
Abstract
Mesothelioma is an incurable asbestos-related cancer with a high symptom burden. Its long lead time means cases in the military context tend to be amongst veterans. Research into the lived experience of mesothelioma is sparse. Research shows British veterans and their families are likely to have particular needs accessing health services and support. This study explored the psychological effects of mesothelioma in the UK military context from the carer's perspective. It comprised a secondary data analysis of interview data plus semi-structured interviews with family carers of UK veterans with a mesothelioma diagnosis. Themes developed included ‘Going the extra mile’; ‘Shifts in previously robust characteristics and roles’; and ‘Needing to know’. Military culture impacted both patients and carers, with participants reporting a reluctance to show weakness. Carers experienced guilt and traumatic stress symptoms. Moral injury was reported relating to carers’ interactions with the Ministry of Defence (MOD) and the National Health Service (NHS).
Background
Malignant mesothelioma is an incurable disease, usually linked to asbestos exposure, with two main types: malignant pleural (MPM) and peritoneal mesothelioma (Cancer Research UK, 2021). It is generally diagnosed in older people, and survival rates are poor (Cancer Research UK, 2021). Symptoms appear after a long latency period (20–50 years), often with rapid progression and late-stage diagnosis (Nuyts, Nawrot, Nemery, & Nackaerts, 2018). In advanced disease, symptoms become severe, sometimes proving difficult to control (Ball, Moore, & Leary, 2016). Although mesothelioma remains incurable, recent advances provide more treatment options (Colarusso, Terzic, Achard, & Friedlaender, 2019).
Research into mesothelioma's lived experience remains sparse, resulting in lack of awareness of its unique psychosocial impact (Harrison, Gardiner, Taylor, Ejegi-Memeh, & Darlison, 2021). A recent scoping review revealed: the importance of timing of interventions and delays in the medical journey; the impact of uncertainty; ubiquitous negative feelings, including about identity change; issues relating to positive/negative aspects of communication (Sherborne, Seymour, Taylor, & Tod, 2020). Subsequent studies have reinforced these findings, identifying elevated levels of depression, anxiety and traumatic stress symptoms in both patients and carers (Bonafede et al., 2020; Hoon et al., 2021). Further research into the psychological effects of mesothelioma is required to map potential impact occurring alongside developments in medical treatment/prognosis (Sherborne et al., 2020). This also applies to informal carers, whose wellbeing is important (Colarusso et al., 2019; Lee & Lyons, 2019). Informal carers’ experience has not been a focus of mesothelioma research to date (Guglielmucci et al., 2018), leaving an important gap considering the disease's high symptom burden and complexity. Studies exploring specific groups’ experiences have also been recommended, such as military veterans (Sherborne et al., 2020).
Asbestos exposure in the Armed Forces (AF) has been shown from diverse sources including accommodation and damaged buildings during conflict and aid-delivery (Ejegi-Memeh et al., 2020). Despite surveys of military infrastructure and equipment, asbestos may present an on-going risk (Ministry of Defence, 2019). British veterans diagnosed with mesothelioma caused by exposure during service are entitled to an enhanced pension or lump-sum payment (Ministry of Defence, 2016). For veterans with dual civil-military exposure, complex claims can add to the stress of diagnosis and prognosis (Ejegi-Memeh et al., 2020).
The long latency period means military cases usually occur amongst veterans. British veterans and their families often have particular needs in accessing health services, care and support (Hynes & Thomas, 2016). Many older British veterans experience social isolation (Albertson, Taylor, & Murray, 2019). They may show greater reluctance to seek medical treatment due to a sense of self-sufficiency (Williamson, Harwood, Greenberg, Stevelink, & Greenberg, 2019). Veterans’ reluctance to seek help can impact their carers. Thandi et al. (2017) found veterans’ carers sometimes felt unable to cope with caregiving demands, and the military partner's lack of/delay in help-seeking caused relationship strain. Carers ascribed veterans’ extreme reluctance to accept informal care to embarrassment and pride, which could distress and frustrate carers (Williamson et al., 2019). A sense of humour is highly valued in the British Armed Forces; it allows individuals to face danger and enhances group bonding (King, 2004). It has helped UK veterans in therapeutic groups cope by increasing their sense of camaraderie, reducing frustration and helping them cognitively reframe stressful situations (Caddick, Phoenix, & Smith, 2015; Kopytin & Lebedev, 2015). However, such humour can create barriers by masking veterans’ support needs from services (Hitch, Harper, Armour, & Waterhouse-Bradley, 2020). When military personnel transition to civilian life they may be reluctant to abandon their ‘militarised’ body (Grimell, 2019). Continuing physical exercise after leaving is important to many veterans (Williamson et al., 2019). Military training of the body “fosters a capacity to ‘soldier on’ in the face of corporeal adversity” (Hockey, 2012, p. 9). However, men with a fixed view of masculine physicality as essential to their identity may have worse health outcomes (Stansbury, Mathewson-Chapman, & Grant, 2003).
The recent Military Mesothelioma Experience Study (MiMES) (Ejegi-Memeh et al., 2020) aimed to address lack of evidence about the experience and health/support needs of British veterans with mesothelioma. MiMES identified unique challenges for them, and their families. This article details a qualitative study designed to address identified evidence gaps relating to mesothelioma's psychological effects, particularly from the carer's perspective, and also regarding mesothelioma's effects in different workforce groups.The study therefore explored mesothelioma's psychological effects in the UK military context from the carer's perspective.
Methods
This study used Interpretative Phenomenological Analysis (IPA) and semi-structured interviews with informal carers of UK veterans diagnosed with mesothelioma. Interviews were from two sources:
a Secondary Data Analysis of interview data from MiMES an empirical study: six semi-structured interviews with family carers of UK veterans with mesothelioma.
The University of Sheffield's Ethics Committee approved. The Secondary Data Analysis supported and informed the empirical study, generating initial insight, identifying sensitising issues and allowing fine-tuning of the interview schedule. Reusing data has positive ethical implications, for example, economically using data from charity-funded research (Chauvette, Schick-Makaroff, & Molzahn, 2019).
Methodology
Interpretative phenomenological analysis (IPA) methodology underpinned the study. IPA is a qualitative approach having a dual phenomenological/hermeneutic stance, with experience, idiography and interpretation as key characteristics (Smith, Flowers, & Larkin, 2009). IPA has often been used for research into illness experience, particularly experience of existential importance (Smith et al., 2009), e.g., terminal cancer. IPA pays attention to individual nuance, thus addressing a gap in the mesothelioma literature (Sherborne et al., 2020). IPA's use for the Secondary Data Analysis was informed by Spiers and Riley’s (2019) method for dual analysis of interviews with general practitioners. Reflexivity is key to IPA (Smith et al., 2009), therefore reflexive notes were kept throughout planning, data collection and analysis.
Sampling and Recruitment
For the Secondary Data Analysis, we selected the four MiMES transcripts where carers were interviewed separately from the patient. For the empirical study, participants were selected purposively focussing on people sharing two life experiences: caring for someone with mesothelioma and being in the military community. Eligible participants were aged 18 + ; the main informal carer for a UK military veteran with a diagnosis of mesothelioma (living/up to 24 months deceased); capable of informed consent.
To recruit, study information was circulated by Mesothelioma UK (a charity supporting people with mesothelioma and their families) via email, website, Facebook and Twitter. Information was also circulated by local asbestos support groups (ASGs) and military support organisations. Interested people could phone the Mesothelioma UK helpline. Helpline staff informed potential participants about the study, who chose whether to participate.
Seven participants came forward. One dropped out, giving no reason, after receiving the Information Sheet. Regarding sample size, IPA does not aim for data saturation; it depends on the data's richness, commitment to in-depth engagement with data, and practical constraints (Smith et al., 2009). Six is a typical number of participants for an IPA study (Pietkiewicz & Smith, 2014). Within the homogeneous sample obtained there was variation in gender, age, military/civilian status, service branch, mesothelioma type, geographical location, and carer-patient relationship.
Data Collection
One-off semi-structured interviews were conducted September 2020-March 2021 by VS. She is a counsellor specialising in trauma and bereavement, trained and experienced in conducting qualitative research. VS had ‘outsider’ status regarding the military, and ‘insider’ status as a lung cancer patient. Prior to interview, VS had no relationship with the participants. They were informed her study was for a PhD, funded by Mesothelioma UK. They gave written informed consent.
Interviews were conducted via videoconferencing on the university-approved platform, Google Meet. Only participant and researcher were present. Supplementary Information 1 gives the pilot-tested interview schedule. Digital audio-recording was used, with field notes taken after each interview. Interviews lasted 58–115 min and were professionally transcribed verbatim, then anonymised.
Data Analysis
The first author analysed the data, developing themes using Smith, Flowers and Larkin’s (2009) six steps for IPA. Quirkos software (Quirkos Limited, 2020) was used to store and sort the data, contributing to an audit trail. VS, AT and BT regularly discussed the themes developed to ensure they were credible and grounded in the data.
Participants’ feedback on findings/transcription was not invited. Participant validation is contentious in IPA, as it generates extra data from a different viewpoint/time (Cuthbertson, 2019; Howard, Katsos, & Gibson, 2019).
Participant Demographics
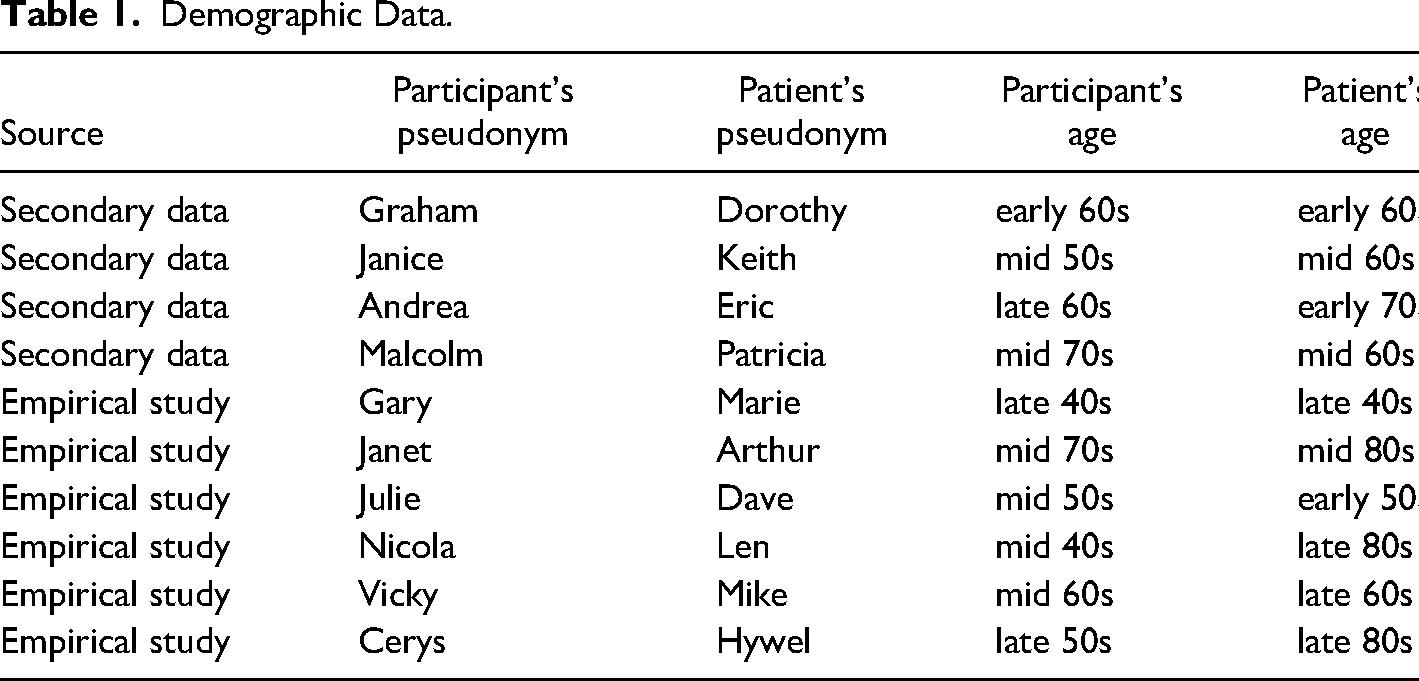
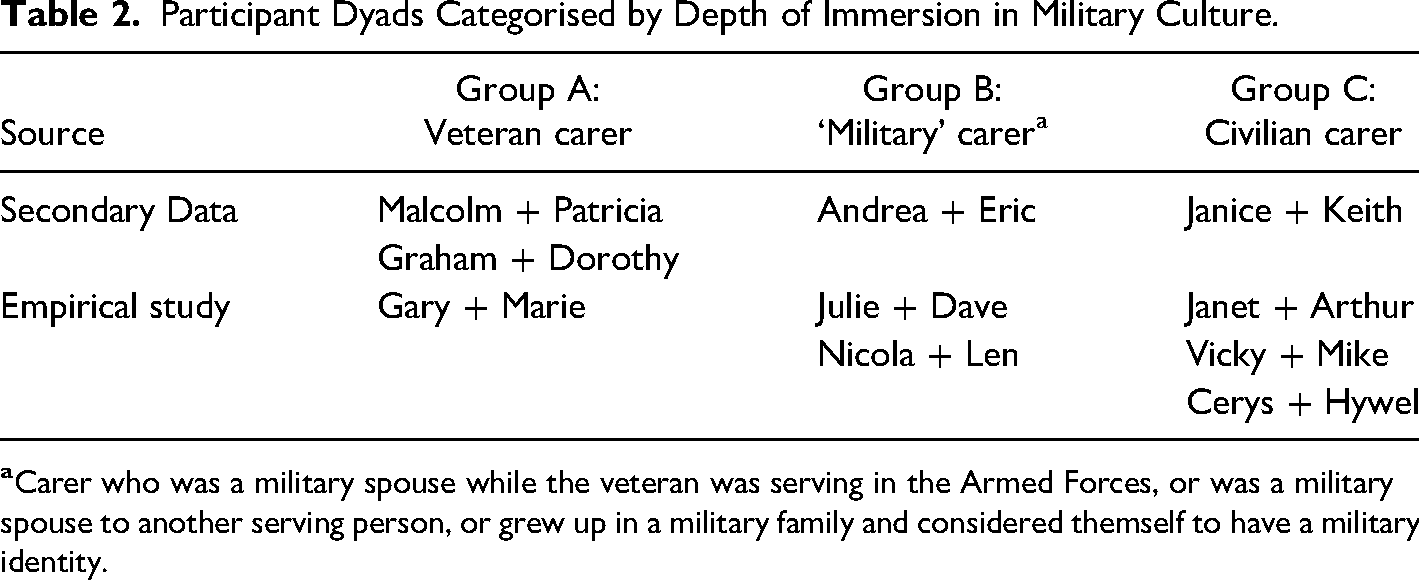
The sample comprised ten participants (see Table 1). Three carers were male veterans, caring for female patients. All carers and patients were White British. The patients had served in the Royal Navy, British Army and Royal Air Force (RAF). The carers had served in the Army and RAF. Table 2 shows each dyad's depth of immersion in military culture. All participants lived in England except for Cerys, who lived in Wales. The majority were the patients’ spouses, but Nicola and Cerys were daughters. The only patient who did not have pleural mesothelioma was Marie, who had peritoneal.
Demographic Data.
Participant Dyads Categorised by Depth of Immersion in Military Culture.
Results
Our data showed many of the psychological effects experienced by the carers and veteran patients mirror those of the wider mesothelioma population, for example, shock at diagnosis and delay-related anxiety. Here, we present selected findings, focussing explicitly on the interface between the carers and patients’ military background and their health experience. Sometimes participants explicitly talked about how military culture affected them/their relatives. Elsewhere, it seemed the military context was influencing their experience outside of awareness; we acknowledged this during interpretation.
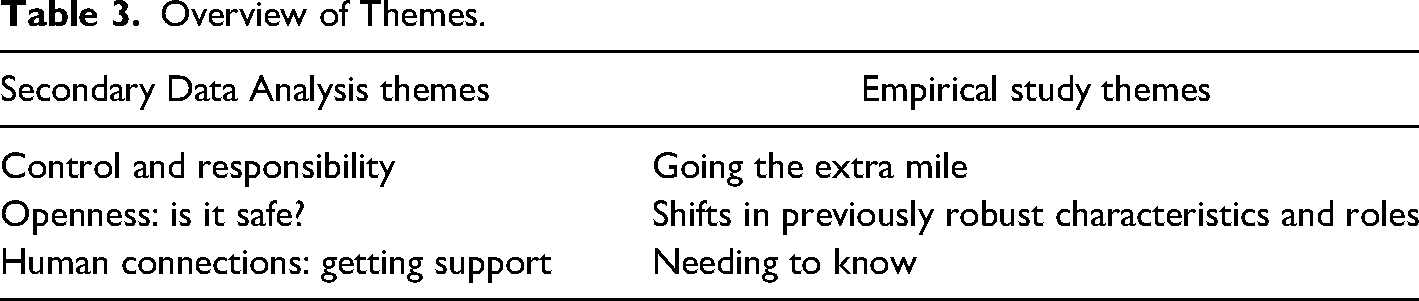
Themes developed from the study's two elements are shown in Table 3. All themes were present in each participants’ data. As the Secondary Data Analysis's findings foreshadowed those of the empirical study, we here present only the empirical study findings, with illustrative quotations. (See Supplementary Information S2 for selected quotations illustrating the Secondary Data Analysis's themes.)
Overview of Themes.
Empirical Study Findings
Going the extra mile
This theme encompassed how patients and carers reacted to the diagnosis/prognosis; how they coped with day-to-day practicalities of living with a terminal illness; and how they experienced the efforts and commitment of others. Most participants highlighted the veteran's military stoicism and self-reliance: “That’s what’s drilled into them – you deal with whatever’s thrown at you. It affected the way he coped with his illness - in a positive way, in that he just got on with it; in a negative way because he was not very good at flagging up that he needed help.” (Julie)
Military values concerning teamwork, efficiency, respect for others, loyalty and selfless commitment were influential but generally not referred to explicitly. Four participants reported the patient's response to the diagnosis/prognosis as a determination to fight on: “’We’re not the type,’ he said, ‘to just sit in a chair and curl up and die. We fight on.’” (Cerys)
For Dave, already disabled, it meant “every day was a battle.” For Gary, the practical tasks of caring plus extra, complex difficulties (NHS complaint, MOD lawsuit) meant keeping going to the point of exhaustion: “I was fighting really, making myself ill, and I was crying in the car on the way to work, just not sleeping.”
Julie felt she should have “carried on fighting” on Dave's behalf when healthcare professionals judged it was time for him to die. For Janet, the abrupt way the prognosis news was broken led to recurrent despair: “I’m wishing my life away because I feel sometimes, I don’t want to cope with this.”
Military culture's emphasis on ‘service before self’ was relevant to carers Gary and Nicola's experiences. For Nicola, ‘going the extra mile’ meant planning efficiently and adapting to changing circumstances, in a father-daughter team: “I ploughed a lot of my efforts into that [achieving a good death].”
She was pushed to the limit managing end-of-life practicalities plus processing the emotional meaning of the imminent death. Her phrase “slight breakdown wibble” demonstrated how she minimised and gently mocked her distress.
Military emphasis on physical fitness means carers neglecting their own health may experience shame. Gary, determined to look after his wife, dismissed his counsellor's suggestions about self-care: “Pff, OK, whatever, I’m a grown man”. One of Janet's coping strategies was snacking: “I think, ‘Well, why not? ‘Cos I might not have him for ever.’ I don’t know what my [diabetes] nurse will say.”
With Dave admitted to hospital, Julie was less able to use her coping strategies, including exercise. In contrast, Cerys could currently balance her caring responsibilities with self-care, getting emotional support from friends while exercising.
Shifts in previously robust characteristics and roles
Participants described and made sense of any personal changes in them and/or the veteran patient and associated psychological effects. Military culture's underlying influence was noticeable for some dyads. Stoicism, selflessness, goal-orientation and humour brought psychological benefits. However, having high standards, especially concerning loyalty, contributed to depression, loss of trust and resentment.
No participants felt the veteran changed profoundly. Two veterans’ integral religious faith helped them cope: “His single biggest coping strategy was his faith.” (Julie)
“I didn’t notice any changes in Michael at all. He was always caring, kind, deeply religious.” (Vicky)
Thoughtfulness was also mentioned by carers Gary and Nicola, as an enduring characteristic of the patient. Although participants did not explicitly make the link to military selflessness, this quality was valued by patients and carers.
Another unchanging patient characteristic was humour: “He was still making nurses laugh the day before he died, and I’m really proud of that.” (Julie)
This was presented by several as part of the patient's positive outlook. However, this could have a downside. Hywel was reluctant to see himself as other than physically capable, frustrating Cerys: “Dad is a little bit of bury your head in the sand. He’ll say, ‘I’m concentrating on trying to live, not bothered about dying.’”
Compared to the elderly veterans’ experience, one of the younger couples’ experience had an extra dimension: “she didn’t want her husband to be her carer; she didn’t want to look vulnerable” (Gary). His wife was distressed at the change in their sexual relationship. This echoed the other younger couple's experience: “He just wanted to sweep all those potential issues under the carpet.” (Julie)
For the two daughters caring for fathers, their healthcare professional identity and experience gave a firm foundation for approaching the illness. Providing personal care did not “faze” Nicola; though it was harder for Len to adjust, “I think it brought us even closer.” Nicola described herself as “more military than civilian”, with a default to the positive. She had planned to use a ‘Hospice at Home’ service but had to step in when this was cancelled. She made sense of this difficult situation by benefit-finding. In contrast, Cerys found her father's struggles to eat caused tension between them, with Cerys sometimes moving into a parental role: “He’s going, ‘No, no, don’t want it, don’t feel like it.’ So that’s hard.”
Without a healthcare professional background to bolster their caring, Vicky and Janet saw themselves as possibly not mentally robust enough, mentioning previous episodes of mental ill-health. Janet's lurking anxiety seemed linked to how she felt changed as a person: “I’m more aware…of “If people criticise, I think it’s personal to me. I’m wanting people to value me, yeah. That’s odd…I know Michael’s made his mark…and I don’t want my life to be…wasted [tearful].”
Michael's religious faith brought him certainty. A mindset of self-control and determination helped him. Vicky tended to compare herself unfavourably to others and doubt her ability to be resilient.
The younger carers Gary and Julie, widowed in mid-life, experienced changes in their sense of self. For Gary these were mostly negative. Expecting masculine goal-orientation, instead he experienced inertia: “I’m a grown man. I know what I need to do, but I’ve got to find something to move on to.” (Gary)
Negative changes included no longer being interested in work and being less smart in appearance: “that's not me at all.” Military values now held less meaning for him. Gary made sense of this change: “I’ve got a different outlook now…I’m ready to go…I probably am depressed, but I’m not going to kill myself or anything, but if I died of something, I’m not that bothered. I look at it as if to say, ‘I don’t care. Get on with it.’”
Julie found herself in an unresolved change-process. Whilst she accepted this, some aspects worried her. Noticing herself withdrawing from people, a “dangerous” process, she explained: “I don’t trust people in the same way. Because, I guess, I don’t trust people to like me for me.”
Other changes made it harder to shape her new life. The traumatic nature of Dave's last days left her with “flashbacks”, and she worried her anger at the MOD would taint her treasured ‘military wife’ identity.
Needing to know
This theme concerned experiences of choosing what to share between patient and carer, and with others. In military culture clear communication is key, with information shared on a need-to-know basis; consequent expectations contributed to psychological effects on patients and carers. For some participants, choosing what to share was straightforward: “I wasn’t afraid to talk to people about dad’s illness, if they asked. I was just saying it as it was.” Nicola
In some dyads, needs differed: “Michael initially didn’t want people knowing that he’d got cancer. And that was tough.” Vicky
Michael's military role had required extreme secrecy, and in this current life-threatening situation he shut down communication. Only the immediate ‘team’ could know, closing off Vicky's coping strategy. Gary experienced a profound change when it came to communicating: “I would just broadcast everything. That might have been a bit overwhelming for some people, but I didn’t care.”
His new strategy made it harder to attend to others’ feelings, including his children's.
Military culture influenced expectations about information exchange with/between professionals (healthcare, MOD, charities). Expectations related to honesty, efficiency, trust, and protecting others. When expectations were met, patients and carers felt reassured, included, cared for. For example, Nicola appreciated being “briefed beautifully” about the coroner's involvement. Janet and Arthur appreciated having the ASG “there at the end of the phone.”
When expectations were unmet, participants were left feeling angry, frustrated, confused, helpless or traumatised. Gary described phoning the MOD for months about Marie's financial claim: “They just lied to me each time. I’m going, ‘What's going on?’” Len and Nicola made complaints about two incidents where hospital staff refused to take time to inform her: “He was very concerned that they didn’t mark him and say, ‘Right, that’s it, you’re not getting certain treatment.’ But it was for the doctor to understand the consequences.”
The bereaved carers in our sample were strongly motivated to help others have access to information they ‘needed to know’ about asbestos health-risks. The military concept of ‘lessons learned’ was important. Military culture also influenced expectations about intra-dyadic information-sharing, resulting in secrecy or clear communicating. Where patient-carer strategies for getting their needs met aligned, they felt connected and supported. Where there was a mismatch, participants reported isolation, frustration, guilt and distress. For three dyads, choosing what information to share seemed straightforward. Gary and Marie talked about “absolutely everything.” Janet and Arthur “were closer if anything.” Nicola proactively helped Len create a metaphor, “going to the Caravan Site in the Sky”, which helped communication right until death, part of their team planning.
The other dyads were less open. Hywel avoided talking about the future, leaving Cerys frustrated. For Vicky and Mike, talking was an important coping strategy. Despite their closeness, secrets were kept. Vicky would “rant” privately about the illness's injustice. Mike protected her from knowing his anxieties, keeping up his image of mental strength. Dave also wanted to protect Julie: “I felt him withdraw from me. And I think that was because he was afraid, but also, he didn’t want to scare me. His biggest fear was dying on his own.”
Dave was a veteran diagnosed with pre-existing PTSD; his anxiety was likely to be a symptom. In turn, Julie protected Dave, but also felt guilty as her weakened Christian faith distressed him.
The implications of the findings from the study's two elements are discussed together in the next section.
Discussion
Discussion of Findings
This study tells us much about the psychological impact of mesothelioma on UK military veterans and their informal carers. Findings are now considered in relation to existing literature and knowledge. We here consider the findings in relation to two aspects of the psychological impact of mesothelioma in this context: ‘Caring for and caring about’ and ‘Guilt, betrayal and traumatic stress’.
Caring for and caring about
Our findings show how the military context influenced many aspects of how the carers cared for/cared about the patient, other people, and themselves. It made sense to many participants to ‘go the extra mile’ in terms of how they cared for their loved one. For three, this meant not asking for help, even when reaching crisis point. Our findings generally support the picture of reluctance in help-seeking in the burgeoning existing literature on informal carers in the military community. A Royal British Legion survey (2021) found veteran carers were 2.5 times more likely than civilians to care for a spouse/partner, and veteran carers caring for a veteran were three times more likely to do so. Nearly half of carers for a veteran had received no support in the last two years, double the general population proportion. Several patients in our study did not want the carer to tell others about their illness, putting pressure on the carer to manage alone. This may reflect the patient's military background, with its emphasis on a tight team working together and excluding outsiders (Brewster, McWade, & Clark, 2021). This has potential impact on carer burden and health.
In our study, underpinning this issue was the concept of military masculinity. This “hypermasculine” culture values toughness and emotional control, in a disciplined, hierarchical structure (McAllister, Callaghan, & Fellin, 2019, p. 258). Physical endurance and toughness are prioritised over self-care. Central is stoicism, that is, “the capacity to endure and ‘crack on’ despite emotional and physical distress”, with expression of empathy framed as “enabling weakness” (McAllister et al., 2019, p. 263). All our participants invoked the concept of military stoicism in their veterans, supporting Williamson et al.’s (2019, p. 6) report of older veterans wanting to appear “tough”.
Military masculinity involves a positioning of femininity as ‘other’, as ‘risky’ within the military environment (McAllister et al., 2019, p. 258), with implications for female carers of military veterans in terms of help-seeking. Military wives/female partners are positioned in contradictory ways: being seen as weaker physically and emotionally, and needing protection; or required to show great practical and emotional resilience in their military support role (Johnson, Ames, & Lawson, 2021; Keeling, Woodhead, & Fear, 2016). These militarised expectations are often internalised (Long, 2021), explaining how carers in our sample, particularly those steeped in military culture (Groups A and B in Table 2), were more likely to keep on going without seeking support. They valued their own independence and ability to get on with things, with matching expectations from the patient.
Our sample included carers for female as well as male veterans. For female veterans, their relationship with militarised masculinity is complicated: on transition, they have to recover a civilian identity and a female identity (West & Antrobus, 2021, p. 7). Female veterans want to be seen as strong, with illness of any sort being seen as weakness (Godier-Mcbard, Gillin, & Fossey, 2021). In our study, Malcolm took pride in Patricia's courage and humour; Gary was concerned Marie was not ‘robust’ enough. The two female carers showing anxiety about their own mental ability to cope were civilians, who may have been influenced by their veteran husband's expectations about women being ‘weaker’. Andrea, a military wife, embodied an ingrained expectation of independence and not asking for help, yet her husband clearly felt wives and families needed protecting. Understanding how a military background may influence patients’ and carers’ coping strategies and expectations of themselves and others can help nurses better meet these families’ care and support needs.
Our study's findings support to some extent the existing literature on the carer's role, which is sparse in relation to male carers. However, new insight has been provided into how a military background may affect carers’ experience of doing care and caring about their loved one, with some atypical manifestations in terms of gender. Our sample included three male carers, who showed a range of responses to their caring role. Malcolm focussed on the practical, responsible, and protective side of his role, seeing it as a job to be done well and solo. Gary took so many tasks into his ‘square’ of responsibility he couldn’t cope; he was aware paying attention to his own needs was incompatible with his “grown man” identity. Graham seemed more like an ally/helper, part of the back-up team to a capable veteran, as if his wife herself was the carer. Judd, Guy and Howard (2019) reported similar findings in their study of UK men caring for a dying spouse/partner. Their participants saw caring tasks as providing a source of purpose and responsibility, like a job; it was important to protect their partners from their own distress and seek help only as a last resort. Nicola's problem-solving style, with its emphasis on positivity, plus discomfort with seeking emotional support, therefore matched a male pattern. None of our three male participants reported issues with taking on household responsibilities, possibly as military training instils relevant skills and pride. This differed from Ussher et al.’s (2013) finding that male carers found the burden of extra responsibilities within the home difficult. Two of our female participants reported feeling closer to the patient, unlike the males. This contradicts Ussher et al.’s (2013) finding that men were more likely to report increased relational closeness with the patient.
Guilt, betrayal and traumatic stress
Half our participants talked about feeling guilty or let down due to expectations and assumptions about how people/organisations should behave. Examples included: not continuing to help the patient fight to live; being a healthy ex-smoker (survivor guilt); anger at the MOD for not providing the expected support and information or the NHS for not working efficiently and taking responsibility when things went wrong. Survivor guilt has featured in the cancer research literature (Perloff et al. (2019), Glaser, Knowles and Damaskos (2019)). It is rare in the mesothelioma research literature, though it appears in the grey literature (Kember (2014); Von St. James (2016)). Bonafede et al. (2020) suggested survivor guilt was why mesothelioma caregivers were more traumatised than patients. Survivor guilt could be relevant to the mesothelioma experience in different ways: exposed caregivers remaining well (including those who caused the patient's contamination); long-term survivors; and carers feeling they have unfairly been spared. Increasingly effective treatments such as immunotherapy may mean survivor guilt becomes more common. Our veteran carers knew they could have been exposed to asbestos, but did not express survivor guilt, perhaps because they saw the MOD as ‘the guilty party’.
Two participants felt guilty about letting down their husbands. Such guilt may spring from a sense of betraying expectations about being a loving partner (Bennett, 2017); or provide a defence against helplessness and grief; or fulfil a loyal, commemorative function (Glaser et al., 2019), chiming with military culture. The powerlessness inherent in receiving an incurable diagnosis can negatively impact someone's belief systems regarding control, justice, predictability and self-image (Glaser et al., 2019).
Turning to traumatic stress, Julie showed symptoms: flashbacks. This aligns with Bonafede et al.'s (2020) picture of female carers being at higher risk for traumatic stress symptoms (TSS). Julie's husband's pre-existing PTSD appeared to be exacerbated by his mesothelioma experience, obstructing his decision-making about treatment. Swartzman et al. (2017) showed cancer survivors with prior trauma were more likely to exhibit TSS; carers had similar proportions of TSS. In military veterans, a cancer diagnosis can have varied impacts, including traumatic stress (Jahn, Herman, Schuster, Naik, & Moye, 2012; Martin, Moye, Street, & Naik, 2014). Veterans’ original trauma could be mimicked by the threat-to-life from illness, amplifying PTSD (Way et al., 2019). The Military Mesothelioma Experience Study (Ejegi-Memeh et al., 2020) did not refer to the combination of mesothelioma in veterans and traumatic stress, apart from suggesting occupational history-taking could trigger distress. Our study therefore adds additional understanding of how traumatic stress may affect British veterans with mesothelioma and their caregivers. This could aid professionals in recognising when traumatic stress is affecting not only military veteran patients but their carers too.
Our data also suggested some participants experienced moral injury. Moral injury is described as: “A negative self-judgement [due to] having transgressed core moral beliefs and values or feeling betrayed by authorities…Its symptoms include shame, survivor guilt, depression, despair, addiction, distrust, anger, a need to make amends and the loss of a desire to live.” (Brock, 2011, p. 1)
Three participants’ experience matched circumstances for moral injury. Their data included many symptoms listed by Brock (above). Existing mesothelioma literature refers to patients and carers feeling anger towards previous employers, complicated sometimes by loyalty (Di Basilio, Shigemura, & Guglielmucci, 2021; Harrison et al., 2021). The Military Mesothelioma Experience Study found participants felt frustrated about perceived inequalities (with some saying the MOD had not fulfilled its duty of care), and about the NHS being less efficient and navigable than the military system (Ejegi-Memeh et al., 2020). Other UK studies document similar difficulty in navigating fragmented mesothelioma services, where communication with healthcare professionals is disjointed (Harrison et al., 2021; Henshall et al., 2021). Our study suggests the distress caused to some carers of veterans with mesothelioma goes beyond frustration, anger and guilt to be conceptualised as moral injury from broken expectations (about oneself or British institutions) arising from deeply held values about loyalty, respect, efficiency and responsibility. Understanding moral injury and its negative psychological effects can enhance professionals’ provision of support for this group.
Strengths and Limitations
Our findings add to the limited existing picture of the complexities for women veterans, and women caring for male veterans, regarding attitudes to help-seeking. This insight is needed as it is important to beware of militarised masculinity being “the only lens through which we understand veterans’ experiences” (Bulmer & Eichler, 2017, p. 173). The extent and nature of survivor guilt in carers for a veteran with a diagnosis of mesothelioma is a novel finding. Limitations relate to the researchers' positionality and the sample. All researchers were female civilians, that is, ‘outsiders’. Whilst our civilian status may have hampered authentic interaction with participants, we may have asked more clarifying questions, revealing extra aspects of their experiences (Abrams, Tabaac, Jung, & Else-Quest, 2020). Participants’ self-selection is a limitation, but their willingness to talk about emotive subjects may have illuminated experiences shared by those less comfortable with openness. Recruitment was challenging due to mesothelioma's rarity and the COVID-19 pandemic, so the sample size was small (n = 10), but appropriate for IPA. IPA's idiographic emphasis means our study illuminates the range of experiences, challenges and responses within the veteran community due to intersectionality. The two-stage design of our study adds an element of triangulation. Although the small sample precludes statistical generalisation, the study may be used to make suggestions of internal generalisability within this population, particularly as the sample includes some diversity (Maxwell, 2020). Sufficient details about participants, methods and researchers have been provided to make consideration of transferability to other contexts possible (Levitt, 2021).
Conclusion
This study provides novel insight into the psychological effects of mesothelioma in the UK military community. Both veterans with mesothelioma and their carers are shown to have particular challenges in relation to accessing and receiving health and care support, which may also apply to veterans with other serious health conditions. Many unanswered questions remain about the psychological effects of mesothelioma on patients and their carers, including in the military context. Further research is needed into moral injury as identified in our study, as it had serious negative impacts on the carers. Similar research could be conducted into moral injury arising from other medical conditions in this military context. As our study was unable to recruit participants outside England and Wales, further research is recommended into the psychological effects of mesothelioma on veteran patients and their carers living in other UK regions and abroad, e.g., Nepal, as this may highlight the effects of cultural differences. Our study showed how keeping up with developments in mesothelioma treatments/trials could involve much work and stress for carers. Further research is needed into how patients and carers are affected psychologically by the newest advances in mesothelioma clinical research. Our study's findings may help develop the support professionals provide to UK military veterans and their carers and illuminate potential research to benefit the wider community of people living with mesothelioma.
Footnotes
CRediT Author Statement
Data Statement
Permission to access our anonymised data may be sought from the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors are grateful to Mesothelioma UK for funding this PhD study (Grant number A16097) and to the University of Sheffield for providing a Publication Scholarship. The authors have no other funding or competing interest to declare. We wish to thank all who participated in this study.
Supplemental material
Supplemental material for this article is available online.