
Abstract
Acupuncture and moxibustion have been accepted as add-on options for primary dysmenorrhea (PD); however, the clinical evidence is still inadequate. We searched AMED, CENTRAL, EMBASE, PubMed, Web of Science, CBM, CNKI, VIP, Wangfang database, ANZCTR, ClinicalTrials.gov, and the WHO ICTRP, from their inception to February 2021. The pooled analysis of 13 RCTs with 675 participants for VAS showed that acupuncture and moxibustion were more effective in managing PD than the control group with the MD of −1.93 (95% CI [−2.80, −1.06] and −2.67 (95% CI [−4.96, −0.38]). With the CMSS, seven studies with 487 participants showed that these modalities were more effective than the control group with the MD of −7.58 (95% CI [−10.97, −4.19]) and −3.78 (95% CI [−6.90, −0.66]). The findings indicated that acupuncture and moxibustion could relieve pain effectively and has fewer adverse events (AEs) in managing PD.
Introduction
Primary dysmenorrhea (PD), known as period pain, is defined as painful menstruation in the absence of pelvic pathology (Kho et al., 2019). The recurrent, crampy, lower abdominal pain during menstruation are the common characters with associated symptoms of nausea, vomiting, diarrhea, headaches, dizziness, muscle cramps, back pain, and poor sleep quality (Kannan & Claydon, 2014; Kho et al., 2019). Globally, PD affects 50% to 90% of women irrespective of nationality or age (Committee on Adolescent Health Care, 2018). Half of these women describe the pain as moderate to severe, restricts their work and daily activities (Committee on Adolescent Health Care, 2018), and have adverse events (AEs) on mood resulting in anxiety and depression; this, in turn, impacts their experience of pain, pain expression, pain behaviors, and coping responses (Bernardi et al., 2017; Gagua, 2013).
Despite the importance of this subject, clinical PD management options are still inadequate. At present, nonsteroidal anti-inflammatory drugs (NSAIDs) are the first-line treatment for PD (Ferries-Rowe et al., 2020; Proctor & Farquhar, 2006). While side effects are commonly reported with NSAIDs, such as indigestion, headaches, and drowsiness, the therapeutic superiority of any individual NSAID on PD management has not been demonstrated (Marjoribanks et al., 2015); moreover, 18% of women with dysmenorrhea are unresponsive to such treatment (Oladosu et al., 2018). As reported, many young women tend to use self-care methods, but they may not necessarily choose the most effective options for PD (Armour et al., 2019). Therefore, finding an effective non-pharmacological method for PD management has a significant potential value and is urgently needed.
As important modalities of Traditional Chinese Medicine (TCM), acupuncture and moxibustion are recommended as safe options with fewer AEs and have been widely used to alleviate pain (Lee et al., 2010; Shen et al., 2019; Zhao, 2008). Previous publications reported that acupuncture and moxibustion treatments are effective for PD (Cho & Hwang, 2010; Gou et al., 2016); however, recent studies have shown that the reporting and methodological quality are suboptimal, limiting their results’ conviction (Yang et al., 2020; Zhang et al., 2018). Thus, this review aims to provide updated knowledge by synthesizing the best available evidence for PD.
Methods
Data Sources and Search Strategy
We searched five English databases and four Chinese databases that including Allied and Complementary Medicine Database (AMED), Cochrane Central Register of Controlled Trials (CENTRAL), Excerpta Medica database (EMBASE), PubMed, and Web of Science; Chinese Biological Medicine Database (CBM), China National Knowledge Infrastructure (CNKI), Chinese Technical Periodicals (VIP), and Wangfang database. To avoid publication bias, we also searched the Australian New Zealand Clinical Trials Registry (ANZCTR), ClinicalTrials.gov, and the World Health Organization International Clinical Trials Registry Platform (WHO ICTRP). The above searches are limited to English and Chinese from inception to February 2021. We contacted authors to identify additional information with missing or incomplete data.
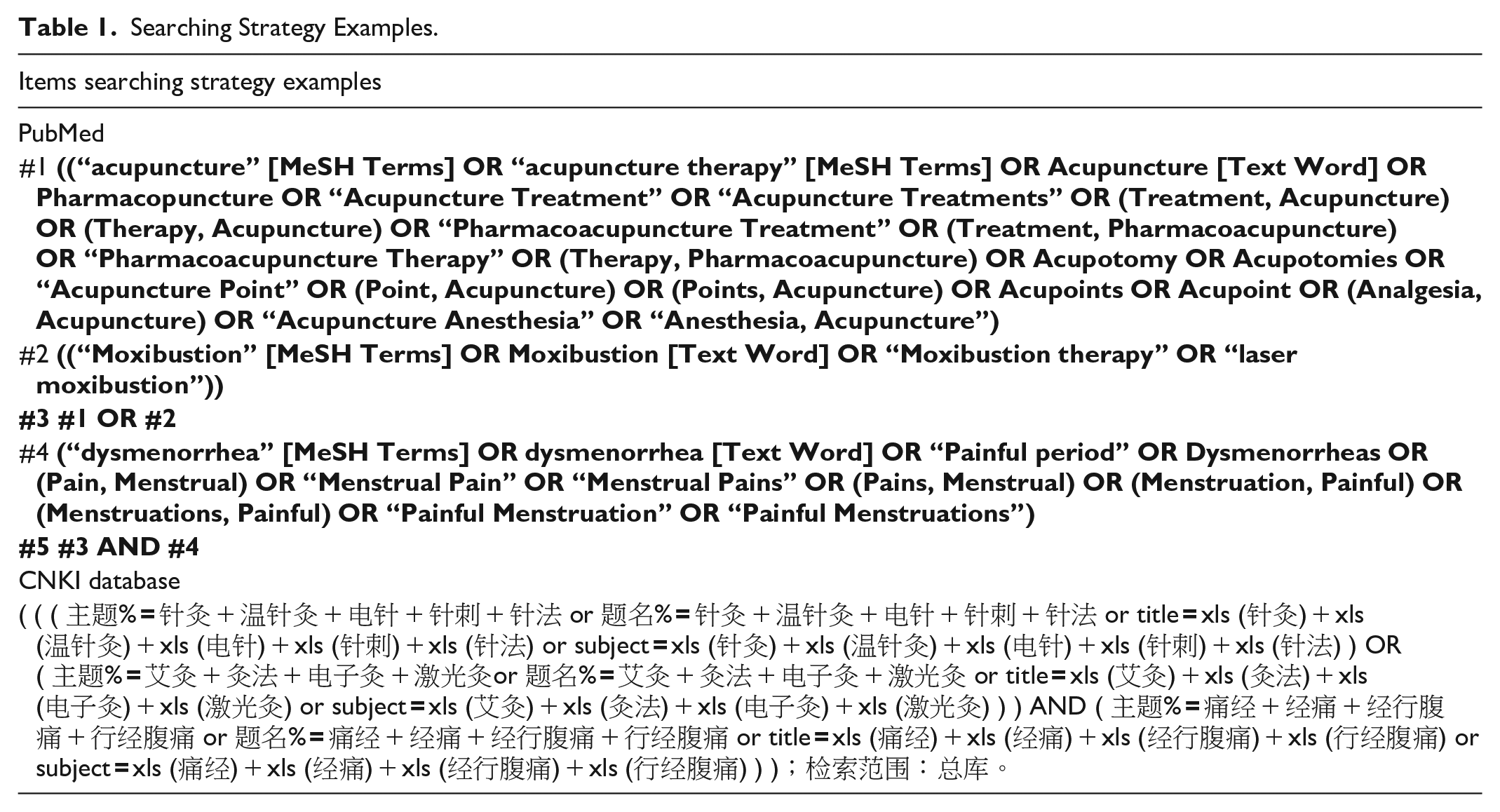
The search strategies were developed through a combination of Mesh terms and keywords: acupuncture, acupuncture therapy, acupuncture treatment, acupuncture point, moxibustion, moxibustion therapy, moxa, laser moxibustion, dysmenorrhea, primary dysmenorrhea, painful period, algomenorrhea, and menstrual pain. The search strategy was adapted to different databases demands, and some examples are shown in Table 1.
Searching Strategy Examples.
Inclusion and Exclusion Criteria
Participants
Women aged 18 to 40 years with a clinically diagnosed PD were included. Western medicine diagnosis criteria were based on recurrent, crampy, and lower abdominal pain during menstruation in the absence of pelvic pathology (Kho et al., 2019). The TCM diagnosis was based on TCM syndrome differentiation, for example, Qi and Blood stagnation; Cold and Dampness stasis. Animal studies, secondary dysmenorrhea, women aged outside of the 18 to 40 age bracket were excluded.
Intervention(s)
All types of acupuncture (manual, electro, or laser) and or moxibustion (direct, indirect, electronic, or laser) were included. Wrist-ankle needle, auricular acupuncture, scalp acupuncture, fire needle, acupoint catgut embedding, acupoint injection, and other non-traditional therapies were excluded.
Comparator
Control treatments included were no treatment, sham group (sham acupuncture or moxibustion), or usual care.
Outcomes
(a) The efficacy of acupuncture and or moxibustion for PD measured by validated tools. (b) The treatment regimen (acupoints formula and intervention dosage). (c) Safety of acupuncture and moxibustion as measured by any reported AEs.
Study type
Randomized controlled trials (RCTs) were included.
Study Selection and Data Extraction
Two reviewers (WL and CW) screened the titles and abstracts of all the retrieved studies by removing duplicates and excluding all irrelevant studies. Only those studies with full text were retrieved for further screening. WL checked all the eligible studies, and discussions with CW, XM, and TK solved any disagreements.
The data extraction was conducted by WL and CW and validated by KL. The extraction content includes characteristics of included studies (authors, year of publication, and study setting); participant (age, sample size, and diagnostic criteria); intervention regime (acupuncture and moxibustion types, acupoints formula, treatment dosage, and control group types); outcomes measurement tools used; and AEs. Where necessary, we contacted authors for further information concerning the exact logistics of the randomization process.
Quality Assessment and Data Synthesis
All included studies were independently evaluated and cross-checked for methodological quality using the Cochrane risk of bias tool (Higgins et al., 2011) by two reviewers (WL and CW), and disagreements were resolved by discussion and consensus with another reviewer (KL). The evaluation items included “random allocation,” “allocation concealment,” “blinding of participants and personnel,” “blinding of outcome assessment,” “complete outcome data,” “selective outcome reporting,” and “other bias.” The items were evaluated for “high risk,” “unclear risk,” or “low risk.”
The data were summarized using the weighted mean difference (MD) with 95% confidence intervals (CI) for continuous outcomes. The test of statistical homogeneity of effects across studies was performed using the χ2 distributed Cochrane Q test, with p ≤ .10 indicating significance, and formally quantified by I2 statistic, with a value less than 25% indicating low, 25% to 50% indicating moderate, and greater than 50% indicating high heterogeneity. The random-effect model was applied to the heterogeneity studies. Causes of heterogeneity were then examined by subgroup analysis and sensitivity analysis. Potential publication bias was explored by funnel plot, Egger’s (Egger et al., 2009) test and Begg’s test (Begg & Mazumdar, 1994). All analyses were conducted using Meta-Analysis Packages in R (Balduzzi et al., 2019).
Results
Study Selection
The PRISMA flow chart of study selection is shown in Figure 1. After a vigorous study selection process, 73 studies were eligible among 9,761 identified studies from 12 electronic databases and clinical trials registry platforms. We evaluated the quality of these 73 studies according to the Cochrane risk of bias assessment. Results showed that 51 studies had a “low risk of bias” in less than five domains, which was considered low quality and therefore excluded. Subsequently, 22 studies were finally obtained for analysis (Figure 2).
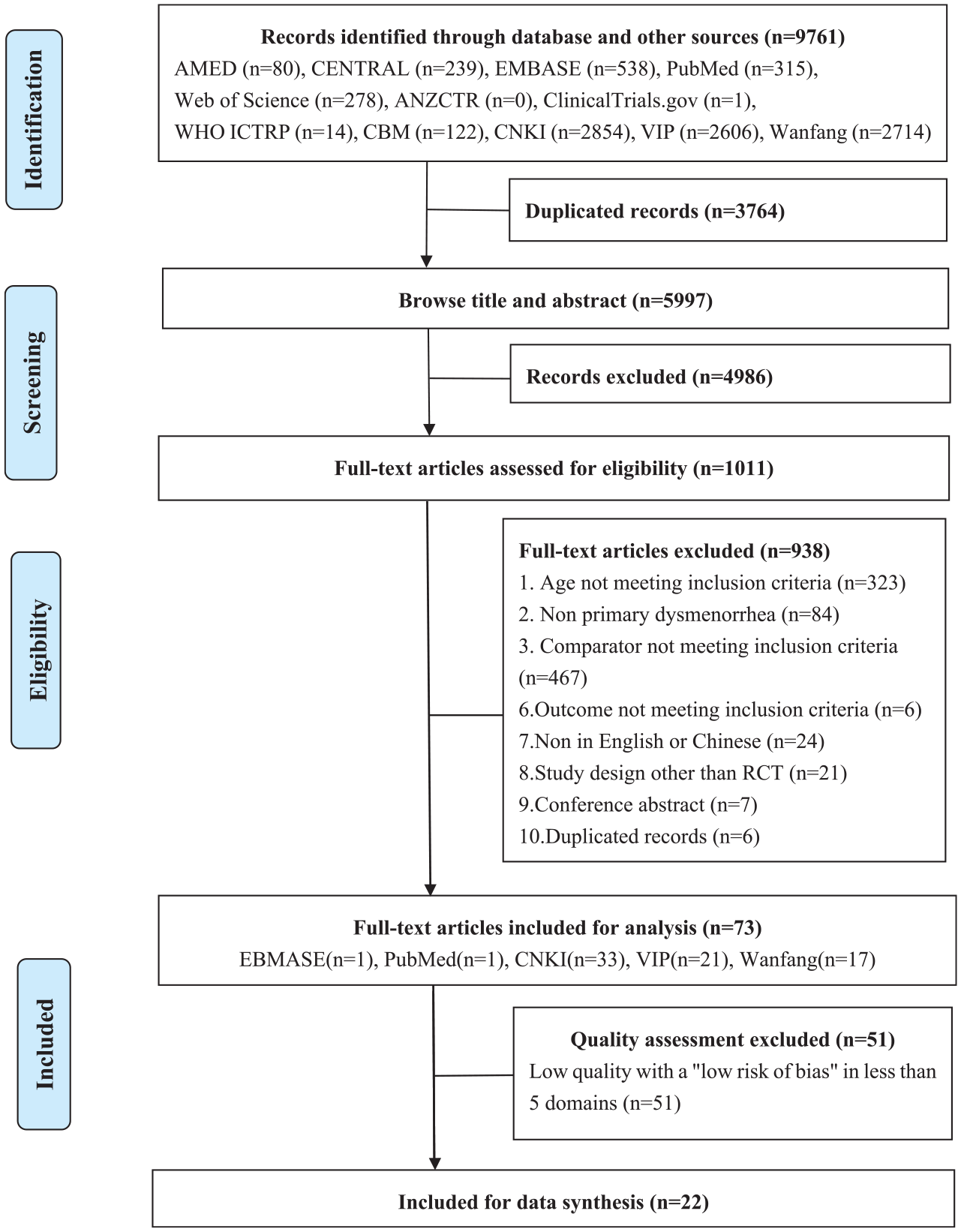
Flowchart of literature selection on randomized controlled trials of acupuncture and or moxibustion for managing PD.
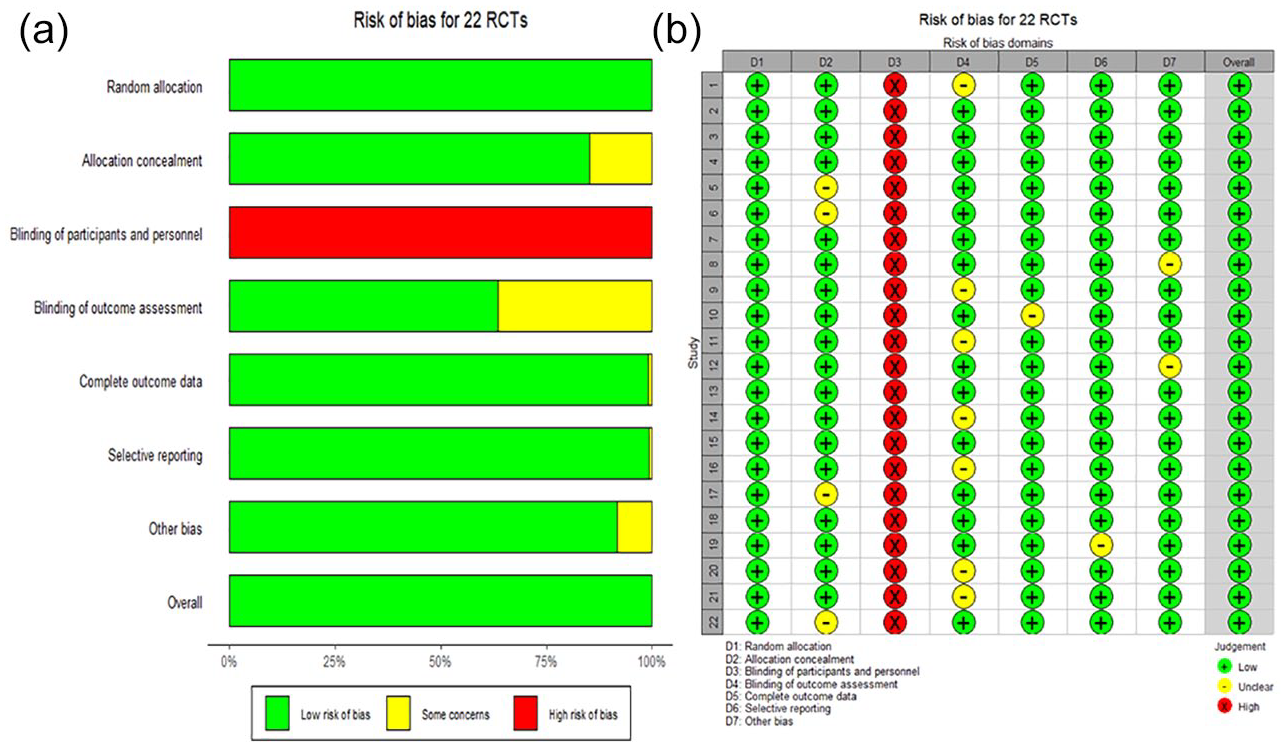
(a) Risk of bias graph and (b) risk of bias summary.
Characteristics of the Included Studies
Table 2 summarizes the 22 studies included in this review, and these studies comprised of 1,634 randomized PD participants, with 4 studies (Sriprasert et al., 2015; Liu et al., 2020; Wang et al., 2019; Yang et al., 2017) published in English and 18 studies published in Chinese. The included trials were mainly conducted in China (n = 21) and Thailand (n = 1). There were 17 studies (Cai, 2012; Chen, 2013; Han et al., 2015; Jiang et al., 2020; Li, 2014; Lin, 2020; Liu, 2008; Luo, 2015; Peng, 2019; Tian, 2020; Wang, 2008, 2016; Wang et al., 2019; Yang et al., 2017; Zhang, 2017, 2019; Zhu, 2015) that measured pain with visual analogue scale (VAS), with no less than 4 cm as their inclusion criteria, while the other 5 (Bu et al., 2011; Deng, 2019; Li, 2012; Liu et al., 2020; Sriprasert et al., 2015) did not report the details of such inclusion criteria. The average participants age in these RCTs was 19 to 27 years.
Characteristic of Included Randomized Controlled Trials on Acupuncture and or Moxibustion for Managing Primary Dysmenorrhea (PD).
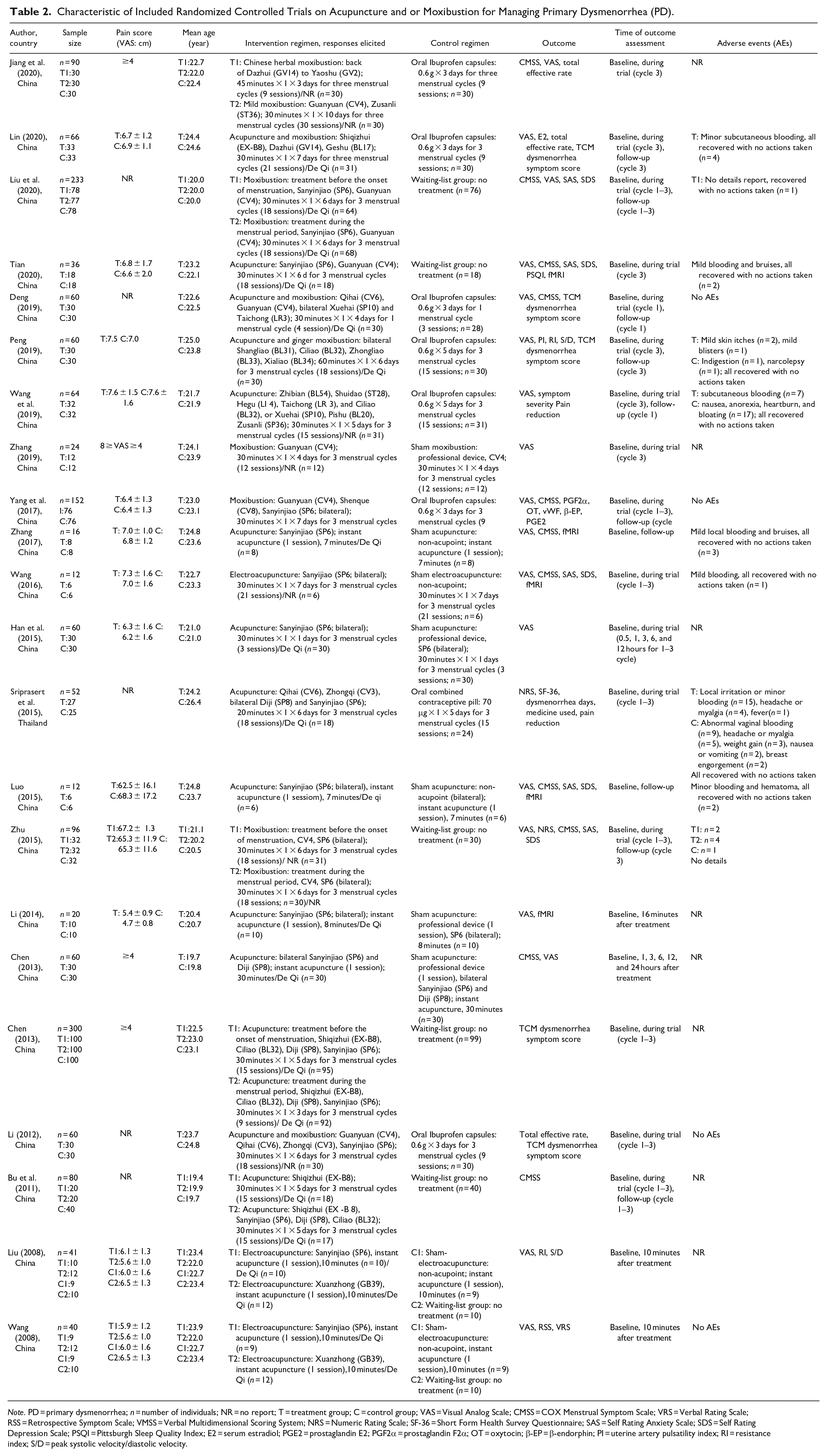
Note. PD = primary dysmenorrhea; n = number of individuals; NR = no report; T = treatment group; C = control group; VAS = Visual Analog Scale; CMSS = COX Menstrual Symptom Scale; VRS = Verbal Rating Scale; RSS = Retrospective Symptom Scale; VMSS = Verbal Multidimensional Scoring System; NRS = Numeric Rating Scale; SF-36 = Short Form Health Survey Questionnaire; SAS = Self Rating Anxiety Scale; SDS = Self Rating Depression Scale; PSQI = Pittsburgh Sleep Quality Index; E2 = serum estradiol; PGE2 = prostaglandin E2; PGF2α = prostaglandin F2α; OT = oxytocin; β-EP = β-endorphin; PI = uterine artery pulsatility index; RI = resistance index; S/D = peak systolic velocity/diastolic velocity.
For the intervention group, there were 13 studies on acupuncture (Bu et al., 2011; Cai, 2012; Chen, 2013; Han et al., 2015; Li, 2014; Liu, 2008; Luo, 2015; Sriprasert et al., 2015; Tian, 2020; Wang, 2008, 2016; Wang et al., 2019; Zhang, 2017), 5 on moxibustion (Jiang et al., 2020; Liu et al., 2020; Yang et al., 2017; Zhang, 2019; Zhu, 2015), and 4 on the combination of both acupuncture and moxibustion (Deng, 2019; Li, 2012; Lin, 2020; Peng, 2019). Besides, there were 15 studies (Chen, 2013; Deng, 2019; Han et al., 2015; Li, 2012, 2014; Lin, 2020; Luo, 2015; Peng, 2019; Sriprasert et al., 2015; Tian, 2020; Wang, 2016; Wang et al., 2019; Yang et al., 2017; Zhang, 2017, 2019) with a single intervention group, and 7 (Bu et al., 2011; Cai, 2012; Jiang et al., 2020; Liu, 2008; Liu et al., 2020; Wang, 2008; Zhu, 2015) included two intervention groups. The details of “De Qi”(tingling, numbness, heaviness, and other feelings) after acupuncture and or moxibustion applied were reported in 16 included studies (Bu et al., 2011; Cai, 2012; Chen, 2013; Deng, 2019; Han et al., 2015; Li, 2014; Lin, 2020; Liu, 2008; Liu et al., 2020; Luo, 2015; Peng, 2019; Sriprasert et al., 2015; Tian, 2020; Wang, 2008; Yang et al., 2017; Zhang, 2017), but failed to report in the other 6 (Jiang et al., 2020; Li, 2012; Wang, 2016; Wang et al., 2019; Zhang, 2019; Zhu, 2015). For the control group, there were five studies on no-treatment (Bu et al., 2011; Cai, 2012; Liu et al., 2020; Tian, 2020; Zhu, 2015), seven on sham (Chen, 2013; Han et al., 2015; Li, 2014; Luo, 2015; Wang, 2016; Zhang, 2017, 2019), eight on oral pills (seven Ibuprofen capsules and one combined contraceptive pill; Deng, 2019; Jiang et al., 2020; Li, 2012; Lin, 2020; Peng, 2019; Sriprasert et al., 2015; Wang et al., 2019; Yang et al., 2017), and two with two options (no-treatment and sham-group; Liu, 2008; Wang, 2008). The outcomes of included studies were presented in different ways, including pain intensity assessment scale, symptom assessment, efficacy index, mental-related factors, and lab tests. There were 18 studies (Chen, 2013; Deng, 2019; Han et al., 2015; Jiang et al., 2020; Li, 2014; Lin, 2020; Liu, 2008; Liu et al., 2020; Luo, 2015; Peng, 2019; Tian, 2020; Wang, 2008, 2016; Wang et al., 2019; Yang et al., 2017; Zhang, 2017, 2019; Zhu, 2015) using the VAS, although three of them were not included, therefore, failed data synthesis in our meta-analysis due to missing information. Ten studies (Bu et al., 2011; Chen, 2013; Deng, 2019; Jiang et al., 2020; Liu et al., 2020; Luo, 2015; Tian, 2020; Wang, 2016; Yang et al., 2017; Zhu, 2015) using the COX menstrual symptom scale (CMSS), however, two of them were not included in our meta-analysis due to missing information. Five studies using TCM dysmorphia symptom score (Cai, 2012; Deng, 2019; Li, 2012; Lin, 2020; Peng, 2019), four studies using Self rating Anxiety Scale (SAS) and Self rating Depression Scale (SDS; Liu et al., 2020; Tian, 2020; Wang, 2016; Zhu, 2015). Nine studies reported AEs (Lin, 2020; Liu et al., 2020; Luo, 2015; Peng, 2019; Sriprasert et al., 2015; Tian, 2020; Wang, 2016; Wang et al., 2019; Zhang, 2017), but these events were mild and all recovered without taking further actions. One study reported events without specific description (Zhu, 2015), four studies suggested these modalities were safe without any AEs (Deng, 2019; Li, 2012; Yang et al., 2017; Wang, 2008), and eight studies did not report AEs related information (Bu et al., 2011; Cai, 2012; Chen, 2013; Han et al., 2015; Jiang et al., 2020; Li, 2014; Liu, 2008; Zhang, 2019).
Quality Assessment
A summary of the risks of bias in included studies is presented in Figure 2. Twenty-two studies were at low risk of selection bias related to the random sequence generation. Four studies did not describe allocation concealment and were at unclear risk of this bias (Bu et al., 2011; Chen, 2013; Jiang et al., 2020; Wang, 2016). However, selection bias did not appear to be an issue in these trials because of the similar baseline among groups. Due to the nature of acupuncture studies, absolute double-blinding was often not possible. Twenty-two trials were at high risk of bias in this category. Among these trials, seven trials reported to having an unclear risk of blinding of outcome assessment (Deng, 2019; Cai, 2012; Li, 2012; Peng, 2019; Sriprasert et al., 2015; Wang, 2008; Zhang, 2019). The complete outcome data and selective reporting were not described clearly for two trials (Luo, 2015; Zhang, 2017), whereas the other two trials were at unclear risk of such bias (Liu, 2008; Zhu, 2015). However, the overall risk of bias for all included studies remained low (Figure 2).
Efficacy of Acupuncture or Moxibustion
VAS
Of the trials that measured pain with the VAS, 13 studies could be pooled for meta-analysis with acupuncture or moxibustion; however, 2 studies with acupuncture plus moxibustion were excluded due to insufficient studies. In subgroup analyses, groups that received acupuncture or moxibustion were effectively managed PD compared with the control group with a MD of −1.93 (95% CI [−2.80, −1.06]) and −2.67 (95% CI [−4.96, −0.38]), respectively. There was statistical heterogeneity for PD outcomes on acupuncture group (p < 0.1, I2 = 86%) and moxibustion group (p < 0.1, I² = 98%). Therefore, we conducted a sensitivity analysis. Sensitivity analysis was performed by removing the studies one by one; the result showed that the pooled effect size was still statistically significant, and the forest plot direction did not change significantly before and after removal. Thus, the high heterogeneity might not be caused by every single study (Figure 3a and b).
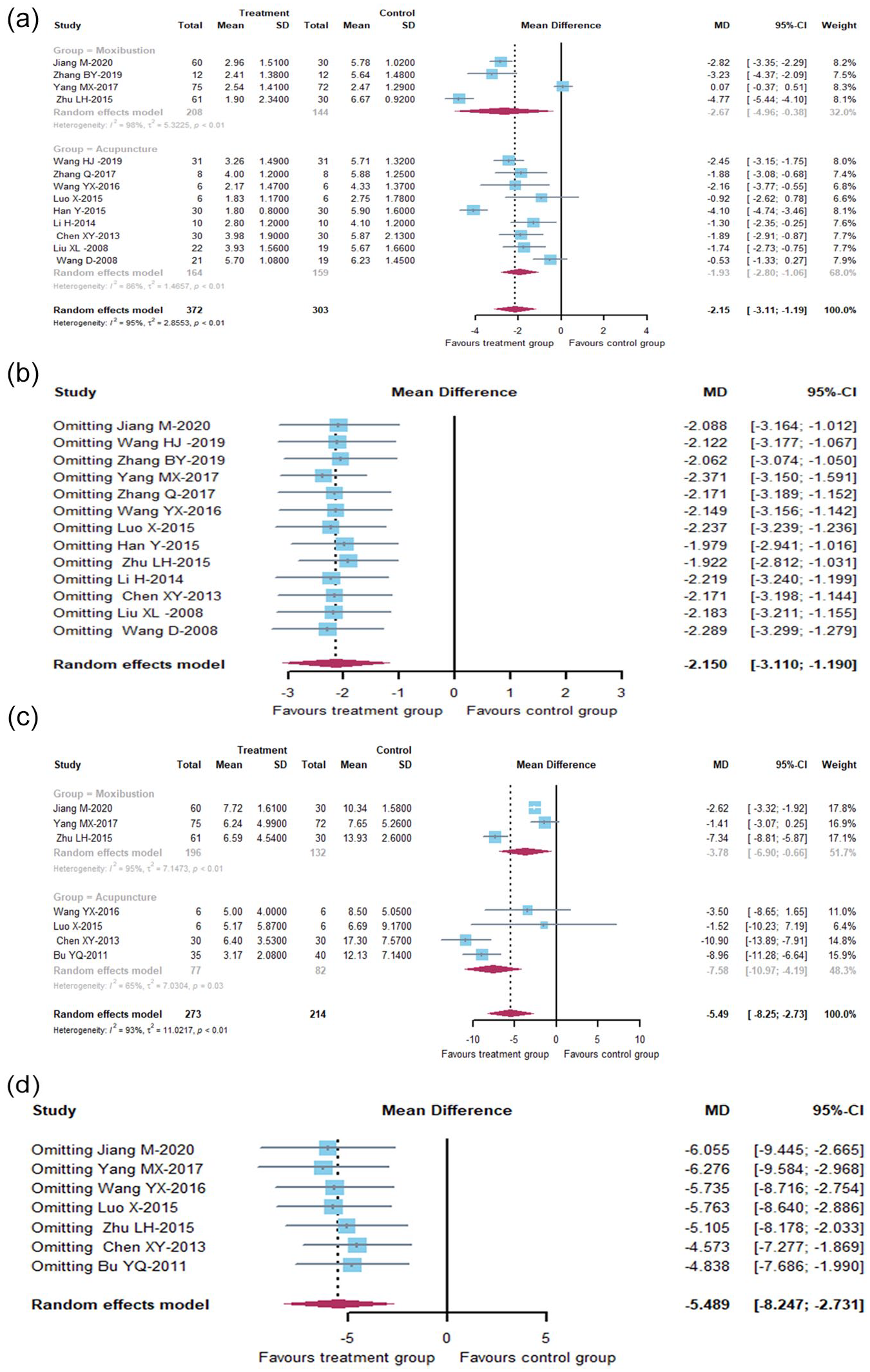
(a) Forest plots of comparison: effect of treatments versus controls on VAS, two treatment groups were grouped separately for relevant subgroup analysis, (b) sensitivity analysis: effect of treatments versus controls on VAS, every study was omitted separately for MD changes, (c) forest plots of comparison: effect of treatments versus controls on CMSS, two treatment groups were grouped separately for relevant subgroup analysis, and (d) sensitivity analysis: effect of treatments versus controls on CMSS, every study was omitted separately for MD changes.
CMSS
Of the trials that measured pain with the CMSS, seven studies could be pooled for meta-analysis with acupuncture or moxibustion; however, one study with acupuncture plus moxibustion were excluded due to the small sample. In subgroup analyses, groups that received acupuncture or moxibustion were effectively managed PD compared with the control group with a MD of −7.58 (95% CI [−10.97, −4.19]) and −3.78 (95% CI [−6.90, −0.66]), respectively. There was statistical heterogeneity for PD outcomes on acupuncture group (p < 0.1, I2 = 65%) and moxibustion group (p < 0.1, I2 = 95%). Therefore, we conducted a sensitivity analysis. Sensitivity analysis was performed by removing the studies one by one; the result showed that the pooled effect size was still statistically significant, and the forest plot direction did not change significantly before and after removal. Thus, the high heterogeneity might not be caused by every single study (Figure 3c and d).
Descriptive Analysis of Other Outcomes
Some included studies could not be subjected to meta-analysis due to the significant variations in acupuncture and moxibustion intervention regimes and outcome measurement instruments. We have tried to synthesize these results, but not satisfactory. Thus, this review narratively reported results from these included trials.
TCM Dysmenorrhea Symptom Score
Five of the included trials reported TCM dysmenorrhea symptom score, with three cold congelation and Blood stasis types (Li, 2012; Lin, 2020; Peng, 2019), one study with Qi stagnation and Blood stasis type (Deng, 2019), and one is a combination of them (Cai, 2012). Four studies reported a significant difference between groups in TCM scores after treatment (p < .05; Cai, 2012; Deng, 2019; Li, 2012; Peng, 2019), but Lin (2020) reported that when compared with the control group, the difference of treatment group did not reach statistical significance.
Total Effective Rate
The total effective rate was defined as the proportion of participants with symptom severity score reduction after treatment, including four grades of “cure,” “remarkable effect,” “improvement,” and “failure.” Three studies (Jiang et al., 2020; Li, 2012; Lin, 2020) reported that the total effective rate in the treatment group was significantly higher than the control group (p < .05).
SAS and SDS
Four studies used the SAS and SDS at the same time (Liu et al., 2020; Tian, 2020; Wang, 2016; Zhu, 2015). Only one of them showed a significant difference between-group after treatment (p < .01; Zhu, 2015), suggesting that acupuncture plays an important role in emotion regulation. Conversely, three studies showed that there was no significant difference between the intervention and control group (p > .05; Liu et al., 2020; Tian, 2020; Wang, 2016), meaning it may not affect improving the anxiety and depression of PD participants.
Treatment Regimen
All the 22 RCTs reported the specifically applied acupoints in their treatment. The six most common used acupoints for managing PD were Sanyinjiao (SP6), Guanyuan (CV4), Ciliao (BL32), Diji (SP8), Qihai (CV6), and Dazhui (GV14). Results also revealed that most of the acupoints used in the included trials were located on the back (e.g., Geshu (BL17), and Yaoshu (GV2)), with some being located at the abdomen (e.g., Guanyuan (CV4), Qihai (CV6)), and Zhongji (CV3) and limbs (e.g., Sanyinjiao (SP6), Diji (SP8), and Zusanli (ST36)).
In this review, 13 studies (Bu et al., 2011; Cai, 2012; Deng, 2019; Jiang et al., 2020; Li, 2012; Lin, 2020; Liu et al., 2020; Peng, 2019; Tian, 2020; Wang, 2016; Wang et al., 2019; Yang et al., 2017; Zhu, 2015) reported that interventions were used once a day for managing PD, and the most common treatment frequencies were six times per week (n = 7), seven times per week (n =4), and five times per week (n = 4), which were consistent with the frequency of once a day above. Moreover, the most common duration of interventions was 30 minutes for each time, and studies also involved 20, 45, and 60 minutes. In addition, six studies (Bu et al., 2011; Cai, 2012; Chen, 2013; Li, 2012; Liu, 2008; Wang, 2008) reported that instant acupuncture and or moxibustion was used to observe the immediate analgesic effect. Nearly 70% of participants in this review received three continuous menstrual cycles treatment for their intervention doses.
Adverse Events (AEs)
AEs were mentioned in 14 trials (Deng, 2019; Li, 2012; Lin, 2020; Liu et al., 2020; Luo, 2015; Peng, 2019; Sriprasert et al., 2015; Tian, 2020; Wang, 2008, 2016; Wang et al., 2019; Yang et al., 2017; Zhang, 2017; Zhu, 2015). Among which, four studies reported acupuncture was safe with no AEs during the trials (Deng, 2019; Li, 2012; Wang, 2008; Yang et al., 2017), one study reported AEs without specific description (Zhu, 2015), nine studies reported specific AEs including local and minor irritation, bleeding, hematoma, bruises, blisters, and these reactions were mild and all recovered that did not affect the participants or the trial (Lin, 2020; Liu et al., 2020; Luo, 2015; Peng, 2019; Sriprasert et al., 2015; Tian, 2020; Wang, 2016; Wang et al., 2019; Zhang, 2017). Conversely, eight studies failed to report any AEs (Bu et al., 2011; Cai, 2012; Chen, 2013; Han et al., 2015; Jiang et al., 2020; Li, 2014; Liu, 2008; Zhang, 2019).
Analysis of Publication Bias
Funnel plot analysis showed that there were no significant publication biases for most analyses. Both Begg’s and Egger’s test results further supported the result of funnel plot analysis (p > .05).
Discussion
Meta-Analysis of Clinical Effect
Our meta-analysis revealed that acupuncture can significantly reduce the VAS, CMSS, and TCM symptom scores of PD participants. The total effect rates of the acupuncture group were significantly higher than the control group. Therefore, acupuncture could be viewed as an effective option for PD, which was consistent with the other report (Cho & Hwang, 2010). Moxibustion is a traditional therapeutic remedy that has been used to treat and prevent disease for more than thousands. Our review suggested that moxibustion can improve the pain symptoms of the participants, which were consistent with a previous study (Gou et al., 2016). Thus, current results showed that acupuncture and moxibustion could be used as complementary or alternative therapies for managing PD.
The result showed an association between acupuncture or moxibustion and reduced pain intensity, with a moderate level of certainty. However, as most studies used a subjective, self-reported index of treatment effects as the outcome measure, this resulted in the inaccurate pain assessment (Salé et al., 2010). Anxiety and depression might have a bidirectional association with dysmenorrhea. Experiencing monthly repeated menstrual pain might increase the risk of anxiety and depression, and psychological disorders exacerbate the severity of menstrual pain (Patel et al., 2006). Only four studies reported anxiety and depression as outcomes in this review, and there was no evidence that acupuncture and moxibustion improved anxiety and depression when managing PD. Therefore, more evidence is required on the associations between PD and mental health to inform holistic health.
In the meta-analysis of VAS and CMSS, the high heterogeneity is evident. One major challenge might be the subjective nature of the symptom presentations and the small sample size. Furthermore, the included studies used different interventions, including acupuncture, electroacupuncture, Chinese herbal moxibustion, and mild moxibustion. The control group included the waiting-list, sham group, Ibuprofen, and combined contractual pill. This might result in high heterogeneity and affect the level of the review. From a clinical perspective, available evidence suggests acupuncture or moxibustion could be a component of pain management. Nevertheless, high heterogeneity in the results suggests that the outcomes of these therapies may be varied. Therefore, we performed subgroup analysis and sensitivity analysis on the included studies, although the results were not significantly different.
Evidence of the Treatment Regimen
This review showed a detailed treatment regimen, including acupoints formula and intervention dosage, might provide a reference for managing PD in clinical practice. We found a set of frequently used points for PD: Sanyinjiao (SP6), Guanyuan (CV4), Ciliao (BL32), Diji (SP8), Qihai (CV6), and Dazhui (GV14), and this result coincided with the previous report (Hwang et al., 2020). These acupoints formula revealed that both local and distal acupoints were used to treat menstrual pain in clinical trials, suggesting that regional points are considered the basic rule of point selection based on the meridian system, and as well as points remote from the disease site also been chosen by the traditional acupuncture practitioners along the described meridian (Lee et al., 2013). A report preliminarily summarized frequently-used acupoints for pain relief and found that needle retention time was mostly 30 minutes (Liang et al., 2020). This idea was consistent with our review, more than half of the studies used a frequency of 30 minutes per time. Moreover, most participants received repeated once-daily treatment for three continuous menstrual cycles. However, the treatment regimen is a variable associated with specific musculoskeletal conditions, environment, and even the patient’s goals. Thus, there should be an ongoing discussion on referral more individual treatment protocols that meet requirements for clinical trials.
Summary of the Safety
Few AEs from the acupuncture or moxibustion groups were reported, which was in line with several previous reviews (Wang et al., 2019; Chan et al., 2017; Tan et al., 2014; Xu et al., 2013, 2014). Local and minor irritation, bleeding, hematoma, bruises, and blisters were the most common AEs identified in our review across all modalities (manual acupuncture, electroacupuncture, Chinese herbal moxibustion, and mild moxibustion), all were mild, and all recovered with no actions taken. Serious side effects were not reported. However, there is no absolutely safe treatment in the world; acupuncture and moxibustion remain associated with AEs and related to some serious risks in certain circumstances. The position, acupoints, duration, depth and angle of acupuncture, the distance between moxa and skin, proficiency of practitioners, patient’s conditions, and even the treatment environment can affect the safety of acupuncture moxibustion. The exact causes of most of these cannot be determined. Issues should be addressed in further experimental studies. In general, acupuncture is safe in the hands of competent practitioners (Vincent, 2001). Adequate supervision and professional training can even further minimize risks during the trials.
Strengths and Limitations
The strengths of this review are as follows: (1) unlike other reviews, this review did not include “RCT” as the search restriction and performed an inclusive search in major databases from their inception, and integrated more comprehensive information; (2) this review conducted the quality assessment with strict criteria to improve the overall quality of included studies, providing new evidence and opening new horizons for systematic review; (3) there was no publication bias in this review, which further improved the quality of evidence; (4) we added the topic of safety in the use of acupuncture and moxibustion, which is proven to be poorly reported in the existing literature.
This meta-analysis has several limitations: (1) this review was limited to Chinese and English research, leading to the possibility of selection bias; (2) in the generation of random sequence, some literature only mentioned the word “random,” but did not specify the random method, which might increase the risk of bias and reduce the quality of research; (3) many results could not be meta-analyzed due to the significant variations in treatment modalities and outcome measurement instruments; (4) some possible reasons for high heterogeneity: small sample size, different syndrome types of PD, nonblinding of participants and practitioners; we tried to reduce the heterogeneity by synthesizing the data separately depending on the characteristics of the interventions and controls, and subgroup analysis, but the unresolved heterogeneity still existed. All those results mentioned above should therefore be interpreted with caution. More rigorous trials are needed to identify the association of acupuncture and or moxibustion with PD and integrate such evidence into clinical care to improve health outcomes.
Conclusions
Based on available evidence, acupuncture and or moxibustion may be associated with significant reductions in PD by the appropriate treatment regimen. Generally, acupuncture and moxibustion are safe modalities and serious AEs after treatment are uncommon when supported with well-established guidelines, practiced among licensed, qualified practitioners.
Footnotes
Acknowledgements
We would like to express our sincere appreciation to the authors who performed all eligible studies included in the present study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the project on Edith Cowan University and Industry Collaboration Scholarship (G1004906).