
Abstract
Little is known about support experiences and needs in the dyads of (1) terminally ill adult children and their parent caregivers and (2) terminally ill parents and their adult child caregivers. The current study aimed at investigating the experiences and needs of adult children and parents in end of life situations regarding their provision and receipt of support. The study employed a convergent parallel mixed-methods design, combining explorative qualitative interviews with the quantitative self-report Berlin Social Support Scales. Sixty-five patients (dyad 1: 19; dyad 2: 46) and 42 family caregivers (dyad 1: 13; dyad 2: 29) participated in the study (02/2018–11/2019). Results show that ill adult children felt less (well) supported than ill parents. Parent caregivers were often limited in the support they could provide, due to their age and health conditions. Hypotheses were deduced from patients’ and family caregivers’ notions to inform dyad-specific recommendations for support interventions.
Introduction
Due to population ageing, an increasing number of adult children are being survived by at least one parent. In addition, it remains a common experience for adult children to be confronted with their parents’ terminal illness. Approximately 4.7 million family caregivers in Germany (Wetzstein et al., 2015) provide care for an ill family member. Family caregivers perform varied and numerous end of life tasks, including managing and coordinating medical care, shopping, performing housework and preparing meals (Navaie-Waliser et al., 2002), providing transportation, and offering personal care and emotional support (Girgis et al., 2013). Family caregivers may also uphold patients’ wishes (Waldrop et al., 2005) and facilitate their passing in a desired location (Ewing et al., 2013; Gomes & Higginson, 2006; Grande & Ewing, 2008).
From the literature on the support experiences and needs of family caregivers at the end of life, we know that they frequently experience care-related burdens (Bijnsdorp et al., 2020; Dobrina et al., 2016; Girgis et al., 2013; Given et al., 2004). However, family caregivers also report positive aspects of the caregiving role, such as satisfaction and happiness with the time spent with the terminally ill relative (Girgis et al., 2013; Grbich, Maddocks, et al., 2001; Grbich, Parker, et al., 2001; Hudson, 2004). Furthermore, we know that the caregiving relationship is often based on reciprocity and mutual support (Benkel & Molander, 2015; Chan et al., 2012; Paul, 1999). The extent of parent caregivers’ involvement has been reported to depend on the family situation, with parents usually less involved in caregiving when the ill adult child has their own family (Benkel & Molander, 2015; Benkel & Molander, 2017). Studies have also indicated that parents may experience their caregiver role as meaningful and cherish the adult child–parent relationship (Dean et al., 2005; Nala-Preusker, 2014; Nelms, 2000; Sohier, 1993). Finally, terminally ill parents and their adult children caregivers may benefit from mutual support, whereby the parent assists the adult child caregiver by taking care of the grandchildren (Chan et al., 2012).
Notwithstanding these first important findings, little else is known about the experiences of providing and receiving support in two particular dyads: (1) terminally ill adult children and their parent caregivers and (2) terminally ill parents and their adult child caregivers. A topical scoping review revealed a lack of (mixed-methods) studies exploring parent–adult child support experiences and needs, highlighting the importance of further research in this area to determine the psychosocial support needs of adult child–parent dyads at the end of life in a range of national contexts. None of the existing studies has included both parent–adult child dyads (Herbst et al., 2020).The present study was embedded in the larger research project Dy@EoL, which aims at exploring the specifics of dyadic interaction at the end of life between terminally ill adult children and their parents (dyad 1) and terminally ill parents and their adult children (dyad 2) (Stiel et al., 2018).
Research Question
The study aims to gain an understanding of the specific end of life support experiences and needs of patients and caregivers within dyads of adult children and parents. Grasping their constructions of their personal situation regarding provided and received support is important for the evidence-based development of recommendations for support interventions.
Methods
Design
The present observational study used a mixed-methods design, embedding quantitative self-report questionnaires in qualitative interviews in a convergent parallel design to provide a more complete understanding of the research phenomenon and meet the complementary strengths and weaknesses of the different methods (Creswell & Plano Clark, 2011). Due to the limited evidence in the research, an explorative design was chosen which draws on the quantitative component in its supportive capacity (Mason, 2006). A semi-structured interview was applied to obtain information on desired levels of support and experiences of providing and receiving support. Quantitative questionnaires were used to elicit socio-demographic details and to measure the cognitive and behavioural dimensions of social support.
Participants
Participants were recruited between February 2018 and November 2019 from one university hospital (via the palliative care unit, palliative consulting service and a press release on the Intra- and Internet), the palliative care unit of an academic teaching hospital, three hospices, three specialised palliative home care teams, one palliative and hospice home care service provider and two general practitioners. Convenience sampling was performed for all known patients in palliative and/or hospice care, as well as their adult children/parent caregivers. Individuals aged ≥ 18 years with sufficient German language skills and cognitive ability to participate and at least one living parent (for dyad 1) or adult child (for dyad 2) were invited to participate in the study by the research team. Individuals were included irrespective of their sex, ethnicity and primary diagnosis. Eligibility was assessed by recruitment partner staff and members of the research team.
All participants were informed about the nature, aim and approximate duration of the study. Patients were given time to ask questions (about, e.g., our reasons for conducting the research), and the presence of family members was facilitated, upon request. Participants were interviewed immediately at first contact or, if they preferred, at an appointed time on another day. If participants appeared overburdened during the interview or when completing the questionnaire, they were provided a ‘time out’. A small gift was offered to participants to acknowledge their voluntary participation.
Qualitative Interviews
A semi-structured interview pertaining to participants’ experiences of social support, perceived roles, communication and burden/relief was conducted (F.A.H, L.G.) until data saturation was reached. Data saturation was determined by constant analysis of the codes abstracted by the research team. The inclusion of patients and family caregivers was stopped as soon as no new codes emerged from the analysis; i.e. as soon as analysis of codes showed consolidated assumptions on participants’ perspectives. Interviews were administered in person in the patient’s room, in one of the recruitment centres, in the project team office, in the patient or caregiver’s home or via telephone. The dyad partner or other relatives were present during some interviews. A flexible interview guide was used, allowing participants to discuss their experiences in their preferred order (Table 1).
Interview Guide (Caregiver Version).
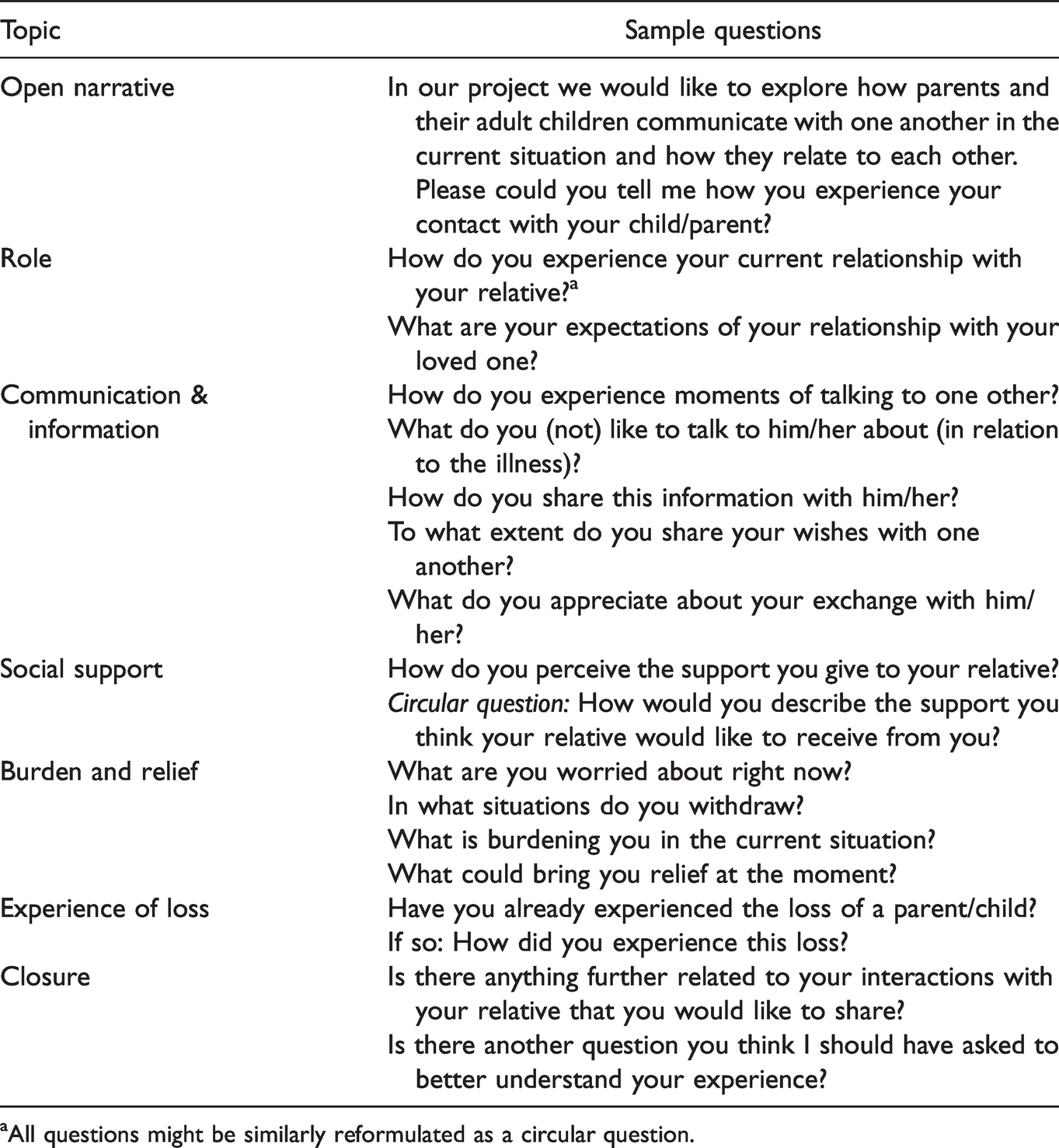
aAll questions might be similarly reformulated as a circular question.
Quantitative Instruments
A socio-demographic questionnaire (patient: 11 questions; caregiver: 14 questions) was administered. Furthermore, dyadic support interaction was investigated using the Berlin Social Support Scales (BSSS) (Schulz & Schwarzer, 2003). The BSSS consists of 52 4-point Likert scale items (1 = strongly disagree; 4 = strongly agree), distributed between 6 subscales (i.e. perceived available support, actually received support [recipient], actually received support [provider], need for support, support seeking, protective buffering) and 1 additional item assessing respondents’ satisfaction with the support. Higher subscale scores (theoretical range: 1.00–4.00) indicate higher levels of the respective dimension of social support.
Data Processing and Analysis
All qualitative interviews were audio-recorded and transcribed verbatim. However, one patient consented to only note taking during the interview; this participant subsequently verified and released the written interview text. Transcripts and interview texts were returned to the participants, upon request. Qualitative data were coded inductively and analysed in MAXQDA (VERBI Software Consult Sozialforschung GmbH, 1989–2020), using a grounded theory approach (Glaser & Strauss, 1967; Strauss & Corbin, 1997). The procedures provided an understanding of patients’ and family caregivers’ construction of their personal situation regarding provided and received support and enabled the researchers to develop hypotheses based on what research participants said and to draw theoretical assumptions. Two researchers (F.A.H, L.G.) independently coded all text. The researchers then developed codes and codings and revised these via consultation. Similar codes were organised into concepts (i.e. subthemes) and further subsumed into higher-level categories representing main themes. Again, discrepancies were resolved in discussion. A third researcher (S.S.) evaluated coding consistency.
Data from the structured questionnaires were analysed in IBM SPSS Statistics 26 (SPSS Inc., Chicago, IL, USA), using standard statistical evaluation tools, in order to provide mean scores, subscale mean scores and frequencies. T-tests were used to determine group differences.
All data were saved in a depersonalised manner. The COREQ qualitative research reporting (Tong et al., 2007) and Good Reporting of a Mixed Methods Study (O’Cathain et al., 2008) checklists were used to ensure comprehensive reporting.
Results
Sample Characteristics
In total, 65 patients and 42 family caregivers participated in the study. The recruitment success rate of patients was 32.8% and of family caregivers 37.8% (Gawinski et al., 2020). Table 2 provides details of all participants and dyads. The mean interview duration was 31.7 minutes (range: 10–78 min). All but five telephone interviews were conducted face-to-face.
Sample Socio-Demographic and Support Characteristics.
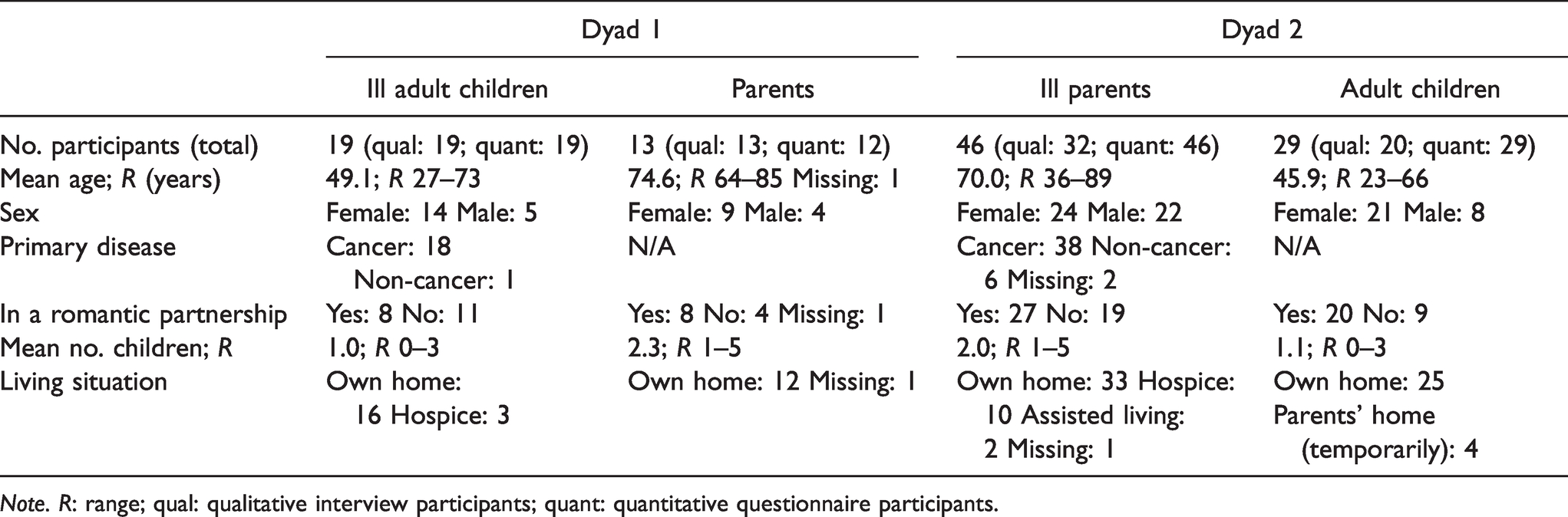
Note. R: range; qual: qualitative interview participants; quant: quantitative questionnaire participants.
One parent caregiver in the dyad 1 group did not fill in the BSSS and socio-demographic questionnaire. Of the 46 ill parents in the dyad 2 group, 5 did not fill in the BSSS and 1 did not complete the socio-demographic questionnaire.
Interview Coding Findings: Support Experiences and Needs in Adult Child–Parent Dyads
The qualitative analysis of the interviews highlighted a main theme of ‘provided, received and desired support’. The nature of the reported support (both given and received) ranged from assistance with nursing and therapeutic activities to emotional and physical attention, general presence (i.e. of the caregiver), minor arrangements to promote the patient’s wellbeing (e.g. provision of extra food), support with bureaucratic tasks and the organisation of the patient’s burial and bequest. One daughter reported that the tasks she provided for her terminally ill father extended beyond their prior relationship: ‘It was just the holding hands or being there, the care with shaving—which I never did before—or cutting fingernails or […] filing toenails’ (A1). Furthermore, a terminally ill daughter described the particularities of the support she received from her father: ‘He is also my battering ram. I can take everything out on him that bothers me’ (P2). Seven core subthemes (concepts) emerged from the analysis:
Patients Supporting (or Wanting to Support) Their Family Caregivers
Patients spoke about how they wanted to do something for their family caregivers in order to give them pleasure (e.g. via a gift) or support them financially. Patients assumed that their family caregivers were helping them as much as they possibly could, despite the terminal nature of their illness. Some patients also consoled their dyad partner. Due to her terminal illness, a daughter struggled to give her elderly mother the emotional support she needed: ‘I have to build my mother up all the time that she moves on, not loses hope’ (P3).
Patients Protecting Their Family Caregivers
Patients reported withholding or concealing information about their illness from their family caregivers: ‘I also don’t want to talk about my illness so much with my children; I don’t want to sadden the children’ (P4). However, they also worried about complaining too much and tried to suppress their tears in the presence of their dyad partner. Both parent and adult children caregivers assumed that patients were trying to minimise their burden. During an interview with a terminally ill daughter and her parents, the mother broke out in tears, imploring her daughter: ‘Don’t spare us! Please!’ (A5). Her husband added: ‘We have just mentioned that we have done a lot, that we were quite tense. [But] we don’t mind coming here. And if we just come for an hour, we don’t mind’ (A6).
Family Caregivers’ Limits in Their Support
Some family caregivers were hampered in their ability to support their loved due to other family commitments or – particularly in the dyad 1 group – the parent caregiver’s own age or poor health: ‘that’s just very difficult, because she can’t support me because she’s so old […] and doesn’t understand that [the terminal illness situation] either and is of cause sorrow-stricken’ (P3). A caregiving mother said: ‘We’re at the end of our rope; we’re also [in the seventies]’ (A5). Living far away from the patient and – particularly in the dyad 2 group – having work commitments or small children to care for were also described as practical restrictions for caregivers. Lack of nursing skills was also considered a hampering factor. An adult son expressed his personal limits regarding the bodily care he was willing to provide to his mother: ‘But now with putting lotion on her body and so on, everything is still okay and changing plasters. But this is the limit’ (A7). Family caregivers in both dyad groups expressed feelings of guilt and concern over their personal limitations in the support they were able to provide.
Patients Resisting/Rejecting Their Family Caregivers’ Support
Some patients denied or did not allow their dyad partner to provide support; others simply felt uncomfortable with their dyad partner’s support or were reluctant to accept it. One caregiver assumed: ‘Maybe that’s a little bit of shame. […] My mum has to be here with me’ (A8). An ill adult daughter remarked: ‘In the beginning it worried me that my mum has to be there for me now, that she has to support me in this way’ (P9). Another patient felt hemmed in by her clucking mother and expressed her desire to spend more time with her partner and alone, seeking ‘a little more freedom’ (P10). Patients also felt guilty about drawing on their parent/adult child’s support, which they assumed to cause their caregiver a lot of trouble. An ill father stated: ‘I regret the fact that he [his son] had to give up his profession because of this [to care for the patient]’ (P11). Finally, some patients assumed that their family would not be willing to provide the amount of support they wanted.
Patients Relying on Their Family Caregivers’ Support
Patients claimed that they could rely on their dyad partner for support: ‘If there’s anything, she is always approachable. […] I was hoping before I came here [the hospice], I’d get the schedule from a funeral home. […] She [the patient’s daughter] spontaneously said: “I’m coming with you, mum”’ (P12). This reliable caregiving was echoed by a caregiving father: ‘I’m there for my daughter. She can wake me up at 12:00 at night or at 3:00, I get up […] and then I’m ready to go’ (A2). Family caregivers also reported observing the patient’s health status and addressing complaints to physicians or actively demanding medical support.
Patients Depending on Their Family Caregivers’ Support
Some patients depended on their dyad partner for support. Indicative quotes included: ‘I’m certainly dependent on my mother at the moment’ (P13) and ‘Taking a shower right now, I have no confidence in myself. […] And it’s important for me that mummy is around […] if something were to happen, that someone would stand next to me immediately. Before I didn’t need anyone, especially not my mother’ (P9).
Desired Professional Support
Asked to report the professional support they desired for themselves or their dyad partner, patient and caregiver responses varied widely. Specifically, respondents requested greater: (a) support for the dyad, (b) support for the patient and (c) support for the caregiver. Regarding support for the dyad, respondents requested joint activities such as therapy with the dyad partner and family convalescent care. With respect to support for the patient, patients requested greater practical help in the household. Furthermore, some family caregivers thought that patients would benefit from psychosocial support in coping with the illness. Others wanted their ill dyad partner to be offered opportunities for exchange with other terminally ill patients – also because they felt emotionally exhausted from providing support. Finally, patients reported unfulfillable wishes that they had not communicated to their dyad partner. In relation to caregiver support, both patients and caregivers voiced the need for psycho-therapeutic and pastoral care. In the dyad 1 group, specifically, ill adult children requested greater general support for their aged parents: ‘My mother is [… old] and herself needs support’ (P3). Also, the issue of prospective nursing care was broached.
Questionnaire Findings Regarding Social Support
Of note, the BSSS data showed that ill adult children perceived significantly less support (relative to the support actually received) than did ill parents (see Table 3 for significant BSSS differences). Moreover, ill adult children were less satisfied with the support they received, compared to ill parents.
Significant Differences in BSSS Scores Between Patient and Caregiver Groups.
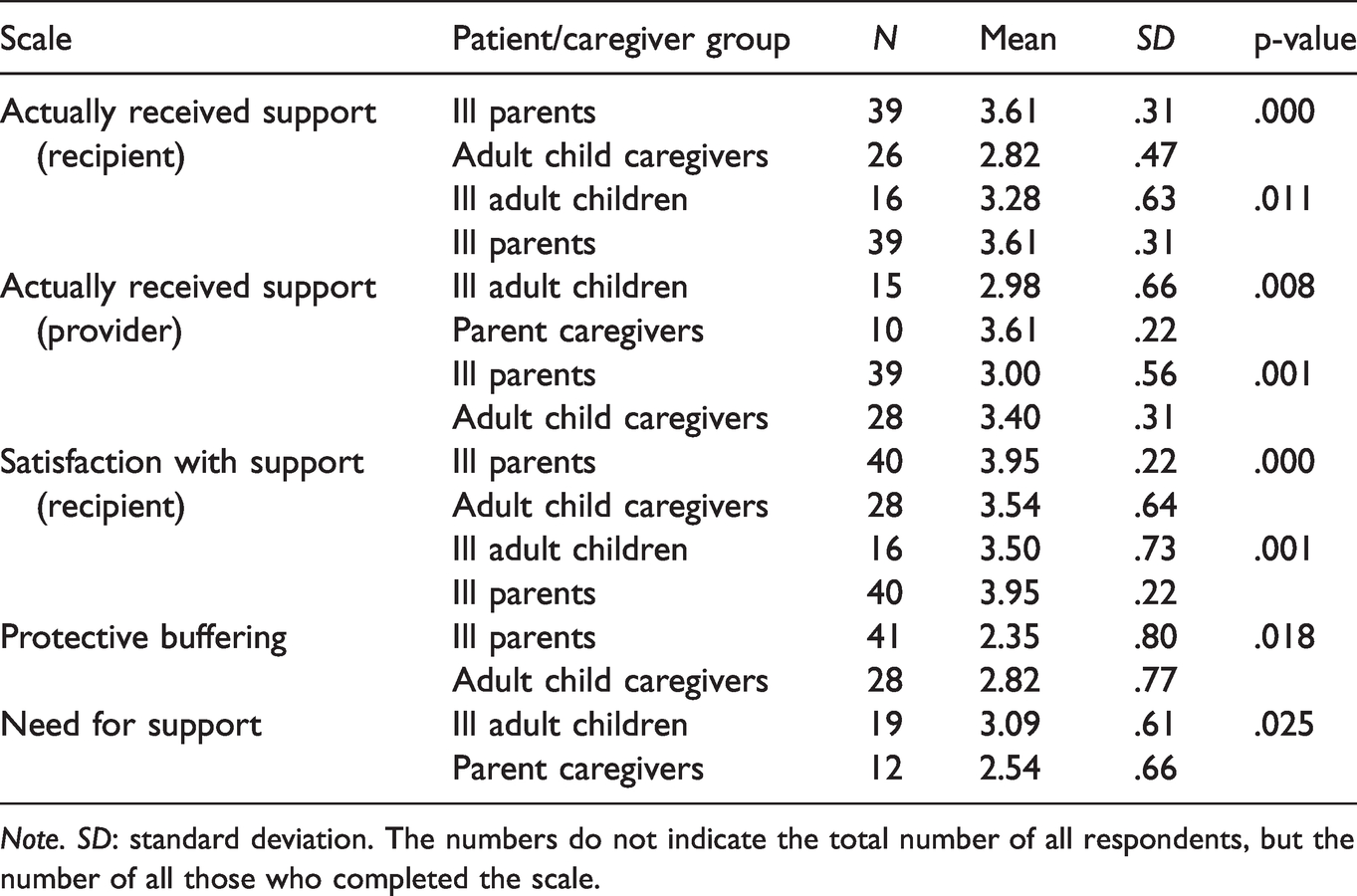
Note. SD: standard deviation. The numbers do not indicate the total number of all respondents, but the number of all those who completed the scale.
The BSSS results show that ill parents perceived a higher level of actually received support than did adult child caregivers. Their satisfaction with the received support was also higher than that reported by the adult child caregivers.
In the dyad 1 group, ill adult children perceived a lower level of actually provided support to their parent caregivers than parent caregivers reported providing to their ill adult children. Regarding the dyad 2 group, ill parents perceived significantly lower support provided to their adult child caregivers than adult child caregivers reported providing to their ill parents.
Ill adult children reported a stronger need for support than their parent caregivers. Finally, adult child caregivers reported higher levels of protective buffering (i.e. from bad news) in their support than did ill parents.
Hypotheses
Combining qualitative interview results and quantitative BSSS results led to the following hypotheses: The parent wants to be closer to the patient, whereas the patient desires more freedom and autonomy (dyad 1). The patient perceives that the parent is substantially burdened and overwhelmed and has the feeling of having to support the parent (dyad 1). The patient sees limits in the support of the parent and wants to spare the aged parent; the support of the patient is exhausting for the aged parent and goes beyond his or her strength (dyad 1). The bodily care required goes beyond the previous parent–child relationship. This can create new intimacy on the one hand, but is also rejected by the patient or the adult child on the other hand (dyad 2). The adult child is only able to support the patient to a limited extent because the adult child cares for the patient from a spatial distance (dyad 2). The patient appreciates the adult child’s commitment, but does not want to burden the adult child too heavily and understands that the adult child has other obligations (dyad 2).
Discussion
The present study adds to the literature on patient and caregiver support experiences and needs by explaining the specifics of two dyadic constellations: terminally ill adult children and their parents (dyad 1) and terminally ill parents and their adult children (dyad 2).
Results from the BSSS showed that ill adult children felt less supported and less satisfied with the support they received from their parent caregivers than did ill parents, with respect to the support they received from their adult children. The interviews indicated that parent caregivers may be limited in the support they are able to provide, due to their age and health conditions. We suggest that ill adult children’s feelings of less support from their parent caregivers may be associated with their perception of parental end-of-life support as awkward or unnatural (Van Humbeeck et al., 2013), preferring support from their partner or children, instead.
Another interesting finding is that, in both dyad groups, patients perceived lower levels of support provided to caregivers; additionally, in the dyad 1 group, parent caregivers reported lower levels of (satisfaction with) the support they received than did ill adult children. This finding is consistent with the results of Spatuzzi et al. (2020), who found that elderly caregivers were at higher risk of experiencing burden than their younger counterparts. Interestingly, in our study, patients appeared to be aware of the strain that caregiving placed on their family members; patients in both dyad groups wanted to protect their caregivers from burden. The literature on informal caregiving demonstrates that family caregivers often feel an obligation to provide support to their loved ones, connected with a physical and emotional burden (e.g. guilt) (Choi & Seo, 2019; De Korte-Verhoef et al., 2014; Grant et al. 2013; Grunfeld et al., 2004; Higginson et al., 2010; Saria et al., 2017; Townsend et al., 2010). From the socio-demographic data we also know that four adult child caregivers in our study temporarily moved to their ill parent’s home to provide support. This included adult children from foreign countries who faced the uncertainty of leaving their families behind for an undefined period of time. However, caregivers also report rewarding aspects of caregiving (e.g. providing good care to their loved one) (De Korte-Verhoef et al., 2014). Supporting a family member and declining the support offered by a family caregiver are closely linked with these issues, as reflected in the present findings. Looking at our results from a more general angle, the quantitative and qualitative data call for family caregivers’ unmet needs in the palliative care trajectory to be addressed as part of standard practice (Hudson & Payne, 2011; Sullivan et al., 2019; Tarberg et al., 2019). Moreover, patients’ feelings of being a burden deserve more attention (Roest et al., 2020). The results of the present study are applicable to health care practitioners, as they buttress Dobrina et al.’s (2016) request to ‘consider the degree of kinship and profile of family caregivers […] to arrange each unique patient–caregiver unit’s support’.
Strength and Limitation of the Study
The major limitation of the present study is its inability to generalise to all terminally ill adult child–parent and terminally ill parent–adult child dyads, as patients and caregivers may experience their situation and support needs differently, depending on their subjective configured histories and particular contexts.
The strength of the study pertains to its varied sample, including participants from a diverse range of backgrounds and ages, with the youngest terminally ill child aged 28 years and the eldest ill parent aged 89 years; similarly, the youngest adult child caregiver was 23 years of age and the eldest parent caregiver was aged 85 years. Diversity was also found in the relationship status; slightly more than half of the patients (53.8%) and two thirds of the caregivers (68.3%) were at the time of their study participation in a romantic relationship.
Conclusion
The family environment, interaction with relatives and psychosocial support have a fundamental effect on the quality of life of terminally ill patients and their perceived burden on family caregivers. The present study disclosed the specific support experiences and needs of parent–adult child dyads. The findings support the claim that patients’ feelings of being a burden deserve more attention; they also support the call to address family caregivers’ unmet needs in the palliative care trajectory as part of standard care. Hypotheses were deduced from patients’ and family caregivers’ notions to inform dyad-specific recommendations for support interventions. One recommendation will likely advise the palliative care team to elicit together with caregiver and/or recipient in which ways care can be shouldered by more than one family member. Regarding the ill parents in our study, our socio-demographic data showed that they have a mean number of two children.
Supplemental Material
sj-pdf-1-ome-10.1177_00302228211008748 - Supplemental material for ‘She Can’t Support Me Because She’s so Old’: A Mixed-Methods Study of Support Experiences and Needs in Adult Child–Parent Dyads at the End of Life
Supplemental material, sj-pdf-1-ome-10.1177_00302228211008748 for ‘She Can’t Support Me Because She’s so Old’: A Mixed-Methods Study of Support Experiences and Needs in Adult Child–Parent Dyads at the End of Life by Franziska A. Herbst Laura Gawinski, Nils Schneider and Stephanie Stiel in OMEGA—Journal of Death and Dying
Footnotes
Acknowledgements
The authors gratefully thank all adult children and parents for their participation in this project.
Authors’ Contributions
F.A.H. (female), a medical anthropologist working as a senior researcher, led the study, collected and analysed the data and wrote the manuscript. L.G. (female), an anthropologist working as a researcher, collected and analysed the data. N.S. supervised the research process. S.S. (female), a psychologist working as a senior researcher, wrote the grant application, developed the study design, reviewed the consistency of the qualitative data and supervised the research process. All authors revised the manuscript critically and approved the manuscript for submission.
Consent for Publication
Individual written informed consent for the research team to publish the study results was obtained from all patients and family caregivers.
Ethics Approval and Consent to Participate
This study was performed in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Hannover Medical School: no. 7610, 04/10/2017. Individual written informed consent to participate was obtained in writing from all participants.
Data Accessibility Statement
The datasets analysed in this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was part of the larger project ‘Dy@EoL – Interaction at the end of life in dyads of parents and adult children’, financed by the German Federal Ministry of Education and Research (BMBF) (grant nr 01GY1711). The funder did not play any role in the study design, collection, analysis or interpretation of data or in the drafting of this article.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.