
Abstract
The care needs of babies, children and young people who use children's hospices have changed over the last decade, with children living for longer, with more complexity. Children's hospice workforces have evolved to continue to meet these needs, including a growth in the number of nurses working at specialist and advanced levels, particularly prescribing. A 15-question survey was sent to all 54 UK children's hospices, which aimed to explore the impact of independent nurse prescribing, and specialist and advanced level nursing practice in UK children's hospices. Forty-one organisations responded, representing 76% of UK children's hospices. Increased autonomy and the ability to respond to the dynamic needs of families, and enabling family choice was recognised and valued by prescribers. Challenges included the breadth of needs of children with life-limiting conditions, and the use of medicines that are either unlicenced or used off-licence. Access to clinical supervision and continuing professional development were highlighted as enablers of prescribing practice.
Keywords
Background
There are 54 children's hospices across the United Kingdom (UK). They are independent, charitable organisations that provide a range of child-focused, family-centred services for babies, children, and young people (children) with life-limiting and life-threatening conditions, together with their families. These are usually offered from the point of diagnosis or recognition, through life, dying and following a child's death. Care services offered by children's hospices include planned and unplanned short breaks (respite), symptom management and end-of-life care, and bereavement support before and after death. The way in which care is provided by hospices has evolved over the last 40 years (Tatterton et al., 2021), to reflect the changing needs of children requiring palliative care.
There has been a significant increase in the prevalence of children with life-limiting and life-threatening conditions – a trend which is expected to continue. Current data (Fraser et al., 2021) suggests that the prevenance of life-limiting conditions in England has increased from 26.7 per 10,000 children in 2001/02 to 66.4 per 10,000 children 2017/18. These changes are particularly notable in infants (under one year), in children from Pakistani, other Asian and Black ethnic minority groups, and those with congenital and genetic conditions, which are more prevalent in children from minority ethnic groups (Iluno et al., 2024).
The care needs of children have also changed. Children are living with more complex conditions, requiring more nursing interventions, and are increasingly reliant on more life-enhancing and life-sustaining technologies, including enteral feeding, ventilation, parenteral nutrition and peritoneal dialysis. Advancements in technologies and science mean that children are living longer with improvements in both life expectancy and quality of life.
Nursing practice has developed in response to the changing needs of the UK population and the multiprofessional dynamics of the healthcare workforce. Nurses are working in more autonomous roles than ever before, with a rise in the number of specialist and advanced level roles (Figure 1) which blurs the traditional role boundaries of nursing, medicine and allied health professionals.
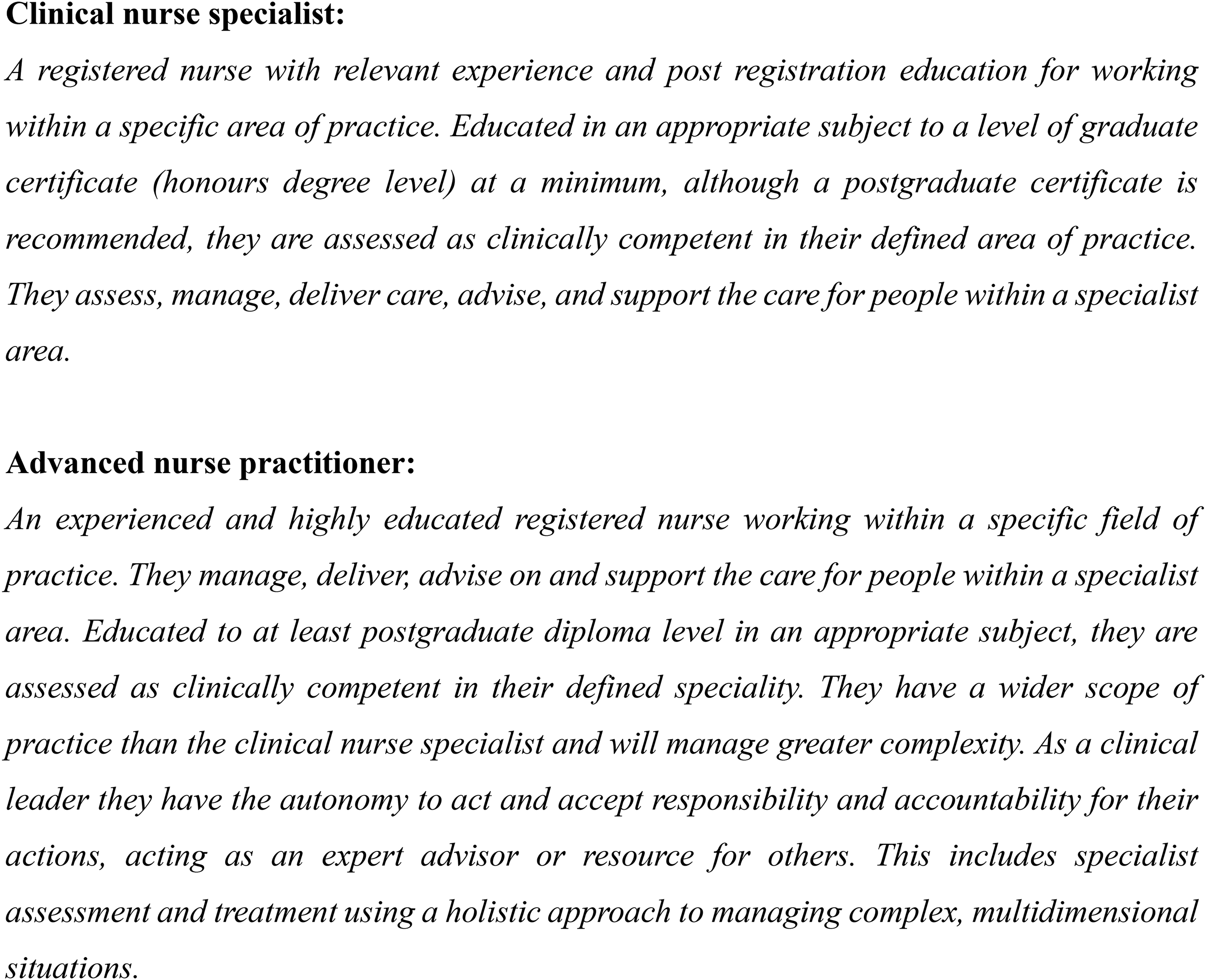
Definitions of specialist and advanced level nursing practice (source: Scottish Government, 2021).
Nurses, and some allied health professionals who train as independent prescribers (often colloquially referred to as ‘non-medical prescribers’) in the UK have some of the most liberal prescribing rights of non-medical professionals worldwide (Cope et al., 2016). Nurse independent prescribers can prescribe a full range of medicines, including off-licence prescribing, and prescribing unlicenced medicines, providing it is within their self-identified scope of practice (Nursing and Midwifery Council, 2018).
A previous study (Tatterton, 2017), following the development and publication of the second edition of the Together for Short Lives Medicines Management Toolkit (Armitage, 2014) identified that registered nurses were making a significant contribution to the prescribing and medicines needs of children in children's hospices. The emergence of nurses in specialist and advanced practice roles was apparent, including clinical nurse specialists, advanced nurse practitioners and consultant nurses.
Aim
The aim of this study is to explore the impact of independent nurse prescribing, and specialist and advanced level nursing practice in UK children's hospices.
Method
A 15-question electronic survey was designed using Jisc Online Surveys to capture the prevalence and practice of non-medical independent prescribers in children's hospices. The survey was based on the survey used in the 2017 study (Tatterton, 2017). The survey contained a combination of open and closed questions, gathering quantitative and qualitative data relating to the practice of prescribers and the context in which they prescribe. The survey was designed to explore scopes of practice, specifically the kinds of medicines that nurses are prescribing, and the frequency and location in which they prescribe. In addition, details of benefits and barriers to prescribing were sought as well as identifying any perceived pressure that nurses felt to prescribe current or new medication.
Validity and Reliability
Several steps were taken to ensure the reliability and validity of the questionnaire. The questionnaire was drafted by MJT and amended by CB and ZPMS. Consultation with hospice-based healthcare professionals was conducted to ensure content validity and contemporary relevance. Reliability was assured through a pilot of children's hospice practitioners based in the North of England. Inter-rater reliability was assessed and assured by inviting multiple practitioners from the same organisation to participate in the pilot, which yielded consistent responses.
Ethics
Ethical approval was sought and granted by the Humanities, Social and Health Sciences Research Ethics Panel at the University of Bradford (reference: EC27876).
Data Collection
An electronic questionnaire was sent to all 54 children's hospices via email to the Together for Short Lives Leaders of Care distribution group and Care Forum – a national electronic forum for professionals working in children's hospice and palliative care services. In addition, the survey was shared on social media, via X (formerly Twitter).
Data Analysis
Due to the relatively small dataset, quantitative data were anonymised and amalgamated using Microsoft Excel by MJT. Qualitative data were analysed using deductive content analysis (Elo et al., 2014), which allowed a richer understanding of the impact specialist and advanced level nursing practice has on the practitioners themselves, children, families and their organisation. These were coded independently by MJT and CB before being discussed and agreed by the other authors. Verbatim quotes have been used to add depth to the quantitative findings.
Findings
Forty-one children's hospices responded to the survey between August and October 2023, representing 76% of children's hospices in the UK. A total of 97 independent nurse prescribers were employed by 25 hospices, which includes those working as advanced nurse practitioners. This contrasted 50 doctors, employed directly by 23 hospices, with a further 45 doctors, most commonly general practitioners, who attended 23 hospices on a visiting basis. Hospices highlighted how an increase in independent nurse prescribing led to a reduction in the reliance on visiting doctors to meet the medicine needs of babies, children and young people in their care.
Nurses and Independent Prescribing
Prescribing practices of registered nurses were explored in detail. The majority of prescribing occurred in children's hospice buildings (n = 34), with almost half of hospices providing home-based access to prescribing (n = 18), and some hospital-based in reach (n = 7). Independent nurse prescribers prescribe medicines most frequently on hospice medicine administration record (MAR) charts (n = 28), or those of NHS or partner organisations (n = 4). Sixteen hospices had access to NHS prescription charts (FP10 forms), 11 of which used electronic prescribing.
Of the 41 hospices who responded to the survey, 39 had access to pharmacy support, most commonly via service level agreement with hospital-based NHS pharmacy services (n = 19), or employed directly by the hospice, usually on a part-time basis (n = 17). Three hospices highlighted access to pharmacy support via informal agreement, through pharmacies local to the hospice, or via the local palliative care network.
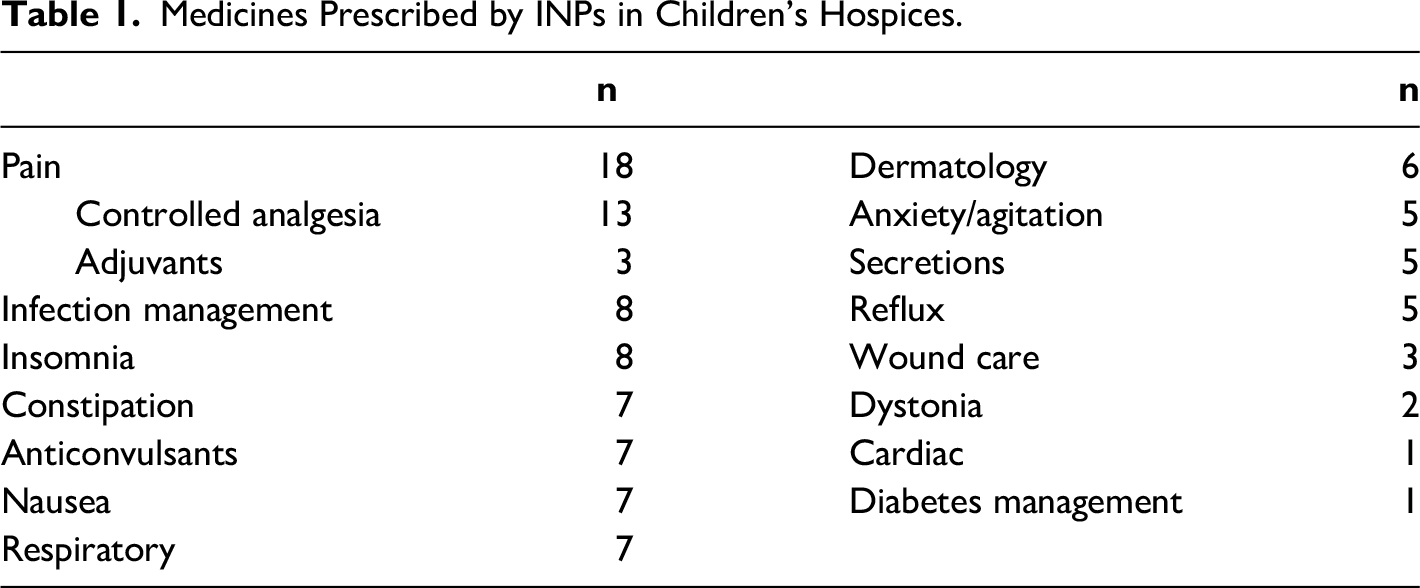
Nurse independent prescribers prescribe a range of medicines, which reflect the range of needs of babies, children and young people with life limiting conditions (Table 1). Prescribing practice included the prescribing of new medicines and the adjustment of existing medicines to manage symptoms. Only four prescribers highlighted prescribing solely to enable the continuation of existing prescriptions. Most prescribing practice related to symptom management, with pain (n = 23), nausea (n = 14), seizures (n = 11) and anxiety/distress (n = 10) being the most common symptoms requiring medication. In addition to symptom management, independent nurse prescribers highlighted prescribing to manage infections (n = 14), as well as medication to manage skin conditions (including emollients and topical preparations) (n = 12), and constipation (n = 8). Prescribers were generally confident in their ability to prescribe and to always practice within their scope of competence, although five prescribers had felt pressure to prescribe.
Medicines Prescribed by INPs in Children's Hospices.
The Impact of Independent Nurse Prescribers and Advanced Nurse Practitioners
Nurses were asked what impact the ability to prescribe had on themselves, the children and families in their care, their colleagues and organisation. Nurses highlighted the increased autonomy that independent prescribing enabled, alongside the ability to provide timely care to children requiring new or amended prescriptions. The link between being able to respond immediately to the needs of children and families was strongly linked with increased job satisfaction. Prescribers recognised the family-centred, biopsychosocial and spiritual perspective of nursing children, and the added value of this when making prescribing decisions: ‘utilising my skills and knowledge to provide total patient care is great […] for example, I am better able to control pain and emotional effects of the physical symptoms.’ (respondent 12) ‘I feel as a nurse I may know the children and family's lived experiences in more detail than my medical colleagues so I can prescribe more holistically in some cases.’ (respondent 16)
Prescribing allowed nurses to lead the development of advance care plans, including anticipatory prescribing. These were most commonly co-produced with multi-agency input, reflecting the interagency delivery of children's palliative care.
Nurses highlighted the impact of prescribing on enabling the choice in place of care for families. The link between prescribing and the ability to provide symptom management and end of life care at home was recognised and celebrated by prescribers: ‘being an ANP in a children's hospice is one of the most rewarding jobs an ANP can do and it really makes a difference to children and families. Respecting [the] choices families [make] in [their preferred] place of care and assisting families to care for their child at home.’ (respondent 6)
Prescribing practice was not limited to unplanned care; practitioners highlighted the provision of short breaks (respite) and how the increased availability of prescribers led to timely care, through signing off hospice MAR charts, as well as the ability to prescribe to continue a supply of existing medicines. Short breaks provided an opportunity for prescribers to review children and the request of families, replacing what might be considered general practice. Prescribers described how these reviews surrounded ‘routine’ conditions including dermatology, constipation and reviewing medicine doses due to changes in a child's weight.
Prescribers valued the opportunities to develop their scope of practice as prescribers and recognised their position as potential role models for colleagues within their organisations. Prescribers were keen to support junior colleagues, through the provision of education and mentorship. The investment in nursing career development was valued and praised by prescribers; numerous respondents highlighted this as a means of recruiting and retaining registered nurses. The increased awareness of medicines, pharmacology and medicines safety and governance was highlighted, providing organisational assurance, and improving working practices, particularly within the nursing workforce and interagency approaches to care.
The Challenges of Independent Nurse Prescribing
Independent nurse prescribing is not without its challenges. This was summarised by one respondent who stated: ‘as a hospice [independent nurse prescriber] it takes a bit more work to ensure practice is kept current.’ (respondent 23).
The majority of the issues expressed by prescribers relate to the breadth of needs of children with life-limiting and life-threatening conditions who rely on hospice services. This was due to the breadth of medicines required by children who use hospices, and the use of medicines that are either unlicenced or used off-licence (García-López et al., 2020). This is compounded by the small number of prescribers who work in individual organisations, particularly where nurses prescribe independently without the support of advanced nurse practitioners or medical colleagues who are based in the same organisation. Prescribers expressed feeling ‘out of their depth’ and described a lack of confidence in prescribing, most notably independent nurse prescribers with less experience.
Having the time to prescribe was a frequently cited challenge by nurses. Many prescribers who responded to the survey work in roles providing direct care, which makes finding time to prescribe challenging. Access to clinical supervision and ongoing continuing professional development was an issue for some prescribers. Again, this appears to particularly affect prescribers who work in organisations without peers who prescribe, or senior clinical colleagues. Prescribers working in smaller hospices described limited opportunities to prescribe, affecting their confidence and perceived ability to maintain the required knowledge and skills to practice.
Enabling Independent Nurse Prescribing in the Hospice Workforce
The impact of education to support prescribing decisions, access to continuing professional development and frequent clinical supervision were cited by almost all respondents. Prescribers highlighted the importance of governance structures within their organisations to support safe and effective prescribing, helping prescribers feel supported in their practice, illustrated in Figure 2.
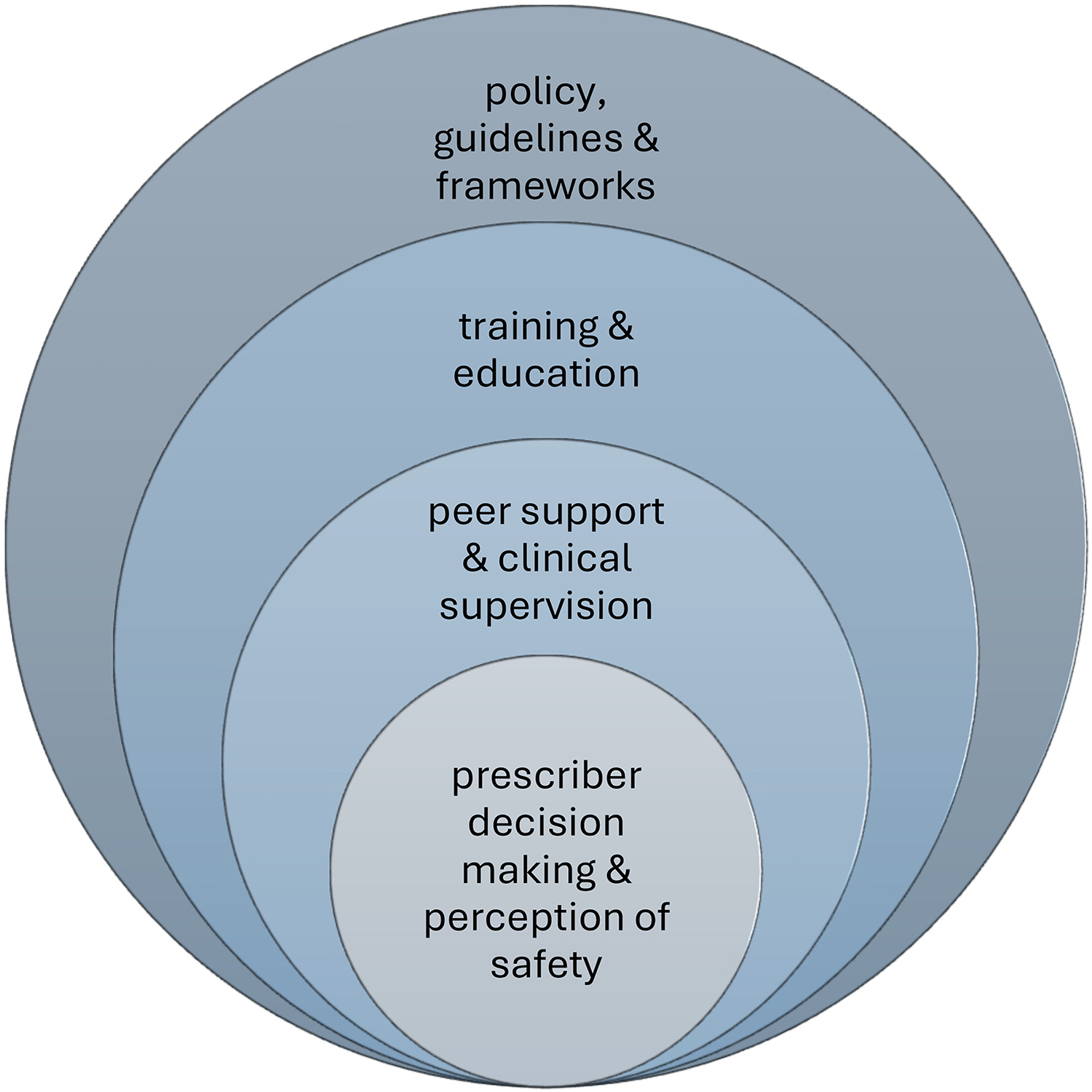
The influence of policy, training and supervision on practice.
More than half of respondents cited the importance of completing an advanced clinical assessment and history taking module and discussed the positive impact this had on their practice. Access to prescribing updates, aimed specifically at non-medical independent prescribers was seen as beneficial, as were updates from organisations such as regional children's palliative care networks, Together for Short Lives and the Association of Paediatric Palliative Medicine.
Peer support was valued by prescribers, particularly where multiagency approaches were taken. Examples of networks that included NHS-employed prescribers, and those that included both child and adult palliative care services were shared, which helped hospice-based prescribers feel less isolated and more connected with the wider workforce. Benefits of peer support discussed by respondents included the defining of scope, and opportunities to develop, through education and shadowing colleagues in other teams and settings. Prescribers who accessed supervision felt a reduced sense of pressure to prescribe medicines, and discussed a wider support network, enabling them to access support with clinical decision making across organisations.
Finally, prescribers in organisations with clear policies and procedures around independent prescribing, which include practice and recognise the need for education and clinical supervision, felt enabled to prescribe. Prescribers experienced less anxiety when the expectations of them as prescribers were made clear by their organisations.
Discussion
This study aimed to explore the impact and contribution of independent nurse prescribers in UK children's hospices. Seventy six percent of children's hospices responded to the survey, identifying 97 independent nurse prescribers working across the organisations that responded, which included nurses working at specialist and advanced levels. Prescribing occurred in a range of settings, with a marked increase in the availability of community-based prescribing, enabling families to make uncompromised choices in their place of palliative care. Respondents discussed the flexibility that having more prescribers within the nursing workforce enabled, as well as ability to respond to the dynamic needs of children and their families. Prescribers faced several challenges, including definition of scope, ability to practice and access to continuing professional development and clinical supervision.
One of the keys to the success of children's hospices in the UK has been their ability to continually evolve to meet the contemporaneous needs of children and families who rely on their care services (Tatterton et al., 2019). In recent years there has been an increase in the demand for care outside of hospice buildings, including care at home, and hospital in reach (Tatterton, 2019). Independent nurse prescribers have been central in enabling this. The greater availability of prescribers within the nursing workforce (Tatterton, 2017) has enabled hospices to provide more community-based care, enabling families to make uncompromised choices in their place of care on an increasing range of services, moving beyond short breaks, to include the provision of symptom management and end of life care (Osborne & Kerr, 2021). INPs allow hospice care teams, often in partnership with other local services, to manage symptoms associated with progressive, deteriorating conditions (Bogetz & Lemmon, 2021), by initiating and titrating medicines in response to the needs of children. Findings from this study suggest that nurses are prescribing an increasing range of medicines to manage broader and more complex symptoms.
The ability to respond to family wishes around their place of symptom management and end of life care was widely cited by hospices as a major benefit on INP. There appears to be increased focus on the delivery of community-based hospice services across the UK, in response to the expressed wishes of families (Barratt et al., 2023). This corelates with developments seen in British adult hospices (Fee et al., 2023), as well as statutory health services, including children's community nursing services (Jones et al., 2023), and hospital outreach teams.
In recent years there has been increasing emphasis on organisations to facilitate choice in the place of care, including a greater focus on providing care at home, which is strongly advocated by policymakers (Bluebond-Langner et al., 2013). There is recognition that care for children with life-limiting conditions must include support for parents and other family members (Gill et al., 2021). The increased ability for hospices, enabled by INPs, to meet the dynamic needs of children means that care at home can extend beyond short breaks to include more complex elements of care, including symptom management and end of life care.
Family centred care (Child and family-centred healthcare: concept, theory and analysis, 2010) is integral to the philosophy that underpins children's hospice services (Tatterton & Walshe, 2018). Hospices strive to meet the needs of children and their families with parity, providing dedicated care to parents, siblings and other family members, including grandparents (Tatterton & Walshe, 2019). The reassurance that improved access to prescribing enabled was widely cited as a benefit of prescribing, not only to families, but to the prescribers themselves, which demonstrates the commitment of hospice staff to services that meet the needs of whole families. Advance care planning is central to this; these provide practitioners with sound evidence base to deliver care (McMahan et al., 2021). Respondents highlighted their role in writing and following advance care plans, which can lead to an increased sense of control and reassurance for families about the current needs of their child, as well as plans for the anticipated deterioration of their child and their condition progresses (Winger et al., 2020).
Our findings identified higher levels of advanced nursing practice across UK children's hospices than have been found before (Tatterton, 2017). The impact of advanced level practice has been widely cited across healthcare (Battista & Sciacca, 2023; Collett et al., 2020; Hickish & Roberts, 2019; Jounaidi et al., 2024; McIlfatrick & Muldrew, 2022), with advanced practitioners taking on new and exciting roles previously held by other practitioners across the sector. In terms of the impact of this on children's hospices, our findings suggest that advanced nurse practitioners are leading the care of children with increasingly complex and dynamic needs, expanding the services offered by some organisations. Increasing the scope of nurses to include specialist and advanced level practice is not without its challenges. The need to ensure access to clinical supervision (Lee et al., 2023) and ongoing professional development (De Raeve et al., 2024) is essential as a means to ensure congruence between professional scope, service demand and family expectations. Clinical supervision plays a large part in the maintenance of INPs being able to confidently and competently prescribe (Davies, 2023). The provision of peer supervision has allowed new INPs to gain valuable supervision from nurses in a similar role and well as from colleagues from other disciplines, thus giving a broader knowledge base and making valuable links across the multidisciplinary team (Henderson & Bell, 2021).
The challenges of this were noted by participants, particularly by prescribers working in isolated roles or in smaller organisations. The increasingly numbers of children, and the complexity of their conditions, coupled with the increasing reliance of nurses in specialist and advanced level roles means that the assurance of high-quality and regular supervision and access to relevant continuing professional development is more important now than ever before. Ensuring this will allow the continued advancement of nursing practice and therefore assurance that hospice services can continue to grow to reflect the needs of those who rely on their vital palliative care services.
Strengths and Limitations
This study is the first to explore the practices, impact and challenges of independent nurse prescribing, and specialist and advanced level nursing in children's hospices. This research was co-produced by nurses with clinical academic and clinical backgrounds, broadening the design, analysis and discussion of the paper, and reducing subjective bias. However, this paper should be considered alongside the limitations. Although 41 hospices were represented in the study, variations in the workforce, organisational structure and scope, governance arrangements, and the number and needs of children and families in their care, may mean that not all findings are representative of all children's hospices.
Recommendations for Practice, Policy and Research
Nurse independent prescribing has a positive impact on children and their families, prescriber job satisfaction and retention of registered nurses. Children's hospices should support the advancement of nursing practice by supporting independent prescribing. INPs should be supported to develop peer support networks of fellow INPs to help them consolidate and expand their scope, based on the needs of those who rely on care services.
Hospices should enable the continuing professional development of INPs, to optimise their practice, particularly around clinical assessment, history taking and decision making. Formal clinical supervision should be provided for prescribers.
Further research is needed to understand the impact of INP on families, and on the ability for hospices to provide community-based INP from the perspective of families. Research should also explore the impact and potential of advanced-level nursing practice in hospices, and the impact of this on the workforce more widely. In particular, studies exploring practices in hospices with nurse and medical prescribing are lacking. An understanding of how this affects scope, and to identify interprofessional issues would benefit hospices in optimising prescribing practices and advanced level nursing in organisations.
Conclusion
Independent nurse prescribers are making a significant contribution to the medicines needs of babies, children and young people who use children's hospices in the UK, with more nurses working at specialist and advanced levels than ever before. Independent nurse prescribing has a positive impact on children and their families who use children's hospices, on the prescribers themselves, as well as the organisation, in terms of workforce satisfaction and nurse retention. The challenges expressed by prescribers are reduced with effective development opportunities, peer support and clinical supervision, all of which appear to enhance the practice of nurses working with extended scope. The introduction of independent nurse prescribers has enabled hospices to provide greater flexibility in the place of care, offering true choice to families of children with life-limiting and life-threatening conditions.
Footnotes
Acknowledgements
The authors would like to thank Valda Forbes and Natalie Elliot, Clinical Nurse Specialists at Bluebell Wood Children's Hospice, who contributed to elements of the manuscript, but do not meet the criteria for authorship.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.