
Abstract
Race/ethnicity and individual-level socioeconomic status (SES) may contribute to health disparities in liver transplant (LT) outcomes. The socioeconomic conditions of a neighborhood may either mitigate or exacerbate these health disparities. This retrospective study investigated the relationship between race/ethnicity, individual- and neighborhood-level SES, and LT outcomes, and whether neighborhood-level SES modified the relationship between individual factors and LT outcomes. Adult individuals who underwent LT between 2010 and 2019 (n = 55,688) were identified from the United Network for Organ Sharing database. Primary exposures were race/ethnicity, education, primary insurance type, and the Social Deprivation Index (SDI) scores. Education and primary insurance type were used as proxies for individual-level SES, while SDI scores were used as a proxy for neighborhood-level SES. The primary outcome was time to occurrence of graft failure or mortality. Cox proportional hazard models were used to examine the associations between the exposures and outcomes. LT recipients who were Black (hazard ratio [HR]: 1.27, p < .0001), completed high school or less (HR: 1.06, p = .002), and had public insurance (HR: 1.14, p < .0001) had a higher rate of graft failure or mortality than those who were White, completed more than high school, and had private insurance, respectively. The SDI scores were not significantly associated with LT outcomes when adjusting for individual factors (HR: 1.02, p = .45) and did not modify the associations between individual factors and LT outcomes. Findings of this study suggest that disparities based on individual factors were not modified by neighborhood-level SES. Tailored interventions targeting the unique needs associated with race/ethnicity and individual-level SES are needed to optimize LT outcomes.
Introduction
Liver transplantation (LT) has been a life-saving option for individuals with end-stage liver disease. The long-term goals of LT are to maintain optimal transplant function (Yoo & Thuluvath, 2004) and to achieve fulfilling lives (Duffy et al., 2010). However, a subset of patients is at risk of adverse outcomes, such as graft failure or mortality. A top priority is to identify LT recipients at increased risk of these adverse outcomes and provide timely interventions. Literature suggests that one’s race/ethnicity and individual-level socioeconomic status (SES), which includes one’s educational attainment, occupation, and financial security, may contribute to variations in outcomes (Braveman & Gottlieb, 2014).
Disparities by race/ethnicity exist throughout the LT process, from access to the transplant to its receipt. Racial and ethnic minorities, including Black, Hispanic, and Asian patients, are less likely to be referred for LT, are often referred at later stages of liver diseases, and are less likely to receive living donor LT, which has advantages in reducing waiting times and post-LT mortality (Barbetta et al., 2021; Mathur et al., 2010; Nephew & Serper, 2021; Nobel et al., 2015). After receiving LT, they have higher risks for worse transplant outcomes. Black LT recipients experience higher rates of graft failure and mortality than recipients from other racial backgrounds (Kemmer & Neff, 2010; Ross-Driscoll et al., 2021).
Individual-level SES, particularly education and insurance types, also contributes to disparities in LT. Educational attainment can influence an individual’s career opportunities, affecting income and employment stability, and ultimately impacting their financial ability to afford healthcare (Zajacova & Lawrence, 2018). It also impacts their knowledge and adoption of healthy behaviors and their ability to navigate healthcare systems effectively (Clouston & Link, 2021; Zajacova & Lawrence, 2018). Lower levels of educational attainment are associated with a higher prevalence of advanced stages of liver disease and increased waitlist and post-LT mortality (Cotter et al., 2024; Fedeli et al., 2015; Sierra et al., 2024; Stroffolini et al., 2020). Furthermore, insurance type affects health outcomes by influencing access to quality healthcare, timely treatment, and continuity of care (McWilliams, 2009; Woolhandler & Himmelstein, 2017). Public insurance holders are half as likely to receive LT compared to private insurance holders and face an increased risk of post-LT mortality (Mansour et al., 2022; Stepanova et al., 2020; Yu et al., 2010).
The influence of an individual’s race/ethnicity and SES on transplant outcomes may vary based on the social and economic characteristics of the neighborhood where an LT recipient lives. Racial/ethnic minorities and individuals with lower SES are often segregated into socially and economically disadvantaged areas, referred to as neighborhoods with low SES (Clouston & Link, 2021). These neighborhoods tend to offer fewer secure and health-promoting environments, limited healthcare access, and reduced educational and employment opportunities. These factors can collectively impede individuals’ capacity to maintain healthy lifestyles, consequently decreasing the likelihood of favorable health outcomes and exacerbating health disparities (Onder et al., 2020; Robinette et al., 2017; Yoo & Thuluvath, 2004).
These health disparities may be more pronounced in urban settings, which frequently exhibit higher racial, ethnic, and economic diversity, than rural areas. While urban areas typically provide better living standards in terms of education, employment, and healthcare than rural areas, these advantages are not evenly distributed (Pew Research Center, 2018). Socioeconomic segregation is more prevalent in urban areas than rural ones (Nilforoshan et al., 2023). As a result, individuals living in disadvantaged, segregated neighborhoods may not have access to as many resources and therefore have poorer health outcomes than individuals living in advantaged neighborhoods in urban areas (Barondess, 2008).
Current literature within the LT population has primarily focused on investigating health disparities in relation to an individual’s race/ethnicity and SES. While neighborhood-level SES was examined as a proxy for individual-level SES in earlier studies (Quillin et al., 2014; Yoo & Thuluvath, 2004), recent research considers it as an indicator of neighborhood environments affecting health outcomes (Niazi et al., 2021; Ross et al., 2017). They documented that lower neighborhood-level SES has a significant impact on increased graft failure and patient mortality (Niazi et al., 2021; Quillin et al., 2014; Ross et al., 2017). However, these studies primarily investigated the independent associations of race/ethnicity, individual-level SES, and neighborhood-level SES with transplant outcomes, without considering that neighborhood-level SES might modify the relationships between race/ethnicity and individual-level SES and transplant outcomes. A recent study found that racial/ethnic minorities living in low SES neighborhoods have a 31% increased risk of not being listed for LT compared to those living in high SES neighborhoods (Strauss et al., 2023). Yet, the modification effect of neighborhood-level SES on these disparities has not been thoroughly investigated in the context of post-transplant outcomes. Furthermore, whether the impact of neighborhood-level SES on transplant outcomes varies across urban and rural geographical regions has not been addressed in existing research. This knowledge gap may limit our understanding of how to develop tailored strategies to address disparities in the LT population. Thus, this study investigated whether neighborhood-level SES is associated with transplant outcomes along with race/ethnicity and individual-level SES in the LT population. We then further examined whether the effects of race/ethnicity and individual-level SES on transplant outcomes differ by neighborhood-level SES and whether the effects of neighborhood-level SES differ by urban and rural geographical regions.
Materials and Methods
Design and Data Source
This study used data from the Organ Procurement and Transplantation Network (OPTN). The OPTN data system includes data on all donor, wait-listed candidates, and transplant recipients in the US, submitted by the members of the Organ Procurement and Transplantation Network (OPTN). The Health Resources and Services Administration (HRSA), U.S. Department of Health and Human Services provides oversight to the activities of the OPTN contractor. This study was exempted by the Northeastern University Institutional Review Board (20-07-08). The study population comprised LT recipients who received LT between 2010 and 2019 in the United States and were 18 years or older at the time of transplant. LT recipients were followed for up to 11 years after transplant in the United Network for Organ Sharing database. Those who received a simultaneous multiorgan transplant were excluded from the study.
Variables
The primary outcome of this study was a composite of graft failure or death occurring within 10 years after LT.
Race/ethnicity and individual- and neighborhood-level SES factors were our primary exposures of interest. LT recipient’s highest education level at registration and primary insurance at transplant were used as proxy variables for individual-level SES. To assess the socioeconomic conditions of the geographical regions in which LT recipients reside, we utilized the Social Deprivation Index (SDI) at the Zip Code Tabulation Area (ZCTA) level (Robert Graham Center – Policy Studies in Family Medicine & Primary Care, 2018). LT recipients’ ZIP code reported at the time of transplant was used to define their SDI using publicly available sources (Robert Graham Center – Policy Studies in Family Medicine & Primary Care, 2018). The widely used SDI is a composite measure of seven sociodemographic characteristics, such as income, education, and house and vehicle ownership, collected in the American Community Survey (ACS) (Butler et al., 2004; Robert Graham Center – Policy Studies in Family Medicine & Primary Care, 2018). The SDI ranges between 1 and 100, with higher scores indicating higher levels of social deprivation. Based on prior research that used the cold spot definition for low- and high-deprivation groups (Liaw et al., 2018), we applied a cutoff of 70 to SDI for our primary analysis.
To define the urban/rural geographical regions where LT recipients reside, we used the ZIP code approximations of rural–urban commuting area codes (RUCA 2.0) that were based on 2006 ZIP code areas (Rural Health Research Center, n.d.). The RUCA defines urban and rural areas considering population density and urbanization as defined by the Census Bureau combined with work commute patterns. LT recipients’ ZIP code reported at the time of transplant was used to assign RUCA codes. We then dichotomized LT recipients into urban and rural residents following the published recommendations (Rural Health Research Center, n.d.).
The recipient’s demographic and clinical characteristics of age, sex, primary reason for LT, Model for End-Stage Liver Disease (MELD) score at transplant, encephalopathy at transplant, comorbidities at transplant (diabetes and renal failure defined as serum creatinine ≥2.5 mg/dl), the number of previous liver transplants, liver dysfunction defined as total bilirubin ≥2 mg/dl at transplant, functional status at transplant, and RUCA code were included in the analysis. In addition, the donor’s age, race, sex, BMI, total cold ischemic time, standardized deceased donor risk index (Feng et al., 2006), and living donor risk index (Goldberg, 2016) were included in the analysis.
Statistical Analysis
Summary statistics are presented for race/ethnicity, individual- and neighborhood-level SES, demographic, and clinical characteristics. A complete case analysis was done, excluding patients with missing values on all the variables included in the analysis. We compared the characteristics of those with and without missing data on these variables (see Supplemental Table 1).
The primary outcome was time to occurrence of graft failure or death, whichever occurred first. Time 0 was defined as the time of transplant and patients without an event were censored either at the time of loss to follow-up or at 10 years. The primary exposure variables were race/ethnicity and the following SES factors: education, insurance type, and SDI.
We estimated Kaplan–Meier curves and Cox proportional hazards regression models to investigate the associations between the outcome and race/ethnicity and SES factors. To understand how these associations might change with and without adjustment for demographic and clinical factors, we fit a series of sequential Cox models: (1) separate unadjusted models for each race/ethnicity and SES factor, (2) separate models for each race/ethnicity and SES factor that adjusted for demographic and clinical factors, (3) one model that included race/ethnicity and all SES factors, and (4) one model that included race/ethnicity and all SES factors and adjusted for demographic and clinical factors. The demographic and clinical factors included in the model were selected based on potential associations with the outcome identified in the existing literature; the exception was that factors that were highly collinear with others (correlation ≥ 0.5) were excluded from the model. Recipient liver dysfunction and functional status at transplant were removed due to collinearity with the MELD score at transplant. Donor age was removed due to collinearity with the standardized donor risk index. Residual-based model diagnostics were applied to assess the proportional hazards assumption, linearity, and potential outliers.
To assess for effect modification of the relationships between the outcome and race/ethnicity and individual-level SES factors by SDI and urban/rural geographical regions, we added interaction terms to model 2 above. We also assessed whether the relationship between the outcome and SDI was modified by urban/rural geographical regions.
One sensitivity analysis was performed using continuous SDI, while a second sensitivity analysis tested model 4 in different donor type (living or deceased) subgroups (see Supplemental Table 2).
Analyses were performed in R version 4.1.0 with RStudio 2022.02.3+492 (“Prairie Trillium” Release for Windows) and a two-sided alpha of 0.05 was used. Survival analysis was conducted using survival package version 3.2-11.
Results
A total of 55,688 LT recipients met the inclusion criteria. Baseline characteristics are presented in Table 1. The mean age of LT recipients was 55.3 (standard deviation [SD] = 10.8). The majority were White (72.0%), followed by Hispanic (13.7%) and Black (8.6%). Over half completed more than high school (52.6%) and had private insurance (54.3%). Furthermore, most were urban residents (85.8%) with a mean SDI score of 49.1 (SD = 28.5). Less than 25% of LT recipients experienced graft failure or death during the 10-year follow-up period.
Summary of Baseline Characteristics and Outcomes (N = 55,688).
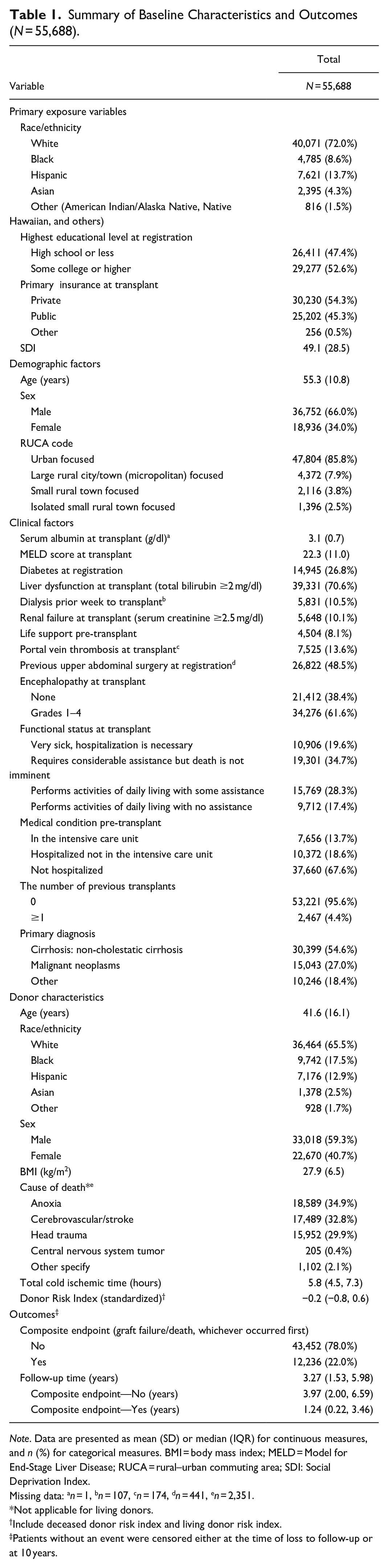
Note. Data are presented as mean (SD) or median (IQR) for continuous measures, and n (%) for categorical measures. BMI = body mass index; MELD = Model for End-Stage Liver Disease; RUCA = rural–urban commuting area; SDI: Social Deprivation Index.
Missing data: an = 1, bn = 107, cn = 174, dn = 441, en = 2,351.
Not applicable for living donors.
Include deceased donor risk index and living donor risk index.
Patients without an event were censored either at the time of loss to follow-up or at 10 years.
Race/ethnicity and all individual-level SES factors were significantly associated with the time to occurrence of graft failure or death in all models (Table 2). Specifically, in the adjusted model with race/ethnicity and all SES factors (Model 4), Black recipients had a higher rate of graft failure or death than White recipients (hazard ratio [HR] = 1.27, p < .0001), while Asian and Hispanic recipients had a lower rate of the outcome than White recipients (HR = 0.83, p = .0001 and HR = 0.88, p < .0001, respectively). Public insurance holders and those who completed high school or less had a higher rate of graft failure or death than those with private insurance coverage (HR = 1.14, p < .0001) and more than a high school education (HR = 1.06, p = .002), respectively. The SDI scores were significantly associated with the outcome in the adjusted and unadjusted single-factor models, but not when race/ethnicity and all SES factors were included in one model. The results of the sensitivity analysis conducted using continuous SDI were aligned with the findings from the analysis with categorized SDI. The sensitivity analysis stratified by donor type (living or deceased) demonstrated different results on the association between race/ethnicity and LT outcomes, particularly in the living donor LT group. Asian recipients in the living donor group had a higher rate of graft failure or mortality than White recipients (see Supplemental Table 2).
Associations Between Race/Ethnicity and SES Factors With Time to Occurrence of Graft Failure or Death.
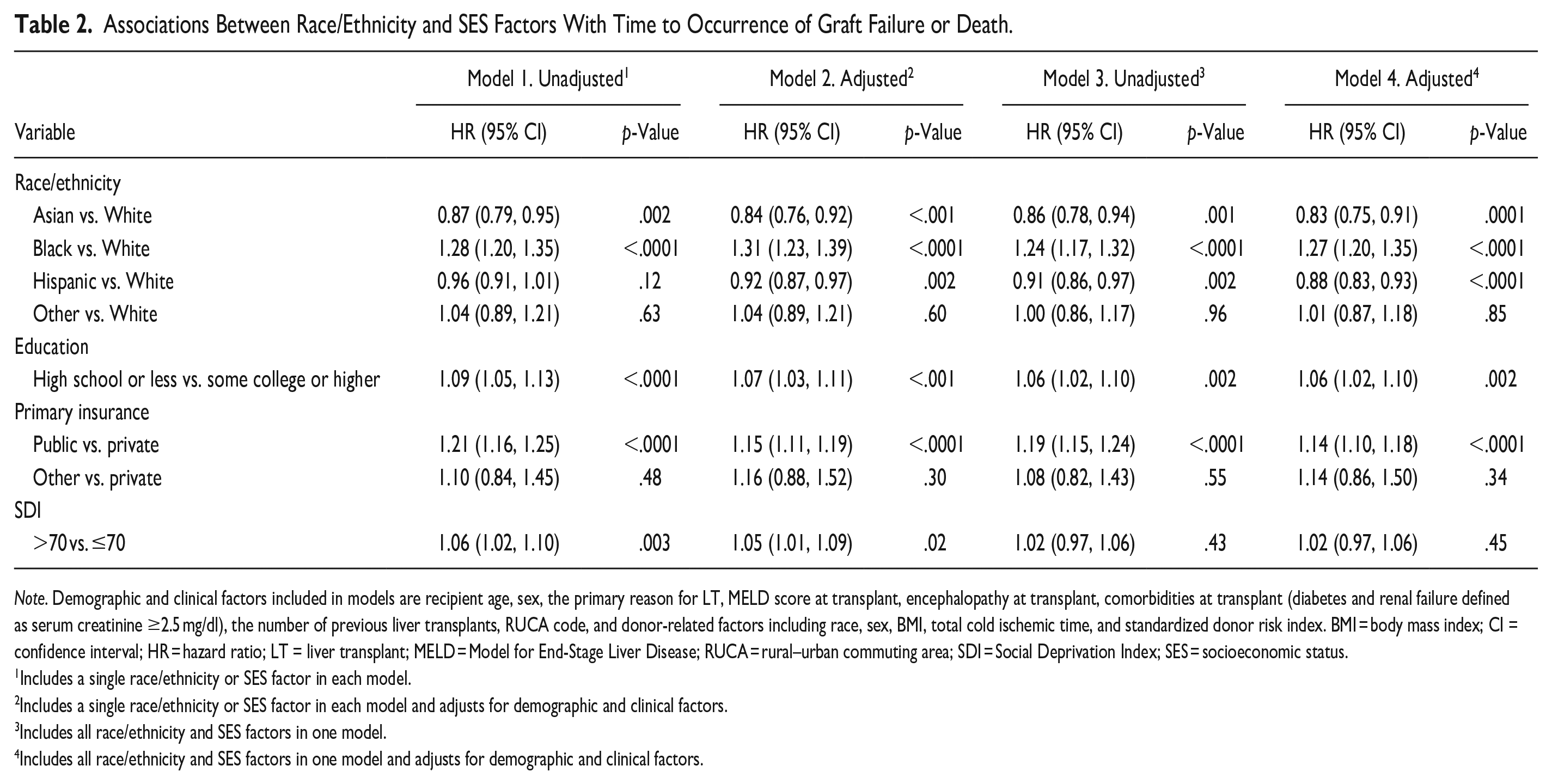
Note. Demographic and clinical factors included in models are recipient age, sex, the primary reason for LT, MELD score at transplant, encephalopathy at transplant, comorbidities at transplant (diabetes and renal failure defined as serum creatinine ≥2.5 mg/dl), the number of previous liver transplants, RUCA code, and donor-related factors including race, sex, BMI, total cold ischemic time, and standardized donor risk index. BMI = body mass index; CI = confidence interval; HR = hazard ratio; LT = liver transplant; MELD = Model for End-Stage Liver Disease; RUCA = rural–urban commuting area; SDI = Social Deprivation Index; SES = socioeconomic status.
Includes a single race/ethnicity or SES factor in each model.
Includes a single race/ethnicity or SES factor in each model and adjusts for demographic and clinical factors.
Includes all race/ethnicity and SES factors in one model.
Includes all race/ethnicity and SES factors in one model and adjusts for demographic and clinical factors.
The association between the outcome and race/ethnicity and individual-level SES factors was not modified by the SDI scores or urban/rural geographic regions (Tables 3 and 4). Finally, the association between the SDI scores and time to occurrence of graft failure or death was not modified by the urban/rural geographic regions (Table 4).
Association Between Race/Ethnicity and Individual-Level SES Factors With Time to Occurrence of Graft Failure or Death by Neighborhood-Level SES.
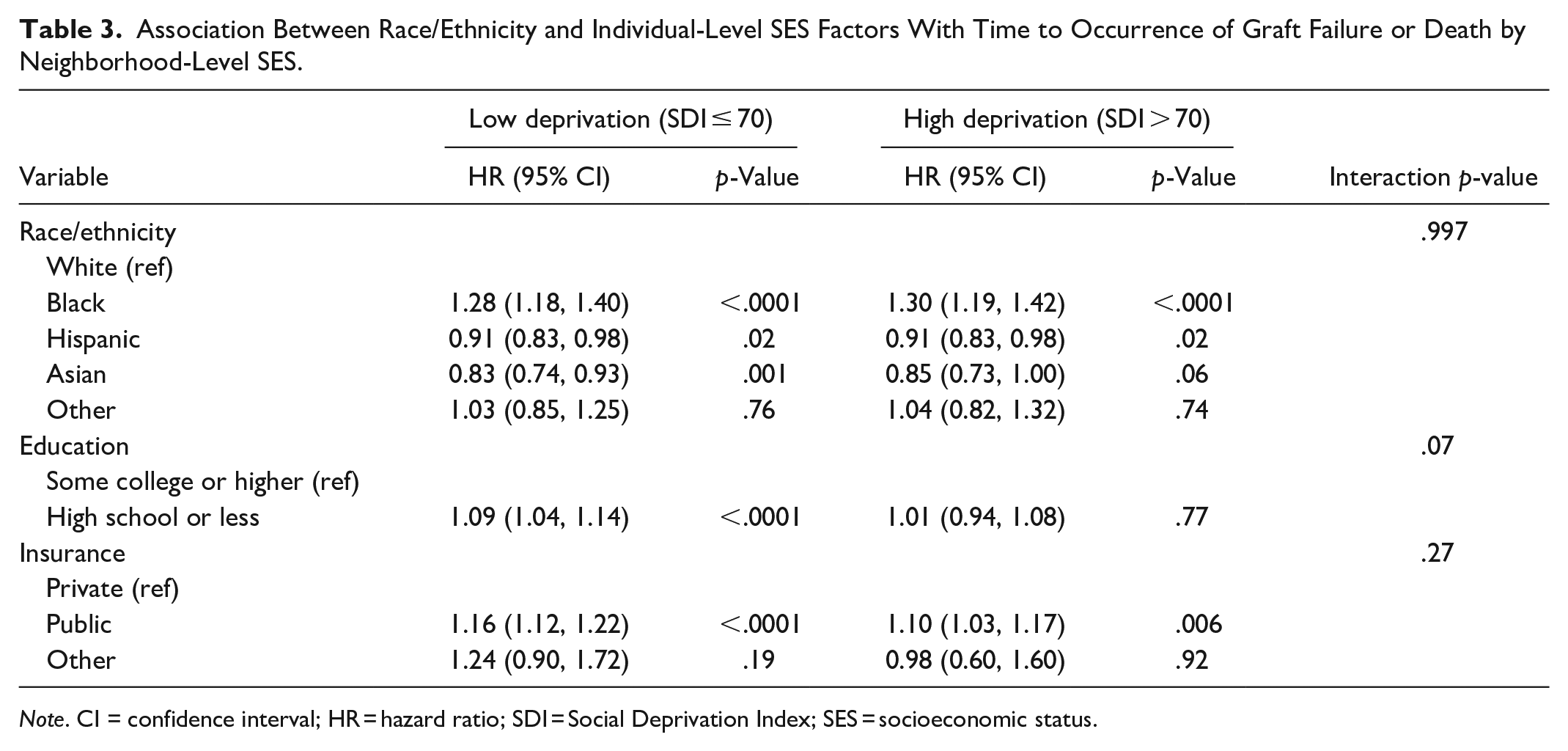
Note. CI = confidence interval; HR = hazard ratio; SDI = Social Deprivation Index; SES = socioeconomic status.
Association Between Race/Ethnicity and SES Factors With Time to Occurrence of Graft Failure or Death by Rural/Urban Geographic Region.
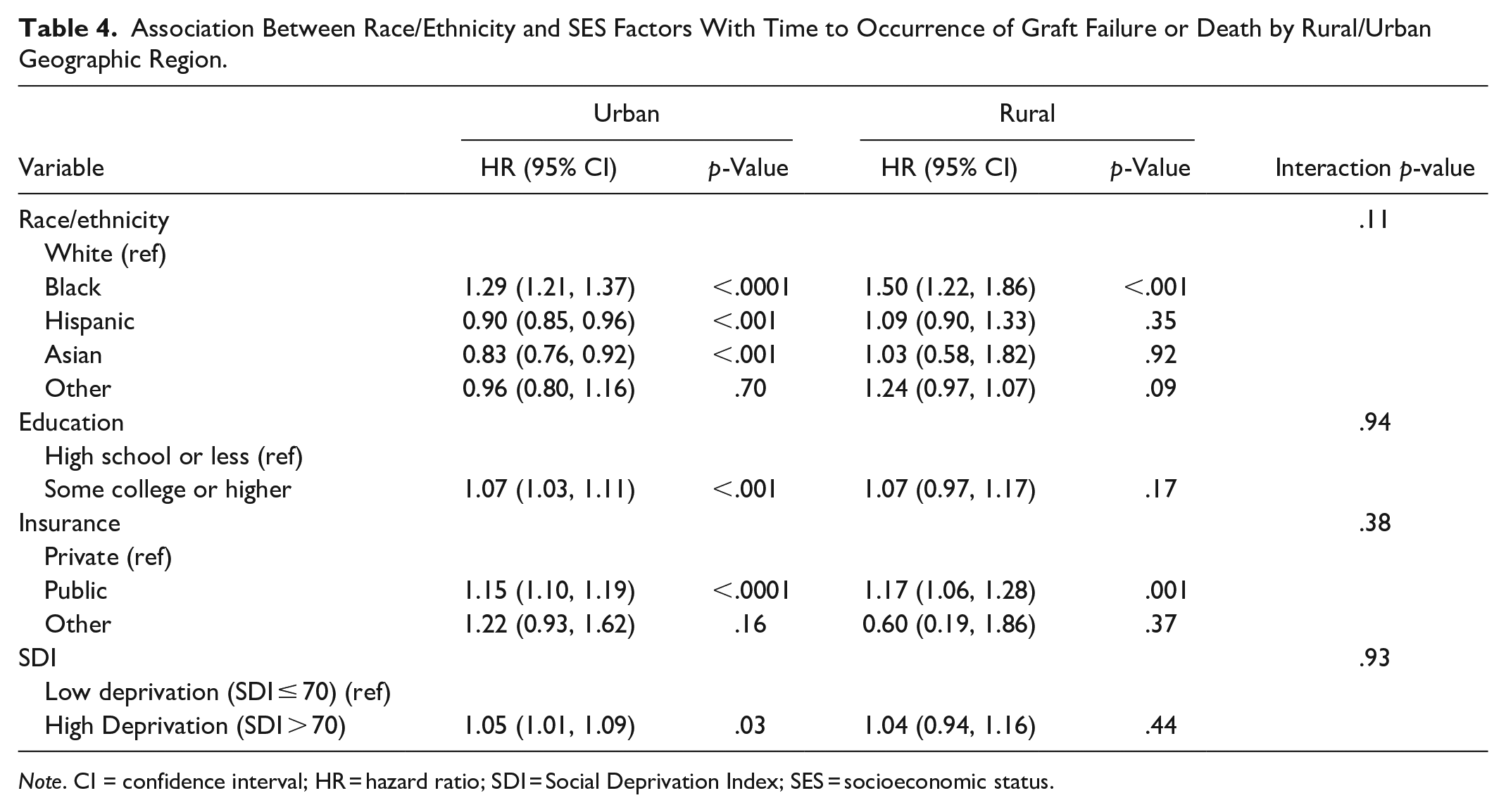
Note. CI = confidence interval; HR = hazard ratio; SDI = Social Deprivation Index; SES = socioeconomic status.
Discussion
This study found that LT recipients’ race/ethnicity, level of education, and insurance type were significantly associated with the transplant outcomes of graft failure or mortality. On the other hand, neighborhood-level SES was significantly associated with the transplant outcomes on its own, but this relationship became non-significant after adjustment for race/ethnicity and individual-level SES factors. Neighborhood-level SES did not modify the relationship between LT recipients’ race/ethnicity, level of education, insurance type, and transplant outcomes. Finally, the effect of neighborhood-level SES was not significantly different by urban and rural geographical regions.
Our findings were consistent with the previous literature that an individual’s race/ethnicity and SES levels contribute to health disparities in the LT population. Black recipients, compared to White recipients, were at higher risk of poor transplant outcomes (Cohen et al., 2007; Nair et al., 2002; Neff et al., 2007). LT recipients with high school education or less experienced a higher incidence of graft failure or mortality when compared to those with college or higher education levels (Goldfarb-Rumyantzev et al., 2006; Gruttadauria et al., 2011; Yoo & Thuluvath, 2004). Suboptimal transplant outcomes were more prevalent among LT recipients with public insurance compared to those with private insurance (Allen et al., 2011; Goldfarb-Rumyantzev et al., 2006; Yoo & Thuluvath, 2004). In addition, our sensitivity analysis revealed that Black and Asian living donor LT recipients were more than twice as likely to experience poor transplant outcomes compared to White recipients, which is much greater than what we observed among deceased donor LT recipients. This could be associated with disparities in receiving living donor LT. They are more likely to receive LT at advanced stages of liver disease than others due to late referrals and challenges in finding suitable donors (Mathur et al., 2010; Nobel et al., 2015; Park et al., 2022). These findings underscore the importance of further research to address and understand the disparities within these specific populations.
Our findings highlighted that, although neighborhood-level SES was linked to transplant outcomes, consistent with existing evidence (Niazi et al., 2021; Quillin et al., 2014; Ross et al., 2017), it did not modify the effects of race/ethnicity and individual-level SES on transplant outcomes. These findings suggest that the predominant determinants appear to be race/ethnicity and individual-level SES. Structural, institutional, and internalized racism may explain these findings (Purnell et al., 2021). Recipients from racial/ethnic minorities may have limited access to high-quality education throughout their lives, impacting their income and employment opportunities (Serper et al., 2018). They may also encounter challenges in accessing high-quality post-LT care and coordinating specialty care, compounded by a reluctance to seek help to overcome these barriers (Arriola, 2017; Keeling et al., 2022). In addition, the chronic stress related to experiences of racism throughout their lives may negatively affect their allostatic load, increasing the risks for adverse health outcomes (Geronimus et al., 2006). The characteristics of post-LT care may also explain these findings. Achieving optimal transplant outcomes requires active engagement from LT recipients in complex health tasks, including regular follow-up visits with the interdisciplinary transplant team, taking immunosuppressants as prescribed, and routine screenings to prevent potential complications like malignancy. Recipients with lower individual-level SES may encounter challenges in adhering to these tasks due to constraints in health literacy, limited social support, and financial burdens.
It is pertinent to consider whether the SDI adequately captured the neighborhood environment. Although it is a composite measure of seven sociodemographic characteristics, encompassing income, education, employment, housing, and household characteristics, it does not include other determinants, such as access to care or health behaviors within the community (Remington et al., 2015). The SDI utilized in this study was at the ZCTA level. However, ZCTAs may encompass neighborhoods with diverse socioeconomic profiles compared to smaller geographical levels such as census tracts (Krieger et al., 2002). Further investigation is needed to explore whether deprivation indices at different geographical levels (e.g., block group, census tract, ZCTA) yield varying results and to identify the most suitable measure for accurately capturing neighborhood environments in this particular population.
The predominant impact of individual-level SES on transplant outcomes remains consistent across urban and rural geographical regions. Residing in urban areas, particularly in advantaged neighborhoods, may offer health benefits, including a healthy environment and proximity to healthcare facilities. However, our study found that certain groups, such as Black recipients or those with lower education and public insurance, may not fully benefit from these resources (Onder et al., 2020). This study did not address other geographic factors, such as the distance to a transplant center, which have been shown to potentially contribute to transplant outcomes (Kelly et al., 2016; Whelan et al., 2021). Future research may consider addressing the influence of these factors in relation to disparities in transplant outcomes.
While this study benefits from utilizing large national longitudinal data, there are some limitations related to data availability. The use of education and insurance as proxies for individual-level SES may not capture the full SES spectrum. We used ZIP codes to define SDI at the ZCTA level, which may not precisely capture the sociodemographic characteristics of the immediate neighborhood where LT recipients reside. As SDI was derived from LT recipients’ ZIP codes at the time of transplant, it may not accurately reflect their current neighborhood if recipients relocated after LT. Lastly, the data did not include certain potential variables, such as genetics, that could be associated with transplant outcomes.
In conclusion, we found a significant impact of race/ethnicity and individual-level SES on transplant outcomes, irrespective of neighborhood factors. Interdisciplinary transplant teams should tailor post-LT care to address the unique needs of LT recipients from minority backgrounds with low individual-level SES. Future studies are needed to better understand their experiences and challenges to optimize transplant outcomes, and ultimately to inform the development of targeted and tailored strategies aimed at mitigating existing health disparities.
Supplemental Material
sj-docx-1-cnr-10.1177_10547738241273128 – Supplemental material for Disparities in Liver Transplant Outcomes: Race/Ethnicity and Individual- and Neighborhood-Level Socioeconomic Status
Supplemental material, sj-docx-1-cnr-10.1177_10547738241273128 for Disparities in Liver Transplant Outcomes: Race/Ethnicity and Individual- and Neighborhood-Level Socioeconomic Status by Niharika Gummaraj Srinivas, Ye Chen, Angie Mae Rodday and Dami Ko in Clinical Nursing Research
Footnotes
Acknowledgements
The data reported here have been supplied by UNOS as the contractor for the Organ Procurement and Transplantation Network (OPTN). The interpretation and reporting of these data are the responsibility of the author(s) and in no way should be seen as an official policy of or interpretation by the OPTN or the U.S. Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Institute of Health Equity and Social Justice Research (IHESJR) at Northeastern University to DK.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.