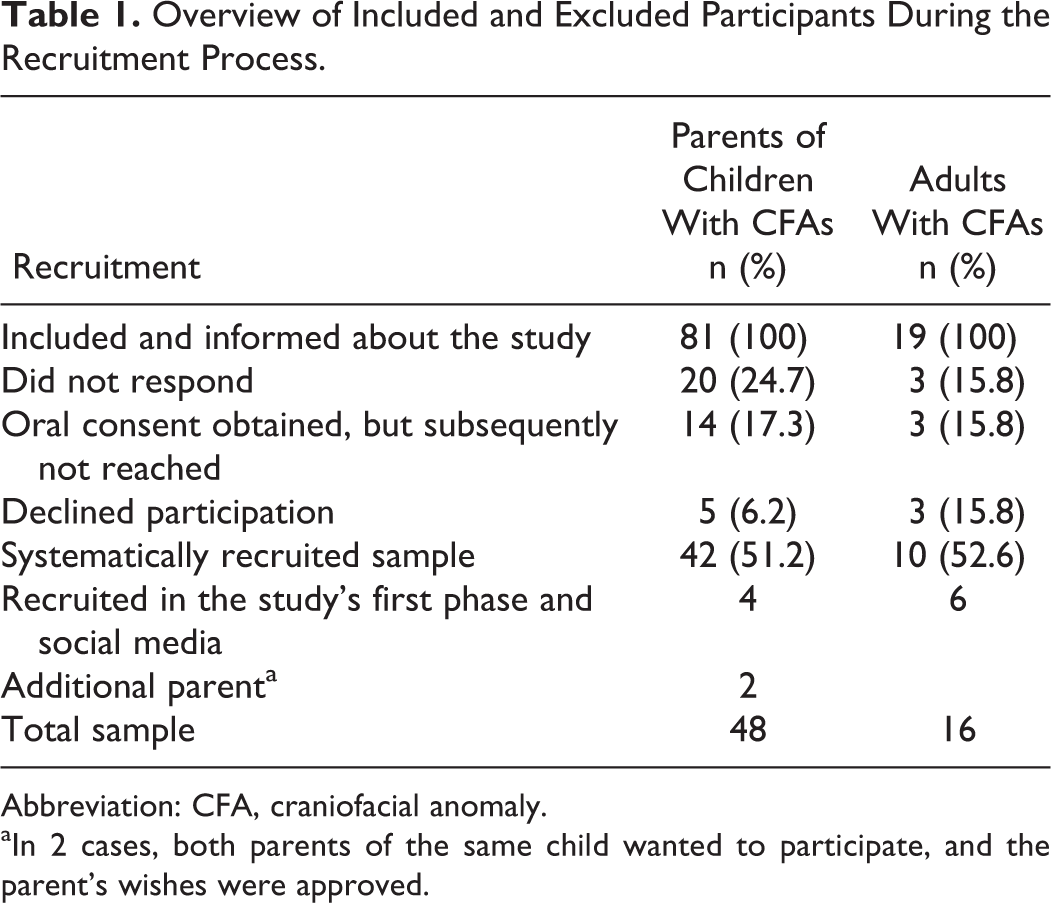
Abbreviation: CFA, craniofacial anomaly.
aIn 2 cases, both parents of the same child wanted to participate, and the parent’s wishes were approved.
A consent form and information about the study, including information about confidentiality and the participants’ right to withdraw, was mailed to patients and parents before the MDT meeting. Appointments for interviews were made by telephone with participants who returned the consent form by post. The remaining participants were approached in person at the clinic. Interviews, lasting approximately 50 minutes, were performed either on the telephone or face-to-face by the first author who is a qualified clinical psychologist and trained in qualitative methods. The interviewer had no prior relationship with the participants and is not part of the MDT.
Participants
As can be seen from Table 1, 64 participants were recruited into the study. The sample consisted of 48 parents (40 mothers, 8 fathers) of 46 children with a CFA (32 males, 16 females), in addition to 16 adults with a CFA (7 males, 9 females). Children’s ages ranged from 6 months to 18 years at the time of the study (Mean [M] = 9.3 years), with one exception, an adult child with a severe developmental disorder, where the parents still had custody for this child. Adult patients’ ages ranged from 18 to 42 years (M = 28.3 years). Individual semistructured interviews were conducted in person (n = 21) or over the telephone (n = 43). Included diagnoses were a few single-suture craniosynostoses, in addition to syndromes such as Treacher Collins, Crouzon, Goldenhar, or Apert, and some very rare genetic conditions (not named in order to protect anonymity). A few children had an additional diagnosis such as autism spectrum disorder, cognitive difficulties, and/or epilepsy. All participants except 8 were of caucasian ethnicity (87.5%).
Data Analysis
Interviews were audio-recorded and transcribed verbatim. Thematic analysis was carried out by 2 of the authors following the guide provided by Braun and Clarke (2006), following 6 main steps: (1) becoming familiar with the data, (2) identifying interesting features of the data by generating initial codes, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes, and last, (6) producing the report. Emerging themes were discussed and checked between 2 authors responsible for analyses, until full agreement was reached, and were subsequently discussed with the other 2 coauthors. As described in Braun and Clarke (2006), themes were chosen for their prevalence and/or their ‘‘keyness’’ in relation to the chosen research questions. The interviews were conducted and transcribed in Norwegian, and quotes chosen to highlight themes were subsequently translated to English. In thematic analysis, it is the content of the interviews that are considered important rather than the number of times each code or theme occurs (Braun and Clarke, 2006). However, all themes and subthemes that were identified are strongly present in the data material.
Ethical Considerations
Relevant referrals or subsequent follow-up were arranged by the clinical psychologist performing the interviews if needed. The Data Protection Office at Oslo University Hospital granted ethical approval for the study (Reference 2016/14088).
Results
An overview of themes and subthemes can be found in Table 2.
Overview of Themes and Subthemes.
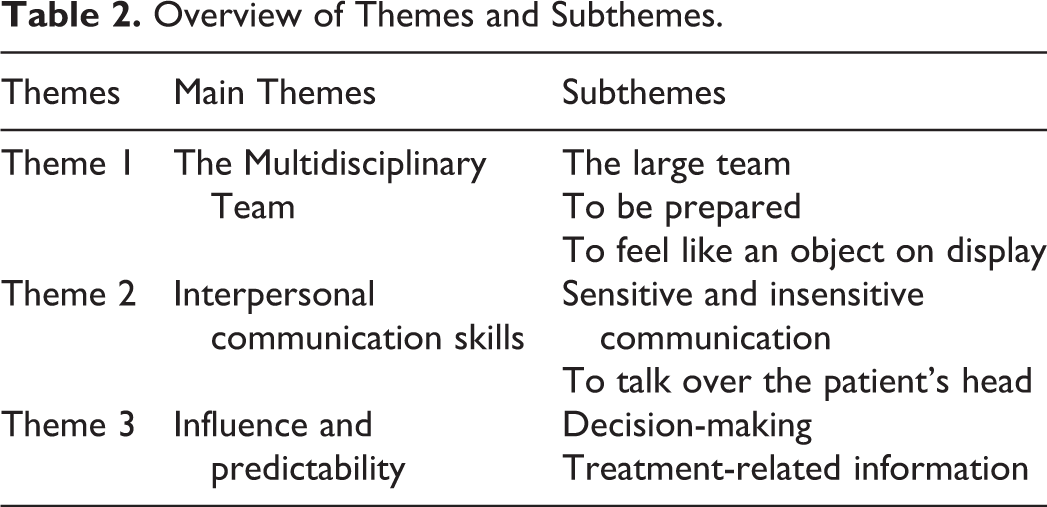
Each of the identified themes and subthemes are described below and are illustrated using the quotes that most clearly represent the themes. Participants have been given randomly selected English pseudonyms.
Theme 1: The MDT
This theme describes a range of experiences and emotional reactions when faced with the MDT. Details are given in the following subthemes.
The Large Team
The first subtheme describes participants’ thoughts, feelings, and experiences concerning the multidisciplinarity and the size of the team, in other words, their (lack of) understanding of the purpose of the number of health-care professionals present in the consultation room.
Emotional reactions ranged from uncomfortable but manageable to strong and overwhelming. For those being overwhelmed, it could be difficult to ask questions or remember and process the information they received during the consultation. I haven’t had any negative reactions to it (the number of people present), but I think that’s because of the setting, that you can ask whatever question you want, and that they explain and elaborate on stuff and so on. (Thomas, father) It’s very demanding to sit there with so many people, even if I’ve been there lots of times (…). It has always been difficult, it has actually been so difficult that I have had problems talking. And that affects my concentration, because I concentrate on not crying, instead of concentrating on what is happening, which means that I don’t communicate very well. This somehow gets worse each time. (Annie, adult) It’s a bit like the feeling you get when you’re at an interview…you don’t exactly feel like you’re on top of the world…but I see the point and I’d like it to be that way, instead of going from office to office, right? (Nicole, adult) I don’t always know who is there, who they are, what they work with, or what the purpose is of them being there. However, (senior consultant) has followed me up almost all the way. And I think that is very important, because it means that someone knows your condition (…), what the problem is and what problems you have had……and this person is also someone you have a sort of personal relationship to. (Alice, adult) I remember when I finished (treatment) and didn’t have to go back again I thought it was really sad! Yeah, because I had seen them so many times, you know, like regularly. Met all of them and discussed back and forth, and suddenly it was finished. And I actually miss it now and again. (Beatrix, adult) I find it reassuring that there are professionals present when decisions are being made. For example, if the oral surgeon says that we need to do this and that, the neurosurgeon can interrupt and say “but we have to remember this and that,” yes, so they don’t start some treatment process without considering that everything is connected. (Linda, mother) Most of all I’m grateful and happy about the team’s existence (…) it is really great to come (…). The level of expertise we as parents feel we need to make us feel secure, that can be found in all members of the craniofacial team. (Lydia, mother)
To Be Prepared
The second subtheme highlights participants’ need to be prepared for the setting and number of specialists present during the consultation, the first time they attended the MDT clinic. Participants described uncomfortable emotional reactions when entering the room or during the consultation as a result of not being prepared. This seemed to be linked to the first consultation only, and knowing what to expect on subsequent meetings with the team helped. It was sort of scary to come into a room with so many people (…). I think they should have told us that there are such a lot of people sitting in that room. (Libby, mother) The first time was a bit odd, because you didn’t know what you were expecting (…) it was a bit shocking (…) but it wasn’t a problem the second time when we knew what to expect. (Henry, father). Fortunately, I was prepared (…) and that was good, really (…) because then we knew (…) and we could talk to her (daughter) in advance. (Agnes, mother) We received written information…but oh, I think it’s hard to prepare yourself for what it means before you actually enter the room. (Sandra, mother)
To Feel Like an Object on Display
The third subtheme describes participants’ feelings of being on display, to feel like an object or a thing, as a consequence of being the center of attention during the MDT meeting. Usually there are two or three surgeons who bend over you and in a way, “open your mouth, look this way.” It’s like you turn into a thing when you come into the room. That the human aspect in a way……in a way you are an object who enters the room, who is going to be fixed. (Alice, adult) We were like research objects in a way, that was what we felt, that we were exposed to this kind of external investigating eye. It made me think of pre-Freud psychology, when they put mad people on show. (Leo, father) The setting is very special, it’s like presenting a project, and have it accepted or rejected. And it’s your son. (Ruth, mother)
Theme 2: Interpersonal Communication Skills
The second theme sheds light on aspects of the specialized health professionals’ interpersonal communication style or skills that the participants described as important to them.
Sensitive and insensitive communication
Participants described several characteristics they felt were important in health professionals, such as being seen as a human being, being cared for, and listened to. The experience of such characteristics seemed to work as a shield against a feeling of objectification and could help them cope with the demanding aspects of the setting. Some of the people (…) looked after me really well. Most of them were good at listening to me, they didn’t just see me as…a project. Most of them really took care of me as a person. (Beatrix, adult) It was a surprise to come into that room and just, hi, oh, that’s a lot of people, but it wasn’t a problem, and that had a lot to do with the doctor who was in charge of the meeting, the way he behaved was great, and that’s very important when you have that kind of team, that there is someone who is good at talking and being human. (Maria, mother) The chief surgeon…he is in control of the show, we call him The King in our family. He is really good, honest, direct, and accommodating, and things happen, it’s not just talk, you see? I feel that he is very compassionate. (Kimberly, mother) I don’t know if they really listened to me, I tried to say that I was having trouble and that I struggled a lot, in some way it was a cry for help, but they were just focused on all the other things, on what they would do. (Oscar, adult) Some mindless comments like “yes, your forehead is a bit bulky,” and if (my son) did not experience this as a problem himself, they kind of told him it was. (Linda, mother)
To “talk over the patient’s head”
Some participants felt that the specialists sometimes talked “over their heads” or used a medical language that they did not understand, while some other participants appreciated that the specialists talked in a way that was understandable. They talked to each other (…) and only occasionally to me, and they talked a little “over my head” with their doctor language. (Betty, adult) When you enter the room…they should try to put away the “expert” and the medical terminology. (Janet, mother) I feel it was nice to talk to the doctors, and the doctor who sat next to me, he was very clear, he talked to me in a way that I understood, so that was great. (Adam, adult)
Theme 3: Influence and Predictability
The third main theme describes treatment-related factors that may strengthen or reduce participants’ sense of predictability and influence during treatment-related decisions.
Decision-making
Participants described that they felt involved in treatment decisions and were asked what they thought or wished for. We do get our say, also when it concerns something being put off or delayed. So that means they often take our advice, they ask us what we want to do in regard to (our daughter). (Aaron, father) They have asked us all along. I feel that on the whole it has been up to us, what is going to happen, when it’s going to happen.…yes, I feel that we have been very involved. (George, father) We were told that we could have a saying regarding the timing of surgery, but that wasn’t really taken into account after all. (Brenda, mother)
Treatment-Related Information
Participants described a need for a predictable treatment process, with information about future treatment plans (what, how, and when). A lack of a clear plan created feelings of insecurity and uncertainty. I need to know a bit more about the way forward. They can’t give me a guarantee for what it’s going to be like, but I should be able to envision some kind of plan for my future (…). I am the sort of person who needs to know details about things, you know? As a parent (…), you think about your child’s future. (Lisa, mother) My experience is that there has been a lot of back and forth. For example, once, they said “yes, we can do that” and then the next time I met them they said “no, we can’t do it” (…), hence not very predictable. There’s been a lot of disappointments, when they’ve said that they can (…) and then nothing becomes of it, and you feel really upset about it. (Annie, adult) We feel included in drawing a plan. And that gives us predictability. It is very, very reassuring that there’s someone who knows when it’s wise to start with the different things. (Sandra, mother)
Discussion
The present study investigated how adults with CFAs and parents of children with CFAs experienced the treatment offered by an MDT. Many participants expressed satisfaction with the quality of follow-up and treatment planning they received. Nevertheless, some aspects of the multidisciplinary care were experienced as demanding, potentially impacting upon satisfaction with treatment and follow-up.
The findings indicated that the organization of the consultation with the MDT was experienced as emotionally challenging, first of all if participants were not prepared for the number of health professionals present and their function. A recent study based on a craniofacial sample (Pidgeon et al., 2017) showed that a leaflet providing specific information about the MDT appointment led to lower levels of anxiety in parents who attended consultations. The development of a leaflet like the one described in Pidgeon et al. (2017) could possibly be a next step in the current treatment setting, hopefully contributing to parents feeling more prepared to their first consultation. Preliminary results from our study subsequently also led the team to include a photograph of the whole team when sending out invitations for the MDT, a change that has not yet been assessed.
Being the center of attention and “on display” was described as challenging, reducing participants’ ability to attend to the information they received and to ask questions. Theories about how stressful situations that result in emotional discomfort and anxiety affects cognitive function could shed light on these findings. Attentional control theory (Eysenck et al., 2007) describes how anxiety, both as a personality dimension and as a temporary condition, affects cognitive resources needed to carry out complex tasks that require attentional focus. The theory postulates that distress and anxiety directs awareness toward stimuli that are perceived as threatening and reduces the ability to focus on other, perhaps more important aspects of the situation. The MDT setting may be categorized as a complex task for patients and their families: facing a number of medical experts while at the same time being expected to participate actively by asking and answering questions about health and symptoms. Participants are also expected to process and remember the information they receive. Our findings suggest that reducing participants’ anxiety may also increase their ability to effectively take part in the consultation and influence their own treatment process.
Irrespective of whether participants experienced MDT consultations as emotionally demanding or not, they appreciated its multidisciplinary nature, rather than going from one specialist to another. They acknowledged that the variety of health professionals present meant that all aspects of treatment could be answered during the same consultation. Separate appointments are known to create additional challenges to an already stressful treatment pathway (Heineman et al., 2017). Additionally, if physicians are seen separately, confusion as to which treatment option to pursue may arise. Patients may also feel like each physician does not really know what the other specialists they saw offered, or how the treatment plans fit together (Heineman et al., 2017). Research on patients with cancer indicates that MDTs are associated with better clinical decision-making, better clinical outcomes, more positive patient experiences, and more work satisfaction for team members (Taylor et al., 2010). The present findings suggest that participants experienced the team as competent and recognized the advantages with the current organization of care, in spite of its emotionally demanding aspects. The findings also showed that confidence in the team and perceived personal direction of treatment depends not only on levels of anxiety and its impact on attention but also of many additional factors, such as health professionals’ use of language and communication skills, and perceived objectification. More research is needed about how consultations could be arranged so that psychological strain is reduced in the patient, while also keeping MDTs’ current advantages.
Health services have placed an increased emphasis on involving patients in health-care decisions, where treatment decisions should combine the physician’s medical expertise and the patient’s personal priorities. Patients also increasingly report wanting to be involved in decision-making (Charles et al., 1999; Bowling and Ebrahim, 2001; Chewning et al., 2012). In the case of rare and complex CFAs, some aspects of treatment may be necessary to restore function, possibly restricting shared decision-making. However, shared decision-making involves listening to patients’ preferences and expectations even though some final decisions will be made by the physicians and identifying areas of decisions that patients may be included in, such as timing of surgery. A wish to delay surgery, as an example, may be important in the patients’ or the family’s adjustment to everyday life, by reducing absence from school or social activities (Roberts and Shute, 2011). Patients’ preferences may therefore be affected by the nature of the decision to be taken, where patients may prefer an active role in minor decisions and a more passive role in more complex decisions (for a review, see Say et al., 2006).
When the ideal of shared decision-making is difficult or restricted, other factors contributing to involvement in the treatment process may become more central, such as information and preparation before surgery, information about the treatment pathway, and health professionals’ communication style. Recent reviews of the literature (Klifto et al., 2017; Riedl and Schüßler, 2017) have demonstrated the centrality of the patient–physician relationship; a better relationship had a positive effect on objective health outcomes, and good communication skills enhanced patients’ treatment-related behavior. Research on other patient groups point to preferences in shared decision-making being influenced by demographics (gender and education), subjective experiences of health, diagnosis and health status, type of decisions needed to be made, and the quality of the interaction patients report having with health professionals (Say et al., 2006). More research is needed to determine whether specific factors may be at work in the care of rare CFAs.
The results from the present study confirm the importance of health professionals’ use of a sensitive communication style and understandable medical language. These factors seemed to affect the perception of other treatment-related issues, such as how much and how good information participants felt they had received regarding the treatment pathway, and to which degree they felt involved in the treatment process.
Person-centered care is a health-care approach that seeks to treat the patient as a person and correct typical biomedical approaches that, according to this approach, are too pathology and disease oriented (Entwistle and Watt, 2013). In the current study, some participants described a feeling of being objectified and how being placed at the center of attention and facing the MDT generated feelings of being only a medical case or an interesting diagnosis. Nevertheless, the experience of objectification also seemed to be associated with the health professional’s communication style and social skills, and some participants explicitly mentioned that if the surgeon was attuned and understanding, feelings of objectification were reduced. Patients with rare CFAs often go through complex and long-term treatment, including potentially painful surgical interventions. It is therefore crucial that health professionals involved in their treatment focus on meeting these patients with compassion, respect, and responsiveness to subjective experiences and support autonomy, in line with a person-centered care approach (Beaune et al., 2004; Entwistle and Watt, 2013).
Clinical Implications
Preparation
Families and patients need to be prepared for their first consultation with an MDT. Information should preferably be given in written form. The document should include information about the approximate number of team members and their function, in addition to some information about consultation structure, content, and purpose. Parents should also be advised to prepare the child for the MDT consultation, and/or could be advised to write down questions they may have in advance, and bring them to the consultation.
Language
Health professionals need to increase their awareness about how they communicate with patients, and among themselves when patients are present. Medical terminology may create a distance between patients and physicians and leads to the patient feeling like an interesting case more than an individual. In some cases, the use of medical terminology may be difficult to avoid when health professional discuss aspects of treatment with each other while the patient is present. Health professionals should be transparent about this and explain why a discussion is necessary, and if possible and needed, inform the patient about the discussion.
Sensitivity toward individual differences and subjective experiences
Health-care professionals should be aware of the subjective aspects of individuals’ experiences and expectations, and each person’s unique way of understanding what is happening. Asking about the patient’s understanding and expectations is therefore crucial and could guide the health professionals toward a better understanding of the individual’s needs.
Treatment plan
Health professionals need to acknowledge that some patients need a clear treatment plan in order to cope with future treatment-related challenges. When this is not possible, as may be the case in the treatment of complex CFAs, information and explanations about why this proves difficult is of central importance for the patients’ well-being.
Shared decision-making
Patients need to feel that health professionals listen to their preferences and expectations, also when final decisions will be made by the physicians. Multidisciplinary teams should strive for giving patients the opportunity to influence some decisions, such as timing of surgery, when possible. Explanations and information are of central importance along the way.
The patient–physician relationship
Several participants spontaneously named some of the key physicians in the craniofacial MDT and described the importance of their treatment-related relationships. Many had known the specialists for a long time and had developed a relationship of trust with them, which functioned as a reassurance. Multidisciplinary teams should be aware of the need for some patients and their families, to have a main physician who they may rely upon and confide in.
Strengths and Limitations
To our best knowledge, this is one of the first qualitative studies to explicitly and exclusively focus on patients’ and parents’ perceptions of treatment experiences with a craniofacial MDT. Another strength is its large sample. Participants were recruited systematically through the team’s patient lists. Due to centralized treatment in Norway, it is reasonable to think that the study sample also is representative of patients with CFAs.
Results are believed to be relevant also to other patient groups with long-term and complex follow-up. More knowledge is needed regarding the impact of previous treatment experiences, expectations for treatment, education level, individual and personality differences, and variations within and across conditions on patients’ and parents’ satisfaction with treatment and MDTs.
Despite the study’s strengths, some limitations have to be acknowledged. First, the range of different CFAs included in the present study may have complicated the interpretation of findings. Conditions ranged from simple craniosynostoses to more complex and rare CFAs and users’ experiences could be expected to vary according to these differences. However, findings did not seem to vary according to specific conditions, underlining the subjective nature of psychological adjustment (Rumsey and Harcourt, 2004). Second, the large sample restricted in-depth explorations of themes and subthemes, and the large variation in treatment-related experiences was difficult to cover in one article. Therefore, only overall and general findings were presented, and future studies will be needed to investigate the details of individual perceptions and treatment needs. Additionally, the study did not include children’s or adolescents’ experiences of multidisciplinary care, which is another important voice that should be addressed in future research. Last, the analyses revealed that the interview guide could have been more explorative regarding shared decision-making and the perception of treatment-related information, in order to provide more detailed information about patients’ and parents’ experiences of this important and central issue.
Conclusion
The present study aimed at better understanding the support needs of parents and patients affected by CFAs and their experiences of the ways in which the follow-up treatment services are organized. Although many participants were satisfied with the quality of the multidisciplinary care they received, several aspects of treatment were also described as emotionally demanding. Participants wished to be better prepared for the multidisciplinary consultation and advised health professionals to avoid extensive use of medical language. Participants also reported the need for more extensive information about future treatment plans when possible. Future research should explore how to optimize health professionals’ communication process with patients and their families, including challenges regarding shared decision-making that may be specific to the follow-up of rare CFAs.
Footnotes
Authors’ Note
For access to any resources associated with this manuscript, please contact the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Norwegian Extra Foundation for Health and Rehabilitation. Grant number: 2018/FO203158.