
Abstract
Introduction:
This study aimed to synthesise the best available evidence on the safety and efficacy of using moxibustion and/or acupuncture to manage cancer-related insomnia (CRI).
Methods:
The PRISMA framework guided the review. Nine databases were searched from its inception to July 2020, published in English or Chinese. Randomised clinical trials (RCTs) of moxibustion and or acupuncture for the treatment of CRI were selected for inclusion. Methodological quality was assessed using the method suggested by the Cochrane collaboration. The Cochrane Review Manager was used to conduct a meta-analysis.
Results:
Fourteen RCTs met the eligibility criteria. Twelve RCTs used the Pittsburgh Sleep Quality Index (PSQI) score as continuous data and a meta-analysis showed positive effects of moxibustion and or acupuncture (n = 997, mean difference (MD) = −1.84, 95% confidence interval (CI) = −2.75 to −0.94, p < 0.01). Five RCTs using continuous data and a meta-analysis in these studies also showed significant difference between two groups (n = 358, risk ratio (RR) = 0.45, 95% CI = 0.26–0.80, I2 = 39%).
Conclusion:
The meta-analyses demonstrated that moxibustion and or acupuncture showed a positive effect in managing CRI. Such modalities could be considered an add-on option in the current CRI management regimen.
Systematic review registration number
CRD42019141785 https://www.crd.york.ac.uk/prospero/display_record.php?ID = CRD42019141785
What is already known about the topic?
Advancements in cancer diagnoses and treatments have improved the survival rate, and long-term survival has highlighted a challenge in the ongoing cancer symptoms management.
Trouble sleeping has been one of the most prominent cancer symptoms which impedes the functional status and quality of life of cancer patients and their families, reduces their compliance with conventional anticancer treatments, and contributes to the increase of their financial burden, and subsequently threatens their long-term survival.
Many cancer patients turn to complementary and alternative therapies such as acupuncture or moxibustion to manage their symptoms due to fear of side effects of drugs that can further exacerbate cancer symptoms.
What this paper adds?
We synthesised the best available evidence on the safety and efficacy of using moxibustion and/or acupuncture to manage cancer-related insomnia (CRI).
Moxibustion and/or acupuncture showed a positive effect in managing CRI, and such modalities could be considered as an add-on treatment in the current CRI management regimen.
High-quality, clinically driven, and full-powered RCTs with an exploration of ‘ideal dosage’ of moxibustion and/or acupuncture for managing CRI are required in future research.
Introduction
Insomnia is one of the most common disorders worldwide, 1 and the prevalence of CRI is substantially greater than in the general population, with 49.4% of the high prevalence. 2 CRI is highly persistent, especially in women. 2
CRI impedes the functional status and quality of life of cancer patients and their families, reduces their compliance with conventional anticancer treatments, and contributes to increasing their financial burden.3–5 These challenges subsequently threaten their long-term survival. 6 Consequently, many cancer patients turn to complementary and alternative therapies such as acupuncture or moxibustion7,8 to manage their symptoms due to fear of side effects of drugs that can further exacerbate cancer symptoms. 9
As an essential modality of acupoint stimulation, acupuncture and moxibustion can be a promising nonpharmacological intervention for managing CRI, given its potential benefits for cancer symptom alleviation10–13 and its feasibility for practice without increasing patients’ financial and physical burden.10,14–16 However, the previous review showed inconclusive results for the efficacy of acupuncture and/or moxibustion in managing CRI. 17 Systematic investigation of the safety, efficacy, and effectiveness of such interventions is thus essential to improve patients’ symptoms and quality of life.
Advancements in cancer diagnoses and treatments have significantly improved the survival rate, with 91% of patients in Australia reaching a chance of survival for 5 years or more. 18 However, long-term survival has highlighted a challenge in the ongoing management of cancer symptoms as patients can experience various unpleasant symptoms (such as CRI) throughout their illness trajectory.
CRI includes difficulty falling asleep, multiple awakenings during the night, or early morning awakenings with an inability to get back to sleep. Nearly half of all patients receiving cancer treatment experience trouble sleeping. 2 Insomnia has been one of the most prominent cancer symptoms and generally co-occurs with fatigue and depression as a symptom cluster.2,4,19–25 Common causes of CRI include medications (sedatives, hypnotics, and anticonvulsants), chemotherapy, radiation, or hormonal therapy. 26 Other factors such as pain, hot flushes, nausea, and vomiting, poor sleep hygiene, and lifestyle can also affect sleep patterns. 26
Sleep medications such as benzodiazepines, hypnotics, antihistamines, and tricyclic antidepressants are commonly used in conventional medicine (using drugs, radiation, or surgery) to treat insomnia. However, the effects of these pharmaceutical agents on CRI have been inconclusive, 27 and caution is advised with these agents as they may lead to next day trouble sleeping, dependence, and rebound insomnia once discontinued. 26 Exploring alternative approaches as adjuvant treatments have therefore been proposed to reach an optimal outcome of cancer symptom management.28,29
Acupuncture and moxibustion have been very well embraced by many communities worldwide to support optimal health and quality of life.16,30 The philosophy of acupuncture and moxibustion is central to living, yet little is known by many health professionals due to insufficient knowledge of such therapies.8,31 The conceptions of holistic health practice 32 fully embrace and are compatible with these modalities’ philosophy and theoretical underpinning,8,33 and yet have not been well integrated into health curricula and practice. 8 Why do we need to know about such modalities? Because your patients are using them!
The overall aim of this systematic review (SR) is to synthesise the best available evidence on the safety and efficacy of using moxibustion and or acupuncture to manage CRI in adults. The review questions are as follows:
Is moxibustion and/or acupuncture treatment more effective than conventional medicine or sham treatment at managing CRI in adults?
What is the best available and evidence-based treatment regimen (acupoints formula and intervention dose) using moxibustion and or acupuncture for managing CRI?
What is the best available evidence on the safety of moxibustion and/or acupuncture for CRI?
Materials and methods
Design
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement 34 was employed to provide a framework for this SR.
SR protocol registration
To promote transparency, reduce potential bias and avoid unintended duplications, this SR protocol was registered (CRD42019141785) with PROSPERO: https://www.crd.york.ac.uk/prospero/display_record.php?ID = CRD42019141785
Eligibility criteria
The following were the eligibility criteria (PICOs) of the present review:
Participants/population: adults with a clinical diagnosis of CRI. Exclusion: animal studies, adolescents under 18 years of age and elderly over 70.
Intervention(s): all types of acupuncture (manual, electro, or laser acupuncture) and or moxibustion (direct, indirect, or combined with a needle). Auricular and other acupoint stimulations were excluded.
Comparator(s)/control: conventional medicine (usual treatment or standard care) or sham group (sham acupuncture or sham moxibustion).
Outcome(s):
○ The efficacy of moxibustion and/or acupuncture for CRI measured by any validated tools. ○ Moxibustion and acupuncture-related adverse events and their possible causes.
Types of study to be included: randomised controlled trials (RCTs).
Search methods
In China, the history of Traditional Chinese Medicine (TCM) can be traced back 5000 years, and there has been a dramatic increase in research for the past 20 years.8,35 The inclusion period for this review is from the inception date of the databases to July 2020, published in English or Chinese. The Cochrane editorial board recommend including co-authors with different language skills to enable the inclusion of trials in languages other than English. 36 This is particularly important in this case, as there are many Chinese publications on this topic.
Information sources
Nine databases were searched – Allied and Complementary Medicine Database (AMED), Cochrane Central Register of Controlled Trials (CENTRAL), Excerpta Medica database (EMBase), MEDLINE, and Web of Sciences for English publications; CBM (SinoMed), CNKI (知网), VIP (维普), and WANFANG (万方) for articles that published in Chinese. Additional searches, including the Australian New Zealand Clinical Trials Registry (ANZCTR), ClinicalTrials.gov, World Health Organisation (WHO), and International Clinical Trials Registry Platform (ICTRP), were also conducted to avoid publication bias. Manual quest and reference list search were also included.
Search strategy
Search strategy encompassed the following steps: an initial partial search of each database, then assessing the key text included in the title and abstract of each paper to explore and identify keywords and index terms. These keywords and index terms were then applied to each database to explore further search terms to form a search plan; that is to say, each database had its own search strategy. For example, a search strategy for MEDLINE is presented in Table 1. The next step was to apply a specifically developed search strategy to each database for a full search.
Search strategy for MEDLINE.
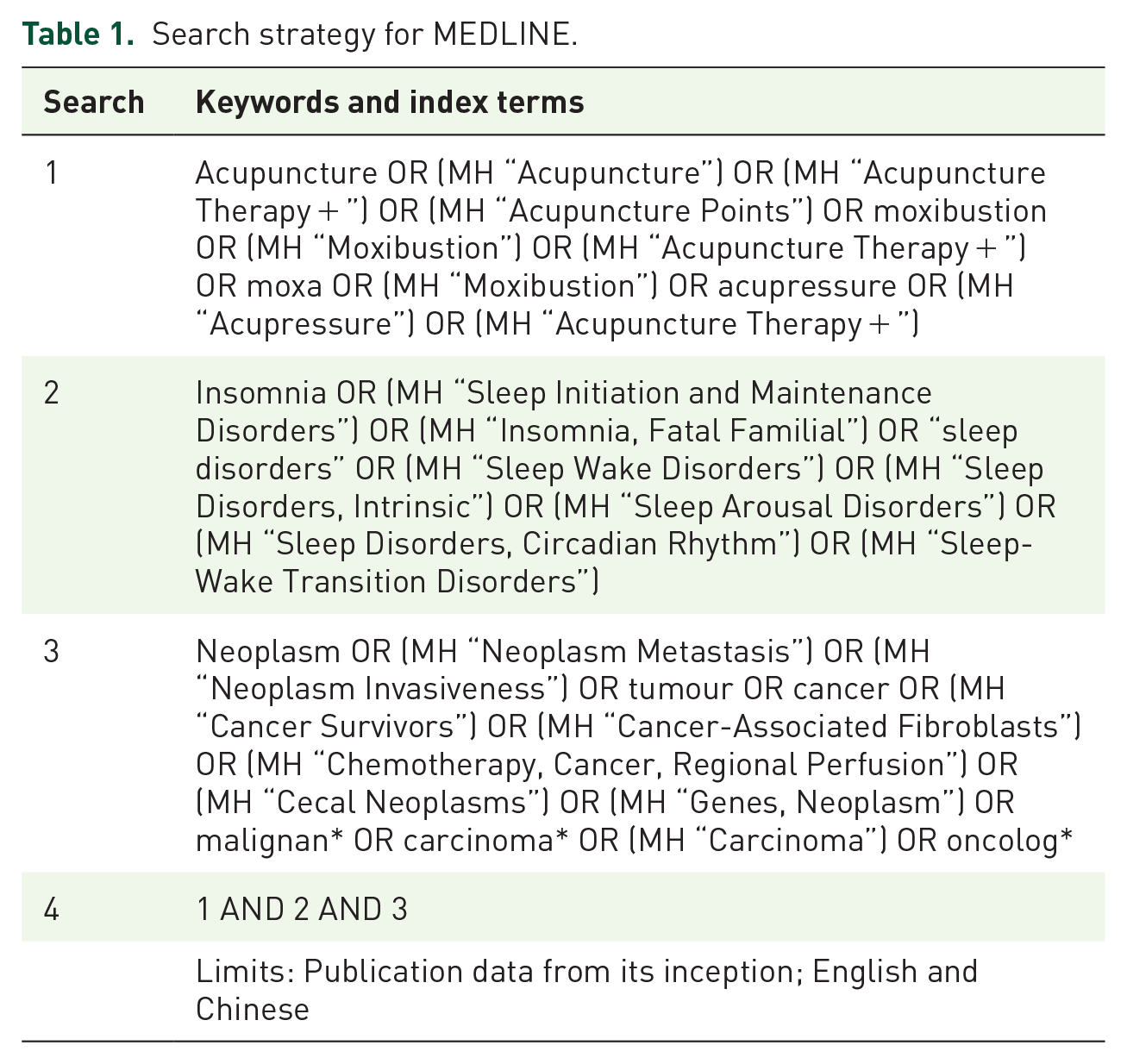
The four Chinese databases were searched using Mandarin keywords and index terms, whereas the other five English databases were explored using English keywords and index terms.
Moxibustion, acupuncture, and acupressure are all based on the theories underlying TCM and involve stimulating acupoints to achieve a desired therapeutic effect. For this reason, we also included acupressure-related keywords and index terms in the searches.
‘艾*’, ‘针*’, ‘穴*’, ‘睡眠障碍’, ‘失眠’, ‘睡眠’, ‘肿瘤’ and ‘癌症’ were the keywords used in the electronic search of Chinese databases; and ‘acupuncture’, ‘moxibustion’, ‘moxa’, ‘acupressure’, ‘insomnia’, ‘sleep disorders’, ‘neoplasms’, ‘tumour’, ‘cancer’, ‘malignan*’, ‘carcinoma*’ and ‘oncolog*’ were searched in English databases.
Due to moxibustion and acupuncture-related adverse events being poorly underreported, 16 keywords and index terms related to adverse events such as side effects and safety were therefore not included in the searches; however, this outcome was investigated and assessed at a later stage for those studies that were included in the analysis of this review.
Four reviewers (EH, MJ, XH, and CW) independently performed the data extraction, screening, and selection process. The reviewers had clarified with the original authors when there were missing or unclear data.
Search outcome
This SR included all published and unpublished RCTs conducted in any study setting investigating the efficacy of moxibustion and or acupuncture for adults suffering from CRI. Our search followed the eligibility criteria and our protocol which was registered (CRD42019141785) with PROSPERO.
Quality appraisal
Risk of bias (ROB) for all included individual studies and across studies were assessed at the study level using the Cochrane ROB tool and allocate domains (randomisation, allocation, concealment, blinding, attrition bias, selective outcome reporting, and other bias) with Low, Unclear, or High ROB. 37 Disagreements between reviewers were resolved by discussion.
Data abstraction
With a predefined data extraction excel sheet, data extracted from the included studies including the characteristics of study (authors, year of publication, design, and setting), participants (age, gender, sample size, diagnostic, and reason for moxibustion and or acupuncture), intervention dosage (duration, frequency, and intensity), acupoints formula, comparisons, treatment outcome and measurement tools used, and adverse event.
Synthesis
RevMan 5 (version 5.3; the Cochrane Collab-oration, Oxford, UK) was used to conduct a meta-analysis. Efficacy was measured with 95% confidence intervals (CIs) and weighted mean difference (WMD) for continuous outcomes, and risk ratios (RRs) with 95% CIs were calculated for dichotomous outcomes. Forest plots were used to identify heterogeneity I2 statistics (1%–100%) and imprecision. The findings were also communicated in narrative form, and tables and figures to assist in data presentation.
Results
Study selection
Figure 1 outlines the search process. Literature search generated 2685 articles. A total of 1015 duplicates and the subsequent 1573 citations were excluded based on title and abstract screening; 97 articles were, therefore, remained for full-text assessment with the application of our inclusion criteria. Eighty-three citations were further excluded due to insomnia was not the primary outcome (n = 2), participants not meeting inclusion criteria (n = 50), conference papers (n = 12), clinical trial protocols (n = 10), study design other than RCT (n = 6), intervention other than acupuncture/moxibustion (n = 2), and language other than English or Chinese (n = 1).

Flowchart of literature selection on randomised controlled trials of acupuncture for the management of cancer-related insomnia.
Study characteristics
This SR included a total of 14 randomised controlled trials (RCTs) with 1187 participants. Table 2 summarises the characteristics of these included RCTs. The RCTs were published between 2011 and 2019 inclusive, with one conducted in Sweden, one in Denmark, three in the United States, and nine in China. Cancer types in these studies include breast cancer (n = 4), Thyroid cancer (n = 2), Lung cancer (n = 2), lymphoma (n = 1), and a combination of various cancer types (n = 5). The 14 RCTs encompassed moxibustion (n = 5),38–42 manual acupuncture (n = 5),11,43–46 and electro-acupuncture (n = 4)47–50 modalities. As for the comparisons, five RCTs compared moxibustion as an add on to conventional medicine;38–42 two compared the combination of moxibustion and acupuncture to conventional medicine;45,46 one compared acupuncture to sham acupuncture and no treatment; 43 two compared acupuncture to conventional medicine;11,44 one study compared electro-acupuncture to sham acupuncture and waitlist group, 48 whereas three compared electro-acupuncture to conventional medicine.47,49,50 Out of 14 studies, only four reported adverse events, and the most frequently reported outcomes were mild and moderate needling site soreness and pain (n = 9).39,43–45
Characteristic of included randomised controlled trials on acupuncture and or moxibustion for managing cancer-related insomnia (CRI).

AIS, Athens Insomnia Scale; AT, acupuncture therapy; C, control; CRI, cancer-related insomnia; EA, electro-acupuncture; F, female; HT, hormone therapy; ISI, Insomnia Severity Index; M, male; NR, not reported; PSQI, the Pitttsburgh Sleep Quality Index; RCT, randomised clinical trials; SA, sham acupuncture; SD, standard deviation; WLC, waitlist control.
Synthesis of results
Twelve out of 14 studies provided outcomes of the Pittsburgh Sleep Quality Index (PSQI) that were measured as continuous data,11,38–50 of which eight did not provide the standard deviations for the mean difference.38–42,45,46,50 For the 12 studies, no significant differences in PSQI were observed at baseline between the treatment and control groups (all p > 0.05). Furthermore, for these studies, the mean PSQI score at baseline for the treatment and control groups was collectively at 12.4, with a mean difference of 0.17 (i.e. a CV of 1%) is minimal. Given that the PSQI baseline differences were statistically insignificant, and the absolute mean difference was negligible, the authors decided to input the post-treatment PSQI scores into the RevMan software for the subsequent meta-analysis. 95% Cls and WMD was calculated for continuous outcomes (Figure 2). Meanwhile, 5 out of 14 studies provided outcomes that were measured as dichotomous data.41,43,45–47 RRs with 95% CIs were calculated for such outcomes (Figure 3). The forest plots were used to identify heterogeneity I2 statistics (1–100%) and imprecision.

Efficacy of moxibustion and or acupuncture for the management of cancer-related insomnia: outcomes measured as continuous data.

Efficacy of moxibustion and or acupuncture for the management of cancer-related insomnia: outcomes measured as dichotomous data.
Outcome measures
Is moxibustion and or acupuncture treatment more effective than conventional medicine or sham treatment at managing CRI in adults?
The included 14 RCTs showed superior effects of moxibustion and/or acupuncture compared with conventional medicine and sham treatment. A meta-analysis also showed positive effects of moxibustion and or acupuncture.
Moxibustion versus conventional medicine 5 RCTs compared the effects of moxibustion as an add on treatment with conventional medicine.38–42 One study measured the outcome with PSQI, and the score not only showed a significant change (favours moxibustion), participants in the treatment group also used less sleeping pills than the control group (p < 0.05). 39 Another study showed a statistically significant difference between the treatment group and the control group. Moxibustion demonstrated a superior effect compared to conventional medicine. 38 Although the other three studies have different sample populations – lymphoma, 40 thyroid carcinoma,41,42 and the moxibustion treatment regime were completely different yet, the score of PSQI in these studies showed a decrease in the treatment group compared to the control group (p < 0.05), and the authors concluded that moxibustion could effectively improve insomnia in their study.
Moxibustion and acupuncture versus conventional medicine 2 RCTs assessed the effects of the combination of moxibustion and acupuncture compared to conventional medicine.45,46 Both studies have the same sample population – various types of cancer patients, and their results were not quite the same. One study 45 showed a PSQI score with a significant change (favours moxibustion and acupuncture), and the effective rate of the treatment group was higher than that of the control group (p < 0.05). In another study, 46 the PSQI showed no statistical significance (p > 0.05) between two groups upon completion of the treatment. However, on follow-up, the effective rate of the treatment group was higher than that of the control group (p < 0.05). This study suggested that the effect of using moxibustion and acupuncture to treat tumour patients with insomnia is as good as conventional medicine, but its long-term effect is better with no side effects.
Acupuncture versus conventional medicine 2 RCTs compared the effects of acupuncture and conventional medicine.11,44 One study found that immediately post-treatment, there was a statistically significant (p < 0.05) difference in insomnia severity from baseline for both groups. The between-group difference favoured conventional medicine. However, the improvements for both groups were maintained at the 20-week follow-up point. 44 The other RCT found that the PSQI score of the treatment group was significantly lower than the control group (p < 0.05), and they concluded that acupuncture could effectively improve CRI. 11
Acupuncture versus sham acupuncture and no treatment 1 RCT assessed the effects of acupuncture compared to sham acupuncture and no treatment groups. 43 The authors concluded that 52% of patients experienced a significant effect in the acupuncture group compared with 24% in the sham group (p < 0.05). A statistically significant positive effect was seen in the acupuncture group compared with the sham acupuncture and no-treatment groups. The authors concluded that acupuncture significantly relieves sleep disturbances and is a good and safe treatment in managing CRI.
Electro-acupuncture versus conventional medicine 3 RCTs compared the effects of electro-acupuncture and conventional medicine.47,49,50 One study found that after treatment, the score of PSQI of the patients in the treatment group was significantly lower than that in the control group (p < 0.01), and the authors claimed that electro-acupuncture can effectively improve CRI. 50 Similarly, one study found that the mean reduction in PSQI total score was significantly greater in the electro-acupuncture group as compared to the conventional medicine group (p < 0.05). 49 The other study found a significant improvement in CRI parameters in bother treatment and control groups. Furthermore, the study found that a 12-weeks electro-acupuncture has the same positive effect as a 2-year conventional medicine. 47
Electro-acupuncture versus sham acupuncture and waiting list group 1 RCT assessed the effects of the electro-acupuncture compared to sham acupuncture and waiting list group. 48 The authors found that both electro-acupuncture and sham acupuncture produced nonsignificant improvements in the PSQI score over time (p = 0.058 and p = 0.31, week 8 and week 12, respectively). Interestingly, as the previous paragraph demonstrated, studies comparing EA to conventional care have more positive results. The discrepancy between the study that did not find a significant difference between electro-acupuncture (EA) versus sham procedure and the studies that demonstrated a positive effect of EA might be due to the different research designs employed. Whether to use a sham group in this field of clinical trials is often a debate.51,52
Comparators For conventional medicine as a comparison, five trials found statistically significant benefits for those receiving moxibustion as an add-on treatment;38–42 two trials showed the combination of moxibustion and acupuncture to outperform conventional medicine significantly;45,46 two trials from our meta-analysis significantly favours acupuncture compared to conventional medicine;11,44 yet, another three trials find statistically significant in favour of electro-acupuncture versus conventional medicine.47,49,50
Regarding sham acupuncture as a comparison, one trial found acupuncture to outperform sham control 43 significantly, and another trial found electro-acupuncture outperformed no active control intervention group. 48 The authors suggested that acupuncture is a promising alternative to manage CRI.
Meta-analysis 12 RCTs used PSQI scores as continuous data measuring the effects of moxibustion and/or acupuncture for the management of CRI. These studies showed superior effects of moxibustion and or acupuncture compared with conventional medicine and sham treatment. A meta-analysis also showed positive effects of moxibustion and or acupuncture (n = 997, MD = −1.84, 95% CI = –2.75 to −0.94, p < 0.01) (Figure 2). Five RCTs used continuous data testing the effects of moxibustion and or acupuncture for the management of CRI. These studies showed superior effects of moxibustion and or acupuncture compared with conventional medicine and sham treatment. A meta-analysis also showed significant difference between 2 groups (n = 358, RR = 0.45, 95% CI = 0.26–0.80, I2 = 39%, Figure 3).
What is the best available and evidence-based treatment regimen (acupoints formula and intervention dose) using moxibustion and or acupuncture for managing CRI?
In this review, the most frequently used acupuncture points for breast cancer include PC6, KI3, SP6, and LV3; GV20 for thyroid cancer; KI1, KI6, BL62, HT7, EX-HN3, EX-HN1, and Anmian for lung cancer; and KI1 for lymphoma. Given the cancer types, intervention modalities and treatment regimens were varied in the included studies. Some studies did not report their treatment plan in detail; therefore, it is very difficult to form a unified treatment regime in this review. In addition to conventional clinical diagnosis, Chinese medicine pattern identification and clinic expert consultation are crucial processes in formulating a standard treatment regime for a specific CRI management.
What is the best available evidence on the safety of moxibustion and/or acupuncture for CRI?
In general, these modalities are safe with few adverse effects if administered by a trained professional, and this conclusion is in line with the existing review. 16 However, the adverse effect was poorly reported in the included studies, with only 4 out of 14 studies reporting adverse events. One RCT reported local area allergy/skin lesion in the moxibustion group (n = 3); 39 one reported mild and moderate needling site soreness, itchiness, and pain in the acupuncture group (n = 9), 44 one reported mild and temporary fatigue, pruritus, and nausea in the acupuncture group (n = 5), sham acupuncture group (n = 8), and no treatment group (n = 1); 43 and one reported local area soreness (n = 1), and bruises in the local area (n = 1) in the acupuncture group. 45
ROB across studies
The results of the ROB assessment for the 14 included RCTs are detailed in Figure 4.11,38–50 For selection bias, all RCTs had a low ROB with adequate sequence generation. However, only nine studies had a low ROB with adequate allocation concealment.38–43,44,48,49 For performance bias, only two studies had a low ROB with blinding of participants and personnel.43,48 For the detection bias, all trials failed to report blinding of outcome assessment. For attrition bias, ten studies had a low ROB on dealing with incomplete outcome data11,38,40–44,46,49 whereas four studies had a high ROB.39,45,47,48 For reporting bias, all studies had a low ROB with selective reporting. Similarly, for other bias, all studies appear to be free of other sources of bias.

(a) Risk of bias graph: review authors’ judgements about each item’s risk of bias item presented as percentage across all included studies. (b) Risk of bias summary: review authors’ judgements about each item’s risk of bias for each included study. +, low risk of bias; –, high risk of bias; ?, unclear.
Discussion
Summary of evidence
We have successfully updated the evidence by adding additional eight RCTs compared to the previous review. 17 Results from 14 RCTs with 1187 CRI patients were summarised in this SR. Moxibustion and/or acupuncture were associated with clinically relevant effect sizes in managing CRI compared to conventional medicine and sham treatment.
The previous review 17 included six RCTs. Only three had a low ROB for allocation concealment, and two did not report the sequence generation method. In our review, we performed a rigorous ROB assessment, and the survived 14 RCTs overall high in quality, which can impact the results of the current meta-analysis. However, a reminder that there is always a subjective element in these assessments could affect the outcome of our conclusion.
The results of this SR are different from the previous review. 17 The previous review showed inconclusive results due to ‘a lack of high-quality studies’. 17 Our review, however, found that there are benefits in moxibustion and or acupuncture to manage CRI. We also found a trend between increased treatment dosage (frequency, intensity, and duration) and a reduction in the severity of CRI. For example, our ‘survived’ higher-quality studies conducted in China turn to have longer treatment sessions and higher frequency, showing superior outcomes.11,46
Relevance to research and practice
Higher quality, lower ROB, with powered sample size RCTs with adequate follow-up post-intervention to assess the efficacy and effectiveness of moxibustion and or acupuncture for the management of CRI are required in future research. Future research on clarification of ‘ideal’ dosage of moxibustion and or acupuncture for an average patient managing CRI would be helpful. With the emergence of integrative medicine, more trials that model real-world settings in different countries, compare moxibustion and or acupuncture as an add-on treatment versus conventional medicine alone as a primary comparator, may provide results that directly inform clinical practice, and therefore are required in future research. These trials can provide evidence for patients when making treatment options, for practitioners when referring their patients to a Chinese medicine practitioner, for decision-makers when providing resources to support cancer CRI treatment, and for policymakers when producing related economic policies that are relevant to CRI. There are challenges within the sham-controlled trials for acupuncture studies due to some sham techniques may not be capable of acting as placebo treatments. 51 Sham acupuncture techniques, therefore, should be carefully considered when implementing a sham-controlled clinical trial. 51 Pragmatic trials that were designed to answer a question about decision making in clinical care, 52 where the control treatment can be an established standard therapy or a no-treatment group, 51 could also be an option when designing a trial. Perhaps the increasing use of protocol submission before clinical trials will force authors to make greater efforts, which should be a future editorial requirement. The review provides some level of support for moxibustion and or acupuncture as a treatment for CRI.
Limitations
There are several caveats concerning the overall findings of this review: (1) The level of ROB of included studies across the seven ROB domains. No trials were assessed as having a low ROB across all domains. (2) The dominance of trials from China may compromise the transferability of the results. Only five trials were conducted in other countries – the USA (n = 3), Denmark (n = 1), and Sweden (n = 1). (3) Studies conducted in China tend to have larger effect sizes, this may be due to the dosage (frequency and duration) of treatment regimen (the frequency at least), and the number of total treatments delivered in these studies was greater than studies conducted in other countries. One can argue there may be an association between the larger effects seen in these studies from China and a high ROB of these trials, especially in performance bias and detection bias. For example, this lack of blinding is likely to increase the nonspecific/attention effects of those in the treatment group and may overestimate the effect size. (4) The adverse effect was poorly reported in the included studies, with only four trials reporting the adverse effect.
Conclusion
Our meta-analyses demonstrated that moxibustion and/or acupuncture showed a positive effect in managing CRI, and such modalities could be considered an add on treatment in CRI management. These modalities are generally safe when carried out by qualified practitioners and supported with well-established clinical guidelines. However, the findings need to be interpreted with vigilance as the positive effects from this review seemed to relate to the predominance of Chinese studies.
Given the ROB inherent in much Chinese medicine research, although there is now more positive evidence than inconclusive results from existing reviews, there is still a need for more high-quality, well-designed studies to prove the benefit beyond reasonable doubts, and the efficacy from different dosages and intensities is still unknown. Furthermore, future studies should report adverse effects comprehensively to facilitate the safety assessment.
Footnotes
Author contributions
All authors contributed to this study.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is funded by Edith Cowan University Early Career Researcher Grant -2019 (G1004342).