
Abstract
Despite evidence for the usefulness of augmentative and alternative communication (AAC) for young children with complex communication needs (CCN), several barriers prevent children from accessing AAC intervention. This qualitative study is focused on understanding the lived experiences of parents accessing and learning how to use speech-generating devices with their young children (3-6 years) with CCN. Findings generate insight into the similarities and differences across families’ experiences through several categories and themes: (a) foundational perspectives (determination and resilience; finding balance); (b) experiences getting access to an AAC device (initiating access; navigating barriers); (c) experiences using an AAC device (learning and navigating challenges; supporting their child’s communication at home and in the community; seeing progress); and (d) surrounding factors (family structure, informal supports, and demands; access to services and professional supports; the COVID-19 pandemic). Implications for practice and policy are discussed related to how to improve AAC access and intervention.
Keywords
A child’s early years are a formative developmental period, and communication is at the center of this learning. Children’s communication and language learning acts as a vehicle for broader development, shaping cognitive, social, and literacy-related learning (Kaiser & Trent, 2007). Yet, building effective communication skills is complex. Many young children with disabilities have complex communication needs (CCN)—including children who are nonspeaking and who do speak but cannot meet all of their day-to-day communication needs using speech alone (Beukelman & Light, 2020). Children with CCN often experience considerable challenges with everyday communicative interactions, which can have a cascading impact on their learning, social participation and relationships, access to inclusive environments, behavior and self-determination, and overall quality of life (Drager et al., 2010). Therefore, early intervention and early childhood education must involve protecting and promoting all children’s right to communicate (Biggs & Meadan, 2018).
Augmentative and Alternative Communication
Technologies and interventions associated with augmentative and alternative communication (AAC) have undergone substantial development in recent decades, and AAC intervention is an evidence-based practice for children who have CCN (Drager et al., 2010; Ganz et al., 2017; Light et al., 2019; Morin et al., 2018). AAC refers to ways of communicating besides spoken language, including when other communication modes are used alongside or in place of speech (Beukelman & Light, 2020). There are two main types of AAC—aided AAC and unaided AAC. Unaided AAC includes ways of communicating that do not require additional tools outside the body, such as gestures, facial expressions, and manual signs. Aided AAC refers to the use of external tools for communication (e.g., boards or books with picture symbols, and high-tech speech-generating devices [SGDs]). Determining the prevalence of young children who would benefit from AAC is challenging because difficulties using verbal speech for communication may result from differences or impairment across many domains (e.g., cognitive, motor, social, linguistic, sensory; Beukelman & Light, 2020). However, the need for effective AAC intervention with children with disabilities is great. Using data from multiple studies, the Rehabilitation Engineering Research Center on Augmentative and Alternative Communication (RERC-AAC, 2019) estimated that approximately 95% of young children with cerebral palsy, 80% with Down syndrome, 50% to 60% with autism, and 50% to 60% with other intellectual and developmental disabilities would benefit from AAC intervention.
A strong and growing body of research indicates that children with CCN can learn to use high-tech SGDs and that doing so can improve children’s outcomes (Ganz et al., 2017; Kasari et al., 2014; Lorah et al., 2022). For instance, Kasari et al. (2014) conducted a randomized controlled trial with 61 children with autism who were minimally verbal (5-8 years). One group of children received a blended developmental-behavioral intervention that focused on speech alone; the second group of children received the same intervention with the addition of an SGD. Kasari and colleagues found that children in the SGD group showed greater improvements in language and communication than those whose intervention did not include AAC (Kasari et al., 2014). Other research shows similar outcomes of AAC intervention for even younger children, such as toddlers and early preschoolers (Romski et al., 2010; Walters et al., 2021). Beyond improving language outcomes, effective AAC intervention in young children can have a cascading impact on other areas of development, including social skills and relationships, academic skills, and challenging behavior (Romski et al., 2015).
Barriers and Facilitators to AAC Access and Use With Young Children
Despite the evidence for the effectiveness of AAC intervention for young children, persisting myths and misperceptions create barriers to early AAC access (Romski & Sevcik, 2005; Sigafoos et al., 2021; Walters et al., 2021). Romski and Sevcik (2005) explained three common but unfounded myths: (a) AAC is the last resort in intervention, (b) AAC hinders or stops further speech development, and (c) children must have a certain set of skills or be a certain age to benefit from AAC. Research evidence demonstrates that these myths are false; however, they still impact early access to AAC for young children who could greatly benefit from it (Sevcik et al., 2008; Walters et al., 2021). Although no known study has directly addressed how widespread these myths might be, Wilcox et al. (2006) found the majority of service providers felt there were young children on their caseload who should have been using assistive technology such as AAC but were not doing so. Lorang et al. (2022) surveyed 376 speech-language pathologists (SLPs) to better understand the limited use of AAC with young children birth to 3-years-old. They found that SLPs were more likely to introduce AAC to children who were not yet speaking and less likely to introduce AAC to children who were already using even a small number of spoken words. They were also more likely to use sign language and low-tech aided AAC (e.g., photographs and pictures) over high-tech aided AAC (e.g., SGDs and switches).
Given this landscape, it is clear that early interventionists, teachers, and service providers have critical roles not just in providing direct services to children with CCN but also in (a) identifying children who might benefit from aided AAC and (b) dispelling myths that might hinder effective communication support. Binger et al. (2012) described the role of an “AAC finder” in an interdisciplinary team. Such a person facilitates AAC access by identifying children who might benefit from AAC and then facilitating referral to professionals with AAC assessment expertise. Rather than being one specific role or professional, many different people can act as an “AAC finder,” including family members, family friends, service providers, educators, and medical providers (Binger et al., 2012).
Nonetheless, access to AAC by itself is not enough to lead to desired outcomes. Learning to use aided AAC takes time and teaching, and children need the people around them to value, recognize, and support their communication (Biggs et al., 2019). Young children learning to use SGDs or other forms of aided AAC need (a) opportunities within their natural environments to learn language and communication and (b) communication partners in these environments who are responsive to children’s communication attempts and who scaffold and support children’s use and learning of language with AAC and speech (Biggs & Meadan, 2018). Because a young child’s home is their most important environment, their parents and other family members are their most important communication partners. Thus, there has been increasing focus on improving the family-centeredness of AAC services and on equipping professionals to partner with families to support AAC use and strong communication outcomes in the home (Coburn et al., 2021; Douglas et al., 2022; Mandak et al., 2017).
Families often find it complex to integrate SGDs or other forms of AAC into their day-to-day interactions. In their survey of early-intervention SLPs, Lorang et al. (2022) found more than one-third felt caregiver buy-in was the most significant barrier to AAC implementation. Many studies have focused on family rejection of AAC devices (i.e., dismissed prior to any attempt) and abandonment (i.e., discontinued use despite ongoing need), revealing several key barriers: (a) persistent myths may slow or prevent looking to AAC as an option, (b) professionals may lack training and knowledge about AAC, (c) families may experience difficulty accessing quality intervention services and service providers, (d) families may struggle to support AAC given the other demands or responsibilities they juggle, (e) families may be dissatisfied with the AAC systems selected for their child, and (f) families may feel isolated and lack support when they are trying to use AAC in the home, including lacking support from professionals and others in their social networks (Donato et al., 2018; Johnson et al., 2006; Moorcroft et al., 2020).
Purpose
Gaining a deeper understanding of the views and experiences of families who are using aided AAC in their home may be one of the most impactful next steps for addressing these challenges. For instance, one Australian study involved semi-structured interviews with six parents of children and youth who used SGDs (2-18 years). Parents in this study explained that they faced many challenges, including variability in professionals’ knowledge, lack of communication with service providers, and being placed on long waiting lists. They also emphasized the importance of timely, well-coordinated supports and family-centered practices (Anderson et al., 2014). Building on this research, the focus of this study was to understand the experiences of families in the United States who have young children (aged 3-6) learning to use high-tech SGDs. We addressed the following question:
Method
This descriptive qualitative study involved analysis of semi-structured interviews collected as part of a larger study exploring language, literacy, and play at home for young children using SGDs. Qualitative description aims to offer clear but comprehensive descriptions of phenomena in which the analysis and interpretation of findings remain fairly “data-near” (Sandelowski, 2010). Our team’s theoretical framework was pragmatism, meaning that we made decisions about sampling, data collection, and data analysis based on our desire to gain practical understanding about a real-world issue that could then be used to inform action (Patton, 2015). Related to positionality, our research team was comprised of a faculty member (a White female who was the second author) and two undergraduate students (both White females, who were the first and third authors). Two other undergraduate students (a Black female and a Black male) also assisted with data collection. Each member of the research team came with a strong interest in AAC but had varied amounts and types of personal and professional experience with AAC and children with CCN and their families. None of the researchers were AAC users themselves. We used reflexivity to enhance the rigor of this research by reflecting on our positionality and potential biases throughout the research process through critical reflection, team debriefing, and memoing (Patton, 2015).
Participants and Recruitment
Participants were 14 mothers of young children with CCN who were learning to use SGDs. To be included, parents needed to be the parent or primary caregiver of a child who (a) was between 3 and 6 years of age, (b) had access to an SGD at home, (c) accessed the device with a finger or part of the hand, (d) communicated intentionally in any mode, and (e) lived in Tennessee, Illinois, or New York. These three states were chosen so that we could recruit participants from different geographical areas, each with different structures related to early intervention and early childhood special education. Our research team adopted a multi-pronged recruitment approach that involved distributing electronic flyers through community resources, speech-language pathologists working in both school and non-school settings, AAC device companies, and social media. As a strategy to recruit families from diverse and underrepresented backgrounds, we recruited through both disability-related community resources (e.g., parent support groups) and non-disability-related community resources (e.g., faith communities, community centers, and pediatric clinics), anticipating that this multi-pronged approach would be needed to reach families not well-connected to disability-related community resources. Flyers included information about the study and explained to potential parents that the broader project involved approximately 3 to 3.5 hours of activities conducted at times they chose (i.e., an interview, online questionnaires, and two video-recorded observations of parent-child interactions during book reading and play). Participants received US$200 in gift cards and two children’s books for their time. The recruitment materials also directed families to a link to complete an initial screening questionnaire. After a parent completed the online screening questionnaire, a research team member contacted them via a phone call to confirm eligibility.
Table 1 displays information about the mothers and their children. Mothers ranged in age from 31 to 50 years (M = 38.7). The majority were White (71.4%), and all but one had a bachelor’s or master’s degree. The children with CCN were an average of 4 years; 8 months in age (range 3-6 years). Nine were boys and five were girls. Eleven of the children lived in two-parent households. More than half had two or more siblings who lived at home (57.1%); three children had one sibling and three had no siblings. Although annual family income ranged from less than US$10,000 to more than US$120,000, nearly two-thirds of families (64.3%) reported annual household incomes of US$100,000 or more. Five families (35.7%) lived in urban areas and nine in suburban (64.3%). No families were from rural areas. Most families were monolingual English-speaking.
Characteristics of Participating Mothers and Their Children With Complex Communication Needs.
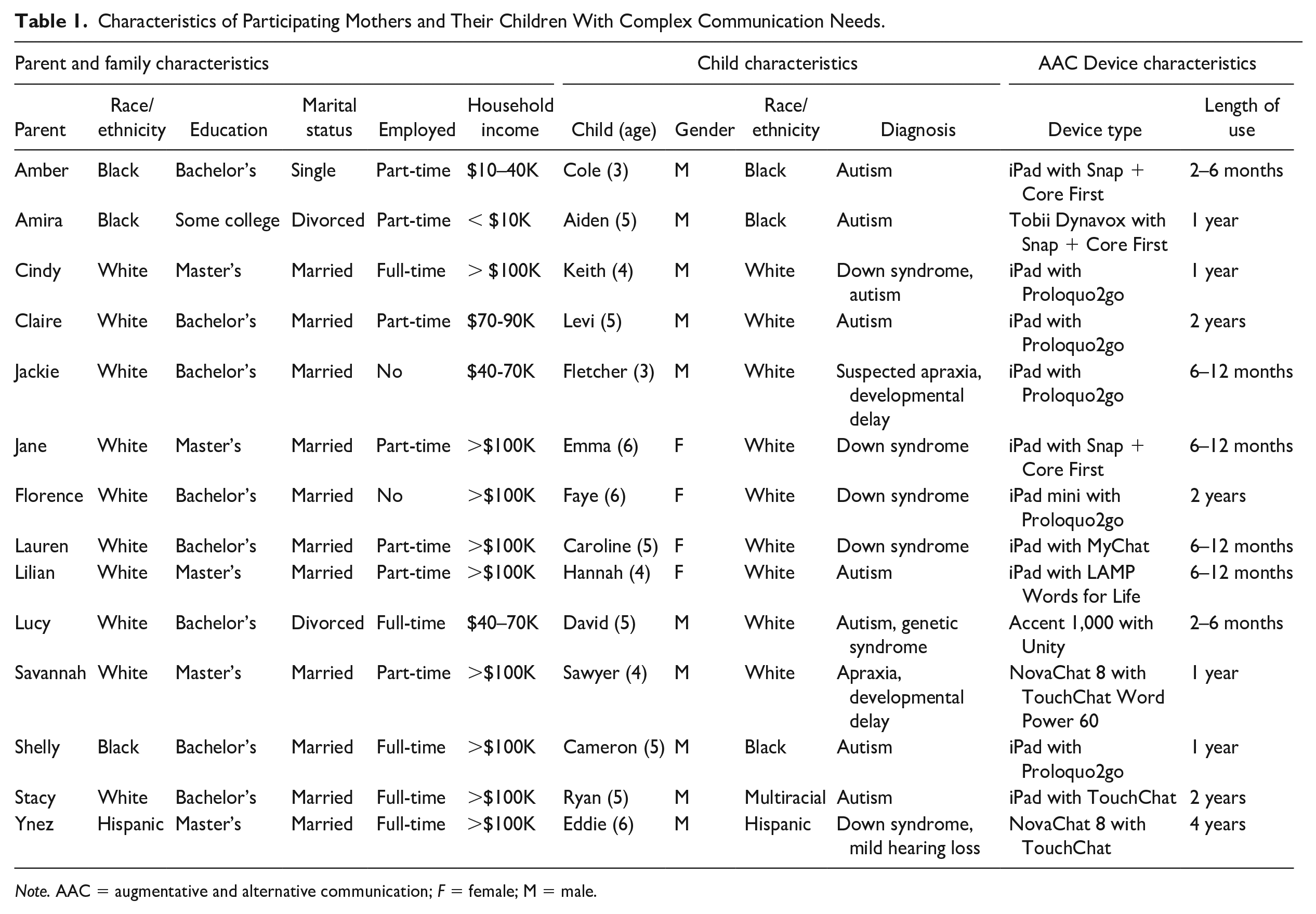
Note. AAC = augmentative and alternative communication; F = female; M = male.
Data Collection
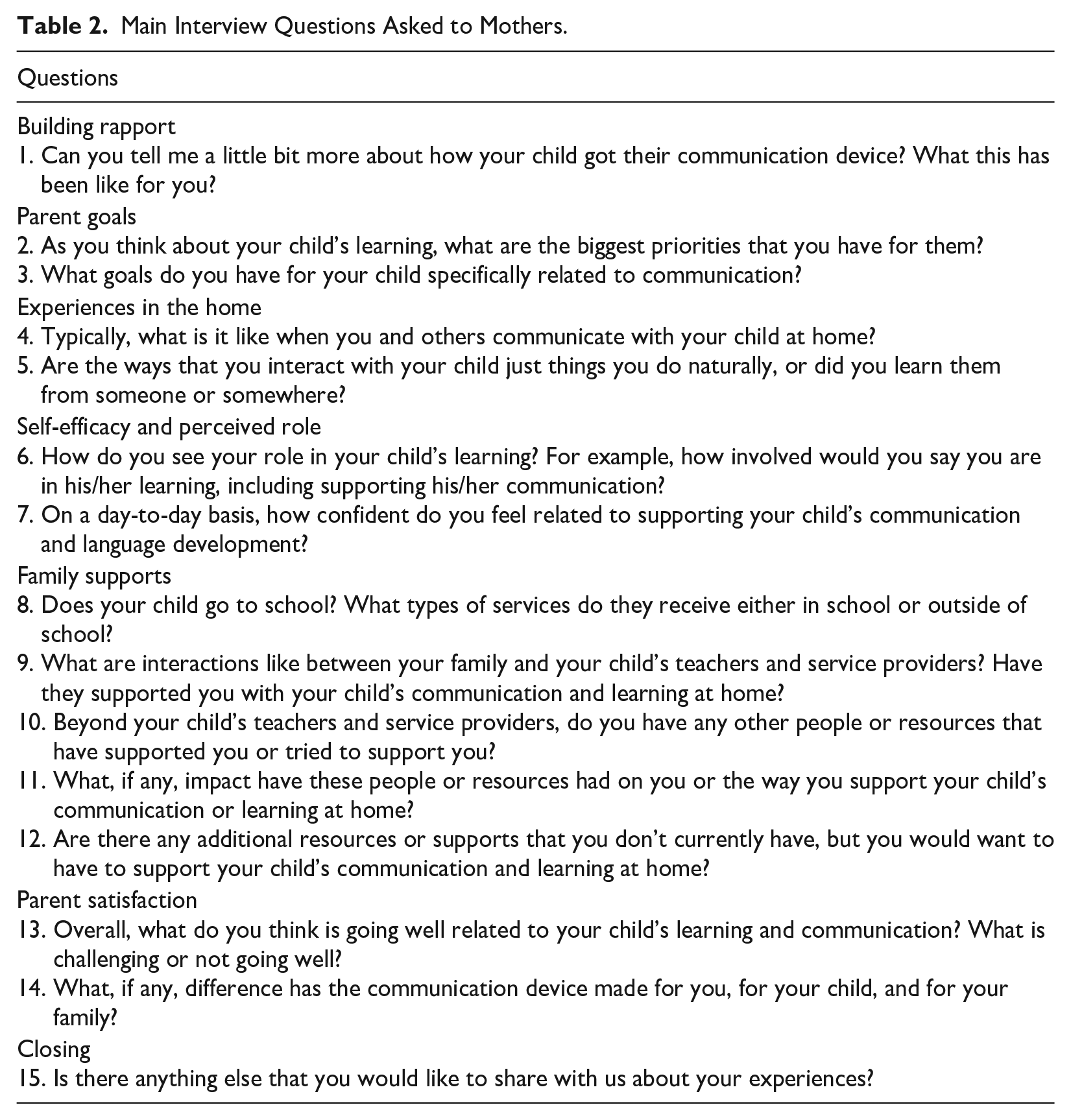
Data were collected through individual, semi-structured interviews with each mother. Interviews were conducted by one of the research team members through an online videoconferencing platform, Zoom. Interviews were audio and video recorded. The length of interviews varied, ranging from 25 to 118 min (M = 57 min). The research team developed an interview guide by reviewing prior research and evaluating conceptual support for each question; then, interview questions were iteratively refined for clarity and usefulness based on feedback from experts and parents of children with CCN. Interviews consisted of 15 main questions (see Table 2). Each interviewer used the interview guide to maintain consistency while adopting a conversational style which involved asking additional follow-up questions to encourage participants to expand on or clarify their responses. To promote collaboration across the research team, each researcher completed a written reflection guide immediately following the interview (Patton, 2015) and discussed the interview with the larger team during weekly meetings.
Main Interview Questions Asked to Mothers.
Data Analysis
In accordance with our pragmatic framework for the study, we analyzed data with a focus on generating insights that could inform action (Patton, 2015). Strategies to ensure rigor and promote credibility and trustworthiness included researcher reflexivity, creating an audit trail of decisions and data, utilizing constant comparison and iterative rounds of analysis, conducting member checks, and triangulating across researchers by engaging in collaborative coding and analysis (Brantlinger et al., 2005; Patton, 2015). We utilized within and across case analysis to strengthen our understanding of families’ experiences (Ayres et al., 2003).
As data were collected, interviews were transcribed verbatim, checked for accuracy, and deidentified. Within 1 to 2 weeks of each interview, we conducted within-case analysis, which involved having the interviewer re-listen to the interview and draft a 1- to 2-page summary of key ideas. Each summary was reviewed by at least two other research team members (who listened to or read the transcript of the interview and then offered comments to improve the summary), and then edits to the summary were finalized by the team member who drafted the summary. We then presented the summary to the participant as a member check (Patton, 2015). We asked participants for written feedback on their summary, which we elicited through two questions: (a) To what extent does this summary reflect your views and perspectives? (b) What would you add or change to make the summary better capture your views and experiences? All participants responded to the member check and said it matched their experiences. In addition, two participants made a few clarifying revisions, and five added additional stories or elaborations. All additions from participants were added to the corpus of data for analysis.
After all of the study data were collected, interview transcripts and member checks were imported into Dedoose (Version 9.0.46) for further analysis across cases. We used an iterative and inductive approach with three rounds of coding, allowing findings to emerge from the data (Saldaña, 2021). Each round of coding involved collaboration through critical discussion and analytic memoing (Patton, 2015; Saldaña, 2021). For the first coding round, each transcript was assigned to two different team members to independently conduct open coding by flagging excerpts in each transcript with relevant codes (i.e., initial coding; Saldaña, 2021). Whenever appropriate, we created in vivo codes that incorporated the participants’ own language in the code name (Saldaña, 2021). After independently coding a set of one or two transcripts, all three authors met to reach an agreement on excerpts and codes. We continuously updated an electronic codebook which included a list of codes, their descriptions, excerpt examples, and relevant notes.
Following open coding, the second coding round began by having all three researchers independently review all of the coded data (through reports of excerpts that were organized by code) and memo about connections between codes and ideas. The team then met to conduct the second round of coding—which consisted of grouping the codes into categories, themes, and sub-themes. The third round of coding then involved the first and second authors revisiting all of the transcripts and excerpts to search for confirming and disconfirming evidence (Patton, 2015). The researchers reviewed excerpts, evaluated the interpretation of each theme, memoed about the properties and dimensions of each theme, and made any needed changes to code applications.
Findings
Findings are organized into four categories: (a) foundational perspectives, (b) experiences getting access to an AAC device, (c) experiences using an AAC device, and (d) surrounding factors. Quotes are attributed to individual participants using pseudonyms.
Foundational Perspectives
The first category of themes related to foundational perspectives of mothers—their attitudes and dispositions that both played into and were shaped by their specific experiences getting access to an AAC device for their child and then using that device. There were two themes: (a) determination and resilience, and (b) finding balance.
Determination and Resilience: “Whatever Will Help My Son” (Amira)
All of the mothers were determined to support their children, and they showed resilience when they were faced with challenges—largely coming from a deep motivation to make sure their children could have a “good life” (Amira) which meant a variety of things for parents. Communication access was a critical part of how they envisioned their child having a good life—they wanted their children to be able to use language and communication to “engage with people” and “establish relationships” (Savannah), “begin learning how to read” (Jane), and communicate “how she’s feeling, or if something happens at school” (Lauren).
Although mothers described similar values and motivations, their determination and resilience manifested in different ways. Florence, Amber, and Jackie talked about their roles as advocates, and they were frequently seeking out ways to ensure high-quality services for their children. Florence explained: I was upfront early on that I wanted her to go [to the same school as her brother] and I wanted her to be included. And, you know, I talked to the principal about different things that we can do . . . that would foster just inclusion and diversity among the whole student body.
Several of the mothers talked about how they had to make weighty, and even costly, decisions to help their child access what they believed would be the best possible education—switching schools, home-schooling, or enrolling their child in therapeutic schools rather than traditional kindergarten programs. Amira had multiple children with disabilities and described the personal sacrifices she made to be able to ensure they could access services: I had to stop working. I only work one day because of [my children] so that they can get better. So I can have time to get them from school and take them to the private therapies and stuff, and just spend a bunch of my time with them. . . . You just keep going and not give up.
Other mothers showed their resilience by pursuing learning opportunities for themselves, whether through online training resources (Jackie, Lilian) or by observing or learning from service providers (Stacy, Shelly, Lucy). For example, Stacy described seeking out formal and informal training sessions with her son’s speech therapist, saying “His therapists have been really, really helpful.”
Finding Balance: “I Don’t Want to Be His Therapist” (Stacy)
Mothers also shared that parenting was challenging, and they often struggled to find peace with the tension between what they wanted for their child and what they felt they could actually provide—they felt deeply invested in supporting their children, but they also knew they could only do so much. Every mother described feeling overwhelmed at times by their role in supporting their child’s development, particularly while juggling other responsibilities. They sought to find balance for themselves in light of the pressure they and others put on them to be so many different things for their child. Lilian was a licensed counselor who had stopped working to stay home with her child. She explained: Being a therapist, I feel like I have a lot of resourcefulness. I like to learn about things. I have a lot of strengths that a lot of parents don't have. I have time. I don't have a job [currently]. . . . But I still feel completely lacking in confidence whenever it comes to being the one. You know, if my child needs to talk, I feel like it’s all up to me. . . . So much of it rests on my shoulders, you know? It’s very overwhelming most days.
As they struggled to find balance, mothers wanted to feel they could truly be their child’s parent, not their therapist. “Sometimes I catch myself being more of a therapist than a mom playing with him” Amber explained. Savannah described wanting to “protect [her] relationship” with her child, and Claire wanted her home to be “a free space.” Lucy emphasized: I don’t want to be a therapist because that’s a lot of specialized work and I don’t have the capacity to do it. I don’t have those skills, and I don’t have that patience. And, you know, I also don’t want David to feel like he’s always in every situation kind of being expected to sort of perform like that, you know? With his mom sometimes he can just, you know, be and let go [of] that.
Parents described wanting to work closely with service providers as they found this balance, but they wished service providers understood how overwhelming was for them to learn about AAC and juggle so many different responsibilities. Lilian explained: I think sometimes they really don’t understand . . . how much complexity there is in language and communication development that we just do not know. You know, the lay person does not know about all these things and you really don’t think about them until you have to. And then once you do, it becomes very overwhelming to know that you make a difference in terms of your child’s language acquisition and their communication ability. . . . So just giving some emotional support, but then also just really understanding how clueless parents can feel, even if we’re educated, even if we’re intelligent, these are just not things that we think about.
Experiences Getting Access to an AAC Device
The second category related to families’ experiences getting access to an AAC device, which involved two themes: (a) initiating the process and (b) navigating barriers.
Initiating the Process: “I Felt Like That Meant He Was Never Going to Talk” (Lucy)
Mothers’ experiences getting access to an SGD varied widely. Some mothers described having good experiences with someone who initiated the process and walked with them throughout each step—in other words, an “AAC finder.” Professionals such as speech-language pathologists, early interventionists, and early childhood educators acted as the “AAC finder,” but family friends did too. Some parents were excited about their provider’s recommendation to trial an SGD with their child. Claire described being thrilled when her son’s speech-language pathologist brought up an SGD after they had been “carrying around a notebook with hundreds and hundreds of little Velcro PECS.” Yet, the idea of an SGD caused fears and hesitation for many parents. Several mothers explained it made them wonder and worry that the communication device would hinder their child’s ability to use speech. Professionals acting as “AAC finders” played important roles in calming parents’ fears and answering their questions. One mother, Shelly, shared: At one point I didn't think it was even a good idea for her. I'm like, “Why does she need a device if she’s starting to say words?” Well, once her therapist told me like “She’ll get more confidence, and then the frustration will go away if she has something near her to like tell you exactly what she wants.” That was the best thing she ever told me. Because once I figured that out it’s like “Oh wow, she does actually have more confidence to communicate.” So, she doesn’t get frustrated.
Some mothers acted as “AAC finders” themselves because they were the ones to initiate the process. When this happened, professionals usually still had important roles. For instance, Lauren initiated getting an AAC evaluation, but then she explained that the school “pushed it for us.” After learning about AAC, Savannah sought out someone with AAC expertise who could assist her in initiating the process. She explained: I reached out to [an AAC consultant] with some questions mainly about the process. Because I didn’t know what the process for this through the school district was, and I just reached out to be educated. I was so thankful I did because, you know, there’s obviously a well-researched process for deciding which device is right for what child, and that was really valuable to us going through the process having that knowledge.
Jackie, however, described being the driving force for getting her son an SGD without a lot of involvement or support from professionals—initiating the process, researching AAC online, trying a few different options at home (i.e., different AAC apps on an iPad), and eventually purchasing something herself. Several factors seemed to contribute to this experience, including that her son’s providers had very limited AAC experience, that Jackie wanted this type of involvement, and that the COVID-19 pandemic impacted services. Jackie explained: I don’t know if we would have been as intensely involved in it to begin with [if it weren’t for the pandemic]. . . . But I don’t regret implementing it ourselves, because I think that I just started with what most people would consider too big [for the set-up of vocabulary on the device]. I really think that gave him more opportunity to expand, rather than being on a small board.
Navigating Barriers: “It Was Extremely Easy” (Amira) vs. “It Was a Process” (Cindy)
Mothers had to navigate many challenges to get their child’s SGD. These challenges included negative perceptions that others held about their child or AAC, administrative procedures and delays, and difficulty with access to funding. For some families, the process seemed “relatively easy.” Ynez explained: Our early intervention speech therapist advised us to start the process early. . . . And so, our early intervention coordinators set up the appointment. We went through the evaluation. And then, based on the results of his evaluation, they made recommendations on the best device.
However, other families were frustrated about the barriers that stymied their journey. Several mothers wished they could have gotten access to a device sooner, explaining that AAC was put off because of professionals’ perceptions that their child was too young or did not have skills that were perceived as prerequisites. Savannah explained that her son was not “on the radar for AAC” because he lacked an official diagnosis. Cindy described starting the process “early” because she felt it was important, but professionals at the time were recommending against AAC because they felt her son was too young. Although she was “happy” to have acquired the device, she felt discouraged that she was “always the one asking for new things” and did not have the support she wanted from service providers. Other mothers were frustrated that service providers argued against certain devices without a lot of rationale. Once the process was finally initiated for her son, Savannah felt that the chosen device was “too simplistic.” When she proposed a different device, she was told that he would move up “once he shows us he can handle that.”
Finding the “best device” (Ynez) was also complicated by funding. Participants primarily described two ways their children’s devices were funded, each having their unique challenges: (a) through insurance or (b) from the school district. Parents who acquired a device through insurance often encountered delays, needing to go back and forth with insurance companies for approval. “Insurance is not happy,” Amber explained, So, I’m still kind of hitting bumps in the road, I guess, because it’s such an expensive device. It’s crazy because his primary insurance is the one that’s given us problems. . . . The whole process has been so lengthy and tricky.
Parents also described delays when they acquired a device through their child’s school, such as having to wait long periods for the device to be sent to their home (Shelly) and facing “device shortages” in the district (Florence). Savannah also added that she considered obtaining a device through her child’s school but ultimately decided to go through insurance to be able to have more “autonomy and control” over the device.
A few parents purchased the device out-of-pocket (Jackie, Lilian, Claire) or obtained funding through another organization or non-profit (Ynez), but they also experienced challenges. Both Jackie and Lilian waited for a sale to purchase an AAC application for their child to use on an iPad. Claire’s claim was denied by insurance, and so she purchased something herself: Our insurance denied the Nuvo. I think it was seven or eight thousand dollars out of pocket at the time. I don’t know may still be that much. But I went back to the speech-language pathologist at our language clinic, and I said, “What is that?” She said it’s an iPad with an app that we buy. And I asked how much it was and, like the Nuvo is also an iPad in a fancy case with a special program on it, and I was like okay $7000 we can’t afford that . . . [So] we bought a used iPad.
Lauren shared what she hoped the process would look like for other families in the future.
I wish these communication devices were more easily accessible. . . . Just seems like our school specifically was instrumental in getting her one; they were very supportive and pushed for it. And I feel like that’s not the case everywhere. We had tried to go through an organization to get one prior to that and we never heard back so [it was] kind of frustrating, especially when they’re super expensive and it’s not easy to go out and spend $800 on you know, a device like this. And I feel like it’s really helped her, so I wish they were more easily accessible.
Experiences Using an AAC Device
The third category related to families’ experiences using AAC and supporting their child’s communication. This involved three themes that built on one another in a cyclical way: (a) learning and navigating challenges, (b) supporting their child’s communication at home and in the community, and (c) seeing progress.
Learning/Navigating Challenges: “It’s Both Empowering . . . [and] Very Overwhelming” (Lilian)
Mothers described various challenges associated with using AAC. Some talked about technical challenges, such as not knowing how to operate the device or troubleshoot problems (Lilian). Amira and Amber both talked about feeling frustrated when their child’s device broke on different occasions, particularly because it took a long time to get repairs or a replacement device. A few mothers explained they did not know what to do when their child explored or stimmed with the device. Florence shared: We’ll get it out and we'll get off track from what we were trying to figure out—what she wanted. And suddenly, she's pushing just random buttons. And I think that's where I lack the expertise in keeping her focused on telling us what she wants.
Many challenges related to inconsistency in how the SGD was used at school or therapy services, as compared with home. Some mothers explained their children used the device more at school than at home. Lauren shared that her daughter “doesn’t really listen to us as well as she does the teachers, so it’s been a little bit more difficult to get her to actually use [the device at home].” Others were frustrated that their child’s providers did not use the device at all. Jackie expressed: All I'm saying is encourage him to take his talker to centers, please. Encourage him to bring his talker with him to the circle. ‘Cause they're like, ‘Oh, well it’s on his desk. He goes and gets it if he wants something to say.’ I’m like, “Do you leave your tongue on your desk?” I mean I really don’t know how to answer this. You know, “Do you have to go walk across the room to get something to talk or to have people understand you?”
Therefore, every mother emphasized communication and collaboration with their child’s teachers and service providers. Shelly had positive experiences: I speak to all her teachers and therapists at least once a month and we communicate if there’s an issue. Her teacher I speak to her every day. I’m pretty involved, asking them, “What can we do at home with her?” And practice this. And she’ll let me know what’s on her IEP, and what she’s working on, and I’ll try it sometimes on the weekends.
Other mothers described limited communication and collaboration. For Lilian, gaps in communication made her feel uncertain about how to use the device at home and made her feel stuck as an intermediary between individual service providers.
In terms of like a cohesive plan, we’re not really doing that. I pretty much have to be the go-between between both of those sides and that gets very difficult. . . . I would really love a better game plan of like what I can be doing better at home. And, like, I would love to be able to figure out how we can all be kind of working on the same kind of stuff to help her, but it just kind of seems like that’s been a big struggle . . . it is a lot of people and a lot of different, you know, puzzle pieces that aren’t quite coming together.
Mothers typically described limited support from providers related to AAC, and most of the support they did have focused on the technical and operational aspects of the device, rather than on how to integrate it into their day-to-day lives and interactions. Cindy felt the training she received was “really fast.” Because they did not get a lot of support, mothers described relying on “the instinct of being a mom” (Amira) or trying to pick up strategies while observing SLPs or other therapists. According to Lucy: I guess I just see what his therapists do with him and try to emulate it. You know, to a degree, I don’t want to do all the work that they're doing, but I do want to be accessible to him. . . . Yeah, I think I've just been to a lot of therapy sessions.
Several mothers worked in related professions (e.g., general or special education, physical therapy) and described relying on that background knowledge. Jane described her “special set of skills” as a special education director.
Well, we were never given any training. Again, like, I have more knowledge in this area than the average bear, so like I could figure it out. I can program a device. I have enough skill that I know how to do it. But, we were not given any training on it.
Still, even mothers with background knowledge shared it was difficult to integrate the device into daily routines. “I am a preschool special education teacher and have been for twenty years. It was very overwhelming. I wan’t quite sure what we were supposed to do with it,” shared Ynez. Ultimately, Lilian and other mothers wanted more support: I just feel like being more able to access, you know, quality training would be good, especially for a parent. Because I can read books on like speech language and stuff that aren't written for a parent. But there's not a lot of things that are just written for parents and like if you don't have a background in these kinds of areas. But if I had more coaching like from the people that work with Hannah in terms of like what I can be doing, that would be helpful.
Supporting Communication: “We Try Our Best at Home” (Cindy)
Parents primarily talked about how their child’s communication was related to two key aspects of their life together as a family—their child’s behavior and their connectedness as a family. Therefore, these values influenced parents’ attempts to use the device at home. Lilian and Lucy tried to use the device to engage and build a connection with their child, such as by using the device for exploring and discovering what their child knows (e.g., “testing” the child on their knowledge of food or colors). Other parents worked to reduce their child’s frustration by attempting to use the device for their child to clarify their communication attempts. Shelly explained, “That’s when I would encourage her to use the device—if she doesn’t know exactly how to say it, or we’re not understanding.” Mothers also emphasized using multiple means of communication to clarify meaning, such as pointing or signing in addition to the device. Participants tried to use the device in different routines and activities at home, ranging from “potty training” and “playing games” (Amber) to “academic work” (Jane). Claire also described taking the device to places in the community such as church or the grocery store to teach her son how to “apply it in different situations.” Similarly, Jackie talked about downloading the communication app on other family devices besides her child’s main SGD saying, “We try really hard that he takes it everywhere.”
Participants explained that although they tried their best to use the device at home, they often questioned what to do or if they were doing things right. AAC felt “not natural” (Cindy). Despite trying to use the device with her child, Amira described being “not so lucky,” meaning that she felt the use of the device was not going as well as she had hoped. Similarly, Florence talked about doubts that came when she compared her situation to that of others, saying “I know somebody who has it [the AAC device], and her daughter has Down syndrome, same age, and she’s great on it. And, you know, I keep thinking, what are we doing wrong?”
Seeing Progress: “I Think Things Are Getting Better” (Amira)
Despite the challenges, mothers thought AAC had made a positive impact on their child’s communication, language, and social engagement. Ynez felt her son had become a more “active participant” in social interactions with peers. Claire mentioned that her son “seems to want to engage more socially” with her and his other family members. Lucy was so proud that her son could tell her “things that he wouldn’t be able to say with his voice.” Savannah commented: I am absolutely convinced there is no way he would be saying what he’s saying or trying to say what he’s saying if he did not have the device. Like articles of speech, like verb tenses that he’s just aware of now. There is just no way he would have been at that point to like be trying to say those things. It just made him aware like language-wise of so many things. And, obviously, his participation in the classroom. I mean it’s just like changed his life.
Many mothers also discussed how their child’s challenging behavior and frustration had reduced since having a way to communicate effectively. Amber shared, “I went from having a child banging his head against the wall because he couldn’t communicate, to the child that is able to tell me and point to what he wants.” Amira expressed similar feelings: Last year I was kind of a little bit scared of him because he still had that tantrum. But, the beginning of this year toward the end of last year, it’s been changed. It’s changed drastically. So yeah, it’s improved. And I think that’s [the AAC device] the reason.
A few mothers talked about improvements in communication leading to “self-determination” (Jackie) and happiness. Lucy explained: I think it has definitely given him a real feeling of agency with being able to express himself. It’s so obvious, he is just delighted with it. And so that makes me happy. And to see David feel confident and happy and excited about something makes me feel really good.
Seeing progress also helped change mothers’ perceptions of AAC to be more positive, especially when mothers were hesitant or fearful of initiating it in the first place. Stacy reflected: It’s made a huge difference. And honestly, I was afraid of it because I really wanted Ryan to be able to speak, like to verbalize language. So, I was like no he’s gonna rely on that. He’s going to not try to talk. But, it’s been the total opposite. If anything, I think that the device has encouraged his verbal language because he now understands the power of words and of being able to request. And he’s now engaging way more. I don’t think he would have done that otherwise.
Although most mothers talked about seeing progress with their children, they still varied in whether or not they felt satisfied. Some battled discouragement because progress felt slow. Lilian talked about “managing her expectations,” especially when she was tempted to compare her daughter to other children of a similar age and disability. Florence explained: Somedays you think, “Oh this is going great.” And then somedays you think, “Oh we have so far to go.” . . . So, we move forward with knowing what we know and hoping it’s for the best, and you know adjust ourselves later on if we need to. And I think I always kind of approach it as a continuing process . . . we’re always going to be working on this [communication] with her. And so, it doesn’t have to all be right now. It’s a process.
As Florence described this “continuing process,” it became apparent that her positive perspective fueled her to keep with the journey—to continue learning and navigating challenges, and to continue working each day to support her child’s communication. Patterns like this played out across families. Too much frustration or worry made it more challenging for mothers to tackle the next challenge or learning demand, impacting how they were able to support their child each day. On the contrary, mothers felt reinforced and strengthened when they could see their children progressing and learning, and this bolstered their confidence—not only in their child but also themselves, helping them to rise to meet the next challenge.
Surrounding Factors
The fourth and final category related to factors surrounding families’ experiences, which involved the themes of (a) family structure, informal supports, and demands; (b) access to services and professional supports; and (c) the COVID-19 pandemic.
Family Structure, Informal Supports, and Demands: “The Reality of Our Day-to-Day Life” (Jane)
Many of the factors surrounding families’ experiences with AAC are related to their day-to-day lives—including their family structure, demands on their time and energy, and access to resources and social support. Several mothers felt well-supported, but others felt the bulk of the responsibility fell on their shoulders. Cindy explained feeling “like I do everything in my kids’ lives.” As a single mother, Amber described the challenges of navigating services and balancing work and family life: Being a full-time employee, you know, it’s hard to do with a kid with autism because you don’t have a lot of time to spend with them. So, going part time probably was the best thing for me, because now I’m able to have more quality time with him versus it just being the weekend. . . . I wish companies were more lenient to a parent that has a child with a disability, and more understanding. Because working full time you don’t have a lot of time with your child.
In general, most mothers felt overwhelmed trying to balance responsibilities. And, they felt they did not get to spend as much time focusing on their child’s communication as they would like. Lucy explained: “I am just too busy trying to get through the day and David’s basic needs of getting fed and clothed and, you know, having healthy bowel movements and getting to school.” Similarly, Lauren described: “We’ve got three kids. They all do activities. They’re all in different schools. My husband works 40 hours a week; we’re both working from home. I’m working like 20 hours a week and then 10 hours with volunteer.”
Financial resources and difficulties also impacted families’ experiences. When it came to training opportunities, Jackie sought them out but was limited by cost. She explained, “I go to whatever I can get into without having to pay for conferences.” Claire talked about finances too: I was really thankful that somebody told me, even though my husband does work, if you have a special needs child, they can still qualify for [state insurance] because I didn’t know that in the beginning. We were paying for all of this out of pocket, and I didn’t know. And we were tanking really fast. And I mean we’re still paying off debts from that time and I just didn’t know. But, thankfully, we were educated and we applied. We learned that because he has enough special needs, he does qualify, so we still pay co pays and they add up very, very quickly, when you receive all of these services.
Finally, social support also played important roles in families’ experiences. Many mothers talked about receiving help from extended family members who were “wonderful and supportive” (Florence) and “helpful” (Stacy), but not every family had that type of support. Other mothers described feeling supported by being able to connect with other parents through social media (e.g., Facebook groups) to “to learn more and have more ideas” (Amira). Mothers also shared wanting support through in-person groups. For instance, Amber explained: It would be good to have like a bigger network. Or like, parents that could bring their kid with them and have, you know, a sitter on hand where we could do monthly meetings. Or you know, sit down and discuss what was going on with our child, and just kind of vent.
Access to Services and Professional Supports: “We Just Got Lucky” (Shelly)
Other factors surrounding families’ experiences related to the nature of services and supports they were able to access for themselves and their children. Several mothers talked about the inequities they saw related to accessing quality services and professionals. When they felt happy with their child’s services, they often credited it to “luck.” Ynez explained: We have been very lucky. I tell people—anyone who will listen—that our early intervention team, we sort of had a dream team. And so I had a lot of support along the way. . . . We’ve been very fortunate in that in that way.
Some mothers credited their “luck” to the fact that they had knowledge and experiences to draw from because they worked in related professions. Jane shared: I have a special set of skills where like if I need something, I know where to find it or I know who to ask. So, I can’t think of something in particular that I wouldn’t know how to get if I needed it
Mothers described having to advocate to navigate long wait lists to enroll their child in schools they preferred (Amira, Shelly), get a diagnosis (Cindy, Amber), get access to applied behavior analysis (ABA) therapy (Amira, Cindy, Amber), and get access to other private therapy services (Lilian). Cindy explained that her child was chosen from a waitlist for ABA therapy “only because I have been on their case every week when this is happening.” Amira described feeling “shocked” that one of her children got off the waitlist for a magnet school.
In addition, mothers described access to and the quality of services being related to the nature of their child’s diagnosis and support needs. Florence acknowledged: So, Faye’s diagnosis is Down syndrome and so it’s very straight forward and black and white. And we’ve never really had trouble getting services because it’s always kind of assumed that she’s going to be behind in various things.
On the contrary, mothers like Lilian, Claire, Ynez, and Cindy talked about it being difficult to find service providers who worked well with their child. Cindy described the challenges: Keith is a complex kiddo. I think many providers are afraid to treat him because of his dual diagnosis and not being familiar with his communication program. . . . One of his first speech therapists did not want him to use a communication device. She stated it will limit his progress with speaking. . . . Another therapist said she did not feel comfortable treating Keith with the increased level of support he needs. . . . It’s so challenging and hurtful when a medical professional is quick to judge someone, especially since I’m in a similar field. I feel like some of these therapists cannot relate to the challenges families who have a child with such complex needs face on a daily basis. It’s hard on our family.
COVID-19 Pandemic: “We Made It Work for the Circumstance We Were in” (Shelly)
Mothers discussed the positive and negative impacts of the COVID-19 pandemic. Most had gone through the process of acquiring an AAC device either amid the pandemic or in the time just before the start of the pandemic, which tended to cause delays. Many mothers talked about challenges with virtual learning. Shelly shared: It was tough because I had to put her in a baby chair for her to pay attention, for her to focus. And she’s like, ‘I don’t understand, I don’t understand. My teacher’s in the computer and like this is how we're learning?’ It's very confusing for an adult, so could you imagine a kid on the spectrum? Like it’s a huge change, so it was a huge transition for us.
Lauren explained, “It was just all frustration. It was tears. She wasn’t paying attention. She wouldn’t sit down. She would cry.” She went on to discuss the residual stress this caused for her and her family saying, “We got frustrated to the point where I was crying. I didn’t want to do it. I wasn’t looking forward to it.” Savannah shared that she “essentially quit [her] job” to support her children at home during the pandemic.
At the same time, several mothers described unexpected positive impacts from the pandemic. Ynez saw more progress in her son’s language and play during the pandemic: “And it was because we were home, you know? . . . It was what it was. And so, we made the best of it.” For some parents, teletherapy provided a new opportunity to learn from service providers. Amber explained that her son’s speech therapist “became more of [her] coach” after they switched to virtual therapy. Florence also described feeling grateful to have a closer partnership with her child’s service provider.
I think access to the therapist that you don’t when you just, you know, have a parent teacher conference a couple times a year, or maybe you know a meeting here and there, or whatever. Being able to see the session going on, and in a lot of cases being responsible really for delivering the physical aspects of it on my end, it was invaluable really. I mean, it was something that we wouldn’t have had except for COVID, and probably won’t have again.
Discussion
Young children benefit from AAC intervention, but many barriers stand in the way of children getting early and high-quality communication support (Drager et al., 2010; Light et al., 2019). Improving service delivery requires gaining a strong understanding of families’ views and experiences. We wanted to gain insight related to the experiences of families that could inform potential practice and policy changes, so we interviewed 14 mothers of young children about their lived experiences. We identified many factors that for some families acted as facilitators for getting AAC access, but that created challenges for others—funding, perceptions and knowledge of professionals, and whether they had an “AAC finder” to help on the journey. After they had acquired a device for their child, mothers often felt overwhelmed with learning to use it; yet, at the same time, they conveyed an unwavering motivation to support their child at home. These findings extend prior research and have implications for practice in several key ways.
We would assert that one of the most important findings relates to seeing the strength and resilience that mothers demonstrated. Mothers showed their dedication in different ways, based on things like their personality, family structure, and competing demands. For instance, Amira’s determination to support her son took shape in her persistent efforts to seek out quality educational and therapeutic services. Her attitude to “just keep going and not give up” allowed her to bounce back even in the face of great challenges. Jackie, Lilian, and Amber described their roles as advocates. Other mothers, like Stacy and Lucy, showed a deep desire to learn from their child’s teachers and service providers. In all of these cases, mothers showed great commitment to supporting their children, which was clearly evident in the way they navigated challenges. Yet, it is also important to notice that most mothers still felt overwhelmed about aspects of supporting their child’s AAC use and communication development, and they wanted to find a balance where they could feel like a parent and not a “therapist.”
It is essential that service providers and educators recognize the different strengths, needs, and preferences of families having children with CCN. Family-centeredness means that providers recognize the strengths and capabilities of families and then build on these strengths (Dunst & Espe-Sherwindt, 2016; Epley et al., 2010). Yet, AAC services are often not family-centered. Mandak and Light (2018b) conducted online focus groups with speech-language pathologists serving children with CCN and found they felt dissatisfied with the family-centeredness of their own services. In a companion study, parents themselves rated family-centered services as occurring even less frequently than professionals (Mandak & Light, 2018a). One of the foundational challenges for truly family-centered practices might be that providers fail to see the strengths and capabilities of families when they manifest in different ways—particularly considering that more than one-third of early-intervention SLPs cited “parent buy-in” as being the greatest barrier to effective AAC intervention (Lorang et al., 2022). The goal of family-centered AAC services should be to understand each family’s unique dynamics and then use this to tailor services, minimizing disruption to the family while maximizing outcomes for children, parents, and whole family units (Coburn et al., 2021; Mandak et al., 2017). According to Bailey et al. (2006), “the real test is whether a program promotes positive outcomes for families” (p. 228). In conjunction with the broader literature, findings from this current study suggest that AAC services within early intervention and early childhood special education might be falling short of these goals for many families.
Second, mothers’ experiences getting their children access to an SGD varied fairly widely. Some described the process as “relatively easy,” but others had to navigate significant barriers (e.g., negative perceptions or limited expertise of professionals, difficulty with access to funding, feelings of loss or worry associated with getting an AAC device for their child). Similarly, Biggs and Hacker (2021) found that parents, educators, and service providers all identified many determinants of AAC access that spanned across ecological systems, including factors related to (a) the child, (b) school, home, and community microsystems, and (c) and broader factors (e.g., school policies, the support networks of service providers and educators, societal and cultural influences). As shown by the stories of the mothers who participated in this study, having an “AAC finder” is important—whether that person is an early interventionist, speech-language pathologist, AAC consultant, or family member. Without an “AAC finder,” parents of children with CCN may not otherwise know that AAC supports exist or could benefit their child (Binger et al., 2012).
In addition, a question remains of who actually has AAC access, and who does not. This question was only further emphasized in our minds when we—despite our attempts to recruit a diverse sample—still recruited primarily White mothers from professional backgrounds. We attempted to involve families from diverse racial and socio-economic backgrounds by recruiting through broader community resources (e.g., pediatric clinics and faith communities) that might serve a more diverse group of families than disability-related organizations alone. We also directly targeted recruitment within neighborhood communities within larger cities that had larger populations of families from underrepresented groups. However, despite these efforts, our sample did not represent the breadth of the population within the three selected states. Our recruitment challenges should be considered in light of a broader context, which demonstrates there are clear racial, ethnic, and socio-economic disparities with regard to which families and children have access to the best early assessment, diagnosis, and services—including but not limited to disparities in AAC services (Pope et al., 2022; Singh & Bunyak, 2019). Therefore, it is critical that the field seeks not only to identify but also to mitigate the barriers that children and families from marginalized backgrounds experience related to communication access. This will require attention to many complex and multifaceted factors, across multiple systemic levels—including addressing barriers in practice and to participation and representation in research.
A final key finding was that families’ experiences tended to follow a cyclical pattern: that is, parents had to navigate challenges and learn about AAC; they worked to support their child’s communication at home with the device; and this impacted the type of progress they saw, which then influenced their confidence and motivation to tackle new challenges. A cycle like this produces cumulative advantage/disadvantage—in other words, “the rich get richer; the poor get poorer” (Dannefer, 2003). In the present study, families who had access to greater resources (e.g., stronger support from professionals or their informal support networks) generally felt more confident about supporting their child’s communication at home, and then they described seeing more progress. The opposite is also certainly true: Families who lack training and resources may become increasingly frustrated and discouraged by the lack of progress, ultimately leading to the abandonment of the AAC device. For example, in Moorcroft et al. (2020), parents who had abandoned AAC devices explained that they did so because they received inadequate support from service providers and lacked support from others in their social networks (e.g., teachers, medical providers, family, and other community members).
Limitations and Future Directions
The findings from this study are contextualized within a relatively small sample and should not be assumed to generalize to all families with young children learning how to use an SGD. In addition, despite efforts to recruit participants from diverse and underrepresented backgrounds, the sample overrepresents White, English-speaking families from middle and upper socio-economic backgrounds. Participating parents also included only mothers (no fathers or other caregivers), and the sample did not include any families from rural communities, despite our attempts to recruit from these communities. Another limitation is that data were collected through just one interview, providing a retrospective snapshot of families’ experiences. Future studies could include designs that capture families’ experiences across time and through different methods of data collection (e.g., interviews, observations, focus groups, and surveys). Considering these limitations, future research should focus on the perspectives of individuals not represented or underrepresented in this study—including fathers; families from rural areas; families from underrepresented racial, ethnic, and socio-economic backgrounds; and families with diverse structures.
Implications for Practice and Policy
Service providers such as early interventionists, teachers, and SLPs play key roles in supporting young children with CCN. These professionals can make a difference for children and their families by successfully facilitating AAC access for children who would benefit from it. But, they can also create barriers if they have insufficient knowledge or unfavorable perceptions of AAC. It is also important to recognize that the “AAC finder” role (Binger et al., 2012) does not belong only to these providers. For example, pediatricians can also play a significant role by recognizing children who could benefit from AAC during well-child visits and then facilitating parents’ connections to other providers with AAC expertise. Even more, the important roles of professionals continue after a family has accessed AAC for their child. Parents in this study were clear that they wanted to learn more than simply how to operate the device—they wanted to know how to use the device in everyday routines. Doing this will require that AAC services become individualized and family-centered, ensuring that intervention is meaningful and practical for families and that it maximizes positive outcomes for families, including by building on natural routines and families’ strengths and preferences (Coburn et al., 2021; Mandak et al., 2017). With this, it is important that providers see parents as equal but distinct partners, seeing the parenting role as being different than “being a therapist” while valuing and treating parents as experts on their child.
Training programs (e.g., university programs, mentorships, and fellowships) have an equally important role given their responsibility to equip the professionals who work with children with CCN. High-quality AAC-related training and field experience are vital components of pre-professional and continuing education programs to dispel myths about and build capacity for effective AAC use with young children. Moreover, this training is necessary for a broad range of professionals, including but not limited to early interventionists, general and special education teachers, paraeducators, SLPs, and other service providers such as occupational therapists and medical personnel. Professional education must also focus on equipping providers to partner with families to carry out quality family-centered practice.
Finally, policymakers and leaders have the power to implement policies that could provide better support to families and their young children who use or could benefit from using AAC. There is a critical need to address the issues that are causing barriers to AAC access for young children, including policies at the school, district, state, and federal levels, and perhaps most notably related to insurance billing. Families’ stories from this study suggest that the families whose children are able to access AAC when they are young appear to be those who have greater access to resources and connections. These disparities must be attended to in policy changes to ensure more equitable access to AAC intervention and support for all families and their children.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.