
Abstract
Background
Assistive technology (AT) is increasingly promoted in UK adult social care policy, research often focuses on devices rather than how disabled people experience and use technology. This study explored how everyday technologies contribute to autonomy and inclusion, moving beyond functional or efficiency-driven perspectives.
Objective
To understand how disabled adults in residential care settings used assistive and mainstream technologies in daily life, and to identify the contextual conditions that support positive outcomes.
Methods
Using a realist-inspired disability studies framework, this study combined iterative literature review with interviews and focus groups involving disabled tech users and assistive technology professionals. Analysis focused on four user-defined outcomes: autonomy, independence, wellbeing, and social inclusion.
Results
AT supported positive outcomes when embedded in relationally supportive environments with consistent staffing, accessible infrastructure, and cultures that validated user-defined goals. Participants reported increased agency, confidence, and participation when technology use was normalized and staff were engaged. These outcomes depended on organizational readiness, not device functionality alone.
Conclusions
Assistive Technology becomes meaningful through everyday use in trusted support systems. To improve outcomes, care providers must invest not only in devices but in relationships, values, and infrastructure that enable everyday autonomy.
Background
Assistive technology (AT) is increasingly promoted in UK adult social care policy as a solution to workforce shortages, budget constraints, and rising care demands. However, while policy discourse tends to emphasize efficiency and digital transformation, 1 the experiences of disabled people using AT—particularly in residential care settings (RCSs)—remain underexamined. Much of the existing literature focuses on technology procurement, device functionality, or cost-effectiveness, rather than how AT is experienced, embedded, or made meaningful in everyday life.2–4
Research on the outcomes of AT use has often reflected medical or functionalist models of disability, wherein technologies are framed as tools to “compensate for” impairments or reduce dependency.5,6 In contrast, the social model of disability foregrounds barriers in the environment, yet has been critiqued for underemphasizing the embodied, affective, and relational experiences of disabled people—particularly those living in congregate care settings.7–9
In response to the limitations of both medical and social models, a growing body of work has explored Critical Realist Disability Studies (CRDS) as a way to understand disability as a dynamic interaction between impairment, social context, power, and material conditions.10,11 CRDS provides a philosophical and methodological framework for interrogating not only what outcomes occur, but how and why they come about in particular settings. This approach has proven particularly relevant in studying AT, where contextual variation and relational dynamics often shape whether technology becomes empowering or marginalizing.12,13
Emerging realist implementation literature has also highlighted that successful AT outcomes depend not only on device availability, but on the domestication of technology—its integration into routines, relationships, and organizational culture.2,14 Factors such as staff engagement, leadership buy-in, and user-defined goals are often as important as hardware or infrastructure. However, these dimensions are rarely included in policy guidance or commissioning processes, 4 and they remain under-represented in empirical studies within adult social care.
Finally, most existing studies underemphasize outcomes related to autonomy, wellbeing, identity, and social participation, which disabled people themselves often identify as central to quality of life.5,9 Emotional satisfaction, peer mentorship, and creative or leisure engagement through technology remain peripheral in many evaluations, despite their reported significance by disabled users.
This study responds to these gaps by applying a realist-informed disability studies framework to investigate how AT use is experienced by disabled adults living in UK residential care settings. Drawing on interview and focus group data alongside iterative literature synthesis and stakeholder input, the research explores the contextual conditions and mechanisms that shape user-defined outcomes. The findings focus on four domains prioritized by stakeholders: autonomy, independence, wellbeing, and social inclusion.
Materials and methods
Research design
This study used a realist-informed research design to explore how disabled adults living in residential care settings (RCSs) experience assistive and mainstream technology in their daily lives. The approach combined elements of realist review and realist evaluation with stakeholder-engaged qualitative inquiry. The aim was to develop explanatory insight into the contextual conditions and mechanisms that support positive outcomes for disabled technology users.
The study was not intended to generate generalizable prevalence data, but rather to build, refine, and test program theories about how assistive technologies work in practice. A realist-informed methodology was selected over a systematic review or purely inductive qualitative design due to the limited and fragmented literature directly addressing AT use by disabled people in RCSs. The flexibility of this approach allowed the researcher to respond to evolving insights, adjust research questions during data collection, and prioritize user-defined outcomes throughout the process. Figure 1 below shows a visual map of this research approach. Map of methods process.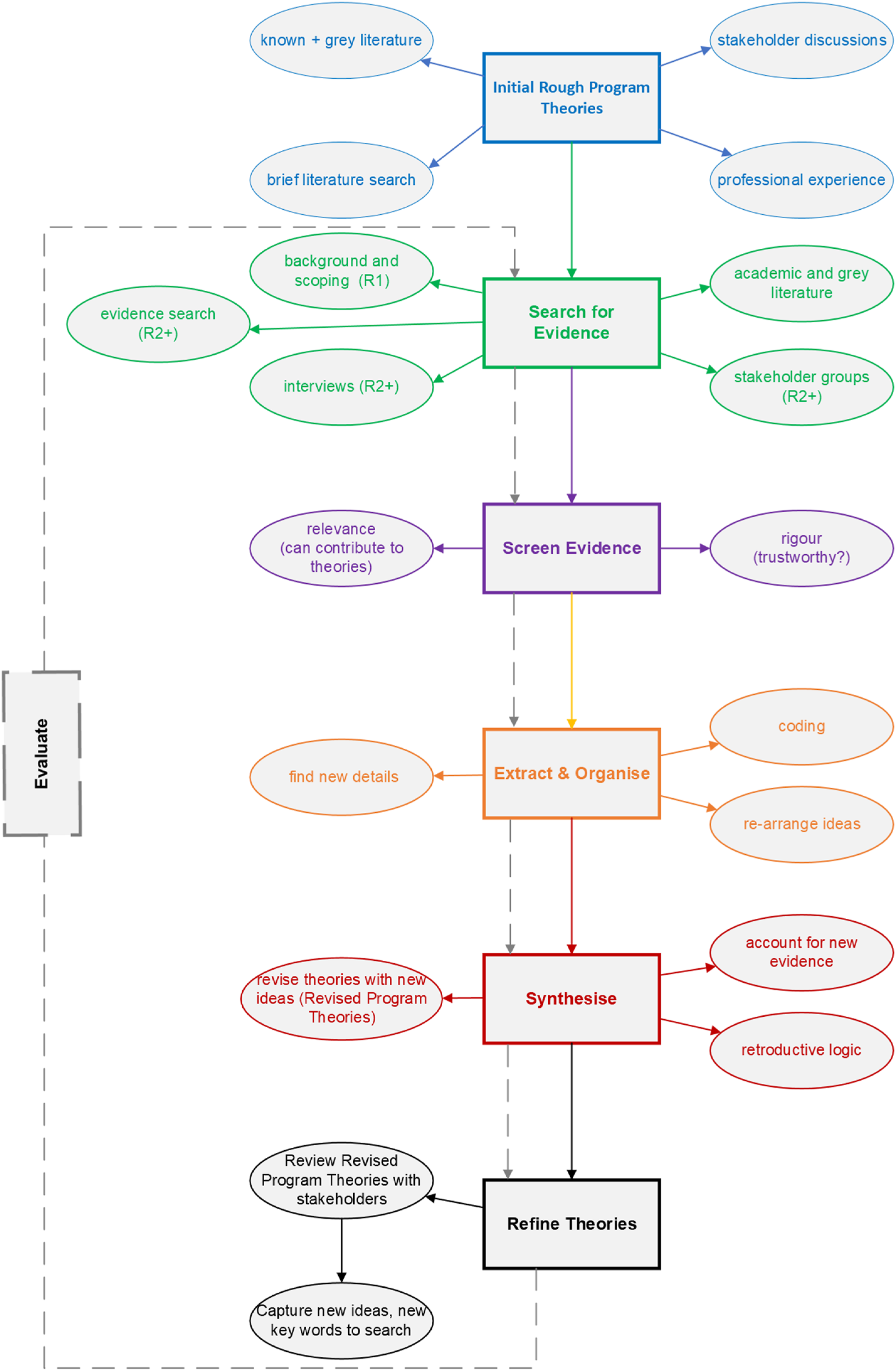
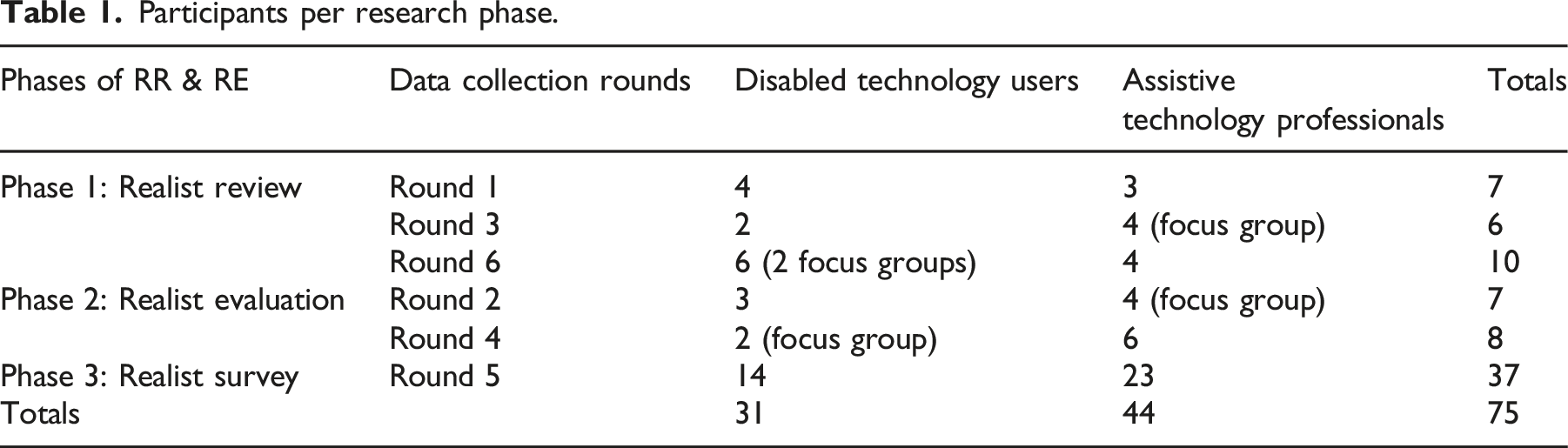
The study design included three core phases: (1) an iterative review of academic and grey literature to generate initial theories; (2) multi-round interviews and focus groups with disabled technology users and assistive technology professionals to refine and test those theories; and (3) a stakeholder survey to prioritize which outcome domains and causal pathways should be emphasized in the reporting of findings. The researcher conducted a total of 22 interviews and 4 focus groups across the combined participant groups to identify key factors contributing to positive technology outcomes.
Participants
Two stakeholder groups were recruited: (1) disabled adults who used assistive technology in residential care settings, and (2) professionals involved in the implementation or support of assistive technology in adult social care. Participants were recruited through a combination of accessible digital outreach, social media (LinkedIn, X/formerly Twitter), professional mailing lists, and snowball sampling. Accessible recruitment materials were offered in multiple formats (infographic, video, audio, and text).
Participants per research phase.
Procedures
The study began with theory-building interviews and a realist-informed literature review. Theories about how AT outcomes emerged were drawn from empirical and theoretical sources and shaped by stakeholder insight. These informed subsequent interview and focus group protocols, which varied across rounds to reflect the evolving focus of inquiry.
All interviews and focus groups were conducted remotely via accessible platforms. Sessions were semi-structured, guided by the theories under development at each phase, in keeping with realist methodological principles. As such, no fixed set of interview questions was used across all sessions. An illustrative sample of prompts is provided in Appendix A. Sessions lasted between 45 and 90 min, were audio-recorded with consent, and transcribed by the researcher. Between data collection rounds, emerging theories were reviewed and refined collaboratively with participants and stakeholders.
In the final research phase, a brief stakeholder survey was used to help prioritize which domains and explanatory theories should be emphasized in reporting. Participants from both stakeholder groups were asked to rate the importance of various enabling conditions for achieving positive outcomes in four domains: autonomy, independence, wellbeing, and social inclusion. The survey did not contribute new qualitative data but served as a tool to inform the focus of explanatory analysis. A summary of survey results is presented in Appendix B.
Data analysis
Data were analyzed using a realist-informed thematic approach guided by retroductive reasoning. Interview and focus group transcripts, along with relevant literature, were reviewed iteratively to identify patterns, mechanisms, and contextual conditions that appeared to influence technology outcomes.
Coding focused on identifying how specific outcomes—defined by participants—were shaped by enabling or constraining factors within the care environment, relationships, or organizational culture. Analytic memos and theory refinement exercises were used to develop explanatory narratives and identify areas requiring further inquiry.
Stakeholder feedback played a key role in refining program theories throughout the research. In the final stage, stakeholder survey results helped prioritize which domains and causal configurations were most relevant for reporting. This survey input did not drive coding but influenced how the findings were organized and emphasized across the four key domains. A full set of illustrative context-mechanism-outcome configurations (CMOCs) is included in Appendix C.
The realist-informed process was complete when key domains were saturated with explanatory data and no new major mechanisms emerged from subsequent interviews or stakeholder engagement.
Results
These findings reflect the integration of interview and focus group data with literature-informed theory and stakeholder prioritization. Thematic domains were developed through an iterative, realist-informed process in which emerging patterns were tested and refined across multiple rounds of data collection. In the final phase of the study, a stakeholder survey was conducted to help prioritize which outcome domains and enabling conditions were most meaningful to participants.
The four domains presented below—agency and autonomy, independence, wellbeing and satisfaction, and social inclusion—were identified in both the qualitative data and stakeholder survey as the most relevant areas where assistive technology (AT) was experienced as impactful. In each subsection, the top five enabling factors identified in the survey are reported alongside the corresponding narrative findings. While findings are not presented in formal CMOC format, causal configurations are discussed in realist-informed terms. A full list of illustrative CMOCs can be found in Appendix C.
Agency and autonomy
Key enabling factors for autonomy.
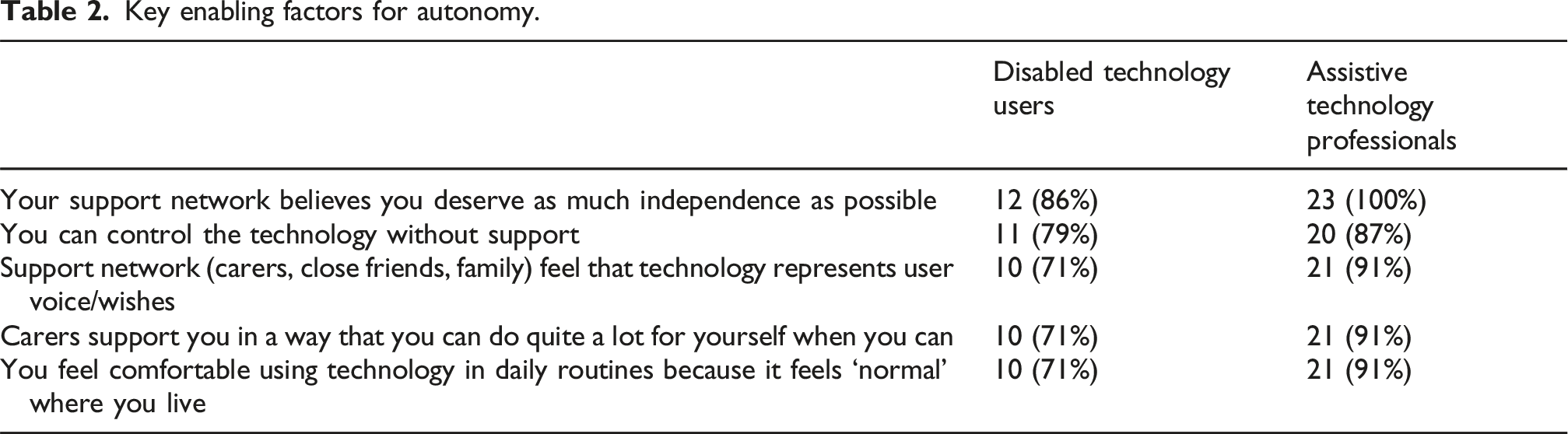
Narrative data supported these survey findings, with participants describing autonomy as emerging when assistive technology was used to express preferences, assert boundaries, or shape daily routines. AT was not inherently empowering; instead, its value was realized through relational processes that legitimated users’ decisions and actions.
Participants gave examples where AAC outputs or smart speaker commands were treated as valid expressions of will. In one case, a request to live with a partner was initially ignored but later respected once the care team recognized the person’s AAC use as their authentic voice. “I think they were probably more worried that there might be an unwanted knock-on effect of letting these two people live in adjacent rooms with an adjoining door than perhaps was really there, and I think [the right communication technology] just gave the center managers the confidence to say ‘okay, fine, we know that this is what these two people want and we also know that they understand that decision.”—AT Professional
In settings where staff held strong values of self-determination, users were encouraged to select their own tools, configure settings to enable independent use, and use technology to make real choices. One AT professional described coaching support staff to “listen with intention” to AAC devices and respond accordingly, even if it meant slowing down routines. “You bring [staff] in and you say ‘look, come and talk to X. Have a conversation and then think about how that conversation would have gone if the tech wasn’t there’.”—AT Professional
In contrast, autonomy was constrained in environments where staff second-guessed AT outputs or viewed them as unreliable. Risk aversion sometimes led to decisions being made on the user’s behalf, even when the person had demonstrated capacity using technology.
Several users described how autonomy improved when AT use was socially normalized within the care setting. Routine presence of smart speakers, tablets, or AAC devices reduced stigma and encouraged users to integrate technology into social or support interactions more confidently. These findings illustrate that autonomy was produced not just through device use, but through systems of relational trust, normalized use, and institutional belief in the person’s right to choose.
Independence
Key enabling factors for independence.
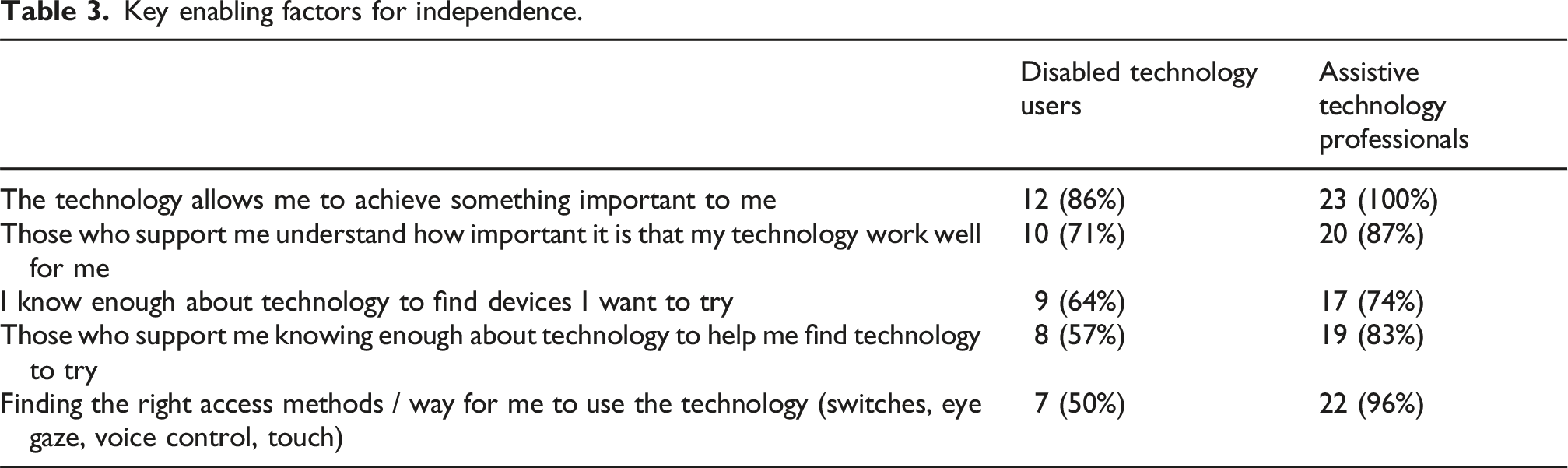
Narratives reflected a view of independence as contextual and relational, not absolute. Participants described independence as the ability to act on one’s own terms using the tools and supports best suited to the situation. In many cases, small moments of success—such as using a voice-controlled assistant to adjust lights or music—were foundational to broader autonomy.
These moments often began with scaffolded support and moved toward self-initiated use. One user described how success with smart speakers and an accessible laptop opened up interest in exploring additional technologies. “[now I’ve got this tech], I’m always interested in what the next invention is going to be…what’s coming next?... I’m actually doing something all day!”—Disabled Tech User “I can monitor my own health and understand my health better… my smartwatch tells me my heart rate, when I’m stressed, when I need to drink water…it counts all your steps and calories.”—Disabled Tech User
The importance of personalized access methods was emphasized throughout. Participants using switches, eye gaze, or customized touch setups described more successful outcomes than those using default interfaces. These access strategies were critical in translating intent into action—particularly for users with limited motor control.
Organizational factors also mattered. In environments where tech support was integrated into daily routines, users had more opportunity to experiment, troubleshoot, and explore. In contrast, when tech support was viewed as extra or burdensome, users experienced stalled progress—even when the tools had potential or gave them additional metrics about their health.
These findings underscore that independence was made possible by aligned systems of staff competence, access strategies, and personal motivation, with technology acting as a facilitator rather than a driver.
Wellbeing and satisfaction
Key enabling factors for wellbeing and satisfaction.
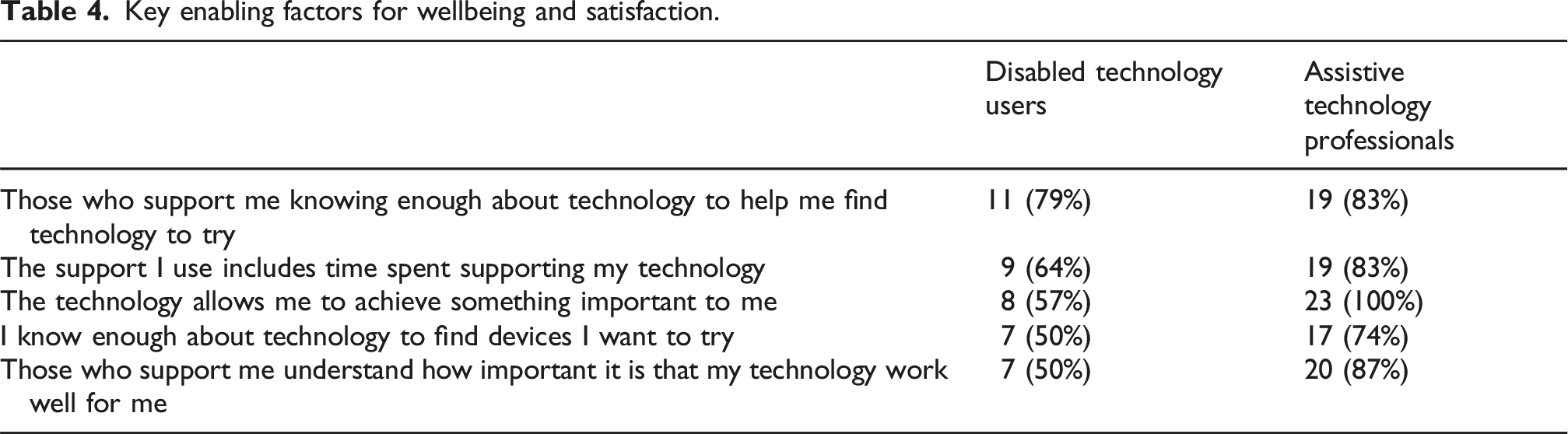
Participants described AT as enhancing wellbeing when it was used for enjoyment, creativity, or meaningful connection. This included listening to music, watching shows, drawing, gaming, or staying in touch with loved ones. These uses were sometimes overlooked in formal support planning, but were central to how participants experienced fulfillment.
Some users described pride in becoming “tech mentors” to others—whether supporting peers or helping staff navigate tools. This shift in identity was empowering and contributed to personal satisfaction. “I’ve got one [an Alexa]! I’m on top of the world! … they call me Mr. Tech Guy here! … I like helping people, yeah. I don’t mind helping them [other residents] solve a problem they are having with their computer or something.”—Disabled Tech User
Staff attitudes were a major influence. In settings where leisure and exploration were treated as legitimate goals, users had more opportunity to try new apps or tools. Where this was deprioritized, satisfaction diminished—even when access to technology remained available. “I think it’s also that they have the motivation themselves…sometimes that motivation needs to be supported and nurtured… it’s as important as teaching how to actually use the technology.”—AT Professional
Wellbeing was also shaped by reliability and consistency. Participants described frustration when devices didn’t work or were inconsistently supported. In contrast, proactive maintenance and responsive troubleshooting contributed to stable use and better mood. These findings illustrate that technology supported wellbeing when it was used relationally and responsively, aligned with personal interests, and integrated into daily care in emotionally meaningful ways.
Social inclusion
Key enabling factors for social activities and participation.
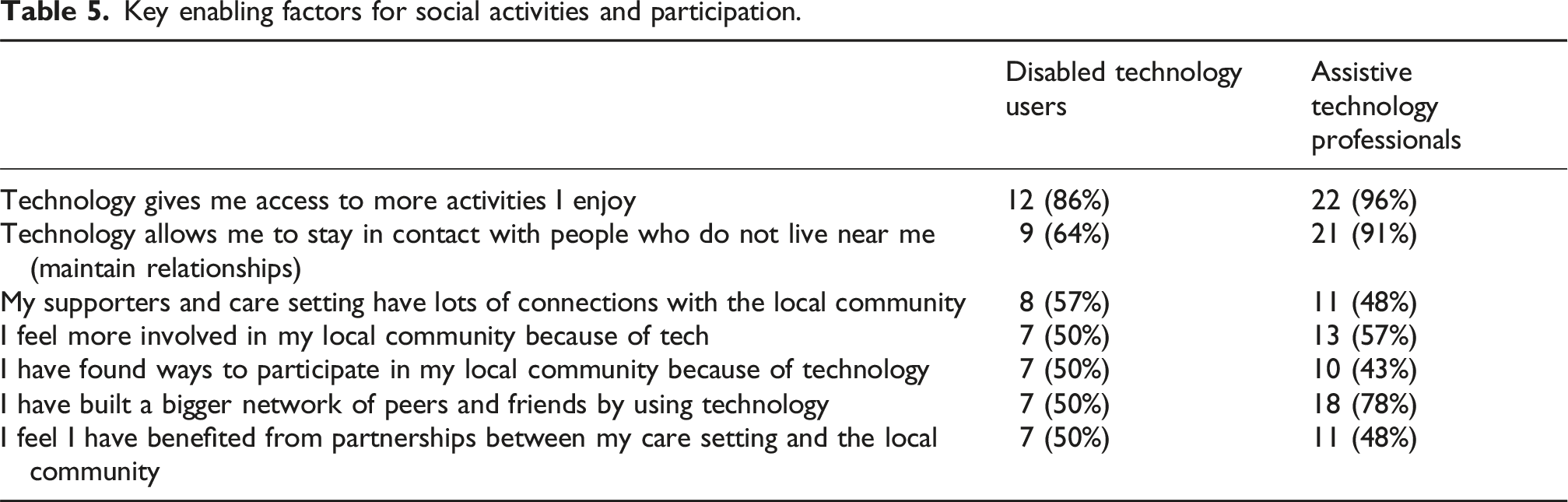
Participants described AT as a lifeline to social connection, particularly during periods of isolation. Tools like video calls, social media, and online games were used to maintain relationships, access communities of interest, and participate in group activities from home. “I’ve got my iPhone…I contact people now with FaceTime. FaceTime is a really brilliant feature. It’s so handy…I really prefer video calling now.”—Disabled Tech User
For some, the asynchronous nature of digital platforms made social participation more accessible than in-person interaction. Those with anxiety, slower processing speeds, or communication challenges appreciated the control and pacing offered by virtual engagement. “We talk on WhatsApp… I use WhatsApp to organize meetings…I sometimes use it to order food… not just to meet my care needs, but also to connect with my carers.”—Disabled Tech User
Peer interaction also played a role. In some care settings, users shared tips, taught each other features, or participated in tech groups organized by staff. These settings fostered shared identity and a sense of belonging. “They can also use their iPad to engage in online games… they recognize people from their online avatars…begin to have brief chats… previously communication was always initiated by others. Now…they can access entertainment and interaction whenever they want.”—Assistive Technology Professional
Staff who maintained connections with local communities were better able to support participation—such as helping users attend virtual religious services or hobby groups. Where this was absent, opportunities were more limited.
Overall, social inclusion was supported when technology use was relational, personalized, and scaffolded by trusted support—creating space not just for contact, but for contribution, identity, and belonging.
Discussion
This study examined how disabled adults in UK residential care settings experience assistive and mainstream technology in daily life. Drawing on a realist-informed framework, it explored the conditions under which AT supports four user-defined outcomes: autonomy, independence, wellbeing, and social inclusion. These domains were prioritized by stakeholder participants as central to positive technology experiences and were shown to emerge through a complex interplay of individual, relational, and organizational factors.
The findings confirm and extend existing literature on assistive technology in adult social care, while also introducing new insights that challenge policy assumptions and address critical gaps in implementation and outcomes research. This section interprets the results in relation to prior work and discusses their implications for care practice, technology deployment, and disability theory.
Reframing autonomy: From tool use to relational recognition
The findings underscore that autonomy is not simply an individual trait or a function of device control, but an outcome shaped by relational trust, organizational culture, and values-based support. This aligns with Lid’s 13 and Watson’s 10 arguments that autonomy must be understood relationally, not just procedurally. The present study expands on this by showing how recognition of AT output as valid communication becomes a pivotal mechanism for user agency—especially for AAC users and those with complex communication needs.
This challenges traditional models that locate autonomy within the individual or the device. Instead, it supports CRDS claims12,15 that autonomy is achieved through enabling environments—where staff beliefs, routines, and communication norms shape the legitimacy of user choices. It also builds on earlier realist work 2 by emphasizing that “domestication” of technology—making it a normal part of daily life—is essential to supporting user-led autonomy.
Rethinking independence as relational capacity
Independence, as reported by participants, was not defined by the absence of support but by the ability to control when and how support was needed. This nuance supports critiques of both medical and social models for offering overly simplistic views of support and dependence.7,8 Instead, it aligns with realist theories of context-mechanism interaction: independence emerges when users have access to appropriate tools, trusted relationships, and environments that encourage skill-building and experimentation.
The study reinforces earlier findings that staff capability and confidence are crucial to enabling technology-based independence.3,14 It also offers new insights into how staff framing of AT use as routine, not exceptional, creates space for users to develop confidence over time. These findings extend the concept of organizational readiness beyond infrastructure to include attitudes, habits, and value alignment.
Wellbeing and identity: Overlooked outcomes of technology use
Wellbeing and satisfaction—often marginalized in formal AT evaluations—emerged in this study as highly significant to users. Participants described how AT supported emotional expression, personal identity, and purpose—outcomes largely absent from existing implementation literature. This resonates with critiques by Berghs et al. 9 and Schalock et al., 5 who argue that quality of life must include affective and identity-based domains.
The study contributes to CRDS by illustrating how technology becomes a medium for reclaiming valued identities, particularly when users are recognized as competent or even expert in their use of tech. These identity shifts were reinforced by peer mentoring, creative exploration, and user-led innovation—domains rarely emphasized in social care commissioning or policy.
By centering these affective and expressive dimensions, this research challenges the dominant policy logic that positions AT as a tool for efficiency, surveillance, or dependency reduction. It reframes AT instead as a vehicle for participation, pride, and emotional wellbeing—with implications for how funding and training should be structured.
Social inclusion as an emergent, tech-mediated process
The findings on social inclusion show that AT use extends beyond access to communication or community—it enables identity development, relationship continuity, and contribution. While prior work has explored how technology mitigates social isolation (e.g., during COVID-19), this study deepens the discussion by identifying how AT supports belonging and reciprocity.
This aligns with broader realist and disability studies perspectives that emphasize the social situatedness of technology.2,12 It also expands implementation research by showing how staff facilitation, peer networks, and even small acts of digital participation can generate sustained social inclusion.
Of particular note is the value placed on asynchronous and digital-first engagement by participants. These preferences—especially among those with communication or sensory differences—suggest that inclusive practice must involve not just physical access but digital fluency and emotional readiness.
A user-informed view of assistive technology outcomes
This study builds on critical perspectives that advocate for technology used by, not on, disabled people.10,12 The stakeholder-informed structure of this research—particularly the use of a prioritization survey—allowed for user-defined values to shape the interpretation and reporting of findings.
Rather than evaluating AT through provider-defined metrics such as cost savings or task reduction, this study uses user-identified outcomes to assess what works and why. In doing so, it demonstrates the potential for CRDS-informed inquiry to center lived experience without abandoning causal explanation.
Methodological strengths and limitations
This study demonstrates the utility of realist-informed, stakeholder-driven inquiry in contexts where traditional methods may overlook complexity or user priorities. The iterative design enabled theory refinement, responsiveness to participant feedback, and integration of explanatory frameworks.
However, limitations must be acknowledged. Recruitment challenges led to underrepresentation of people with higher support needs or limited digital access. While the survey phase helped validate findings, it may have overrepresented digitally fluent or already-engaged participants. The lack of direct involvement from local authorities is another gap, particularly in understanding system-level implementation barriers.
Finally, while CMOC-style logic was used to guide theory building, findings are not reported in full CMOC format due to the desire for accessible, thematic communication. A full list of illustrative CMOCs is provided in Appendix C.
Implications for policy, practice, and research
Findings suggest that to enable meaningful AT outcomes, care providers and policymakers must move beyond a focus on devices and infrastructure. Instead, investment must be made in: • Staff training and organizational culture that supports autonomy, experimentation, and user-led learning • Flexible care routines that include time and permission for technology use beyond task completion • Recognition of wellbeing and social inclusion as valid and valuable outcomes of AT
Future research should examine how institutional incentives, commissioning frameworks, and digital exclusion shape technology uptake across the sector. There is also scope to explore more peer-led or co-designed AT training models, given the emerging role of disabled users as informal tech leaders.
Conclusion
This study explored how assistive and mainstream technologies support autonomy, independence, wellbeing, and social inclusion for disabled adults living in residential care settings. Using a realist-informed disability studies approach, it highlighted the mechanisms and contextual conditions that enable technology to become meaningful in everyday life.
The findings demonstrate that positive outcomes arise not simply from the presence of assistive technology, but from how it is used, supported, and valued within relational, organizational, and cultural contexts. Autonomy emerged when technologies were trusted as extensions of user voice; independence developed when systems allowed for exploration and self-directed learning; wellbeing was fostered through emotional connection and identity-building; and social inclusion was made possible through intentional support for digital and community participation.
These insights challenge conventional policy and commissioning approaches that prioritize efficiency or device distribution over user-defined outcomes. They also expand the evidence base by centering the lived experiences and priorities of disabled people and assistive technology professionals. By framing AT as part of a broader support ecosystem, this research offers a more nuanced understanding of how everyday technology use contributes to everyday autonomy. Future work should continue to prioritize user-led outcomes and examine how systems can evolve to consistently enable these empowering experiences.
Supplemental Material
Supplemental Material - Everyday tech, everyday autonomy: Understanding how assistive technology works in UK care settings
Supplemental Material for Everyday tech, everyday autonomy: Understanding how assistive technology works in UK care settings by Julie Eshleman in Technology and Disability
Footnotes
Acknowledgments
The author wishes to thank all participants for sharing their experiences and contributing their time to this work. The author is also grateful for the professional feedback and supervision of Dr. Liz Forbat, Dr. Kirstein Rummery, and Dr. Steve Rolfe and their support in completion of the research to fulfill requirements for the degree of Doctor of Philosophy. Finally, thanks to the support from the Assistive Technology team at Leonard Cheshire, including Steve Tyler, Dave Hursthouse, Kay Barnes, Will Baker, Toby Wallace, and Nathan Southward.
Ethical considerations
The project was vetted by, and received approval from, the General University Ethics Panel at the University of Stirling.
Consent to participate
Informed consent was obtained from all participants.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and publication of this article: The work was supported by Leonard Cheshire.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.