
Abstract
Background
Extended reality (XR) has previously been used to train control of upper limb prostheses. It is however unclear what characteristics an XR environment should have in order to become a usable and effective training tool.
Objective
The objective was to develop a framework describing the most important factors to be incorporated when designing an XR environment to train prosthesis control.
Methods
A mixed method approach was used. A narrative review was conducted to explore factors that should be considered when designing an XR environment for prosthesis control. Subsequently, a preliminary framework, based on these factors, was rated by prosthesis users and therapists and discussed during focus groups.
Results
Fifty out of 489 articles were included. The preliminary framework comprised 62 factors in four domains: feedback, control, exercise and environment. Five prosthesis users and eight therapists participated in three focus groups. A final framework was developed which contained 46 factors in the four domains. End-users considered all domains to be equally important, since domains and factors influence each other.
Conclusions
The developed framework can be used to guide the design of an XR environment to train prosthesis control.
Keywords
Introduction
Virtual reality (VR) enables a user to step into a virtual world and to interact with virtual objects therein. A virtual world can also be experienced via a computer screen in a non-immersive VR (NI-VR) configuration. The use of a head-mounted display allows immersion of the user in the virtual world by presenting a digital environment. This can be fully immersive VR (I-VR) or combined in the real world environment as in augmented reality (AR). Using controllers or a connection with a motion capture system, the visual image of one’s hands can be added to interact with objects in the environment, resulting in an engaging first-person perspective. Extended reality (XR) is the overarching term for these kinds of digital environments. Due to rapid commercialization, VR has become an affordable method for skill-training purposes, 1 in fields ranging from surgery 2 to stroke rehabilitation. 3 Consequently, a virtual training environment can be developed which promotes motor learning of a difficult skill. Motor learning can be enhanced by, for instance, an enriched environment, adaptation of the level of difficulty based on the current abilities of the user and tailored feedback. 4
Upper limb prostheses that are controlled using electromyography (EMG) are difficult to master and therefore require intensive training. 5 Surface EMG electrodes measure action potentials that are generated when the muscles are activated (myosignals). The extensor and flexor muscles in the forearm are often used as inputs to generate the myoelectric prosthesis’ opening and closing movements, respectively. However, activating these muscles to control a prosthesis hand is a difficult task, especially when more complex control patterns, such as co-contraction, are needed to switch between the modes of the prosthesis. 5 Hence, prosthetic training is needed to enhance dexterous prosthesis use and it can benefit from the engaging VR environment and added visual or haptic feedback. 6 A systematic approach is needed to determine which factors are important to be incorporated to achieve optimal efficacy of an XR environment for training prosthetic control.
Since current attempts to use XR environments for prosthetic training are mostly still in the pilot testing phase, patient involvement is limited in their development.7–13 Garske et al. (2021) argued that often the decisions about a game aspect might not reflect the opinions of the target audience, but rather mostly reflects the opinions of the development team. 14 The design and development of XR environments seems often based on the interests of the researchers, lacking a broader perspective where also user-needs should be included. Reviews showed that around 50% of the studies are performed to investigate specific technical aspects of an XR instead of evaluating the whole XR and user experiences.13,15 Importantly, such design and development is often performed in a non-disabled population.13,15,16 From this knowledge, it can be concluded that the end-users’ opinions on XR training for prosthesis control should be better understood. This could benefit the positive experience of the user and could facilitate a flow state experience during training to enhance the usability and effectiveness of the XR environment.15,17 Through collaboration and user-centred design, meaningful training environments can be developed.18,19 The aim is to provide a framework of the factors that need to be taken into consideration when developing an XR environment to train myoelectric prosthesis control. Additionally, the aim is to validate this framework with the input of end-users, thus including both prosthesis users and therapists. This research will provide insights on the needs of end-users about game design for an engaging training.
To achieve this aim, a narrative review was conducted to determine from the literature what the important design factors are that might be of interest for an XR environment. A narrative review was chosen since this type of review is more qualitative in nature, that is, concerns information regarding the XR environment. No judgement was express in the preliminary framework, no ranking was provided on which factors would be most beneficial. In the second part of this paper, the relevance and importance of those factors is validated with the help of end-users, therapists and prosthesis users, using a questionnaire. Focus groups were organized with the aim to understand the rationale behind the choices made in the questionnaire. A final overview of factors that are most important when creating an XR environment to learn to control upper limb prostheses was created.
Materials and methods – narrative review
Search strategy
A search strategy was developed with the help of a certified librarian (Appendix 1). PubMed and Web of Science were systematically searched by the first author (SGR) using MESH terms and search terms related to prosthesis use and virtual reality environments. The search was conducted in March 2023 and restricted to articles published in 2013 or later, to find the most recent developments of the past 10 years. Previous research shows that many developments in the use of VR for myoelectric prosthesis training took place around 2018, 20 Note also that technological developments go relatively fast in the last decade, making the more recent contributions more relevant, therefore a 10-year window seemed appropriate.
Eligibility criteria
Articles were included if: 1) they discussed the use of virtual or augmented reality for prosthesis training of the upper limb; 2) they were published in English; 3) were published in or after 2013 and 4) full text was available. No restrictions were provided for the type of article. The first author (SGR) performed the article selection procedure and data extraction. An article was included if it mentioned an advice, observation or outcome regarding the use of XR for prosthesis control. From here, common topics were searched within the findings that had overlapping characteristics. Domains were determined by the first author (SGR) based on broad grouping of the findings. The findings were further divided into subdomains, which consisted of a group of findings with similar characteristics within a domain. Within the subdomains, the factors are the smallest units related to the core of the advice. All authors approved this final framework. The Scale for quality Assessment of Narrative Review Articles (SANRA) was used as checklist to report the methods and results. 21
Results – narrative review
The systematic search yielded 489 articles (Figure 1), of which 188 articles were selected during the title selection and 102 during the abstract selection, respectively. The full text of these 102 articles yielded 45 articles for inclusion, in addition to five more articles which were added from the references. An overview of the included articles can be found in Appendix 2. The articles that were excluded focused on unrelated topics about the training of a motion classifier or pattern recognition and did not include enough information regarding the XR or included body-powered prostheses. Flow diagram of the inclusion of articles from two databases.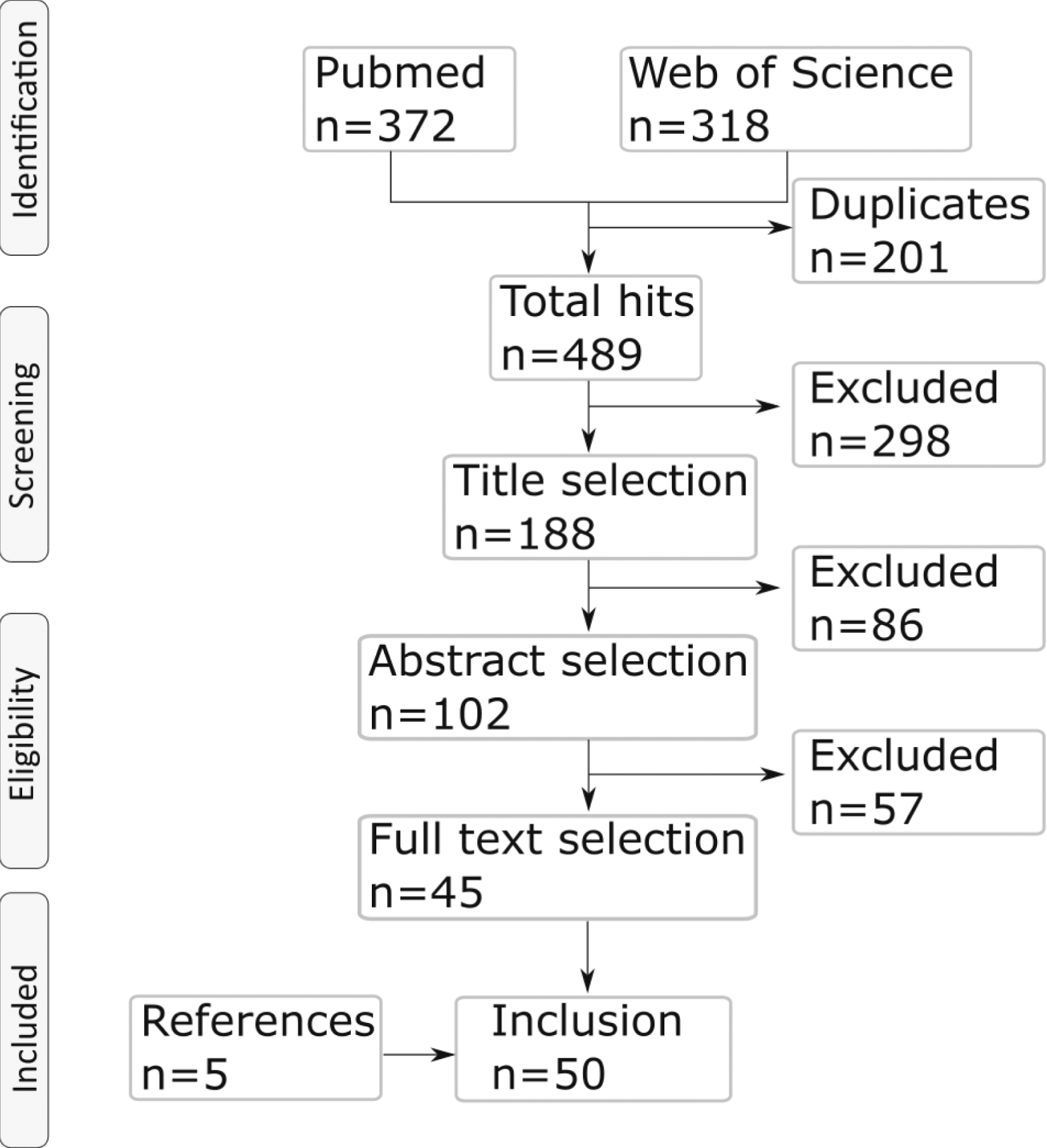
After reading the articles, 62 factors were extracted. Factors were grouped into four domains: feedback, control, exercise and environment. To organize the list of factors with similar topics within each main domain, three to four subdomains were constructed. In the following sections, the domains, subdomains and factors are introduced; a graphical overview of the preliminary framework can be found in Appendix 3.
Feedback
- Topic on which feedback is provided describes the kinematics or kinetics on which feedback is provided. This can for instance be directed at the force production,22–26 on the joint motion that is performed
27
or at the EMG contraction/amplitude.28,29 Feedback can also only be provided on the game score.
30
- The way feedback is provided to the user indicates the stimulation through which feedback is provided. This can be in the form of kinaesthetic stimulation (vibrations),7,31–36 auditory stimulation (sound)
37
or visual stimulation.13,15,26,31,32 - Content of the feedback can be provided by adding animations in real-time on what movement is expected from the user.
7
Feedback during the performance of ADL tasks
38
might be necessary. Difficult tasks might need additional feedback compared to easier tasks.
22
Furthermore, positive feedback instead of negative feedback might be important.
28
Control
- Focus of the training in the domain ‘control’ includes the focus of the training with respect to the muscle activation. Training can be focused on co-contraction/switching commands,28,30,39,40 prolonged contraction,28,30,39 single muscle activation28,30,39 or separability and consistency of patterns.41,42 - Calibration describes the factors regarding the calibration of the system. Calibration of the EMG in different arm positions is necessary since electrodes might shift when postures change.10,43 During the use of pattern recognition, recalibration must happen more often to train the classifier during training.
44
Lastly, the difficulty of the control must be comparable to daily life.28,45 - EMG contains the factors that describe the signal produced by the user and fed to the prosthesis. Providing the visual representation of the EMG signal to the user might be helpful for control.
28
There might be a weight difference between VR and real use of a prosthesis which must be taken into account since it could affect the EMG signals.12,15,44,46 A time-delay between the contraction and the movement of the prosthesis must be minimal, time lag of EMG signals must be prevented.47,48 It might be interesting to train graded EMG control for proportional control.
30
Exercise
- Goal of the exercise describes what training goal is pursued, concerning prosthesis use. The accompanying factors are muscle development,
14
muscle endurance,
49
control of the prosthesis (ability to perform certain grips)14,49 and ability of using the prosthesis fluently.
14
- Execution of the exercise describes the different ways in which a task can be accomplished within the body, like using both hands (bimanual movements),30,50 use the full range of motion (including overhead movements),7,30,51 perform the exercise standing instead or sitting
52
and use full body movements, meaning not only the prosthetic hand.
14
- Focus of the exercise describes the factors that provide the goal of the training, namely just for fun,14,20,38,40,53 practice of activities of daily life,7,14,20,38,52,54,55 facilitate the transfer from VR to real world,14,20,38,40 train subtasks of a movement
54
or to minimize compensatory movements.42,56 - Difficulty and attention included how much the exercise is adaptable to the users’ level,15,54 if there is progression in difficulty during the game14,15,28,57 and what the focus of attention is, since external focus of attention shows better results compared to internal focus of attention.
41
Environment
- Rewards in the training describes the rewards that the user is earning by performing tasks to stay engaged. Rewards might be important8,47 and can have many forms, like achieving goals in the serious game,8,30 a high score
58
or the ability to receive in-game upgrades.8,30,58 People differ to the extent that they are triggered by different rewarding systems14,49. For some users, the game-like nature, which makes the experience competitive, is important.7,58 - Graphics of the environment describes what the user sees in the XR environment. The general graphics (design and looks)
58
and the quality of experienced immersion might be important in VR.11,27 Since the real world is represented in VR, the accurate representation of the position of the hand,
7
accurate physics of objects50,59–61 and real looks of the prosthesis and environment might be important.
12
Regarding the environment itself, it might be important to use a daily life environment.12,51 - Usage of the platform includes factors that describe how, for what and by whom the platform can be used. The platform can for instance be used as a community to talk and interact with other prosthesis users
62
or as a testing environment for different prostheses.
63
The platform could also be used for able-bodied persons to train or play serious games together with prosthesis users.
47
The software related factors are the logging of activities and usage and the privacy of the application which might be important when the system is used at home and the information is sent to a therapist.15,30 Finally, the platform must be user friendly for the therapists14,30 and patients.
54
The area of the environment might be important, as it should be large enough to move around in it.
52
- User’s choice in the environment describes factors on which a user has influence to change aspects in the environment. For instance, the environment can be made adaptable to the user’s preferences,14,28,30 or have a relatable main character.
14
Other factors are the addition and influence of background music.
57
To give the users influence, they might be able to choose aspects within the serious game or game-story,8,30 which can be provided as a variation in included games such as puzzles, quizzes, adventures and shooting/fighting games.
14
Materials and methods – focus groups
For the reporting of the qualitative part of this manuscript, the Consolidated Criteria for Reporting Qualitative Research criteria (COREQ) were used. 64
Participants
Prosthesis users and therapists were invited to take part in separate focus groups. Inclusion criteria were: 1) aged over 18 years; 2) ability to speak and understand Dutch; 3) experience with a myoelectric prosthesis at or proximal from the wrist for more than 1 year for prosthesis users and, for the therapists, at least 5 years of experience of treating the target group. Fifteen prosthesis users from the University Medical Center Groningen, Center for Rehabilitation, were approached by sending an information letter from their medical doctor (CKvdS). Therapists were recruited during a symposium for health care providers regarding upper limb prosthesis in the Netherlands and via the network of one of the authors (CKvdS). The aim was to include six participants per focus group, since this should be enough for data saturation. 65
Ethics
The Medical Ethical Committee of the University Medical Center Groningen provided a waiver for further ethical approval of the study (METc UMCG 2023/109). Participants of the focus groups provided written informed consent before participation. A gift voucher and reimbursement for travel expenses were provided at the end of the focus group to the prosthesis users. Therapists did not receive a gift voucher nor travel expenses, since the focus group was held online.
Interviewer and coders
The focus group interview was conducted by the first author (SGR, PhD), who has previous experience in conducting focus groups and qualitative research. 66 Two female bachelor students (see acknowledgements) conducted the data analysis under the supervision of the first author (SGR). There was no prior relation between the interviewer or the coders and the participants.
Data collection
Explanation of the questionnaire.
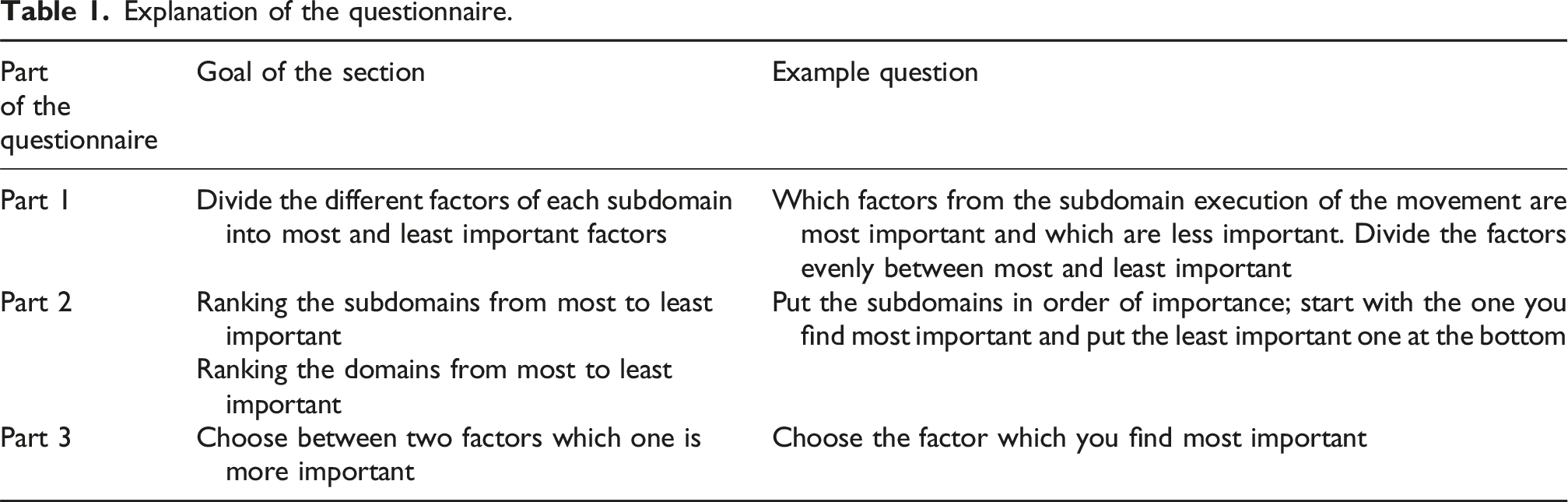
Socio-demographic information of the participants was additionally gathered. Prosthesis users were asked about their age, sex, marital status, highest educational degree, work status, origin of the short arm, side and level of the short arm, cause of limb defect, time since amputation (if applicable), type of prosthesis, self-rated experience with their current prosthesis (unexperienced, somewhat experienced, moderately experienced, experienced and very experienced) and how they learnt to use their prosthesis. Therapists were asked about their age, sex, occupation, years of experience with prosthesis users, which tools they use for training and how many prosthesis users they see per year.
The focus group for prosthesis users was conducted in the rehabilitation centre of the University Medical Center Groningen, Groningen in the Netherlands, the focus group of the therapists was held online. An interview guide was used to structure the conversation. The focus group started with an introduction about the purpose of the meeting, background of the involved researchers and the time schedule. First a VR environment (The Simulation Crew®, Nijmegen, the Netherlands) was shown to the participants, since it is known that participants are better able to comment on an existing environment compared to only imagining it. 28 In this VR environment, the user plays a barista who has to prepare coffee orders for the waitress, while practicing grasping and releasing of cups using a prosthetic hand. After the demonstration, the participants were asked to provide feedback on the current VR using the preliminary framework. Using a slideshow, all domains were addressed separately, and participants were asked to comment on their initial thoughts of the VR. Subsequently, the answers of the completed questionnaires were shown on the slideshow and the results were discussed. Participants were asked to explain why they judged some factors to be more important than others and why some aspects were considered less important. The focus groups were audio-recorded and field notes were taken. The text was transcribed ad verbatim. The transcript was not returned to the participants for comments or corrections, they did however receive a short summary of the main results.
Data analysis
Transcripts were uploaded in Atlas.TI (version 26). A framework method was used to analyse the data, entailing the following subsequent steps: 1) familiarization; 2) construction of themes and coding scheme; 3) indexing; 4) charting and 5) mapping and interpretation. 67 The initial coding tree was the structure of the preliminary framework from the narrative review. Two students performed the initial coding and reached consensus with the first author present. Additional codes were added when necessary. The data from the questionnaires was exported; every factor that was placed in the ‘most important’ box received one point. The sum of the tallies showed how many users found a specific factor important.
Results – focus groups
Characteristics of the prosthesis users that participated in the focus groups.
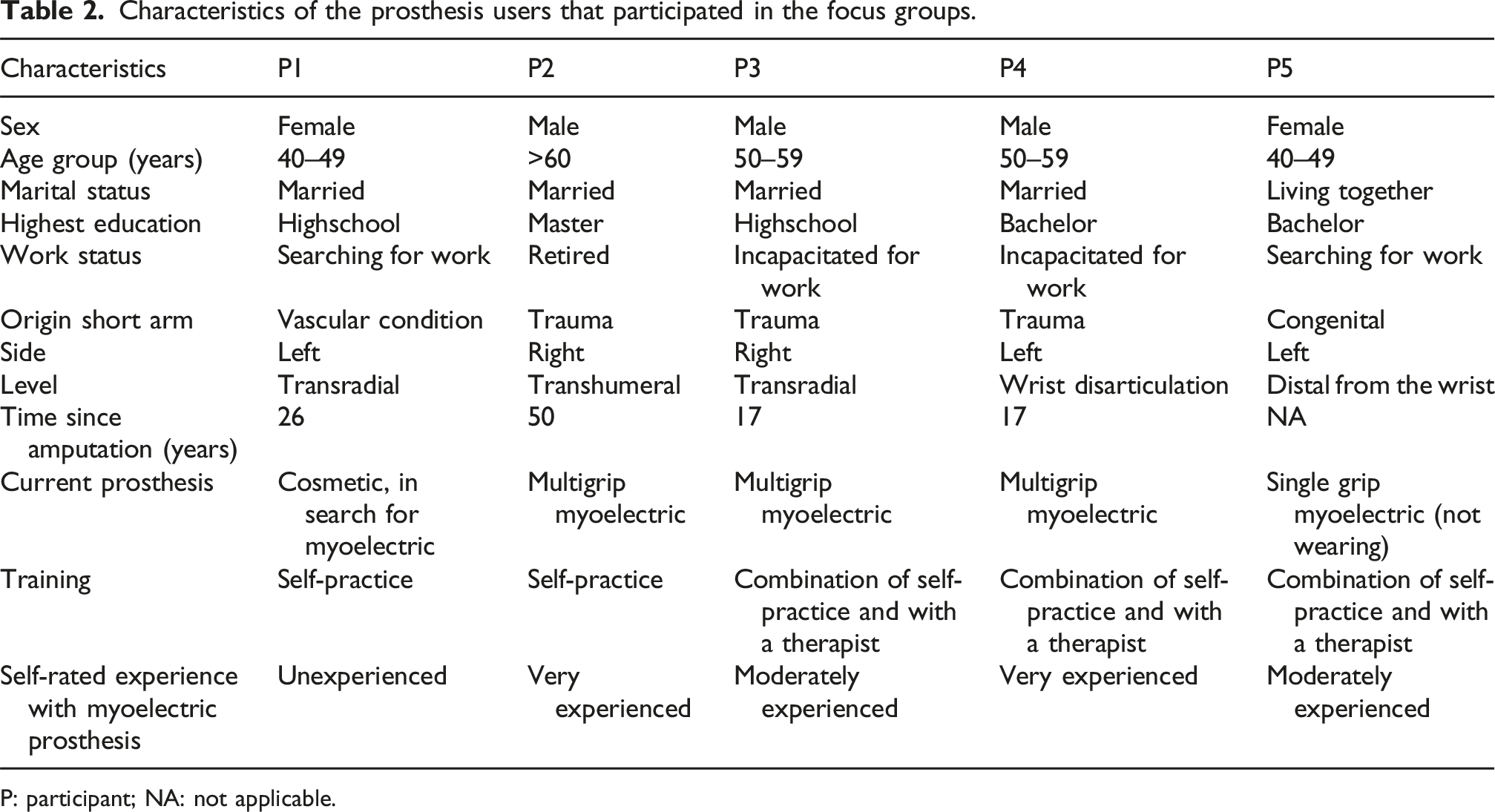
P: participant; NA: not applicable.
Characteristics of the therapists that participated in the focus groups.
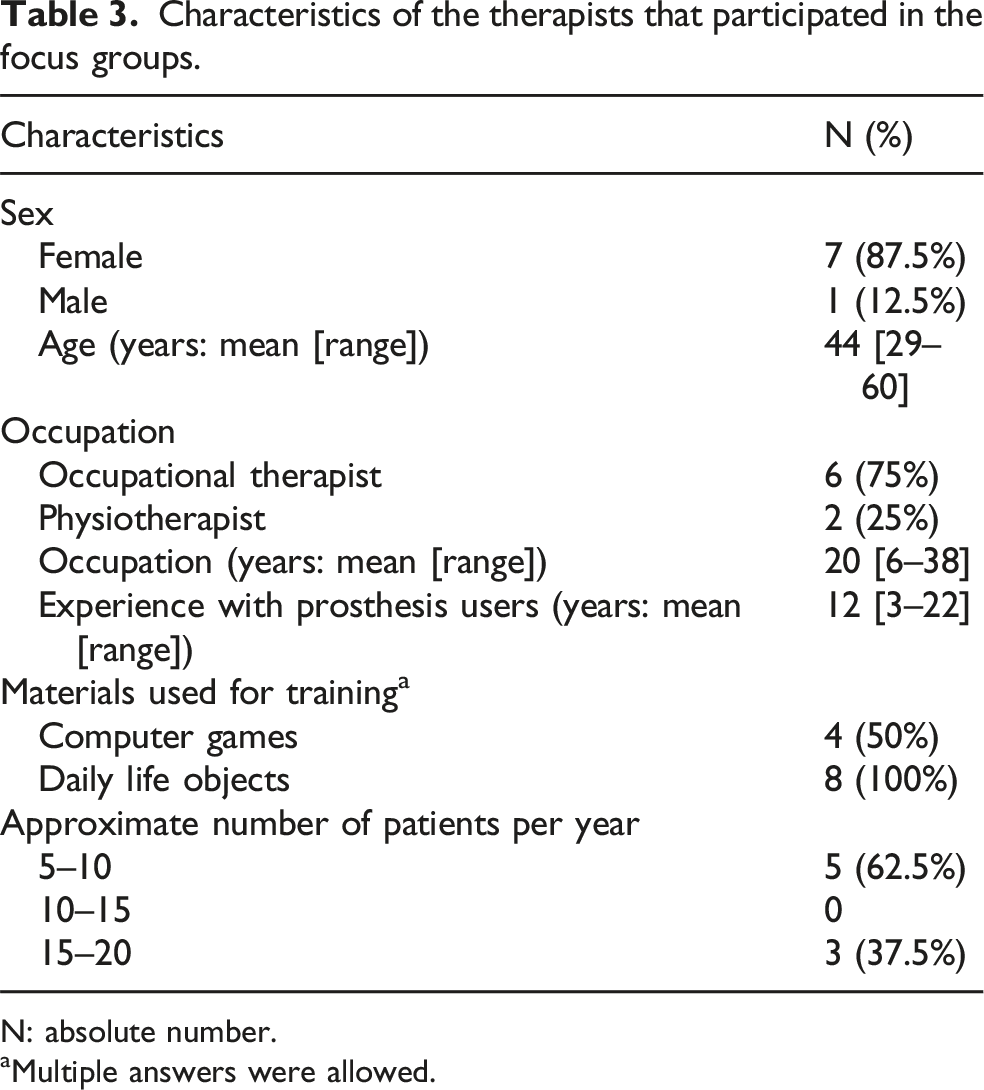
N: absolute number.
aMultiple answers were allowed.
The results of the questionnaire are shown as bar graphs, for both prosthesis users and therapists (Figure 2). Prosthesis users and therapists generally agreed on the most and least important factors per subdomain. There were a few exceptions such as content of the feedback and EMG for control, where the most important factor according to prosthesis users was the least important factor according to therapists. The results of the questionnaire were discussed during the focus groups, which further elucidated the opinions of prosthesis users and therapists. Appendix 4 shows the results of the qualitative analysis from the focus groups: the factors, the findings and the supporting quotes. The section below summarizes the most important findings from Appendix 4 per domain. Outcomes of the questionnaire, which was sent in advance to the focus group participants. Participants had to choose for each factor within each subdomain if it was most important or least important. The factors that were marked as most important were counted; the maximum score was eight for therapists and five for prosthesis users. The middle of the bar is indicated with an additional mark.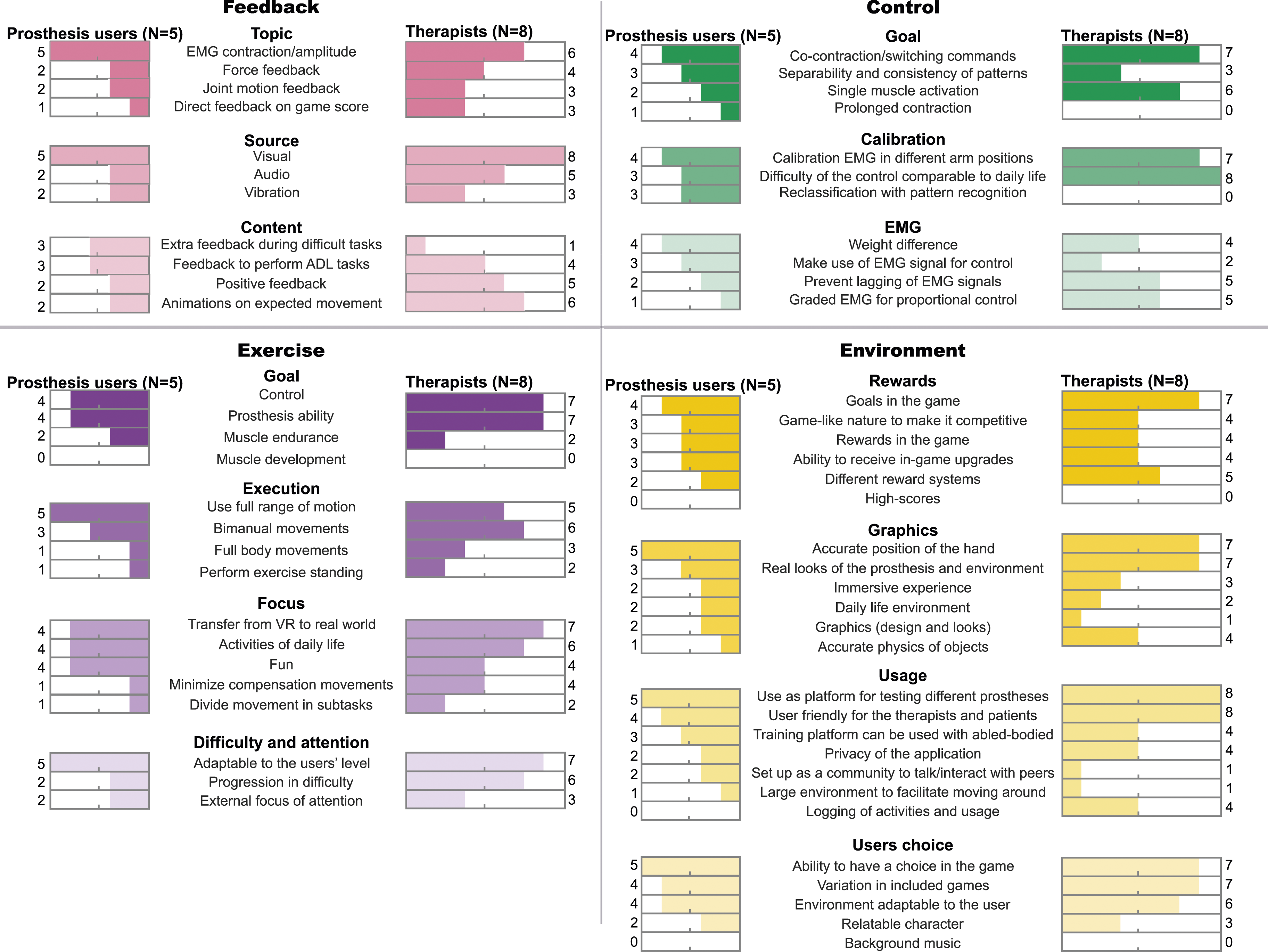
Feedback
The major finding from the focus group was that, contrary to what was found in the questionnaire, positive feedback was the most important factor, since this motivated prosthesis users to continue training. Therapists liked the idea of adding animations of the expected movement, but it was not considered very important, as opposed to the results from the questionnaire. Regarding the type of feedback, EMG and force feedback were deemed most important and could best be visually provided during the learning phase. Prosthesis users and therapists thought that feedback should be turned on or off, based on the needs of the prosthesis user. The therapists would like feedback and EMG signals to be visible to both the user and to them. However, when progressing, feedback should be phased out. Prosthesis users stated that they cannot focus on several types of feedback at the same time, so visual feedback, which was the most important and common form of feedback, needs to be used sparingly. In addition to visual feedback, auditory and vibrotactile feedback can be used occasionally to indicate events such as maximum force production or successful completion of a switching command, which is in accordance with some existing prostheses. However, distracting sounds should be avoided.
Control
End-users thought that XR was a useful way to let prosthesis users experience myocontrol. The most difficult control signals were single muscle activation and co-contraction, according to both prosthesis users and therapists. Using XR to test if novel prosthesis users are able to make these contraction patterns, can help determine if they are suitable for a multigrip prosthesis, which can be very helpful, according to therapists. Prosthesis users foresaw that additional weight should be added to their remnant limb during XR training to simulate the weight of the prosthesis, since the additional weight could alter the EMG signals. Therapists thought it was important to have minimal time lag in the system, less than one second between EMG signal and prosthesis movement, and that proportional control could be trained.
Exercise
Improving the control of the prosthesis was the most important goal of the XR exercise. Movements should be performed while standing and should use a large range of motion in the arm, since a different position of the prosthesis in space affects the EMG signal. Bimanual movements were very important according to all end-users. Therapists stressed the importance of learning the ADL task in the same manner as it will be applied in daily life, which involves the prosthesis hand as an aid to the healthy hand. To improve the transfer from digital to reality, the daily life tasks must be familiar and meaningful to the user. However, the tasks must also be fun, since without fun there is less motivation to train, according to prosthesis users. Users should be challenged with different levels of difficulty, but able to accomplish the tasks since a successful achievement of the goals results in satisfaction, which increases fun and motivation.
Environment
Large individual differences were found in the preferences on rewards, showing that different reward systems should be available which can be turned on or off, based on the user’s preference. In general, all environmental additions such as background music, rewards, feedback or environmental stimuli should have the option to be turned off. Nevertheless, the environment should be easy to set up for the therapist, with a limited number of settings. Competitive gameplay can be useful during later stages of learning to challenge the user. Therapists advocated for a ‘first-person' experience where the user’s arm is visible including a neutral looking prosthesis hand (unbranded), to manage expectations of the prosthesis user. The environment itself was allowed to be futuristic or unreal; however, the task that was practiced must be ADL, according to therapists. Therapists also mentioned that the physical environment that is needed to play in XR should not be larger than a standard therapy room. A unanimous opinion of all end-users was that XR provides the perfect opportunity to test different prostheses and control patterns. Prosthesis users suggested creating an online platform where a user can both train with a prosthesis but also be in contact with peers who already have experience with the prosthesis. The environment should be suitable for all levels of amputation and types of prostheses.
Use of XR during the pre-prosthetic phase was a recurring topic. Prosthesis users and therapists liked the idea of adding this training to usual care. XR training can be used shortly after the amputation. During this period, it provides information regarding the initial abilities of a patient to control their muscles. Based on this information, a better-informed choice can be made regarding which prosthesis might be suitable. Therapists perceived XR to be of added value during the time an amputee is waiting for their prosthesis fitting, to already start the training in XR.
Most important (sub)domain
As a last part of the questionnaire, participants were asked to rate the main domains and subdomains on importance. During the focus group, participants expressed that all domains have interactions with one another, and they did not like to make a forced choice of the most important domain, subdomain or factor. As one therapist described it ‘It is like asking what you like most about bread; the milk or the flour? All of it together makes it bread and the bread is what you can appreciate, not the ingredients’. A ranking of the domains and subdomains is therefore not presented.
Comparisons
Participants were asked to compare two factors and choose their most preferred option (Figure 3). During the focus group it became apparent that people interpreted the term upgrades as if difficulty would progress in XR, instead of receiving new features like a differently coloured prosthesis. However, high scores were not really deemed important by most participants. An interesting observation was made during the focus group with therapists: although they at first thought that ADL was the most important focus of the training, this shifted towards fun during the discussion. They figured that without fun, there is no incentive to train and that this factor is more important than ADL. During all focus groups, it became clear that two-handed tasks were more important than initially thought. Due to the discussion, more participants saw the merit in training with two hands, similarly to how tasks are performed in daily life. Results of the comparisons of two opposing factors. The maximum score was eight for therapists and five for prosthesis users. The middle of the bar is indicated with an additional mark.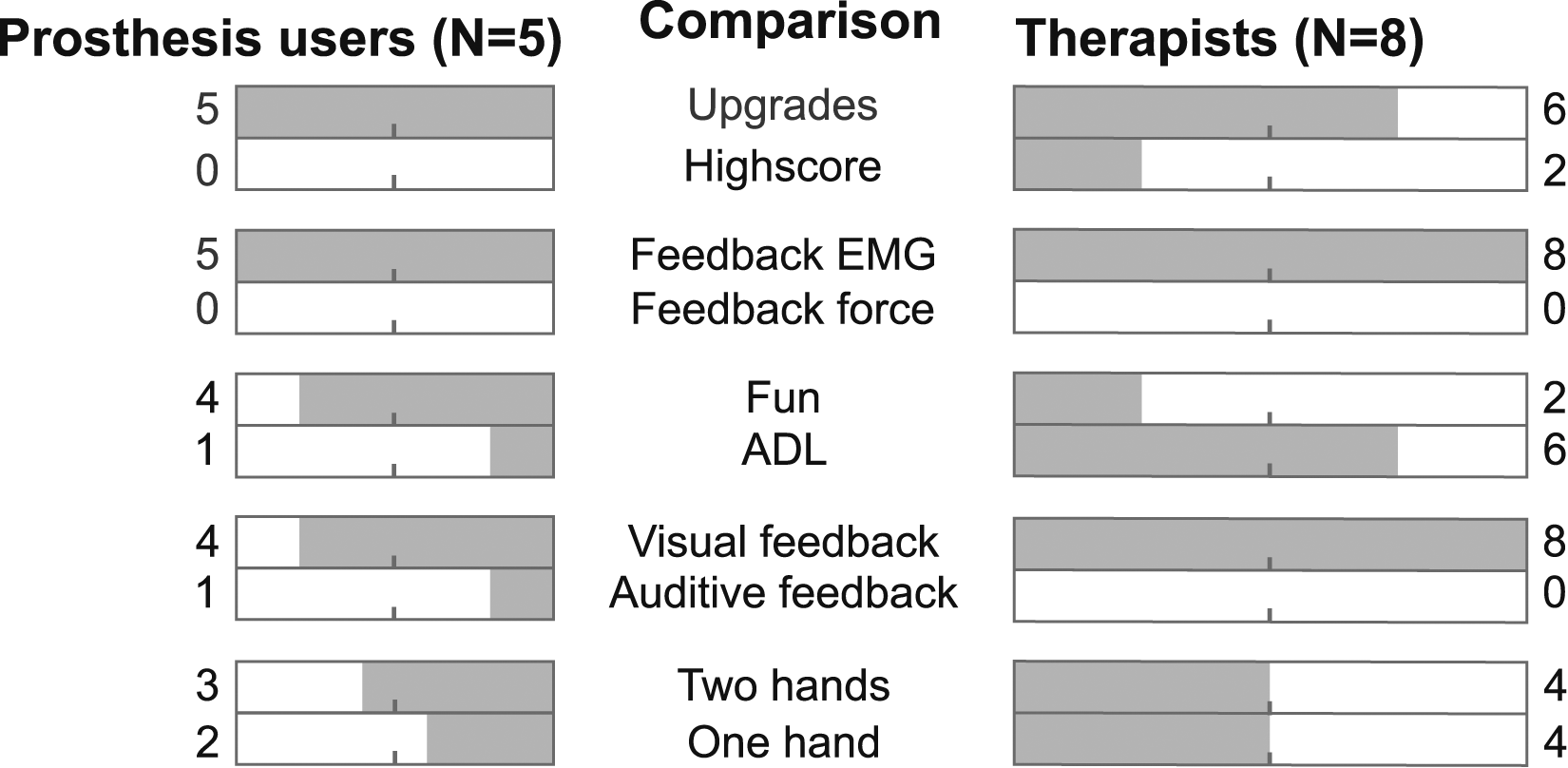
Final/concluding framework
Based on these results, a final framework was consolidated (Figure 4). Eighteen factors were omitted since they were found to be less or not important during the focus group or could be combined with other factors. Phrasing in the framework was adjusted to further explain the factors, based on the comments of the focus groups. Two factors were added to the domain of environment, namely the use of XR during the pre-prosthetic phase and managing expectations of the user. The final framework contains 46 factors with practical advice for designers to develop an XR environment. Factors are ranked within the subdomain based on importance, starting with the most important factor. The final framework contains four domains with each 3 to 4 four subdomains. The factors in each subdomain are arranged from top to bottom on importance, where the factor on top is most important. The subdomains within the main domain are not ranked on importance, since no consensus could be reached.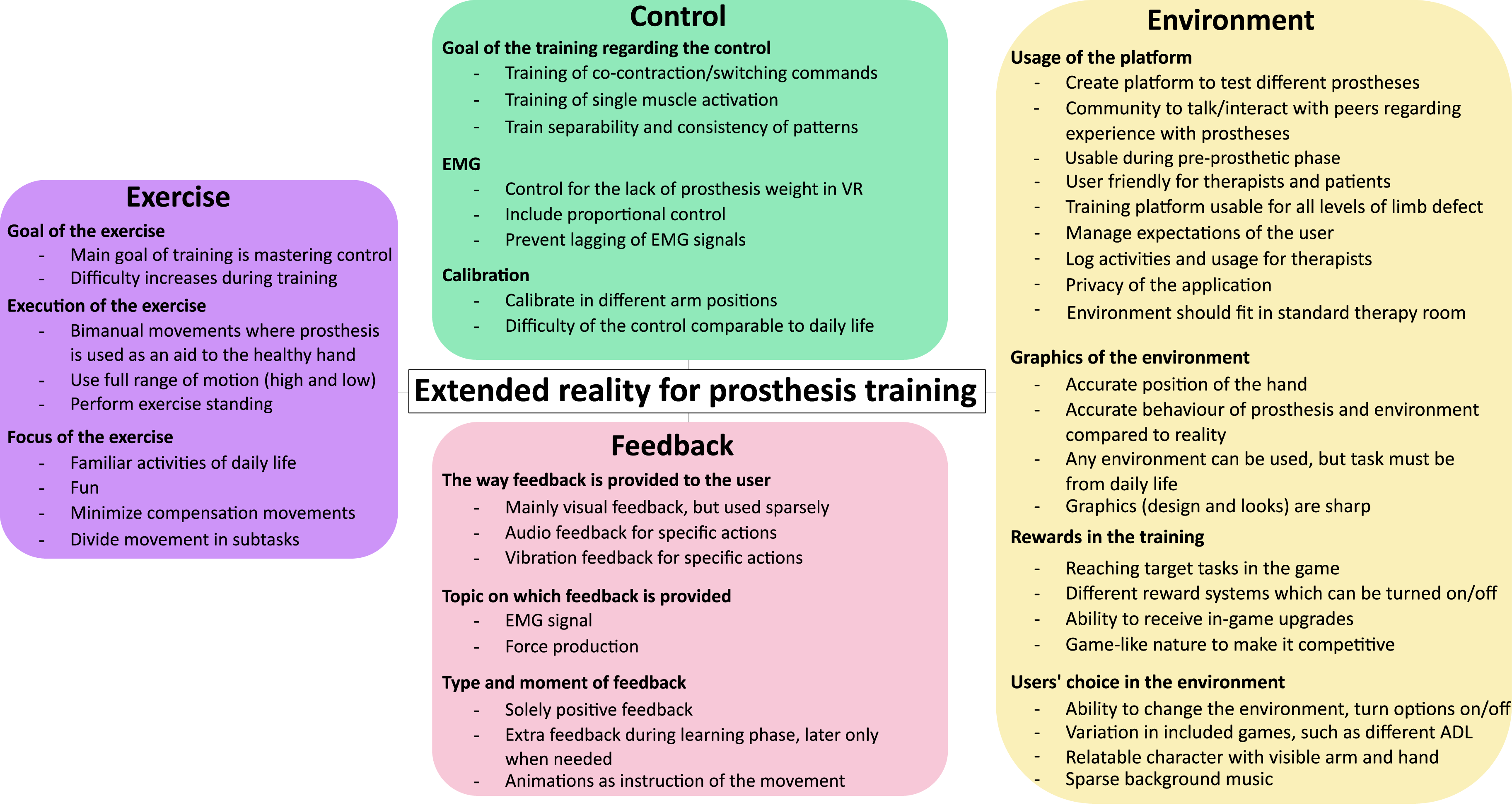
Discussion
Main findings
In this study a framework was developed, based on a narrative review of the latest literature and input from end-users via focus groups, which shows the important factors that need to be included when designing an XR environment to train myoelectric prosthesis control. XR environments have the added benefit, compared to standard prosthesis training, to motivate users, 47 keep them engaged longer 57 and provide objective feedback on their performance in order to continue training and improve their prosthesis control skills. Every domain in this framework contributes to an engaging experience and is therefore important to consider during development. It is therefore not surprising that prosthesis users and therapists expressed that it was very hard to determine which factor of an XR environment is most important, since all factors influence each other. The environment seems to mainly contribute to the fun and engaging part of XR, while the control, exercise and feedback stimulate the user to learn prosthesis control. The last three domains should be tailored to the participants to create a flow experience, meaning that the challenges and capabilities of the users are balanced. 17 The final framework containing 46 factors provides an insight in the wishes and needs of end-users for future developers and researchers. While some factors reflect a wish of the user (‘Create platform to test different prostheses’), other factors are a necessity for every XR environment focused on learning to use myoelectric prostheses (‘Main goal of the training is mastering control’). Developers should aim to implement as many of the recommendations as possible. Since this might not be feasible for all types of VR and AR environments, designers can try to include certain combinations of factors at different stages in a serious game, for instance in different levels or different minigames. The underlying point here is that in doing so, the needs of the end-user play a more prominent role in the development of XR environments, which brings the field to the next level and out of the purely developmental focus.
Rewards for young and old
Although participants in the focus groups generally agreed with one another, there were some topics where views differed. Within the focus group of the prosthesis users, no consensus could be reached on the best reward system. Two participants in particular differed, with a younger participant expressing a strong preference for high scores and in-game features, while an older participant strongly disliked these features and did not care about the environment as long as the task could be learnt. These viewpoints are in agreement with previous research into experienced differences in motivation between older and younger adults, which shows that younger adults are more focussed on competition and graphics of XR while older adults value the enjoyment, performance of the desired movements and physical and cognitive benefits more. 68 Having different reward systems which together with the option to turn options on or off is therefore valuable, to spark motivation tailored to individual users. 58
Bimanual training
Therapists reached the conclusion during the focus group that tasks in XR should be trained using two hands instead of only the prosthesis side. During the discussion, some therapists advocated why bimanual training might be important to facilitate transfer to reality. Due to bimanual training, the interaction between the two hands as well as the role of the prosthesis during the task will be trained. Most studies that were included in the narrative review trained only the prosthesis hand and did not interact with the non-affected hand, with a few exceptions.11,24 The current study and previous qualitative research also highlighted the end-users’ wish to include bimanual training.14,30 It has been shown that ADL tasks are mainly performed with the intact limb, occasionally bimanual but almost never with solely the prosthesis.69,70 Therefore, bimanual training seems essential to be included in XR training, to learn to coordinate the interaction between the hands, especially when performing ADL tasks. 30
Fun more important than ADL
Therapists changed their opinion during the focus group towards the importance of fun during the training compared to ADL. Initially during the questionnaire, most therapists chose ADL over fun, based on their therapeutic views that ADL tasks will result in better transfer compared to fun non-serious games. However, during the focus group, the importance of fun for motivation of the user was further elaborated in the discussion. More therapists agreed with the view that without fun, there is less motivation to train. The debate regarding the trade-off between ADL and fun has recently been highlighted by Garske et al., 20 most serious games are focused on fun but not ADL or the other way around. Serious XR games that have both ADL and are fun to play, are still rare and need further attention to be developed. From the articles that were included in the narrative review only six of the 50 studies included ADL tasks.11,45,50,51,59,61
XR to test and talk
The prosthesis users were enthusiastic about the idea of developing an XR environment in which different prostheses can be tested, combined with a peer support network with other prosthesis users. Prostheses can have different control patterns with varying number of grips which increase the complexity of the control. 71 The idea is that a (potential) user can test a control pattern of a specific prosthesis and join a conversation with users that already have experience with the prosthesis of interest. Testing different control patterns has been shown to improve the selection process of a prosthesis. 71 An even better-informed decision can be made when the prosthesis user can gather additional information on experiences of other users. An online platform might facilitate this using a forum, direct text messages or video calls. Most prosthesis users appear to be open to the idea of online peer meetings. 62 Such a platform should be made in co-creation with users to facilitate their needs within the environment. 62
Motor learning
The framework developed in this study can be further expanded by adding motor learning principles in the training, such as task-specificity or movement planning. Motor learning strategies can enhance the task practice and increase the rate of learning, also in XR environments.4,72,73 Levin and colleagues provided an elaborate overview of some basic principles of motor control and motor learning and how these views can be translated into an XR environment. 4 Note that for those implementing motor learning principles the views underlying the exploited motor learning approach need to be taken into account. 74 The authors are aware that this might be a useful addition to the current framework, perhaps as a subdomain in ‘exercise’. However, adding motor learning principles to the framework seemed out of the scope of this study, since prosthesis users might not be able to comment on these factors and therefore it was not included in these focus groups.
Strengths and limitations
The strength of this study is the use of a combination of literature findings (the narrative review) and users-therapists' opinions (the focus groups) to produce a final framework, which can assist researchers and commercial designers as a reference during the development of XR environments for prosthesis control training. The narrative review has some limitations that require mentioning. Articles could have been missed due to the search strategy used or the databases consulted. Searching an additional database could have resulted in more outcomes; however, PubMed and Web of Science are two of the biggest databases available for medical sciences. Furthermore, one author reviewed the articles, which may have resulted in factors being overlooked. The extracted factors were divided in subdomains based on the opinion of the authors, which might have resulted in disputable classification.
Some limitations of the focus groups need mentioning as well. Only five prosthesis users were included in the focus group, which might not be a representative sample of the diverse upper limb prosthesis population. The questionnaire regarding the importance of the factors was provided in advance to the focus groups, which has some implications. Participants misunderstood some factors, although additional information was provided regarding more difficult to understand factors. Misinterpretation was resolved during the focus group by showing a demo of an XR system and further explaining the factors. Participants could have changed their opinion after the demo and clarification of the factors. Showing the demo of an XR posed a risk of influencing the opinion of the user. The final framework was therefore constructed with the additional input from the focus group. Furthermore, participants disliked that they were forced, in their questionnaire answers, to split the factors evenly between the box ‘most important’ and ‘least important’. The ranking of the domains and subdomains was also experienced as a very difficult exercise, especially since every domain had certain factors that were of importance.
Conclusion
A validated framework was developed regarding the important factors, according to end-users, which need to be incorporated when developing an XR environment to learn control of a myoelectric upper limb prosthesis. The final framework shows the importance of incorporating several factors within the domains feedback, control, exercise and environment. All domains have equal importance, since the interaction between the factors makes XR useful. This manuscript encourages future researchers to employ this framework during the design phase and verify using usability tests whether XR is well-received by end-users.
Supplemental Material
Supplemental Material - Users’ and therapists’ perspectives on the design of extended reality environments to train prosthesis control: Narrative review and focus group
Supplemental Material for Users’ and therapists’ perspectives on the design of extended reality environments to train prosthesis control: Narrative review and focus group by SG Rozevink, A Murgia, RM Bongers and CK van der Sluis in Technology and Disability.
Supplemental Material
Supplemental Material - Users’ and therapists’ perspectives on the design of extended reality environments to train prosthesis control: narrative review and focus group
Supplemental Material for Users’ and therapists’ perspectives on the design of extended reality environments to train prosthesis control: Narrative review and focus group by SG Rozevink, A Murgia, RM Bongers and CK van der Sluis in Technology and Disability.
Supplemental Material
Supplemental Material - Users’ and therapists’ perspectives on the design of extended reality environments to train prosthesis control: narrative review and focus group
Supplemental Material for Users’ and therapists’ perspectives on the design of extended reality environments to train prosthesis control: Narrative review and focus group by SG Rozevink, A Murgia, RM Bongers and CK van der Sluis in Technology and Disability.
Supplemental Material
Supplemental Material - Users’ and therapists’ perspectives on the design of extended reality environments to train prosthesis control: narrative review and focus group
Supplemental Material for Users’ and therapists’ perspectives on the design of extended reality environments to train prosthesis control: Narrative review and focus group by SG Rozevink, A Murgia, RM Bongers and CK van der Sluis in Technology and Disability.
Statements and declarations
Footnotes
Acknowledgements
We would like to thank Evelien Overbeek and Rianne Vogt for their assistance in the qualitative data analysis. We thank The Simulation Crew® (Nijmegen, the Netherlands) for providing the preview of the serious game. This work could not have been completed without the help of the prosthesis users and therapists who participated in the research, we thank them for their valuable insights.
Author contributions
Conception: SGR, AM, RMB and CKvdS. Performance of work: SGR. Interpretation or analysis of data: SGR, AM, RMB and CKvdS. Preparation of the manuscript: SGR. Revision for important intellectual content: AM, RMB and CKvdS. Supervision: AM, RMB and CKvdS. All authors read and approved the final manuscript.
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project has received funding from the European Union’s Horizon 2020 research and innovation programme under grant agreement No. 965731.
Ethical approval
The Medical Ethical Committee of the University Medical Center Groningen provided a waiver for further ethical approval of the study (METc UMCG 2023/109).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.