
Abstract
This study explored men's experience of miscarriage. Semi-structured interviews were conducted with ten men with personal experience of miscarriage, analysed using Interpretative Phenomenological Analysis. Three superordinate themes emerged: ‘This is happening…we’re pregnant!’ captures how men were invested in the pregnancy from either preconception or conception; ‘Left with empty arms, what now?’ uncovers what happened during and following miscarriage; and ‘men feel the loss too, you know’ demonstrates how men crave recognition and appreciation of the loss. Insights are given into the impact that miscarriage has on men and the planning of their families thereafter. We hope the findings enhance health professionals’ understanding of men and miscarriage and assist in challenging both the taboo nature of the topic and outdated, unhelpful stereotypes. Recommendations for future research are provided.
Introduction
Miscarriage is the early loss of a pregnancy. Definitions that distinguish miscarriage from stillbirth vary, but in the United Kingdom the cut-off is 23 weeks gestation (National Health Service, 2015). As many miscarriages happen before the pregnancy is recognised, the exact prevalence is unknown, but between 15% and 20% of clinically confirmed pregnancies end spontaneously before the 13th week (National Institute for Health and Care Excellence, 2014). These ‘early’ miscarriages are more common than ‘late’ miscarriages (14 to 24 weeks gestation). Over 80% occur within the first trimester (Dante et al., 2013).
Markin (2017) suggests that the modern world views miscarriage as a medical rather than psychological event. Yet pregnancy loss is an ambiguous loss: the concurrent physical absence, yet psychological presence, of the infant (Boss, 2004). Multiple layers of loss are involved: the pregnancy identity; the hoped for and dreamed about child; and expectations and plans about becoming parents (Boss et al., 2011; Brier, 2008; Schultz & Harris, 2011). Unlike late miscarriage and still birth, early pregnancy loss has little or no culturally sanctioned grief process, what Doka (1989) coined ‘disenfranchised grief’. Little is known about men's grief following pregnancy loss, as most existing literature and subsequent bereavement care guidelines have focused on women (Nguyen et al., 2019; Obst et al., 2020).
Quantitative research has focused on examining gender differences. Findings include how men are less psychologically impacted (Kong et al., 2010) and grieve less intensely and enduringly than their partners (Beutel et al., 1996) but are more likely than women to deny the loss (Stinson et al., 1992). Women display more sadness, crying, and preoccupation with the loss compared to men (Stinson et al., 1992). There has been criticism that measures such as the Perinatal Grief Scale (PGS; Toedter et al., 1988) measure grief in particularly ‘feminine ways’ (Stinson et al., 1992).
Qualitative research demonstrates that men believe their role in miscarriage is one of support, which often means supressing their emotions through the use of avoidant coping strategies, including increased alcohol consumption compared to women (e.g., Beutel et al., 1996; Jones et al., 2019; Meaney et al., 2017; Murphy, 1998). Some research offers female quotes as evidence for themes (e.g., Meaney et al., 2017), are skewed toward reporting women's narratives (e.g., Abboud & Liamputtong, 2005), or report extracts jointly; making it difficult to distinguish which comments belong to women or men, neglecting the male perspective.
Research includes a range of pregnancy losses such as spontaneous abortion, ectopic pregnancy, stillbirth, or neonatal death (e.g., Due et al., 2017; Nguyen et al., 2019; Obst & Due, 2019; Stinson et al., 1992); termination of pregnancy for nonviable foetal anomaly e.g., Obst et al. (2020, 2021); or ‘late’ miscarriage (i.e., 14 weeks gestation and beyond, e.g., Johnson & Puddifoot, 1996) and therefore does not specifically focus on ‘early’ miscarriage.
This study aimed to specifically capture men's experiences of ‘early’ miscarriage.
Method
Interpretative Phenomenological Analysis (IPA) was utilised, a qualitative research method concerned with the detailed examination of lived experience (Smith et al., 2009). IPA is grounded within the philosophies of phenomenology, hermeneutics and idiography. A key aspect of the approach is the exploration of individual experience and meaning (Langdridge, 2007).
A homogenous purposive sample was sought of men who met the following inclusion criteria: aged over 18; good understanding of spoken English; personal experience of miscarriage before 24 weeks gestation in the past two years. Ethical approval was granted from Teesside University School of Health and Social Care Research Governance and Ethics Committee and the Health Research Authority.
The charity ‘Tommy's’ assisted in the recruitment of participants by posting a ‘recruitment briefing’ on their social media page. A participant information sheet was emailed to interested men and informed consent was gained. All interviews were audio-recorded by the researcher (first author) and transcribed verbatim.
All participants chose to take part in a video call interview which lasted between 30 and 90 min (mean length 78 min). Semi-structured interviews were used to invite detailed, rich, personal accounts of each participant's experience through open-ended questions (Smith, 2011; Smith et al., 2009). Following each interview, participants were debriefed and agreed to be contacted again for participant validation of the themes.
The interviews were analysed using the six steps of IPA described by Smith et al. (2009): reading and re-reading the transcripts; initial noting; developing emergent themes; searching for connections across emergent themes; moving to the next case; and looking for patterns across cases.
Given the researcher's interpretative role (Smith, 1999), biases and expectations about the study findings were recorded prior to collecting data. Furthermore, attending closely to participants’ words during the interviews and maintaining a reflective diary facilitated in ‘bracketing’ the researcher's hunches or theories (Smith et al., 2009). Reflective diary excerpts are available from the corresponding author to inform the reader of the researcher's assumptions and beliefs and accordingly how these may have impacted on the research itself.
The second and third authors separately analysed two transcripts each. All authors reached agreement that the emergent themes were both credible and valid. Any additional or alternative interpretations, as well as any reflective comments, were discussed with the first author and incorporated within the analysis. A summary of superordinate and subordinate themes was then discussed, resulting in revisiting the data in order to reconsider the superordinate themes. Following this, superordinate and subordinate themes were agreed between all authors.
Results
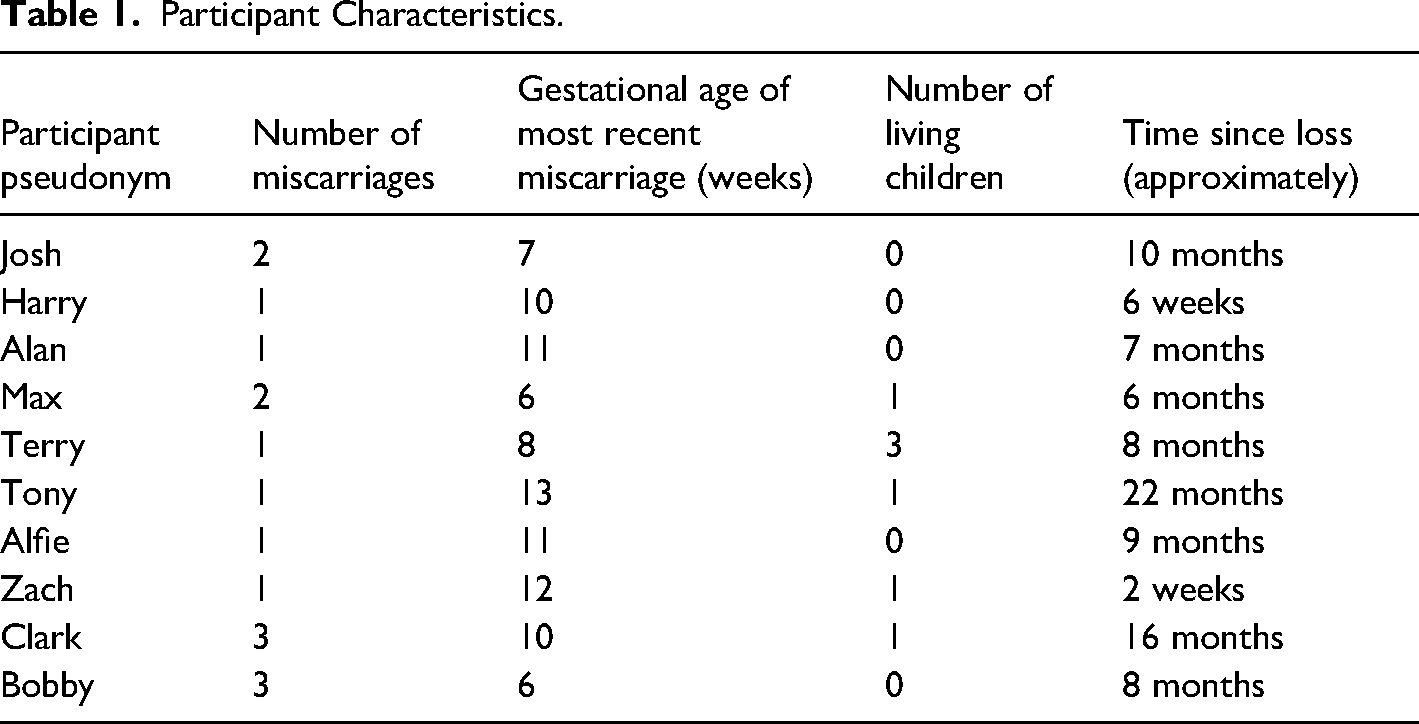
Ten white British men aged between 25 to 49 years (M = 33.8 years) participated. All were in professional occupations and were either married or cohabiting with the partners they had experienced the miscarriages with. Miscarriages experienced ranged from one to three, over half experienced one miscarriage (n = 6). Half of the sample had children whilst the other half did not. Time since loss and taking part in the study ranged from 2 weeks to 22 months; however, eight of the ten participants fell within the range of 10 months ago or less. See Table 1. Pseudonyms have been used to protect participants’ privacy and any identifiable information omitted.
Participant Characteristics.
The themes that emerged are presented in Figure 1. Once emergent themes identified in individual transcripts appear within at least half of the other transcripts, they are categorised as recurrent themes (Smith et al., 2009). This promotes an idiographic perspective, whilst also counterbalancing this perspective with more generic accounts across the transcripts. A superordinate theme is a construct which usually applies to each participant, but which can manifest in different ways within the cases (Smith et al., 2009); thus showing what the participants share, as well as illustrating their individuality. In accordance with this guidance, all three superordinate themes were present in all participants’ transcripts. In addition, the subordinate themes: Thinking about the future; Grief and loss hits hard; I must support her; and Opening up the conversational arena were present in all participants’ transcripts. The remaining subordinate themes were present in at least half of the transcripts.
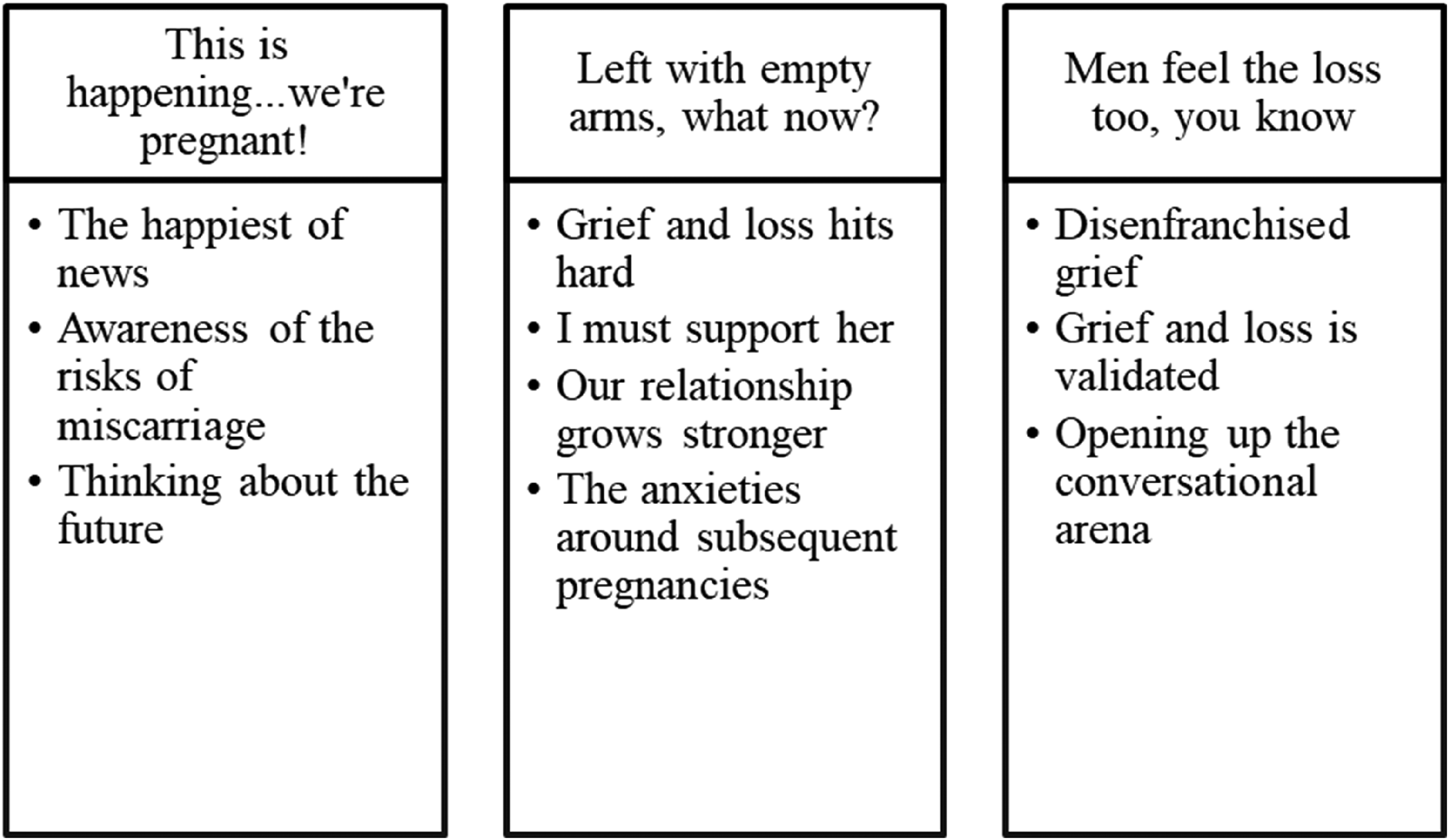
Superordinate (headings) and subordinate (bulleted) themes.
In order to ensure that the data analysis process is transparent and committed to quality, participant quotes are included as frequently as possible. A table of additional evidence is available from the corresponding author, as are transcripts documenting the analysis process. All participants reviewed the results of the analysis and all agreed that the themes adequately reflected their experiences.
This is Happening…We're Pregnant!
Participants were invested in the pregnancy. The possibility of miscarriage was either not recognised or was held with some trepidation.
The Happiest of News
Nine participants conveyed the importance of conception in their pursuit of a longed-for child. For some, conception was quick to happen which communicated a sense of luck or a sign that all would be well: …you hear stories about people trying for years and years and years…needing IVF treatment … so we thought it would be at least a few months but yeah, straight away. (Josh)
For others it had taken longer and led them to question the viability of conceiving: … when you're [a] good couple of months down the road you … [you] start to consider…whether it can happen. So when it happened, yeah, absolutely over the moon. (Harry)
Similar doubts led to consideration of medical intervention: …we've been sort of chatting to the doctor about whether we might end up going down the IVF road…but went away on honeymoon and we got pregnant …it kind of felt quite, quite special…like [I] say we've been sort of been trying for a while. (Max)
The participants clearly communicated their sense of happiness and excitement that the pregnancy was actually happening.
Awareness of the Risks of Miscarriage
Four participants were aware, and three were unaware, of the potential risk of miscarriage. Alan worked as a GP and was especially risk aware: …because of my job [I] knew that [a] high proportion … don't end up…going all the way to term. So [we] didn't go around telling everyone … because having the reverse conversation is even more horrible. (Alan)
Alan was protecting himself emotionally as he understood the potential difficulty in having to tell others a pregnancy had ended prematurely. Tony employed a similar protective strategy, but his awareness was due to a previous loss: …we knew that things go wrong …we didn’t invest as much emotionally in it [the pregnancy]. (Tony)
In contrast, Bobby was distanced from such thinking: …you don't decide you're going to have, to start trying for a baby and…like anything like this [their miscarriage] would happen. (Bobby)
This was a similar experience for Clark: … we were really excited… miscarriage never even crossed our minds at all. (Clark)
Awareness of miscarriage served to guard against investing too fully in the pregnancy in an attempt to protect oneself emotionally. Others had no reason to doubt that investing in the pregnancy was a safe thing to do.
Thinking About the Future
All participants had thoughts and/or images about the future: … you start, start skipping ahead to like all, wonder what we'll call them and what they [will] be like and what will they enjoy… (Max)
Some felt able to consider naming the baby at this early stage: …I think we quickly settled on… [x] … [we] found out the gender early on… (Tony)
Others also talked of how visual confirmation of their baby through an ultrasound scan enabled them to identify as dads: In my head…it was, I’m a dad …we’re pregnant and I’m going to be a father …. (Josh)
However, one participant reflected on how being assigned such a title by midwives was not in keeping with his felt identity at that stage: … it's presumptive…obviously for people that miscarried it's not, and actually for the dads it's not … (Alan)
Early in pregnancy, participants acknowledged the baby and with this came adjustments, planning and imagined futures. The majority did, in some sense, identify as fathers early in the pregnancy. This new role was met with a sense of responsibility and planning.
Left with Empty Arms, What Now?
When describing their experience of miscarriage, men described feelings of grief, loss, and adopting a supportive role. The strengthening of the partner relationship and future family planning were also described.
Grief and Loss Hits Hard
All described immediate and intrusive, re-emergent and chronic grief reactions alongside loss of control, a child, fatherhood, and/or an imagined future.
Josh described overwhelming emotions and the sense of injustice and helplessness; his use of the word ‘ripped’ illustrates the felt brutality: … I just cried … just constantly like, which I have never done before … I had that such deep attachment, to have that just ripped away, it was horrible… (Josh)
Anger was also described: … really, really pissed off at the world to be honest and that's what really still takes me by surprise [as] to how angry I feel about other people having children … (Tony)
For Alfie, anger was directed inwards escalating to thoughts of suicide. Fortunately, he received psychological support: … a lot of… anger, and it was…all turned inwards…I was actually thinking of taking my own life at one point … (Alfie)
Participants discussed how hard the loss was felt when observing others and making comparisons: … still when we see our friends and they've got young babies…I try and not let it upset me… or let it treat my friends in a different way, because … it's not their fault.” (Alan)
Feelings of lost fatherhood faced others: … facing into not becoming a father … just never questioned it … maybe I'm really not going to be a dad and…that being something quite core to who I was for a long time … facing the reality of it not, maybe not happening … (Max)
Participants described the grief felt at the loss of their baby's imagined future: …I didn't think about it as you've lost an embryo … no, you’ve lost a baby … the future's gone and it's kind of grieving for that loss of what could have been … (Max)
…it was absolutely horrible… you have this weird thing of missing something you never really had and just getting like, confused and angry because why am I feeling like this? … (Bobby)
Terry described how the grief continues for him: … it hit me really hard … just how much that attachment to the idea, if not the actual potential person that I had formed… the grief is massive and still goes on … (Terry)
All participants therefore described a myriad of grief reactions in varying degrees at being left with empty arms.
I Must Support Her
All participants described needing to support their partner, often instinctively and at the expense of their own needs: [When he was told they could not find a heartbeat] … I remember at that point, kind of trying to hold it together…for [partner's name] … (Zach)
Hiding their feelings, so as to appear to be strong, was reported: … [partner's name] was very…upset, I was obviously very upset, but kind of trying to hold it together…and be strong I guess. (Max)
For some the physicality of miscarriage prioritised their partner's needs before their own: … [be] as strong as I could … because … you’ve not had any of the physical sort of repercussions of previously having a miscarriage and losing the baby and brutally having gone through pregnancy as well. (Tony)
Participants reflected on how the physical aspect of miscarriage entitles mothers to more support: … it's not physically happening to you … the miscarriage happens to [partner] and I'm just there to help her through it … it's like being … a backseat driver when things start to go wrong … you’re there in a support role in its entirety and that's all your contribution can be … (Bobby)
Others described how their needs were put on hold whilst waiting for the miscarriage to complete: I thought if I look after her then, you know, that that's me doing my job. I can grieve later on … my grieving took place over the next couple of months … (Alfie)
Thus, all participants viewed their role as supporting and be ‘strong’ for their partners during and following miscarriage. For some, this was to the detriment of their own needs being met.
Our Relationship Grows Stronger
Seven participants described how, following the miscarriage, their relationship became stronger. Most reported that it brought them closer together. Three participants either did not discuss relationships or discussed a negative impact.
Alan acknowledged that the miscarriage could have impacted negatively on his relationship, but instead they chose to help each other: I think it kind of pushed us together rather than apart. I know some people, you can find that it drives a wedge between people when bad things like this happen, but I think that we sort of helped each other through it … (Alan)
Others described relationship growth and a team effort: It's actually brought us closer together… because we were both there for each other it's helped us grow stronger as a couple … she said we have been through hell in the last few months, but there's nobody I'd rather have gone through it with. (Alfie)
For these participants it was paramount that they ‘stuck together’, often because only they could appreciate the hurt the other was experiencing.
The Anxieties Around Subsequent Pregnancies
Nine participants described feeling anxious about potential pregnancies, current pregnancies or successful births. One participant made no reference to future pregnancies.
Participants described the real possibility of another miscarriage: …we both decided…to wait a little bit … we wanted to emotionally get to a state where we can accept getting pregnant again and thinking about the realistic possibility of things going wrong again … (Josh)
Some accepted that further miscarriage was something they had no control over and had thus considered alternatives: … [IVF] puts a lot of pressure and stress on relationships and marriages, [it] can become very all-consuming. So, if we ever get that scenario… we’ll just adopt and have a kid that way … there's a chance that she'll get pregnant naturally again. There's a chance it might succeed. There's a chance it might end in miscarriage or she might never get pregnant again … and I kind of accept that. (Alan)
Those men whose partners were pregnant at the time of the interview described significant anxiety: … it's been hell … joy because the baby is coming, but dread because of what we've been through before … every day my partner will get very upset and distressed looking for signs of, is this normal…? (Alfie)
A mixture of pregnancy loss and heightened anxiety in a subsequent pregnancy led others to question their ability to endure a further pregnancy: …it's probably made me a little bit wary about trying again. (Max)
… this [miscarriage] just kind of confirms to me that I definitely can't go through with it again … I still don't want to try again. (Terry)
Future, current, and subsequent pregnancies following loss are entrenched in anxiety to varying degrees.
Men Feel the Loss Too, You Know
Participants reported their grief was disenfranchised and/or validated. All participants recognised how miscarriage, including men's experiences, needs to be recognised and discussed more openly.
Disenfranchised Grief
For eight participants, grief was either not considered as a felt experience, or they were marginalised in their grief in favour of their partner's experience. The medical terminology used by health professionals undermined their felt experience that death had occurred, and at times unhelpful clichés were offered. Participants reported a lack of emotional support and unmet needs: …even the NHS one [website] … was directed at, to the female, not like a couple's thing or as a man what can you expect, what can you do to help, what, where can you get help if you need it … (Josh)
…everyone [at work] knew but no one talked about it … just a kind of, a nod, “you alright?” …and then you get on with it. (Tony)
Participants felt disenfranchised by healthcare: I don't think I once heard anything about … death or dying or dead … what I did notice was that they [healthcare] stopped referring to … it really as any kind of baby or embryo … they started just talking about … ‘pregnancy debris’ or something … they used a lot of words that try to maybe depersonalise it and make it a pregnancy rather than a person.” (Zach)
Unhelpful clichés were offered by others: … when people were trying to be like consoling you and saying ‘oh well, everything happens for a reason’. I'm like really, give me one good reason why that [miscarriage] should happen to anyone, why someone should have to go through that three times … it pissed me off in its entirety… (Bobby)
…we go around [partner's] family and they’d be like … ‘well it's not a baby, so why would you be so upset and it's just like having a heavy period’. (Clark)
…people of a certain generation like my mum and [partner's] mum … very much of the opinion that you know these things happen and it was a kind of a brush under the carpet attitude… (Terry)
Clark further reflects on the difficulty of this type of loss: …there's nothing to miss and I think that was the hard thing is that it's a different sort of loss …you’ve got no memories, but what you have lost is potential memories … that sometimes is a little bit harder I think. (Clark)
Evidently, the loss of a baby was not understood by healthcare professionals, family, friends and work colleagues. Being male either meant men should not feel the grief and loss like their partner, or all support was directed towards the women.
Grief and Loss is Validated
This illustrates the divergence in the data, as seven men felt validated in their grief: … we got this whole flood of really nice messages and cards and flowers … really nice to get that influx of love… (Josh)
For others, memorials or a place to visit were important in validating their loss: …we had two babies that we never got to meet … and that's why we have two little plaques down at the crematorium, we go there every now and then. (Tony)
… they [hospital staff] said…batch cremation … [that was] fine…we would know where it is if we want to go back…and visit. (Zach)
Some participants were offered, and some accepted, counselling: … she [health professional providing post loss debrief] made a point of talking to me several times and … she said ‘don't forget your role in this and your feelings towards this, it's important that you're not forgotten’ and I wasn't expecting that at all … (Harry)
Acknowledgement that a loss has occurred following miscarriage was a validating experience.
Opening up the Conversational Arena
All participants found new ability to discuss their experience, in the hope of helping others. Some advocated that the taboo surrounding miscarriage needs to be lifted and men's experiences acknowledged. This involves challenging gender stereotyping which often prevents men discussing miscarriage: It's so common that you'd think it would be more commonplace to talk about it … you have to change a whole generation of people's way of thinking and talking about horrible things and it's a very difficult thing to change. (Alan)
Some spoke of the need to break the silence around miscarriage in general, but specifically how men experience it and other mental health issues: …men don’t speak about anything mental health … it's just that stigma isn't it, that your meant to be the strong silent one that just battles through and ploughs on… (Bobby)
And that societal level change is required: …more males talking about it [miscarriage] openly about…how it affected them … more needs to be said from the male point of view … (Harry)
…the main thing is about acknowledging that there's generally two people involved in the miscarriage …frustration of not feeling that you can actually say to someone you know, ‘do you realise that was my baby as well?’… (Clark)
I've been striking off lots of conversations…to try and promote a bit of chat about miscarriage among blokes… (Terry)
Participants articulated the need to open up the conversation and increase societal awareness, otherwise men's experiences will remain unacknowledged and their needs unmet. There is a need to break the silence around men and miscarriage; and men are willing to help challenge outdated preconceptions.
Discussion
Little attention has been paid to how men felt about a pregnancy prior to miscarriage. Participants reported feeling happiness and excitement as they considered it may take time to conceive and if it happened unexpectedly quickly, or if they perceived potential difficulties that did not then ensue. These findings build upon the reproductive story model (Diamond & Diamond, 2016), by highlighting that men may also have thoughts about how their conception journey may unfold and can be emotionally invested early in the pregnancy. Some men are aware of the risks of miscarriage and employ strategies to protect themselves. Others, like Meaney et al.'s (2017) participants, felt naive about miscarriage, and were unaware of the risks.
Following miscarriage, participants were shocked to learn of the prevalence of miscarriage, supporting Maker and Ogden's (2003) assertion that miscarriage is typically an unexpected event. Whether or not participants were aware of the risks, all participants reported thinking about the future. The pregnancy had started to have a psychological and emotional presence for participants. Some began identifying as fathers in early pregnancy, illustrating that parental identity and bonding can occur on a conceptual level before any scan occurs. This contradicts previous research which suggests that bonding for fathers commences after an ultrasound scan (e.g., Beutel et al., 1996; McCreight, 2004; Puddifoot & Johnson, 1999; Serrano & Lima, 2006) or birth (e.g., Peppers & Knapp, 1980). Participants talked of an imagined future with the baby, lending support to previous findings that expectant parents hold visions, hopes, dreams, internal representations and expectations about the idealised child, and becoming parents (e.g., Boss et al., 2011; Diamond & Diamond, 2016). It has been suggested that, as fathers do not physically carry a child, attachment begins after birth (e.g., Peppers & Knapp, 1980) yet participants reported forging attachments to their unborn child in the first trimester, thus refuting the ‘paused’ attachment idea (e.g., McGreal et al., 1997; Puddifoot & Johnson, 1997). As in Abboud and Liamputtong's (2003) study, the men experienced intense feelings for some time after the miscarriage. This contradicts Johnson and Puddifoot's (1996) finding, that men's grief is largely felt in the short term.
All participants described how grief and loss hits hard in the very early stages of pregnancy. Reference was made to a range of grief responses, contradicting the popular misconception that early pregnancy loss has little significant emotional impact (e.g., Covington, 2005). There has been criticism that measures, such as the PGS, assess grief largely in terms of typically female responses (e.g., Stinson et al.,1992), without consideration of maladaptive symptoms and behaviours that can often emerge in men, such as substance abuse, alcoholism, anger, or guilt (Jaffe & Diamond, 2011; Martin & Doka, 2011). Anger and jealousy were vocalised by the participants in this study, lending support to this criticism.
Immediate and intrusive, re-emergent, and chronic grief reactions were described, supporting the assertion that miscarriage can be traumatic and psychologically distressing (Rinehart & Kiselica, 2010; Swanson, 2000). The men reported a loss of control, of a child, of fatherhood, and/or an imagined future, supporting previous findings that miscarriage involves multiple losses (Brier, 2008). A novel finding is that miscarriage made some participants question if they would ever become the fathers they longed to be. Some participants tried to make sense of these feelings. This lends weight to the idea that early pregnancy loss as an ambiguous one, involving prospective grieving, stemming from the concurrent physical absence of, yet psychological presence of, the infant (Boss, 2004).
Despite such feelings, all participants wanted to support their partners. As McCreight (2004) found, they believed it was important to ‘live up to’ cultural and stereotypical expectations of their gender (i.e., supportive and strong), often because their partners had to endure the physical aspects of the miscarriage. Like others have found (e.g., Abboud & Liamputtong, 2005; Beutel et al., 1996; Johnson & Puddifoot, 1996), participants reported suppressing and/or avoiding their feelings in order to put their partners first. This was often at the expense of their own needs, leaving some feeling drained and depleted. Stroebe and Schut's Dual Process Model (1999, 2010) suggests that one must navigate grief, balancing loss and restorative aspects of bereavement. Yet participants in the current study often felt unable to grieve given their support role, and, in effect, delayed or denied their own grieving. Societal pressure for men to be the ‘strong one’ (O’Leary & Thorwick, 2006) may explain why grief may be delayed or re-emerges later (Lindemann, 1944, as cited in Jaffe, 2011). Puddifoot and Johnson (1999) similarly concluded that although men may not immediately present a response following miscarriage, they may be at risk of longer-term reactions.
The men described how the experience had brought their relationship closer, or in one participant's case, acted as a catalyst to address pre-existing issues related to having further children. Previous research has indicated that most women wish to discuss pregnancy loss with their partners (Black, 1991; Conway & Russell, 2000) yet 85% of couples share their feelings to a limited degree, if at all (Swanson et al., 2009) and men say nothing for fear of saying the wrong thing (Puddifoot & Johnson, 1997, 1999). The current study indicated that these men felt they could talk to their partners, often due to the absence of others to ‘lean on’. This lends support to Obst and Due's (2019) and DeFrain et al.'s (1996) studies, who found a lack of support outside the couple's relationship meant that most couples turned to one another, which in turn strengthened some relationships.
Unsurprisingly participants spoke of their anxieties around future pregnancies; that they could miscarry again, or would have to consider other options such as adoption. The men also described a desperation to have a successful pregnancy soon, given that further miscarriages may cost precious time; and how they felt unable to cope with another potential loss.
Anxiety and fear around the potential for another loss is well documented in women (e.g., Bergner et al., 2008; Côté-Arsenault & Donato, 2011) and is becoming increasingly documented in men (e.g., Armstrong, 2002; Lang et al., 2011; Meaney et al., 2017). In the current study, participants who had conceived again described the pregnancy as a tormenting experience. What should have been an enjoyable experience was tarnished because of the previous loss(es). Some felt resentful of others who could enjoy their pregnancy. In support of previous research (Franche & Mikail, 1999) these subsequent pregnancies led to chronic hypervigilance. At times this was made worse by the physical aspects of pregnancy that can only be felt by women. This left some participants feeling more vulnerable, as it was not possible for them to be reassured by the baby's movements in the same way women may be. O’Leary and Thorwick (2006) also found that fathers felt that, while work was a temporary distraction, they had difficulty concentrating and called home frequently to check on foetal movements: very different to their previous pregnancies.
Some participants placed importance on ‘catching back up’ given their reproductive stories had been put ‘on hold’. As previously described, reproductive loss can involve feelings of ‘being stuck’ (Diamond & Diamond, 2016). Some participants reported that it was important to keep trying and in some ways this became their focus. Some considered adoption. Others considered how becoming an adult coach at kids’ clubs could provide an additional option of identifying as a parental figure. The findings suggest that men can feel anxious about having a successful pregnancy and birth following miscarriage, and as a result may feel the need to consider alternative ways in which they can have the family they crave. Alternative family planning was not located in the literature reviewed, making this a novel addition to the evidence base.
The participants’ grief was disenfranchised by family, friends, work colleagues and/or health professionals, when it was either not considered a significant loss and felt experience, or they felt marginalised compared to their female partners. As in previous research (e.g., Geller et al., 2010; Lang et al., 2011) some participants felt there was lack of information from health professionals regarding what to expect physically and emotionally, that their feelings were ignored and, in some cases, their grief was not acknowledged. This suggests that the historical view of miscarriage as ‘non-events’ may still linger on, possibly due to a misinformed belief that early loss precludes attachment (Prettyman et al., 1993). Some participants reported that emotional support was solely directed towards their partners, supporting Lang et al.'s (2011) findings that mothers were usually the main focus of healthcare attention, leaving fathers feeling ignored and unacknowledged as a legitimately grieving parent.
Failure to recognise early miscarriage as significant and painful, like other deaths, was experienced by some participants. They described how miscarriage is treated differently to other deaths, noting how conversations around their experience of miscarriage were avoided, dealt with quickly in a non-validating way, or only briefly acknowledged in a superficial way.
As in previous research (e.g., Johnson & Puddifoot, 1996; McCreight, 2004), a range of clichés were offered, for example: “well at least you can get pregnant”; “oh well, everything happens for a reason”. Healthcare professionals also appeared to deny that a significant loss had occurred through the use of medical terminology such as ‘pregnancy debris’.
In contrast, some participants spoke of how their grief and loss was validated by others. For some, memorials, such as plaques at the crematorium, were important in validating their loss and acknowledging a loss had taken place. Some participants were offered ‘batch cremation’ which was reported as validating. Other rituals that marked the loss were also helpful. Some participants were offered, and some accepted, counselling following the loss, which allowed some participants to be more accepting of their feelings.
All participants experienced a new ability to discuss their experience in the hope of helping others. They became aware that the taboo not only has to be lifted but that men's experience needs to acknowledged. Previous research (e.g., Bute & Brann, 2015) highlights the taboo that surrounds miscarriage, a finding echoed by this study. Some participants felt this was a generational issue. Others pondered whether it was a “British thing” which led to the use of euphemisms and avoiding the topic. Some participants spoke of how it becomes uncomfortable when others assume they will simply ‘try again’, as for some, the miscarriage signified the end of further conception attempts. Participants were in no doubt that cultural change was needed to challenge the beliefs and attitudes that keep the topic hidden or avoided.
Whilst participants spoke of the need to break the silence around miscarriage, they also spoke of the continued stigma around men and mental health. They reflected on the male stereotypes of being ‘strong’, ‘silent’, and ‘protective’ and how these are still prevalent and changes to these would require time and effort. They described how the misperception that miscarriage happens to women, not men, still exists. Yet, as in previous research (e.g., O’Leary & Thorwick, 2006) all described how the miscarriage happened to them too, and as such both parents need to be acknowledged. Some felt apprehensive about challenging this, fearing they would be judged, and their masculinity questioned.
The study uncovered some thought-provoking insights into the lived experiences of men experiencing early miscarriage. The key messages are as follows. Men readily invested in their pregnancy and looked forward to the arrival of their baby and the new future this would bring. When the miscarriage happened, men felt considerable grief and loss and were psychologically distressed. Men then readily adopted the ‘support role’ for their wives/partners, and suppressed their own emotions often to the detriment of their own psychological health. During this difficult and traumatic time, men's relationships strengthened as they and their partners turned to one another for support. Considering subsequent family planning, men suffered considerable anxiety either during the pregnancy following the loss or at the thought of conceiving again. For some men this meant they ceased to consider trying to conceive any further children, whereas others experienced the subsequent pregnancy as incredibly anxiety provoking, tormenting and potentially traumatising. Men are clear that society must acknowledge early miscarriage is a death as significant as any other and that they too feel the same loss women feel. Men do not want to be marginalised by their gender and wish to be equally recognised as a bereft parent. Men are clear that society must reject the taboo nature of miscarriage, as well as the outdated cultural and gendered stereotypes that prevent men from discussing it freely without fear of ridicule or assault on their masculinity. Essentially society must end the silence of miscarriage and male experiences within it. Miscarriage should be recognised, irrespective of gestational stage, as a psychological, rather than a solely medical, event.
The results of this study have important implications. The following suggestions are provided for health care professionals, who can:
Increase their awareness of men's investment and attachment to baby preconception, conception and in early pregnancy and the psychological impact of miscarriage for men; Avoid minimising early pregnancy loss, and instead, acknowledge early miscarriage as a significant loss. Be guided by how expectant parents refer to their pregnancy e.g., embryo, foetus, baby, child, by name, etc. and how they identify themselves as parent, father or otherwise; Offer anticipatory guidance regarding what to expect physically and emotionally and the availability of bereavement resources, support, and counselling; Assist men to challenge solely supportive and stoic stereotypes and encourage expression of their own grief including prospective grieving; Prepare men for the common clichés they may be offered from well-meaning family and friends; Review policies and procedures that may dictate that miscarrying parents are admitted to maternity wards; Consider if hospital procedures could be as similar as possible to those used in relation common bereavement rituals. Where a formal event is not possible, encourage the creation of other mourning rituals; Provide men with reassurance in subsequent pregnancies; assess their psychological needs and include them in antenatal care.
Future research may wish to recruit more diverse samples of men. The impact of religion on the miscarriage experience may also be of interest. Exploring the experiences of gay, bi-sexual, or transgender men who have had a surrogate pregnancy which ended in early miscarriage may uncover unique or added challenges. The novel finding, demonstrating the level of investment, future thinking and identifying as fathers at pre-conception, conception or the very early stages of pregnancy, would be worthy of further study. Future qualitative research may better understand the process and narratives involved in future family planning following miscarriage. Future population-based studies are indicated to quantify the number of men that experience psychological distress following early miscarriage. Finally, the study has demonstrated the need to explore whether grief measures are sensitive enough to capture more ‘masculine’ expressions of grief such as anger and jealousy.
Due to the study's idiographic nature, the findings may not be representative of all men's experiences of early miscarriage. The entire sample was of white British men living in England in professional occupations. It may be that those in contact with Tommy's charity were more likely to volunteer for the study and could have differed in their experience compared to men that did not seek such contact.
The first author has personal experience of miscarriage which may have influenced data interpretation. A reflective diary, triangulation with the second and third authors, and participant checking of identified themes sought to minimise such bias and threats to validity.
Footnotes
Acknowledgements
We thank all of the men for their participation in this study, and the Tommy's Charity.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.