
Abstract
On July 6, 2013, a train with 72 crude oil tank cars derailed in the heart of Lac-Mégantic, a small municipality of 6,000 inhabitants located in Québec (Canada). This tragedy killed 47 people. Technological disasters are rarely studied in bereavement research, and train derailments even less. The goal of this article is to increase our understanding of the bereavement consequences of technological disasters. Specifically, we aim to identify the factors that lead to the experience complicated grief and distinguish from the protective factors. A representative population-based survey was conducted among 268 bereaved people, three and a half years after the train accident. Of these, 71 people (26.5%) experienced complicated grief. People with complicated grief (CG) differ significantly from those without CG in terms of psychological health, perception of physical health, alcohol use and medication, as well as social and professional relationships. Hierarchical logistic regression analysis identified four predictive factors for CG: level of exposure to the disaster, having a negative perception of the event, as well as having a paid job and low-income increase the risk of CG. The importance of having health and social practitioners pay attention to these factors of CG are discussed along with future directions for research.
Introduction
In the middle of the night of July 6, 2013, a train with 72 crude oil tank cars derailed in the heart of Lac-Mégantic, a town of 6,000 inhabitants located approximately 200 kilometers east of Montréal (Québec, Canada). The derailment caused a series of explosions and fires that destroyed 44 buildings. A large quantity of crude oil was spilt into the nearby rivers and lake. Forty-seven people were killed. The destruction included residences; more than one third of the population, both families and businesses, was relocated for days or weeks. Many individuals were never able to return home. In a community that size, almost everyone experienced loss, either through displacement or through grief: knowing or being related to someone who died.
Complicated grief (CG) develops more often when death is sudden, unexpected, or violent (Djelantik, et al., 2020; Shear, 2015; Tessier-De Montgolfier, 2010) and differs from normal grief by the persistence of different symptoms for longer than 12 months following the loss (Shear, 2015). CG is particularly likely to occur following the death of a significant person resulting from accidents or tragedies caused by human negligence or technical failures (Kristensen et al., 2012).
Industrial activities significantly increase the risk of explosions, fires, and maritime or rail disasters (Swiss Re Institute, 2017); these events can cause unexpected and violent deaths. Compared to natural disasters, those of a technological nature have long-lasting consequences on psychological health (Bromet et al., 2011; Chung & Kim, 2010; Morgan & Bhugra, 2010). The prevalence of CG in a post-disaster context varies, ranging from 10% to 20% (Rynearson et al., 2002) and up to 95% of bereaved people (Cardoso et al., 2017; Djelantik et al., 2020). Complicated grief in the context of train accidents has received little attention: in the 39 studies focused on grief in the wake of a disaster (Maltais et al., 2020), only one concerned a train derailment (Sigh & Raphael, 1981). In Europe, nearly 2,000 people are killed in train accidents each year (Eurostat, 2018).
Complicated grief has numerous consequences. The prevalence of depression ranges from 10% to 45% (Kristensen et al., 2012). Post-traumatic stress disorder manifests in individuals experiencing CG following a tragic event like a natural or a technological disaster (Kristensen et al., 2012; Suar et al., 2015; Sveen et al., 2016). In the case of disaster, the traumatic circumstances surrounding the loss can also result in morbid or even suicidal thoughts (Dyregrov et al., 2015; Huh et al., 2017; Kim et al., 2017; Suar et al., 2015).
Complicated grief can have adverse consequences on the physical health of the individuals experiencing it: sleep problems (Tessier-De Montgolfier, 2010), chronic diseases such as hypertension (American Psychiatric Association, 2013; Shear et al., 2013), and various other heart issues, such as infarction and arrhythmia (Shear, 2015; Shear et al., 2013; Tessier-De Montgolfier, 2010). Alcohol consumption sometimes increases in the months following a death (American Psychiatric Association, 2013; Tessier-De Montgolfier, 2010), a phenomenon often observed following a disaster (Huh, et al., 2017; Suar et al., 2015). The use of alcohol, drugs, or medication can amplify ruminating thoughts, depression, and despair, while degrading the general state of health (Tessier-De Montgolfier, 2010).
Grief after a disaster can cause individuals to no longer feel at home or to identify with their community (Malone et al., 2011). Social roles and recreational activities can be impacted by CG, causing an avoidance of contact (American Psychiatric Association, 2013; Hagl et al., 2015; Malone et al., 2011; Shear, 2015; Shear et al., 2013). Disengagement with a social network can complicate grief (Hu et al., 2015; Kristensen et al., 2012; Shear, 2015).
Various sociodemographic characteristics are associated with greater risk of complicated grief. Those characteristics include being female (American Psychiatric Association, 2013; Tessier-De Montgolfier, 2010), over 60 (Lundorff et al., 2017; Shear et al., 2013), divorced (He et al., 2014) as well as having lower socioeconomic and education status (Boelen et al., 2016; He et al., 2014). Low self-esteem (Tirgari et al., 2016) and a history of mood disorders increases the risk (Shear, 2015).
Another risk factor for complicated grief is the relationship with the deceased (Li et al., 2015). Higher prevalence of CG has been observed among parents, spouses (especially widows) and siblings: the loss of first-degree relatives (Dyregrov et al., 2015) and not the number of bereavements (Kristensen et al., 2010; Rajkumar et al., 2013). Grief can also be complicated by experiencing for the first time (Tessier-De Montgolfier, 2010) as well as holding blame for the death, either of self or other (Kristensen et al., 2012; Zech, 2006).
Purpose of the Present Study
The present study focuses on the Lac-Mégantic train derailment to better identify the differentiating factors between those suffering from complicated grief from those experiencing a ‘normal’ grieving process. We tested two hypotheses: (1) The presence of complicated grief would be associated with post-traumatic stress disorder, psychological distress, mood disorder, depression, anxiety, negative perception of one’s physical health, alcohol abuse, and anxiolytic and antidepressant use; and (2) The sociodemographic and contextual factors that contribute to the presence of complicated grief would be being female, coming from a lower economic background, being unemployed, having suffered the loss of an immediate family member, and having been highly exposed to the tragedy (e.g., suffering material losses and having a negative perception of the event in addition to the loss).
Method
Procedure
This study was conducted three and a half years after the train derailment. All procedures performed in studies involving human participants were in accordance with the ethical standards of two institutional committees: CER-UQAC (602.21.12) and Centre intégré universitaire de santé et de services sociaux de l’Estrie-Centre hospitalier universitaire de Sherbrooke (2017-544) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
In October and November 2016, by contract with the researchers, a professional polling firm recruited and surveyed, from randomly generated telephone numbers, participants 18 and over residing in the regional municipality of Granit (MRC du Granit). Of the 800 people surveyed, nearly half (n = 387) were living in Lac-Mégantic. The response rates were 47.8% for residents living in Lac-Mégantic and 50.1% for residents living elsewhere. Individuals were asked to answer a close-ended questionnaire either online or by telephone; interviews lasted no more than 30 min. Consent was obtained; participants were informed that they were free to skip any questions and to end the survey at any time without penalty.
Of the total 800 surveyed, 268 were bereaved. Those who had not experienced the loss of a family member or friend were removed from the sample.
Participants
Of the 268 bereaved, they were mostly female (63.8%), 50 years or older (68.6%), married (65.2%), and employed (53.3%). No significant socio-demographic differences existed between the groups of participants. Seventy-one people (26.5%) had experienced complicated grief since the event: they scored 26 or higher on the Prigerson et al.’s Inventory of Complicated Grief Scale (1995). The average score on this scale is 34.4 for those with complicated grief compared to 13.0 for those without it.
At the time of our data collection, the definition of Complicated Grief (CG) and Inventory of Complicated Grief (ICG; Prigerson et al., 1995) were the standard for research. Since then, new constructs have emerged (Eisma et al., 2020; Treml et al., 2020): Prolonged Grief Disorder (PGD) and Persistent Complex Bereavement Disorder (PCBD). PGD represents the ICD-11 perspective and is measured using the PGD-13 (Prigerson & Maciejewski, 2008). PCBD reflects the DSM-5; the PCBI is the measure (Lee, 2015). All three constructs have theoretical and empirical similarities and differences (e.g., Bonanno & Malgaroli, 2019; Maciejewski et al., 2016). The CG appears as a construct distinct from those of PCBD and PGD, with its limitations and shortcomings (Maciejewski et al. 2016); the most notable strength is its prevalence. This facilitates comparison with a large number of empirical studies that have used this concept and the ICG.
Measures
Socio-demographic questions concerned gender, age, marital status, education, gross family income in the last year, main source of income (full-time work, part-time work, old-age pension, or other), living alone or with at least one other person, and living with children under 18 years of age.
The Inventory of Complicated Grief (Prigerson et al. 1995) focuses on two elements: symptoms of separation distress (e.g.: nostalgia) and traumatic distress (e.g.: bitterness, avoidance). The 19 items require participants to indicate how often they have experienced each symptom since the death. The options range from never (0) to always (4). A score of 26 or higher corresponds to complicated or pathological grief (Prigerson et al., 1995). In this study, the alpha coefficient is .91.
The Impact of Event Scale (IES; Horowitz et al., 1979) consists of 15 items relating to intrusion or avoidance in a post-traumatic situation. The four response options address the frequency of each symptom during the last week. Scoring ranges from 0 to 75 points. Moderate risk post-traumatic stress disorder is represented by scores between 26 and 43; with high risk above 44 (Ticehurst et al., 1996). The alpha coefficient is .92 for the overall score.
The six-item Psychological Distress Scale (Kessler et al., 2002; Orpana et al., 2009), includes questions on feelings of nervousness, hopelessness, agitation, depression, discouragement, and uselessness felt over the course of the previous month. Each item is rated on a 4-point scale, for a total score ranging from 0 to 24. The higher the score, the greater the psychological distress. According to the Institut de la statistique du Québec (Baulne & Courtemanche, 2016), people with a score of 7 or more are suffering from psychological distress. The alpha coefficient of this test is .85.
The presence of depressive symptoms was determined by two questions about whether participants felt sad or depressed for at least 14 consecutive days in the past 12 months and whether they had experienced a loss of interest in the things they usually liked. Participants who answered yes to both questions were considered as having symptoms of depression. They were also asked to identify whether they had a mood disorder, such as depression, bipolar disorder, mania, or dysthymia, and whether they had an anxiety disorder, such as a phobia, obsessive-compulsive disorder, or panic disorder.
The Multidimensional Scale of Perceived Social Support (MSPSS: Zimet et al., 1988) measures three dimensions of social support: from family members (4 questions), from friends (4 questions), and significant people (4 questions). Participants are asked to choose from strongly disagree (1 point) to strongly agree (7 points). The scores range from 12 to 84 points. A score of 69 points or more represents a high level of social support whereas 12 to 48 points indicates a low level of social support (Bergeron & Hébert, 2004). The alpha coefficient for this test is .93.
Participants were also asked about changes in their personal, marital, family, and social life since the event. Changes could be positive or negative. They were also asked about medication and to estimate whether the frequency of their alcohol consumption had changed in the years since the train derailment.
Results
Of the 268 bereaved individuals surveyed three and a half years after the train derailment, 35 had lost immediate family members (child, spouse, brother, sister, or parent), 102 experienced the death of one or more extended family members (cousin, uncle, aunt, brother-in-law, or sister-in-law), and 198 one or more members of their social network (friend, neighbour, or work colleague). It was not possible to determine if participants had experienced multiple losses in any one category. Seventy-one people (26.5%) of the 268 experienced complicated grief.
Hypothesis One
Our first hypothesis was “The presence of complicated grief is associated with psychological problems (post-traumatic stress disorder, psychological distress, mood disorder, depression, and anxiety), negative perception of physical health, alcohol abuse, and use of anxiolytic and antidepressant”. To test this hypothesis, we conducted standard analysis of variance (ANOVAs) with Chi-square and t tests.
Participants who lost one or more immediate or extended family members were significantly more likely (p <0.05) to experience CT (33.1%) than those who experienced deaths in their social network exclusively (20.8%). People with CG were significantly more likely (p <0.05) to have feared for their physical wellbeing (50.8%) during the train derailment than those without CG (33.6%). Daily (versus no) exposure to the destroyed town center increased the likelihood of CG (69.0% versus 54.8%, p <0.05).
One quarter of those with CG rated their physical health as fair or poor compared to those without CG, (25.4% versus 11.7%, p <0.05). Similarly, nearly 60% considered that their health had deteriorated (59.2% versus 21.9%, p <0.001%).
Participants with CG were significantly more likely to present signs of post-traumatic stress disorder (84.5% versus 45.2%, p <0.001), psychological distress (52.1% versus 23.4%, p <0.001), and mood (22.5% versus 10.7%, p <0.05) or anxiety disorders (31% versus 15.2%, p <0.01). They were also more likely to have experienced a depressive episode in the last 12 months (59.2% versus 26.9%, p <0.001) and to have consulted a psychologist (23.9% versus 9.1%, p <0.01) or a social worker during the same period (21.1% versus 10.7%, p <0.05). Depressive episodes were much more common among those grieving family (45.2% versus loss in network 20.8%, p <0.01).
Those with CG were significantly more likely to have abused alcohol at least once a week in the past 12 months (14.1% versus 10.2%, p <0.01) and noted that their consumption had increased (19.7%), compared to those without CG since the event (10.7%, p <0.01). More than one third of those with CG (34.3%) had received a prescription for anxiolytics in the prior year, while more than a quarter (28.2%) were taking antidepressants, more than double those without CG (p <0.01). People with CG had a more negative perception of the future (31% versus 19.3%) and of life in general (25.4% versus 14, 2%) following the train derailment (p <0.05).
Tables 1 and 2 demonstrate that participants experiencing complicated grief are also significantly less likely to have access to a high level of social support from their social network (52.1% versus 69.5%, p < 0.001) than bereaved people not in this situation. Moreover, more of the participants experiencing complicated grief noticed a deterioration in their relationship with their relatives (p <0.01) and a decrease in their leisure time (p. <0.01) over the last three years. However, there is no significant difference between participants in terms of the quality of their relationships with their spouse, their children, their parents, or their siblings. In the same way, no difference exists between the two groups in terms of the frequency and quality of their contacts with the various members of their social networks, as well as the number of social activities held outside their homes.
Personal and Family Life of Participants.
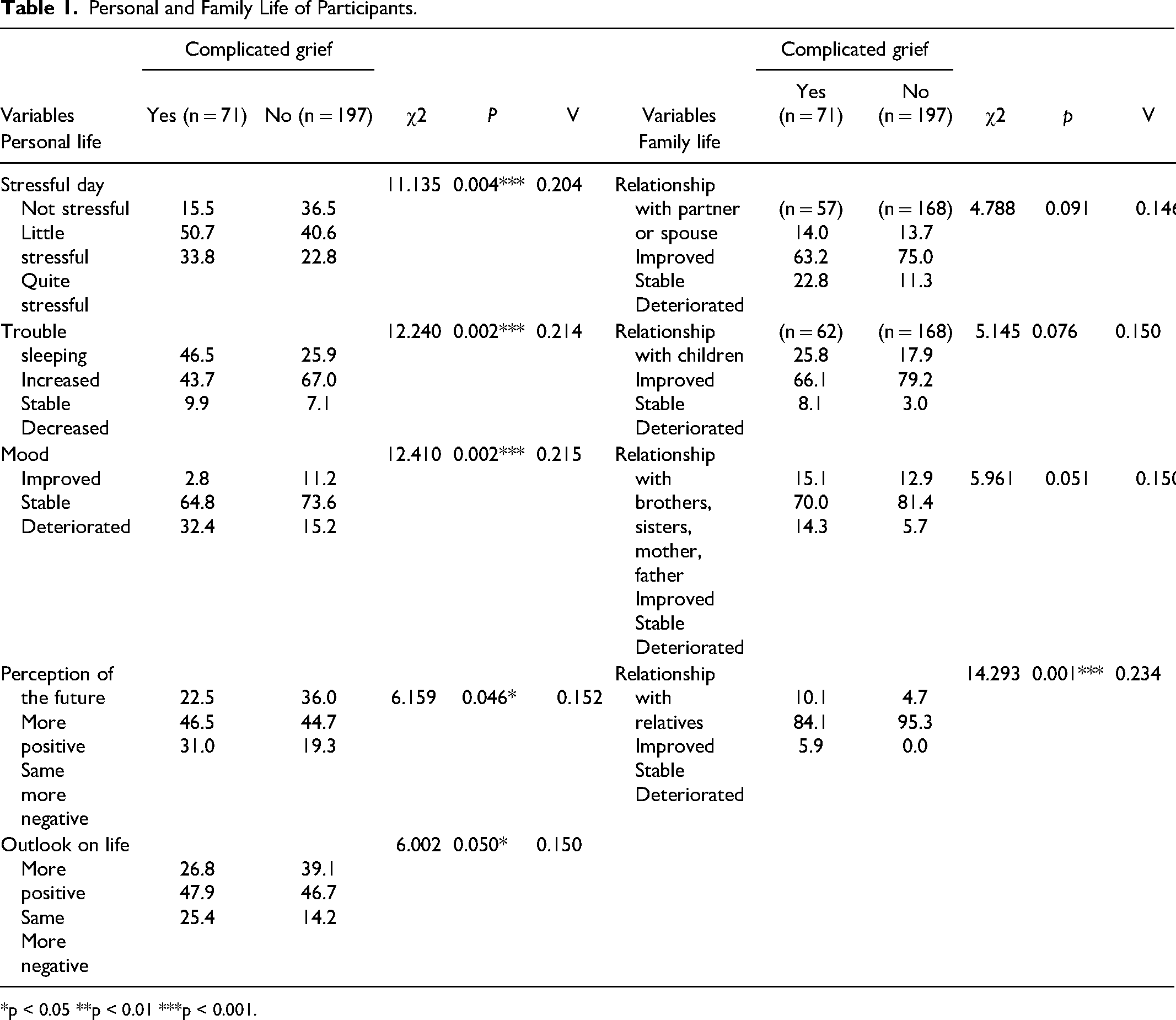
*p < 0.05 **p < 0.01 ***p < 0.001.
Professional and Social Life.
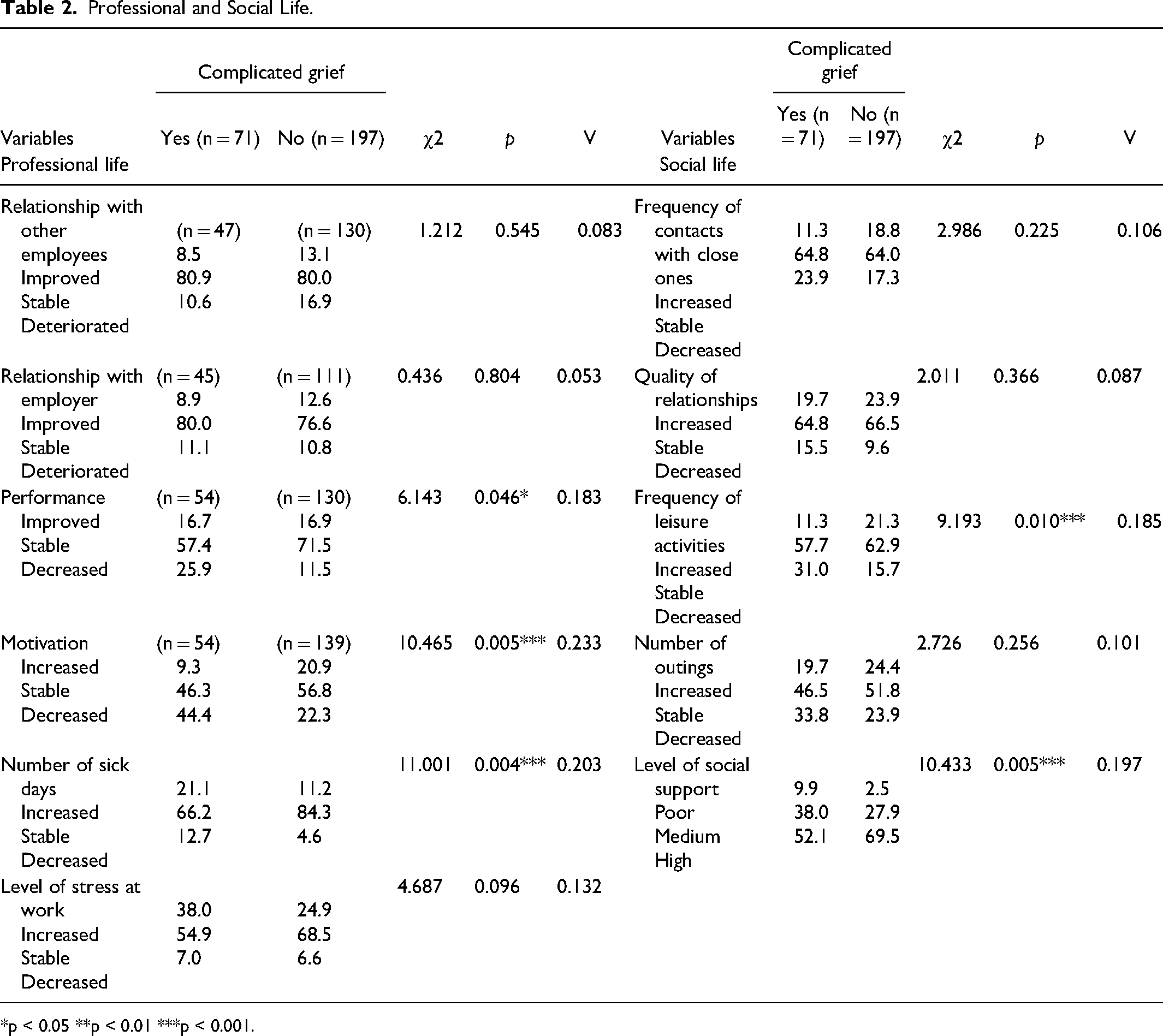
*p < 0.05 **p < 0.01 ***p < 0.001.
With regards to professional life, experiencing complicated grief has negative impacts on motivation at work (p <0.001), job performance (p <.05), and number of sick-leave days they have taken in the last three years (p <0.001).
Hypothesis Two
Our second hypothesis was “The socio-demographic and contextual factors that contribute to the presence of complicated grief are being female, having low-income background, being unemployed, having suffered the loss of an immediate family member, and having been highly exposed to the tragedy (e.g., suffering material losses and having a negative perception of the event in addition to the loss)”. To test this hypothesis, we performed a hierarchical logistic regression analysis. For the dependent variable, we created a binary based on the ICG threshold: those with scores over 25 are considered to have complicated grief. Other variables were categorized into four blocks: socio-demographic variables, social support, link with the deceased and level of exposure. A total of 10 variables were selected for the regression analysis based on their relevance in the literature (see Table 3).
Hierarchical Logistic Regression Analysis of the Complicated Grief (n = 268).
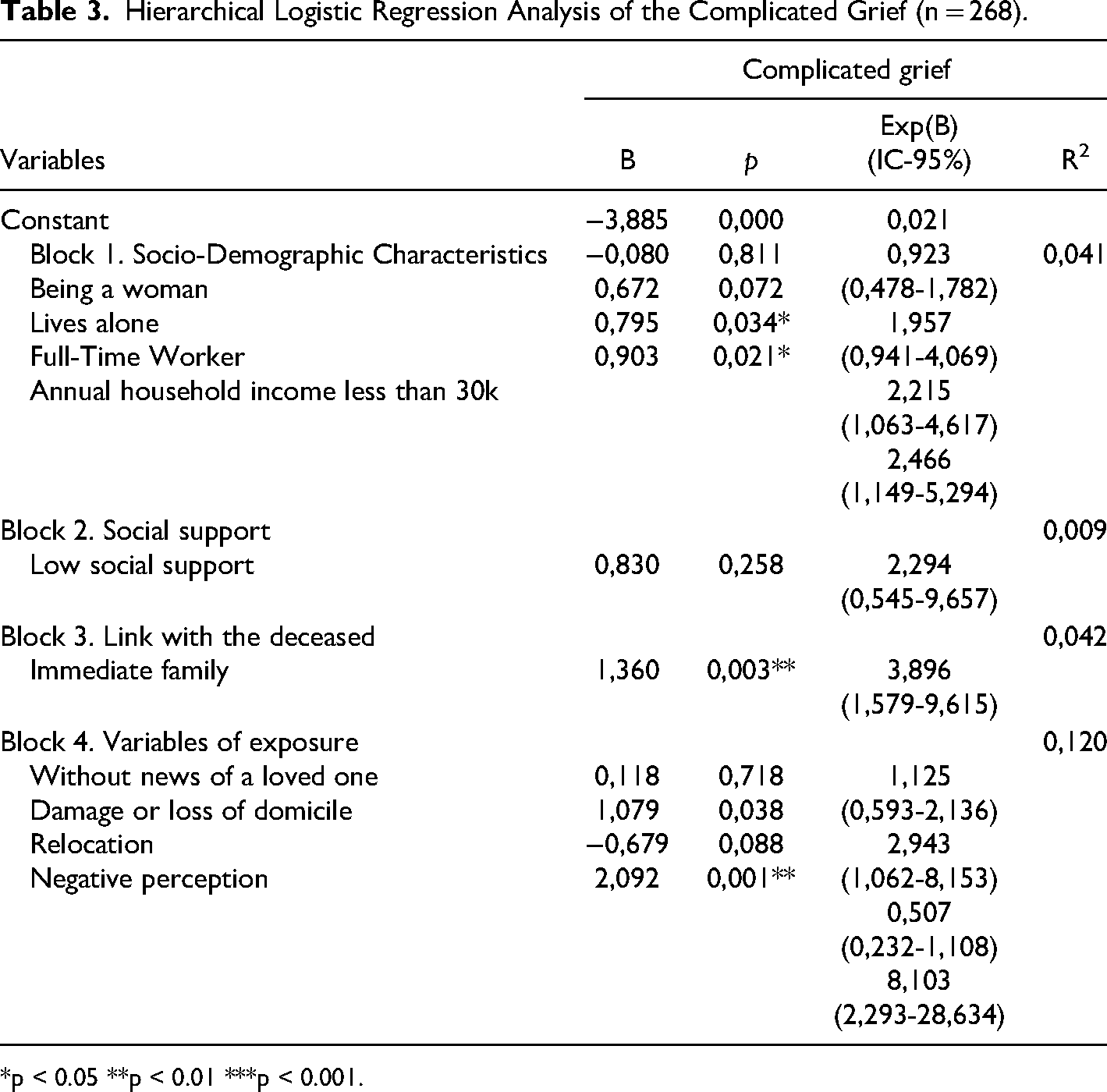
*p < 0.05 **p < 0.01 ***p < 0.001.
According to Nagelkerke’s R2, the selected variables explain 21.2% of the presence of CG. The share of each of the blocks is shown in Table 3. Exposure to the disaster variables further explains the presence of CG (R2 = 0.120), followed by the deceased being a member of the participant’s immediate family (R2 = 0.042). Having an annual income of less than $30,000 doubles the risk of developing CG (B = 0.903, p = 0.21). Similarly, participants with full-time jobs were twice as likely to experience CG (B = 0.795, p = 0.034). On the other hand, having low social support does not appear to complicate the participants’ grief according to this model. Participants who lost an immediate family member had nearly fourfold higher odds of developing CG (B = 1.360, p = 0.003). Finally, the participants’ negative perception of the Lac-Mégantic tragedy multiplied by eight (B = 2.092, p = 0.001) the odds of having complications in the grieving process. However, the variations in the reliability interval of the latter measure are quite large (from 2.293 to 28.634), which may increase the degree of uncertainty of this ratio.
Discussion
The Lac-Mégantic train derailment killed 47 people, including several children and young adults, in a town of 6,000 inhabitants. More than three years later, just over a quarter (26.5%; n = 7) of those bereaved (N = 268) showed signs of complicated grief. By comparison, the prevalence of CG is estimated at between 9.5% and 11% in the context of death by natural causes (Lundorff et al., 2017; Maccalum & Bryant, 2013). Disasters, whether natural, technological, or man-made, have been shown to increase the risk that individuals confronted with a sudden and unexpected death will find it more difficult (Kristensen et al., 2010, 2012; Neria et al., 2007). The prevalence of CG in studies carried out months and years after the collapse of the World Trade Center rose to 43% (Neria et al., 2007) or to 56% (Shear et al., 2006). For adults who lost a family member in the 2004 tsunami, this percentage was of CG 62% (Johannesson et al., 2009).
Our results confirm the impact of CG on physical and psychological health, as well as the negative impact of complicated grief on various aspects of adult life. The increased consumption of alcohol and prescription medication in our sample may be explained by post-traumatic stress, psychological distress, and depression caused by the difficulty of coping with the loss. Several studies on the disaster consequences have shown that the presence of post-traumatic stress disorder, as well as signs of depression and anxiety, is associated with troubles in the personal and professional relationships of the people exposed to the event (Boelen, 2013; Ekanayake et al., 2013; Li & Prigerson, 2016; Shear, 2015; Shear et al., 2013; Suar et al., 2015). Accordingly, there are often multiple concurrent health problems, both for those suffering from CG or post-traumatic stress (Lie et al., 2015; Suar et al., 2015; Sveen et al., 2016).
The logistic regression analyses demonstrate that a high exposure level to the disaster, having feared for one’s life or physical wellbeing or that of someone close, having suffered material damage (relocation or damage to their home), and having a negative subjective perception of the event are all important factors contributing to the presence of CG. These results are consistent with the notion that bereavement in the context of disaster accentuates the stress reactions and defense mechanisms of grief, such as blaming oneself or others (Johannesson et al., 2011; Kuo et al., 2003; Shultz et al., 2012). Injuries, witnessing people dying and the accumulation of losses (e.g., house, furniture, sources of income) have all been associated with the development of CG (Cardoso et al., 2017; Ghaffari-Nejad et al., 2007; Johannesson et al., 2009; Hagl et al., 2015; Shultz et al., 2012).
Our results also indicate that having a low-income background increases the risk of experiencing CG. This may be due to less access to psychological support, because to a lack of time or income. It is important to make support services accessible and available, in work and community, particularly for low-income people.
The Lac-Mégantic event caused a series of negative consequences in the town, including the complete destruction of the popular downtown area and the loss of several dozen jobs. Daily life was disrupted. The constant media gaze that resulted interrupted the potential for support that individuals could provide to each other. Cardoso et al. (2017) conducted a study ten years after the collapse of a bridge; they found that the media coverage of the event increased the risk of complicated grief.
Study Limitations
While the results demonstrate the impact of complicated grief on the overall health of bereaved people, they cannot be generalized to all those exposed to other types of disasters. The cross-sectional approach does not allow for consideration of pre-existing factors that could contribute to CG. Other stressful events, such as job loss, major life, or work changes, or losing another significant person before or after the tragedy are other pre-existing possible factors (Arnberg et al., 2011; Barry et al., 2002; Chan et al., 2012; Shear, 2015; Tessier-De Montgolfier, 2010; Tirgari et al., 2016). The lack of information on the participants’ attachment style and the frequency and quality of relationships with deceased relatives limit the interpretation, given that those are important considerations in CG (Maccallum & Bryant, 2013, 2018).
It is also possible that some people with complicated grief who refused to complete the telephone survey had differing socio-demographic characteristics and health status than those who volunteered. Some participants may not have been completely honest when it came to questions about their psychological health, especially regarding mood disorders, anxiety, or depression, and whether they had been diagnosed by a health professional. The use of validated tests for these last items would have been preferable, but since data was collected through a telephone survey, some questions had to be prioritized over others. The high number of participants in the two groups is, however, a positive factor in the internal validity of the results.
Conclusion
The results of our study are consistent with other studies of complicated grief following a technological disaster, be it is a train derailment (Sigh, & Raphael, 1981), a plane crash (Johannesson et al., 2006; Lenferink et al., 2017) or a marine accident (Arnberg et al., 2011; Han et al., 2017; Huh et al., 2017). Our study shows that people experiencing complicated grief are at greater risk of presenting various mental health problems and social functioning problems than those who are not. Unlike other studies, gender was not a factor that contributed to complicated grief in the Lac-Mégantic community. Nevertheless, our study is in line with other research that shows that losing a member of one’s immediate family remains a risk factor: an important finding for supporting those facing the consequences of a violent death (Djelantik et al., 2020; Klass & Steffen, 2017). Moreover, this study shows that having a full-time job or modest income are factors that contribute to complicated grief. This demonstrates the importance of offering support services in the workplace, especially when individuals are low-income earners.
The implications for health and social service providers are important. The participants with complicated grief consulted psychologists and social workers more than those without CG. People at risk of complicated grief need to be identified and monitored since they are more at risk of developing mental and physical health issues. They require both listening and emotional support, not only from health and social services professionals, but also from those around them (Breen et al., 2020). This is especially pertinent since many of those with complicated grief (n = 34, 47.9%) indicated that they feel they do not always receive enough help from friends and family members when they need it or when they feel the need to share their feelings (which equates to a low or medium level of support).
In future studies on the consequences of technological disasters, it would be interesting to establish the coping strategies of the different groups of bereaved individuals and to see if those experiencing complicated grief employ different strategies to help them to deal with the grief. Obtaining information on the pre-disaster health status of the victims and their immediate family members as well as other life events that may have disrupted their psychological state would also be helpful in interpreting post-disaster data. In addition, it would be useful for statistical analysis purposes to know the exact number of deaths for each of the bereaved to determine if this variable is related to the presence of complicated grief. Conducting a study with participants experiencing complicated grief and post-traumatic stress disorder after a disaster would also make it possible to identify what factors are important in this situation.
Footnotes
Data Availability
The data and material will be available at: https://dataverse.scholarsportal.info/dataverse/LacMegantic or by request at Université du Québec à Chicoutimi, included supplementary information or figure source of data files. Contact: Danielle Maltais: danielle_maltais@uqac.ca
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Social Sciences and Humanities Research Council of Canada, (grant number 77666).
Author Biographies
Since January 1994,
Dr