
Abstract
There is a national shortage of early intervention (EI) providers for young children with disabilities or developmental delays. This needs assessment study employed in-depth semi-structured interviews to explore the perspectives of EI program directors (N = 27) across a large U.S. state on provider retention efforts. Through a qualitative analysis, we identified 12 themes across four overarching categories—(a) compensation and financial incentives, (b) program management and organization, (c) positive climate and culture, and (d) training and mentoring. We discuss implications and suggestions for future research.
The Individuals with Disabilities Education Act (IDEA) Part C emphasizes early intervention (EI) services for young children with disabilities or developmental delays that are (a) family-centered, (b) held in natural and inclusive environments, and (c) collaborative and team-driven (Bruder, 2010). In addition to the family, this collaborative, multidisciplinary team can consist of a variety of providers, including service coordinators, developmental/EI specialists (EISs), speech language therapists (SLTs), occupational therapists (OTs), and physical therapists (PTs). Per the 43rd Annual Report to Congress, approximately 427,234 infants and toddlers received EI services (U. S. Department of Education, 2022). However, nearly all U.S. states and jurisdictions (n = 42) report shortages of EI providers (Council for Exceptional Children, 2020). In a survey conducted by Vail et al. (2018), state EI coordinators were most likely to report shortages of SLTs, PTs, and OTs. These persistent shortages threaten the scope and quality of team-driven services that can be provided to young children and their families, especially those living in high poverty or rural communities (Billingsley et al., 2020; Decker et al., 2021; Fall & Billingsley, 2011; Haring & Lovett, 2017; Kasprzak et al., 2012; Mason-Williams et al., 2020; Palsha et al., 1990).
Factors Influencing Early Intervention Provider Shortages
A variety of factors influence shortages of EI providers. In the field of special education, research has identified the following contributors to teacher attrition—poor working conditions, inadequate compensation, lack of support from colleagues and administrators, poor pre-service and in-service training, and insufficient state and federal funding for educator preparation and development (Billingsley et al., 2020; Billingsley & Bettini, 2019; DeMik, 2008; Mason-Williams et al., 2020; Peyton et al., 2021). Specific to EI, research supports similar factors impacting provider retention—(a) stressful working conditions (e.g., EISs taking on too many responsibilities or home visits requiring long distance travel), (b) insufficient compensation and funding (e.g., therapists leaving for higher paying hospital or clinic positions and EISs leaving for school positions), and (c) pre-service training with limited emphasis on EI (Bruder & Dunst, 2005; Haring & Lovett, 2017; Kasprzak et al., 2012; Vail et al., 2018).
Efforts to Recruit and Retain Early Intervention Providers
Multiple national organizations seek to combat shortages by providing a wide range of supports to recruit and retain EI providers. For example, the Office of Special Education Programs (OSEP) provides funding and resources for attracting, preparing, and retaining high quality special educators and EI providers (U. S. Department of Education, 2020). Specific to retention, OSEP offers research-based briefs in five areas—(a) enhancing professional leadership, (b) induction and mentorship, (c) ongoing professional learning, (d) professional empowerment, and (e) supportive workplace environments. Some specific strategies supported by research include the implementation of Grow Your Own programs (Zascavage et al., 2008), workshops to reduce burnout (Biglan et al., 2013), and additional pathways to promotion (Podolsky et al., 2016). However, most research cited in these briefs address retention for special educators working in public school settings.
Two federally funded centers, the Early Childhood Personnel Center (ECPC, 2020) and the Early Childhood Technical Assistance (ECTA, 2022) Center, provide guidance for states to address EI provider shortages. ECPC offers the Comprehensive System for Personnel Development (CSPD) to address recruitment and retention, among other areas (i.e., professional and leadership standards, pre-service training, in-service training, leadership, coordination, and sustainability, evaluation). In addition, ECTA provides guidance in the form of quality indicators for implementing recruitment and retention strategies that are (a) rooted in data, (b) revised when needed, (c) discipline-specific, and (d) comprehensive (e.g., address collaboration with colleges, induction and mentoring, and incentives and recognition). Specifically targeting EI providers, some strategies supported by research include high quality professional development (e.g., Dunst, 2015), peer coaching (e.g., Romano et al., 2021), and reflective supervision (e.g., Frosch et al., 2018). However, there is little research on the impact of these strategies on retention.
Research on Retention in Related Fields
Research in related fields (e.g., special education, child welfare, social work) may provide insight into the factors that contribute to EI provider retention. In special education, research has explored teacher decisions to stay in the field, identifying the importance of (a) internal factors (e.g., desire to advocate for students with disabilities), (b) support from administrators, (c) a sense of collegiality with colleagues, (d) having strong mentors, (e) job flexibility (e.g., being able to switch schools or classrooms when desired), (f) schedule factors (e.g., having breaks and summers off), and (g) opportunities for professional development (Berry et al., 2011; Lesh, 2017; Lopez-Estrada & Koyama, 2010; Prather-Jones, 2011). In the fields of child welfare and social work, research has explored the decisions of case managers to stay in the field, identifying factors related to (a) clear expectations during the hiring process, (b) induction and mentoring programs, (c) supportive organizations, colleagues, and families, and (d) opportunities for professional growth (Johnco et al., 2014; Webb & Carpenter, 2012).
Rationale for the Study
Little research has explored the perspectives of key stakeholders (e.g., program directors, state Part C coordinators, providers, families) on important factors associated with the retention of EI providers and implications for population level health outcomes (U.S. Department of Health and Human Services, 2022). A few studies have explored stakeholder perspectives on the adequacy of professional development systems (Bruder et al., 2009), the need for partnerships and emotional support for providers (Brotherson et al., 2010), and the implementation of best practices (Decker et al., 2021). However, no published studies have explored the perspectives of EI program directors on their efforts to retain providers. Given that these individuals are often charged with leading program-wide initiatives to recruit, hire, induct, train, and supervise EI providers in various community settings including underserved communities, their perspectives may provide insights into the appropriateness of specific retention efforts. In addition, these perspectives may also inform state and federal policymakers and the future research necessary to identify evidence-based retention strategies specific to the EI field. Thus, we posed the following research question: What are the perspectives of EI program directors across a large state on efforts (e.g., strategies, initiatives, collaborations) to increase the retention of EI providers across various disciplines (e.g., EISs, SLTs, OTs, PTs)?
Method
To gather EI program director perspectives on provider retention for this exploratory study, we employed a general qualitative research methodology (Merriam, 2009). We interviewed EI program directors across a large U.S. state as part of a larger OSEP funded statewide needs assessment and professional development project. In addition to studying retention efforts, our aim was to design a training and implement strategies that were responsive to the diverse assets and needs of EI programs in the state. Through a qualitative interview approach, we were able to capture the nuanced perspectives of key stakeholders and seek to better understand the complex and stressful aspects of staff retention and attrition. Approval from the Institutional Review Board (IRB) from the host university was obtained (Protocol 1759888).
Participants
We recruited the program directors from all 41 contracted EI programs from the state. We advertised the research with support from statewide Part C coordinators at the Health and Human Services Commission. First, we sent an initial email invitation to potential participants detailing the aim of the study. Then, for individuals who did not respond, we sent a follow-up email and/or phone call. In total, 27 program directors agreed to participate, which accounted for about two-thirds (65.9%) of EI programs from the state. Participants were 85% (n = 23) female and 15% male (n = 4), and their experience as a program directors ranged from 1 year to over 20 years. To ensure we had a representative sample, we gathered program data related to program size (i.e., number of children that programs were contracted to serve), geographic region, community type (i.e., urban, rural, combination), organization type (i.e., community center, private non-profit, school district, regional service center), and historic turnover rates, which state Part C coordinators provided. Our sample included participants from all geographic regions in the state and was representative of the statewide make-up of program sizes (i.e., small, medium, large), community types, organization types, and historic turnover levels (i.e., high, moderate, low). Table 1 details the complete program information for participating directors.
Participant Program Information.
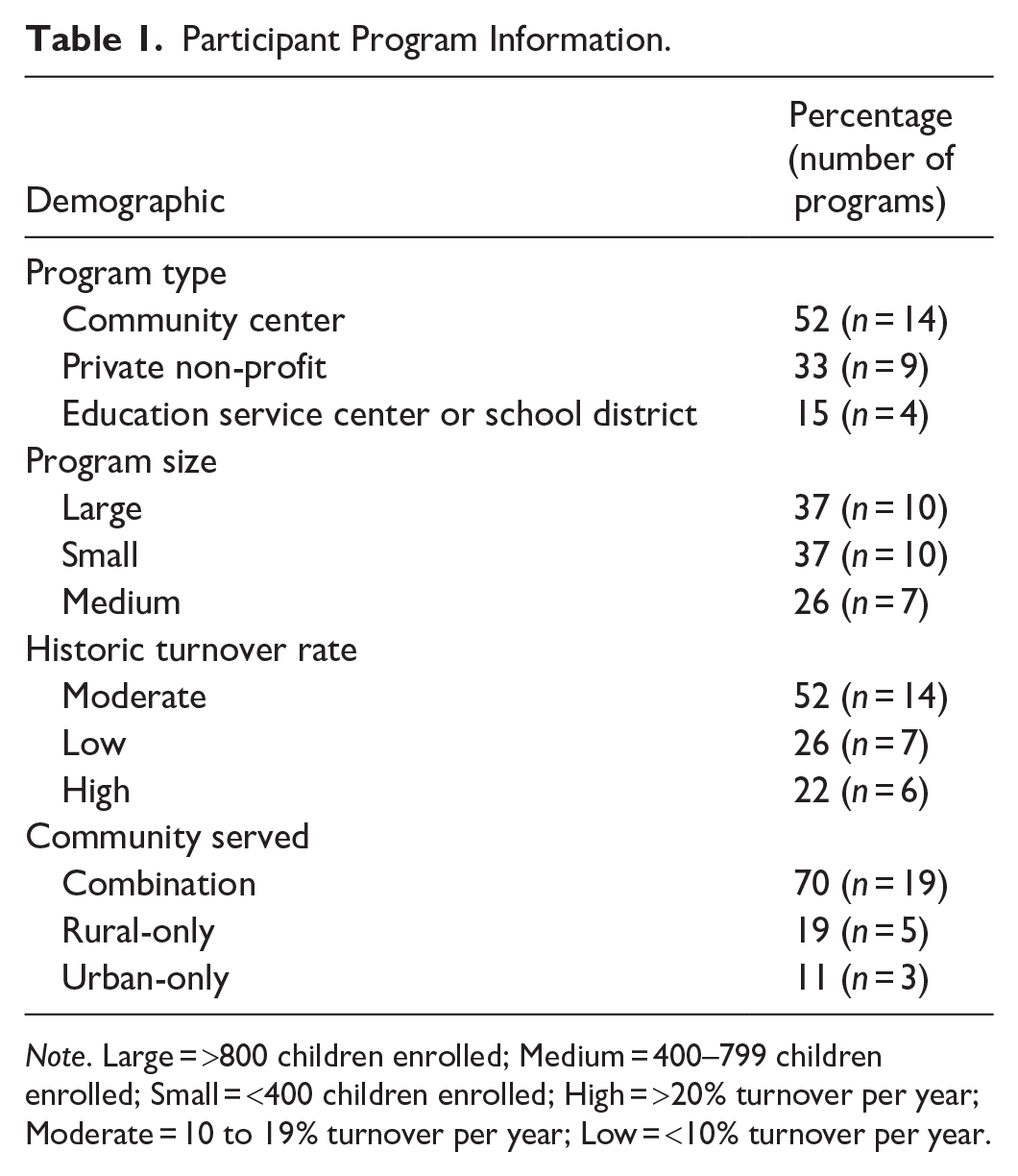
Note. Large = >800 children enrolled; Medium = 400–799 children enrolled; Small = <400 children enrolled; High = >20% turnover per year; Moderate = 10 to 19% turnover per year; Low = <10% turnover per year.
Data Collection
To gather participant perspectives, we conducted approximately 60-minute in-depth semi-structured interviews on a video conference platform (i.e., Zoom). Two university faculty members with special education backgrounds and two graduate students with health science backgrounds conducted the interviews, with one faculty member and one graduate student participating in each. Prior to interviews, we sent participants the questions to review. We asked that participants review program records and debrief with staff to prepare for the interview. During interviews, most participants conferred with their notes and mentioned this preparation work. To start the interviews, we introduced ourselves and engaged in brief rapport-building (i.e., small talk). Then, we reviewed informed consent procedures and asked if participants had any questions about the study (or future project-related activities). Next, we engaged participants in the semi-structured interview. We posed each guiding question as written. Then, for each question, we asked follow-up and clarifying questions, sometimes engaging in unstructured conversation. After conducting multiple interviews, we also began asking questions related to similarities and differences in participant responses across programs. Table 2 lists our six guiding questions, which included an introductory probe, general probes about retention, and targeted probes about retaining staff in different disciplines and with different levels of experience. We audio recorded all interviews and transcribed them verbatim, removing potential personal or program identifiable information (e.g., names, counties, cities, colleges). The first author reviewed the graduate student-generated transcriptions to confirm their accuracy and the removal of all identifiable information.
Semi-Structured Interview Questions.
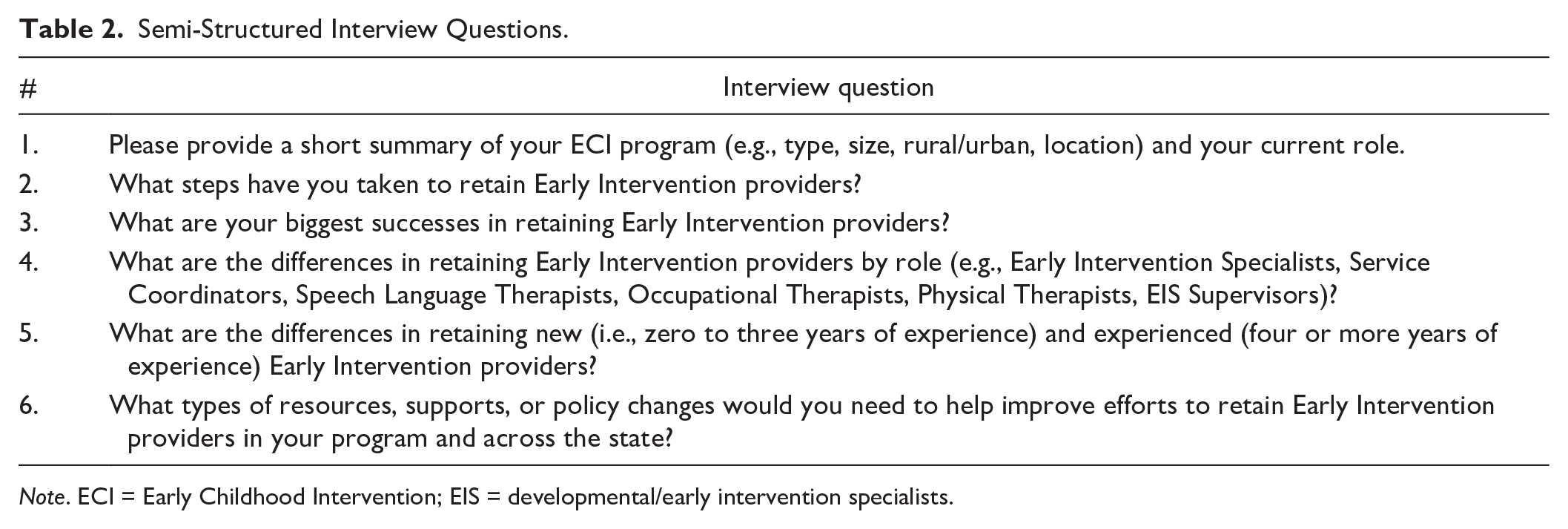
Note. ECI = Early Childhood Intervention; EIS = developmental/early intervention specialists.
Data Analysis
We conducted a collaborative qualitative analysis in Dedoose, an online coding software, following steps for thematic analysis recommended by Braun and Clarke (2006). For the first stage of the thematic analysis, the data analysis team, consisting of the four researchers involved in conducting the interviews and another faculty member with a health science background, reviewed the data and developed initial codes. To start, the lead author read through all transcripts to review general trends and develop a preliminary list of initial codes (e.g., promotion, raise, pay). Then, the whole team met to discuss the initial codes and review a transcript together to practice applying codes to individual excerpts. We then practiced applying initial codes to a transcript individually to further reflect on the adequacy of initial codes and clarify inclusion and exclusion criteria. After meeting to confirm initial codes, we divided transcripts amongst the five researchers (i.e., five or six each) to apply initial codes. We met frequently during this process to review unclear excerpts and revise initial codes. This process concluded with a list of 22 initial codes (e.g., we decided to merge promotion and raise since these were often coupled but we kept pay as a separate code for base-salary or hourly-pay).
For the second stage of the thematic analysis, we identified and solidified themes. The whole team met to review patterns among the initial codes and identify initial categories and themes. Initially, we identified five categories related to financial incentives, climate and culture, recruitment, training, and mentoring. Then, we organized all excerpts by category to identify themes. During this step, the lead author and two graduate assistants reread all excerpts and confirmed that they fit both the appropriate initial code and category to enhance researcher reliability, meeting frequently to come to consensus on coding decisions (Trainor & Graue, 2014). In clarifying and naming themes, the whole team met to discuss common ideas, key quotations, and overlaps between categories and initial codes. Together, we developed an initial report of findings.
After identifying themes, we engaged in a comprehensive member checking process. We shared our initial report and solicited feedback from an advisory workgroup, consisting of state Part C coordinators, consultants from other universities, EI program directors and providers, parents of children receiving EI services, and individuals with disabilities. In addition, we hosted a statewide summit on retention and reported initial themes to EI program directors (e.g., study participants and non-study participants) and other program leaders (e.g., supervisors, trainers, leads). Summit participants had an opportunity to engage in panel discussions, ask questions about study findings, and provide feedback in an informal survey, consisting of Likert scale rating items and open response items. Nearly all survey responders (n = 50) indicated that they were satisfied or very satisfied with the initial categories identified by the research. One said, “There was a lot of research that was presented to back up the information being shared. The panels and questions to the panels were extremely helpful in providing different perspectives and ideas.” After the summit, the research team reflected on feedback to revise initial findings and finalize the identification and naming of 12 themes and 4 categories.
Findings
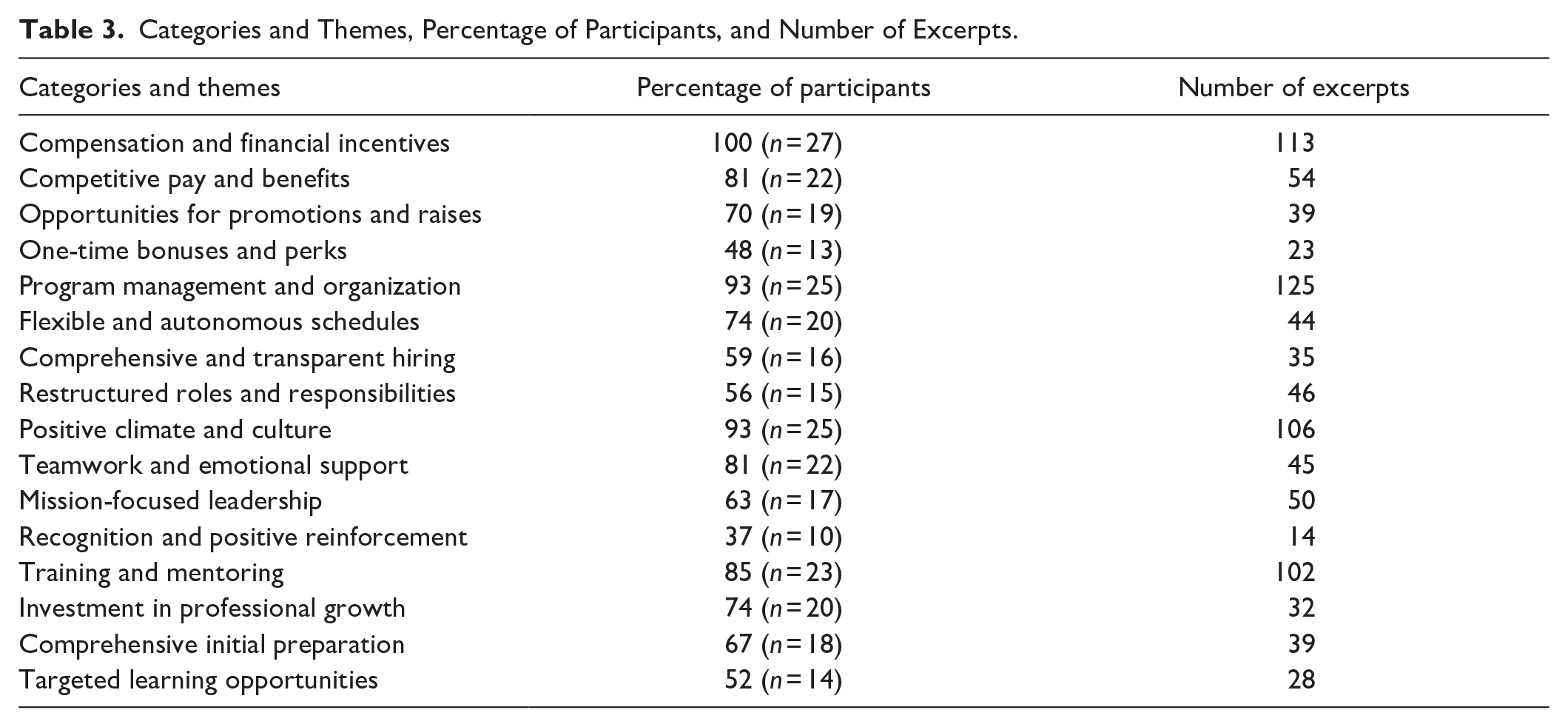
In semi-structured interviews, we asked 27 EI program directors across a large U.S. state to discuss their efforts to retain providers. Our collaborative qualitative analysis of transcripts resulted in 12 emergent themes across four overarching categories: (a) compensation and financial incentives, (b) program management and organization, (c) climate and culture, and (d) training and mentoring. Table 3 lists the categories of themes along with the percentage of participants and number of excerpts associated with each.
Categories and Themes, Percentage of Participants, and Number of Excerpts.
Compensation and Financial Incentives
All participating program directors discussed efforts to retain EI providers via compensation and financial incentives (e.g., hourly pay, salary, benefits, promotions, raises, bonuses). We describe the three main compensation and financial incentive-related retention efforts in the sections below.
Competitive pay and benefits: “Get our average salary comparable.”
The effort discussed by the most participants (n = 22) involved working to offer competitive pay and benefits for new hires. These participants cited low hourly rates or salaries as a significant inhibitor to EI provider recruitment and retention efforts. Often in collaboration with leadership in their parent organization or human resources department, participating program directors described steps to (a) compile and analyze data on current pay, (b) compare pay with other EI programs and similar professions, and (c) work with their budget to offer more competitive pay. For example, Participant 16, a director of a large program with moderate turnover, described comparing EIS salaries across EI programs: We did a comparison with other centers that have behavioral health . . . I tried to get our average salary comparable to those centers. I went to the lower end because I didn't want to overshoot it for this next fiscal year, but that’s still something that I'm looking at.
Similarly, Participant 23, a director of large rural program with low turnover, described working to stay competitive with similar professions: We have tried to remain very competitive with staff. So, we looked across our service area, and compared teacher salaries for our EIS staff for as a comparison. And then home health services, and other hospital settings for our therapy staff.
Although most participants focused on pay, some also described the importance of benefits: “I think our center is fairly competitive with salaries, but our center, in particular, has very good benefits that a lot of applicants don’t think about” (Participant 12, a director from a small program with low turnover). However, no participants described adjusting benefits packages to remain competitive.
Opportunities for promotions and raises: “A career ladder.”
The effort discussed by the second most participants (n = 19) involved re-structuring career ladders to increase opportunities for promotions and raises. These participants cited stagnant pay and limited opportunities for career growth as a contributor to EI provider turnover. Again, often in collaboration with leadership in their parent organization or human resources department, participating program directors designed criteria for promotions and raises based on productivity and longevity. For example, Participant 27, a director of a medium-sized program with high turnover, described providing raises based on productivity: This year we implemented a career ladder that puts staff in charge of getting raises every year if they exceed their job expectations, they’re reaching productivity goals, they're kind of going above and beyond with continuing education, or volunteering for different projects around the center.
Similarly, Participant 11, a program director from a medium-sized program with high turnover, described incentivizing longevity via increased opportunity for promotion for EISs: We did have a requirement for promotion that minimally, they are an [EIS] for three years . . . I’ve been talking to my supervisor team about, “Do we need to bring that down to just two years?” Because people are slipping at that two-year mark. But we’re still analyzing it, “Do we think that would really make a difference or not for retention?”
A few participants, including those whose program was part of a larger parent organization, reported that they lacked the authority to adjust promotion and raise opportunities.
One-time bonuses and perks: “A nice incentive to give.”
The effort discussed by the third most participants (n = 13) involved offering one-time bonuses and perks. In addition to the tangible value, participants tended to discuss the way bonuses and perks helped EI providers feel appreciated. Some directors described formal, annual bonuses connected to productivity, merit, or longevity. Programs varied in their definitions of each. For example, productivity measures included hours of delivered services, hours of delivered billable services, the percentage of services planned in the Individualized Family Service Plan (IFSP) that were delivered, and the percentage of time a provider spent serving families as compared to doing other duties. Beyond formal bonuses, some participants described informal, spontaneous perks (e.g., gifts, gift cards, time off). Participant 24, a director of a large private non-profit program with moderate turnover, described both bonuses and perks: We put some incentives in place where if we have the funding and everyone is meeting their productivity, we might try to give a productivity or merit bonus, you know, if we have the funding. And I think that is a nice incentive to give, or sometimes our CEO might give a half a day off or something like that.
Barriers to providing bonuses and perks included limited funds and restrictive program policies. To overcome this barrier, a few participants discussed paying for perks—“We just chose to do those things personally, like buying a $10 gift card to Starbucks, but again that all comes out of our own personal pocket. Just to try to retain and help employees feel valued” (Participant 4, a director of a small program with high turnover in an urban community). Alternatively, one participant discussed the limitation of bonuses and perks for retention: “No amount of gym memberships, or retention bonuses, or anything like that compares with being able to have summers off and being able to have two weeks of Christmas [like in schools]” (Participant 8, a director of a mid-sized program with high turnover).
Program Management and Organization
Nearly all participating program directors (n = 25) described efforts to address retention via program management and organization, which we defined as the policies and practices set by program directors to hire new providers (e.g., recruitment, interviews) and manage existing providers (e.g., schedules, job duties, supervision). We describe the three main program management and organization-related retention efforts in the sections below.
Flexible and autonomous schedules: “Up to them and their caseload.”
The effort discussed by the most participants (n = 20) involved encouraging flexibility and autonomy in work schedules. These participants cited preferable schedules as a key contributor to EI provider job satisfaction and retention. Flexible scheduling allowed providers to take time off as needed to address personal or family-related obligations (e.g., doctor’s appointments, parent-teacher conferences, school drop-off and pick-up). Autonomy in scheduling empowered providers to create and manage their own schedules (e.g., work longer hours Monday to Thursday and take Fridays off). Program directors encouraged this scheduling if providers met their productivity requirements. For example, Participant 12, a director from a small program with low turnover, explained how much providers valued flexible and autonomous schedules in their overall evaluation of their jobs: How they spend that 40-hours is really up to them and their caseload. So, if someone needs to pick up their child from school, they can do that. They just flex their time sometime within that week to meet their 40 hours. That’s also one of the main things we hear from staff, besides our benefits, the flexibility and schedule is also high in their list.
Similarly, participants discussed providing flexibility and autonomy in providing in-person or remote options for service delivery and program meetings. Participants discussed promoting telehealth to reduce COVID-19 spread and to support providers in rural areas where travel between home visits is especially time-consuming—“We’re using telehealth as much as we can. It’s absolutely an option, especially with decreasing the travel, I encourage it with my staff, even if it’s to supplement what we do” (Participant 19, a program director from a small rural program with moderate turnover).
Comprehensive and transparent hiring: “Don’t want anyone to be surprised.”
The effort discussed by the second most participants (n = 16) involved developing comprehensive and transparent hiring practices. These participants perceived a direct link between the hiring process (e.g., recruiting and interviewing candidates) and EI provider retention. Comprehensive hiring practices included implementing a variety of formal or informal recruitment strategies. Formal recruitment strategies included (a) attending or hosting job fairs, (b) paying for advertisements, and (c) hiring a specialized recruiter. Informal recruitment strategies included (a) hosting student interns from universities and encouraging them to apply, (b) encouraging providers to refer friends or former colleagues, and (c) networking to attract local candidates. For example, Participant 20, a director of a small rural program with moderate turnover, discussed the importance of attracting local candidates: One thing that I try to focus on when hiring is I try to shop local if at all possible. If I hear about a new PT, OT, speech, or EIS, I try to foster those local homegrown people because those are the ones that are going to be the most likely to stay. They don’t have to travel to get to me, they live in one of our counties, and that's why I reach out first.
Transparent hiring practices included (a) discussing the realities (e.g., both positive and negative aspects) of the position with candidates during job fairs and interviews and (b) providing candidates with opportunities to observe EI professionals provide services. For example, Participant 17, a director of a large private non-profit program with low turnover, described the importance of transparency during interviews: We don’t want to sugarcoat it. They [interviewers] always do the good, bad, and ugly of ECI . . . it’s hot and we’re going into homes without air-conditioning, and maybe really humble settings. We don’t want anyone to be surprised about that. You’re going to use your own car, and we don’t want you to be surprised about that. I mean, we literally say, “This is a very hard job.”
Restructured roles and responsibilities: “Take that burden away.”
The program management and organization strategy discussed by the third most participants (n = 15) involved restructuring work roles and responsibilities. These participants cited organizational issues, workload, and overly complex job duties as contributors to EI provider burnout and eventual turnover. The two main types of restructuring efforts aimed at retaining providers included (a) leadership reorganization and (b) job specialization. For leadership reorganization, participants discussed creating additional coordinator positions (i.e., discipline specific leads) who could provide supervision and mentoring. Participant 1, a director of a large program with low turnover, discussed creating a new role to support EISs: We have the two coordinators that work with them, to make sure they meet with them weekly, to go over their responsibilities for their training . . . And now that we’ve created the new roles of the leads, what we’re hoping is, the colleagues will discuss amongst themselves more ideas of how to mentor each other.
For job specialization, participants discussed adjusting workload and responsibilities to create program efficiency and reduce burnout. For example, Participant 12, a director of a small program with low turnover, discussed delegating tasks to create efficiency: We're attempting to implement having evaluation teams, where we have teams that are going to do all of that initial paperwork and everything involved with enrolling children . . . we’re trying to move to have more designated service coordinators to take that burden away from them, so that they can concentrate more on their EIS specialized skills.
Positive Climate and Culture
Nearly all participating program directors (n = 25) described efforts to address retention via a positive climate and culture, which we defined as the intangible aspects of a program that influence interactions between leadership, co-workers, and families. We describe the three main positive climate and culture-related retention strategies in the sections below.
Teamwork and emotional support: “How are you doing?”
The effort discussed by the most participants (n = 22) involved developing a program-wide culture of teamwork and emotional support. These participants cited EI provider isolation, burnout, and trauma with turnover. Strategies to encourage teamwork and emotional support included (a) frequent check-ins and informal group meetings, (b) the development of a committee to address culture and camaraderie, and (c) program-wide teambuilding events. For example, Participant 11, a director of a medium-sized program with high turnover, discussed the importance of emotional support to help providers combat stress: We provide a self-care monthly meeting for them. There’s no talk about performance indicators, there’s no talk about really your position, it’s more just, “How are you doing?” Let’s support them. It’s like a support group for the profession.
When discussing the importance of teamwork and emotional support for retention, participants often discussed challenges associated with COVID-19 (e.g., social distancing, remote work, stress). For example, Participant 26, a director of a large program with moderate turnover, emphasized the ever-increasing importance of cohesion and bonding: So that team building that we used to do, is being missed [since COVID-19] because the work itself can be very heavy and burdensome, but if you have that other part, your team cohesiveness, your team support, it makes a world of a difference for them.
Mission-focused leadership: “Making a difference.”
The effort discussed by the second most participants (n = 17) involved key members of program leadership (i.e., program director, supervisors, leads, mentors) emphasizing the mission of the program. These participants believed that EI providers who had a strong sense of purpose (e.g., improving outcomes for young children and their families) were more likely to stay in their positions long-term. Strategies to promote the mission of the program included (a) emphasizing mission during the hiring process, (b) discussing the mission frequently and posting it publicly (e.g., website, posters, business cards), and (c) embedding the mission in program-wide and individual goals and evaluations. For example, Participant 27, a director of a medium-sized program with high turnover, discussed embracing the mission to encourage providers: We live and breathe the seven key principles of ECI. I keep “The Value of ECI” [pamphlet] sitting on the corner of my desk. Anytime somebody comes in and they're struggling, or they’re frustrated, we bring it back to the family’s perspective, and that we truly are making a difference in the lives of each individual baby that we see.
However, a few participants mentioned that emphasizing the mission of EI could contribute to turnover if providers were unable to meet the demands of the job. For example, Participant 6, a director of a large private non-profit program with high turnover, described the decision-making process for supporting, or firing, a provider who was unable to meet the needs of families: There are families out there that need the service. So, I don’t want to prevent a family from getting a quality service because I can’t help that [provider], or that I feel sorry for that person on staff. So, to me, yes, I want to support staff, but I also want to make sure that the families are getting what they need.
Recognition and positive reinforcement: “Those little things.”
The effort discussed by the third most participants (n = 10) involved leadership providing recognition and positive reinforcement. These participants emphasized the link between EI provider morale and retention. Recognition and positive reinforcement could be tangible or intangible. Tangible strategies included (a) financial incentives (e.g., bonuses and perks), (b) awards (e.g., employee of the month), and (c) celebrations (e.g., holiday parties). Intangible strategies included ongoing verbal praise and recognition (e.g., kudos at staff meetings). For example, Participant 13, a director of a large program with low turnover, described tangible strategies of recognizing providers on social media and newsletters to improve morale:
“We know that those little things bring them a lot of satisfaction in what they’re doing, and they always tell us, ‘That made my day, just seeing that I’m making a difference. It really goes a long way’.” Similarly, Participant 22, a director of a small program with low turnover, discussed developing a more intangible culture of praise and celebration to improve morale: I’ve been really trying hard as a program director to make things a little more fun around here, to give a lot of kudos to staff, and I celebrate everything there is to celebrate, like employee awareness day. There’s always a party going on around here for something.
Training and mentoring
Most participating program directors (n = 23) described efforts to address retention via training (e.g., initial preparation, professional development, continuing education) and mentoring. We describe the three main training and mentoring-related retention efforts in the sections below.
Investment in professional growth: “This is a priority.”
The effort discussed by the most participants (n = 20) involved investing additional money and time in ongoing professional growth. These participants attributed reductions in training budgets with EI provider disengagement, feelings of career stagnation, and eventual turnover. Some common investments in professional growth included (a) hiring full-time trainers or compensating experienced providers to provide mentoring, (b) paying for providers to attend professional development, join professional organizations, or receive continuing education credits, and (c) allocating time or reduced caseloads for providers to receive training. To invest in professional growth, participants mentioned having to make difficult budget adjustments that prioritized the long-term success of the program. For example, Participant 16, a director of a large program with moderate turnover, described prioritizing training: When I took over as director, we didn’t have anything in the budget for trainings for staff. I had to add it to the budget. I’m like this is a priority. We need to get our staff trained, and it helps retain them too . . . they know we're going to help them get further trainings in feeding or some of the new research, they're going to stay on with us.
Alternatively, a few participants described how budgets became so constrained that they had to reduce investments in training. For example, Participant 19, a director of a small rural program with moderate turnover, described losing an individual in a training role so they could instead spend time working directly with children and families: We had someone that is called a “clinical supervisor,” but again when you have a lack of providers, what happens is those providers just get full of kids and caseloads. Even if I try to carve out a percentage of their time to provide some sort of supervision, or mentorship, or something like that, it’s a limited amount of their time.
Comprehensive initial preparation: “Get them where they need to be.”
The effort discussed by the second most participants (n = 18) involved bolstering the comprehensiveness of initial preparation for new hires (e.g., onboarding). These participants emphasized the importance of an intensive and well-rounded onboarding process to address service-oriented skills (e.g., trauma informed practices, feeding, autism), administrative skills (e.g., documentation, policies), and soft-skills (e.g., communication, time-management). Participants emphasized that this onboarding process was necessary to fill in gaps in pre-service training. For example, Participant 3, a director of a small program with high turnover, described preparing recently hired college graduates: We’ve seen that some providers had come in with not enough of the necessary coping skills for the new position, especially in the area that we work in. It’s demanding. It really . . . once they’re hired, we’re going to try our very best to exhaust every possibility, every tool that we have available to get them where they need to be.
In addition to intensive formal training and supervision, participants mentioned the importance of mentoring to help new hires learn the less formal aspects of the job. For example, Participant 14, a director of a medium-sized private urban program with moderate turnover, described the wide range of supports provided by mentors: They go on observation visits with the other staff and then help them learn the paperwork . . . our mileage system . . . learn where the best bathrooms are, where not to go, where to stop for lunch, that kind of thing. That’s really how we mentor.
Targeted learning opportunities: “All those skills vary depending on the person.”
The effort discussed by the third most participants (n = 14) involved implementing targeted learning opportunities. These participants emphasized that one-size-fits-all trainings were ineffective in supporting EI providers and reducing turnover. Instead, these participating program directors (a) analyzed program data to determine critical areas of need, (b) conducted surveys and interviews to identify provider interests, and (c) reviewed individual provider needs to personalize training and support. For example, Participant 1, a director of a large program with low turnover, described providing program-wide training based on areas of need: Everybody will come together . . . we’ll have a half day training, and so we do those whenever we see a systemic problem, we try to go over that, we do a lot of role playing which seems to help people a lot.
For personalized training, Participant 4, a director of a small urban program with high turnover, described the importance of meeting individual provider needs to support retention: Whenever you’re able to train an EIS to meet that productivity—because there are some people that it takes a little bit longer to train, it takes them a little bit longer to pick up organization skills, time management skills, all those skills vary depending on the person and how they learn—that for us would make us successful in retaining.
Discussion
The purpose of this study was to explore the perspectives of Part C EI program directors on efforts to retain providers who work with young children with disabilities or developmental delays and their families. Overall, this study’s findings indicate the need for a comprehensive approach to provider retention, which may in turn serve to enhance Social Determinants of Health (SDOH) in Healthcare Access and Quality for families served (U.S. Department of Health and Human Services, 2022). More specifically, our findings indicate that participants are implementing a variety of program-level retention efforts (i.e., compensation and financial incentives, program management and organization, climate and culture, training and mentoring) that align closely with strategies recommended in OSEP research briefs for retaining special educators (i.e., enhancing professional leadership, induction and mentorship, ongoing professional learning, professional empowerment, supportive workplace environments). One key difference was our participants also emphasized strategies related to compensation and financial incentives (i.e., competitive pay and benefits, opportunities for promotions and raises, one-time bonuses and perks). Especially for EISs, this finding may be reflective of the long history of low pay for workers in early childhood care and education fields (Haack et al., 2022). For therapists (e.g., SLTs, OTs, PTs), who are higher paid, this finding may be reflective of relative decreases in funding and reimbursement rates for EI programs in recent years (Vail et al., 2018).
Another important finding was that participating EI program directors were following some but not all quality indicators developed by ECTA for retention (i.e., strategies rooted in data, revised when needed, discipline-specific, comprehensive). First, only some participants discussed rooting retention efforts in data or revising strategies when needed (e.g., exit interviews to identify why providers left, surveys to provide targeted training), and none described formal efforts to evaluate retention strategies. Second, most participants discussed discipline-specific strategies (e.g., analyzing the competitiveness of salaries across disciplines, providing targeted training and mentoring, reorganizing specific roles and responsibilities for EISs and therapists). Third, most participants emphasized the importance of comprehensive retention efforts (e.g., addressing not just pay but also working conditions and provider support, implementing not just strong induction programs but also ongoing professional development), but only a few described collaborations with colleges, state Part C coordinators, or other EI programs specific to retention efforts. The Division for Early Childhood (2014) provides guidance on recommended practices related to teaming and collaboration.
It is important to note that our study only focused on program-level retention efforts. Research suggests that efforts to reduce shortages and improve the retention of EI providers nationwide requires a comprehensive and aligned approach across multiple systems (e.g., federal, state, professional association, college, individual program; Bruder, 2010; Hebbeler et al., 2012; Ingersoll et al., 2014; Kasprzak et al., 2012; McCollum & Bailey, 1991; Vail et al., 2018). At the state- and federal-level, efforts are needed to address the mix of education- and health-related funding sources (i.e., federal, state, and local funds), reimbursement systems (e.g., Medicaid, insurance, parent fees), and preparation supports (e.g., scholarships, loan forgiveness, decreased certification and licensure costs; Council for Exceptional Children, 2020; Vail et al., 2018). At the professional association- and college-level, efforts are needed to implement standards across disciplines (e.g., Bruder & Dunst, 2005; Bruder et al., 2019) and increase the accessibility of pre-service training (e.g., Grow Your Own programs, fast-track routes, ample field work experiences; Council for Exceptional Children, 2020).
Limitations and Suggestions for Future Research
There are several limitations associated with this research. First, our study only included participants from one state. However, given the large state experiences provider shortages and covers a diverse range of rural and urban communities, the findings from this study could be applicable in similar settings nationwide. Future research should explore retention efforts in additional states, as provider shortages, funding, and policies differ (Kasprzak et al., 2012). Second, our study only included EI program directors. Future research should explore the perspectives of providers, state Part C coordinators, and others involved in retention efforts. Third, our study only included about two-thirds of program directors from the state. Although our sample was representative of programs across the state, there is a chance non-participating program directors had additional perspectives on retention efforts not captured in this study. Fourth, we did not collect demographic data on participant race/ethnicity, education-level, and prior experiences as an EI provider. Future research should further explore the impact of EI program director background and identity. Fifth, the current study was exploratory in nature. Future research should employ additional methodologies to further examine the feasibility, cost-effectiveness, and impact of retention strategies on program-level outcomes, individual provider retention, and child and family outcomes with feedback from multiple stakeholder groups involved.
Conclusion
By gathering the perspectives of EI program directors via interviews, we were able to identify the nuances of participant experiences retaining providers. To date, no published research has gathered the perspectives of EI program directors across a large state with varied demographics specific to this important yet often stress-inducting facet of their work. To support EI program directors and other leaders in the field provide high quality, collaborative services to young children and their families, additional research and training is needed on strategies to improve compensation, working conditions, and supports for providers.
Footnotes
Authors’ Note
The opinions expressed are those of the authors and do not represent the views of the U.S. Department of Education or the Texas Health and Human Services Commission.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by the Office of Special Education Programs, U.S. Department of Education, through grant H325P20005 to Texas Health and Human Services Commission with the University of Texas at El Paso as subcontractor through HHS001088500001.