
Abstract
Early intervention (EI) provision is critical for families who have children with developmental disabilities (DD), but existing evidence suggests accessing EI is not always straightforward. The purpose of this study was to provide a comprehensive description of access to various EI supports (e.g., professionals, services, interventions) for families of young children with suspected or diagnosed DD across the United Kingdom and to investigate perceived ease of access to support, unmet need for support, and barriers and facilitators of access to support. Overall, 673 parental caregivers of children aged 0 to 6 years with suspected or diagnosed DD (e.g., developmental delay, intellectual disability, autism) completed our survey anonymously. Across education, health, and social care, services accessed the most were pediatrics (N = 569, 84.5%), speech and language (N = 567, 84.2%), and general medical practice (N = 530, 78.8%). However, only 18.9% (N = 127) accessed packaged interventions. More than three-quarters (N = 508, 75.5%) reported an unmet need for early support, indicating a mismatch between the availability and capacity of services and demand for support. Parents also reported common barriers (e.g., obstructive services and unhelpful professionals) and facilitators (e.g., supportive and competent professionals, enabling parent factors) of access. Implications for policy, practice, and research are discussed.
Keywords
Early intervention (EI) is the provision of support to ensure optimal child development during early childhood (i.e., 0-6 years), including specific interventions and programs to improve child and family outcomes and contact with various support services across education, health, and social care (Akhmetzyanova, 2016; Dunst, 2008; Harbin et al., 2000; McWilliam, 2016). The provision of EI is important for families of children with developmental disabilities (DD), such as developmental delay, intellectual disability (ID), and autism, due to the presence of delays in cognitive and adaptive skills (American Psychiatric Association, 2013; McDonald et al., 2006; Salvador-Carullaet al., 2011). Furthermore, additional needs, such as child behavior problems and both physical and mental health disparities, can emerge in the early years and persist into adulthood (Allerton et al., 2011; Bailey et al., 2019; Gray et al., 2012; Hastings, 2016; Karpur et al., 2019; Totsika et al., 2011).
Early identification of DD and the provision of EI can improve a range of child and family outcomes including child development and adaptive skills, child behavior, parental mental health, and parental stress (Clark et al., 2018; George et al., 2014; Herman & Marcenko, 1997; Leung et al., 2013; Wallace & Rogers, 2010).However, research data from several studies suggest there are low levels of access to EI for this population, with rates of access as low as 5% for young children with suspected or identified DD (Betz et al., 2004; Birkin et al., 2008; Bromley et al., 2004; Feinberg et al., 2011; McManus et al., 2014, 2020; Rosenberg et al., 2008; Ruble et al., 2005; Salomone et al., 2016; Thomas et al., 2007; Toms et al., 2015; Wei et al., 2014; Zimmer & Panko, 2006). There is also variability in rates of access to EI. For example, Yingling and Bell (2020) found 75.7% of 1,968 autistic children had accessed a state EI program and 71.0% had accessed speech-language, occupational, or physical therapies (respectively, 65.8%, 33.4%, and 18.4%). In contrast, while examining access to EI under Part C of IDEA, a federal law that mandates EI services in the United States, Grant and Isakson (2013) found just 2.7% of age-eligible children across the United States accessed EI, with a range of 1.2% to 6.5% for specific states.
There may be a significant proportion of children with DD who need but do not receive EI, indicating potential unmet need for various EI supports. Furthermore, difficulties accessing EI or services across childhood are reported by parents of children with DD, including difficulties contacting services, limited availability or lack of services, waiting times, cultural barriers, financial barriers, and geographical barriers (Betz et al., 2004; Birkin et al., 2008; Crane et al., 2016; Dababnah & Bulson, 2015; Hussain & Tait, 2015; Khanlou et al., 2017; Kohler, 1999; McWilliam et al., 1995; Zuckerman et al., 2015).
Several factors can influence access to EI for families of children with DD as barriers (factors that have a detrimental effect on access, i.e., prevent, challenge, or stop access) or facilitators (factors that have an enabling effect on access, i.e., sustain, enhance, or support access). These factors can be organized into four levels family (factors related to the family or child), service (factors related to professionals, services, or governing systems), intersection (the intersection of family and service level factors), and contextual (factors related to the context or community; Sapiets et al., 2021).Barriers of access to EI include, for example, lower parental caregiver socioeconomic status (i.e., educational attainment and financial resources), complex referral systems, a poor match between service and family factors (i.e., whether the services provided match the nature of the family’s needs), and limited government funding for EI (Sapiets et al., 2021). In contrast, facilitators of access to EI include, for example, higher parental caregiver socioeconomic status, wide service eligibility criteria, consideration of families’ cultural and contextual background during EI development, and government legislation stipulating funding for EI (Sapiets et al., 2021).
Current literature on families’ access to EI is fragmented. Previous studies typically focused on one aspect of EI provision within the broad scope of EI, such as specific services or interventions (e.g., Birkin et al., 2008; Feinberg et al., 2011; Grant & Isakson, 2013; Karpur et al., 2019), or one developmental condition within DD, such as autism (e.g., Birkin et al., 2008; Thomas et al., 2007; Wei et al., 2014). The findings of these studies are informative at highlighting potential gaps in access to EI, such as gaps in mental health services (Wei et al., 2014). However, there is a lack of research capturing access to a diverse range of EI supports (i.e., across education, health, and social care service systems) for families of children with DD broadly. In addition, a large proportion of available research data on access to EI is either outdated or retrospective, limiting the practical applicability of the findings (e.g., Betz et al., 2004; Birkin et al., 2008; Kohler, 1999; McManus et al., 2020). Research in this area is further limited in scope due to small and potentially unrepresentative sample sizes, especially for young children (e.g., Bromley et al., 2004; Dababnah & Bulson, 2015; Kohler, 1999; Toms et al., 2015).
It is clearly important to ensure families of children with DD are able to access EI. To inform ways to improve EI access, it is first crucial to explore what services and supports families are currently accessing or not accessing, in addition to any unmet need for support and barriers and facilitators of access. Through recruiting a large sample of families of young children with suspected or diagnosed DD across the United Kingdom (UK), the present study aimed to address gaps in the existing research. Our research questions include:
Method
Participants
Overall, 673 parental caregivers of children with diagnosed or suspected DD completed the survey (see Table 1 for key characteristics). The majority of respondents were the child’s biological mother (N = 613, 91.1%) although a few were biological fathers (N = 28, 4.2%), adoptive mothers (N = 13, 1.9%), grandmothers (N = 10, 1.5%), or other caregivers (N = 5, 0.7%). The majority of participants lived in England (N = 505, 75.0%). Compared with whole population census data for England and Wales in 2011 (Office for National Statistics [ONS], 2018), our sample had an overrepresentation of parental caregivers that identified their ethnicity group as White (N = 618, 91.8% of participants; 86.0% of census) and an underrepresentation of parental caregivers that identified their ethnicity group as Asian (N = 24, 3.6% of participants; 7.5% of census), Black (N = 5, 0.7% of participants; 3.3% of census), Mixed/Multiple (N = 8, 1.2% of participants; 2.2% of census), and other ethnicity groups (N = 3, 0.4% of participants; 1.0% of census). Fifteen parental caregivers (2.2%) did not identify their ethnicity.
Participant Characteristics.
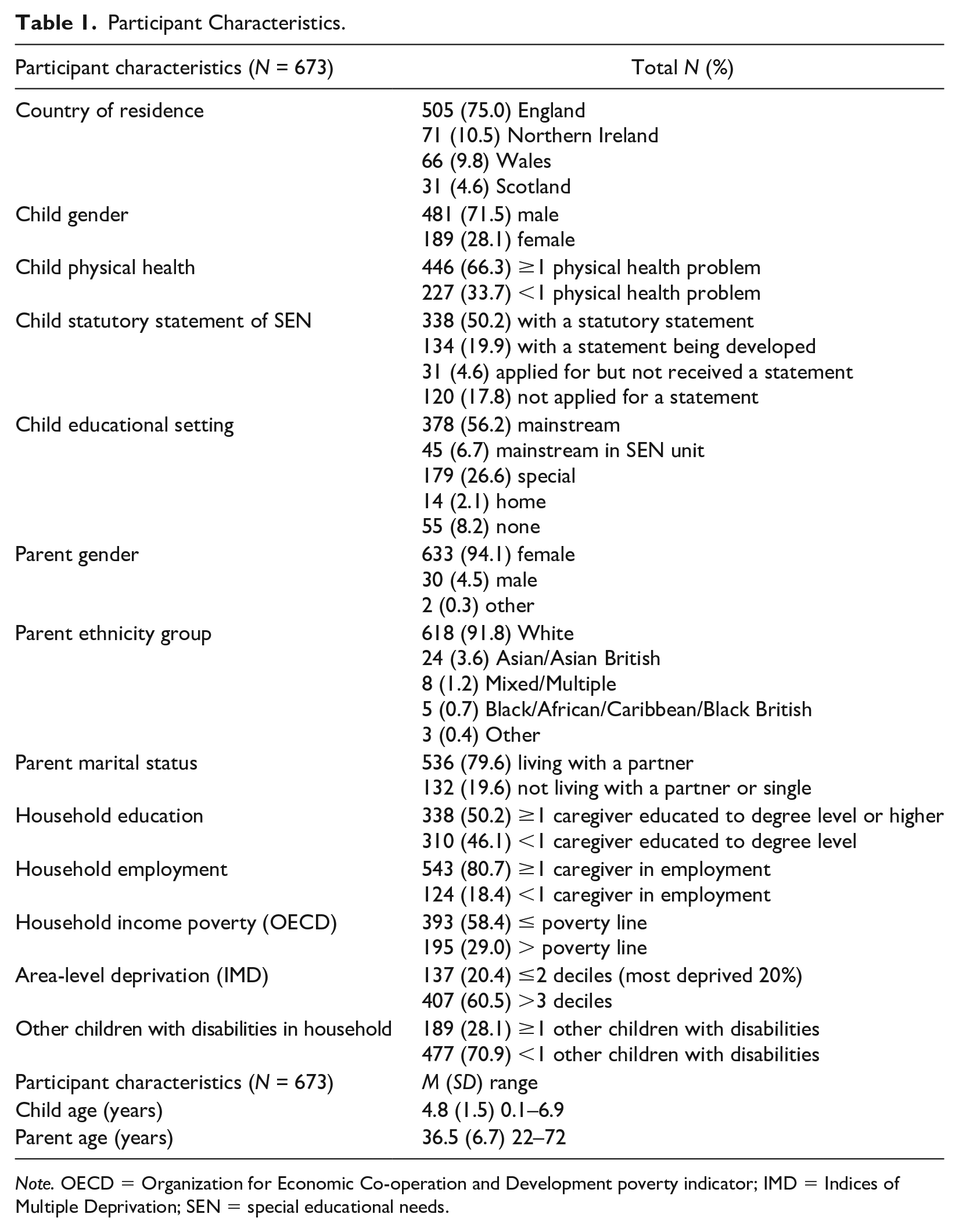
Note. OECD = Organization for Economic Co-operation and Development poverty indicator; IMD = Indices of Multiple Deprivation; SEN = special educational needs.
Child characteristics
The majority of the children were male (N = 481, 71.5%), and the mean child age was 4.8 years (SD = 1.5, range 1 month to 6 years 10 months). A variety of DD diagnoses and labels were reported (see Table 2). The most common DD diagnoses or labels were autism (N = 524, 77.9%), special educational needs (SEN; N = 390, 57.9%), ID (N = 328, 48.7%), and developmental delay (N = 317, 47.1%). More than half of the children also had a physical health condition (N = 446, 66.3%) such as a mobility problem, a visual impairment, a hearing impairment, or epileptic seizures. More than half of the children (N = 338, 50.2%) had received a statutory statement of SEN (i.e., a legally enforceable document detailing the child’s education, health, and social care needs and additional support that must be procured by the local government authority to meet these needs). It is important to note that not all children with SEN will have had their needs recognized through a statutory statement. More than half of the children (N = 378, 56.2%) attended a mainstream educational setting (i.e., school, preschool, and nursery).
Child Developmental Disability Label and Identification Stage.
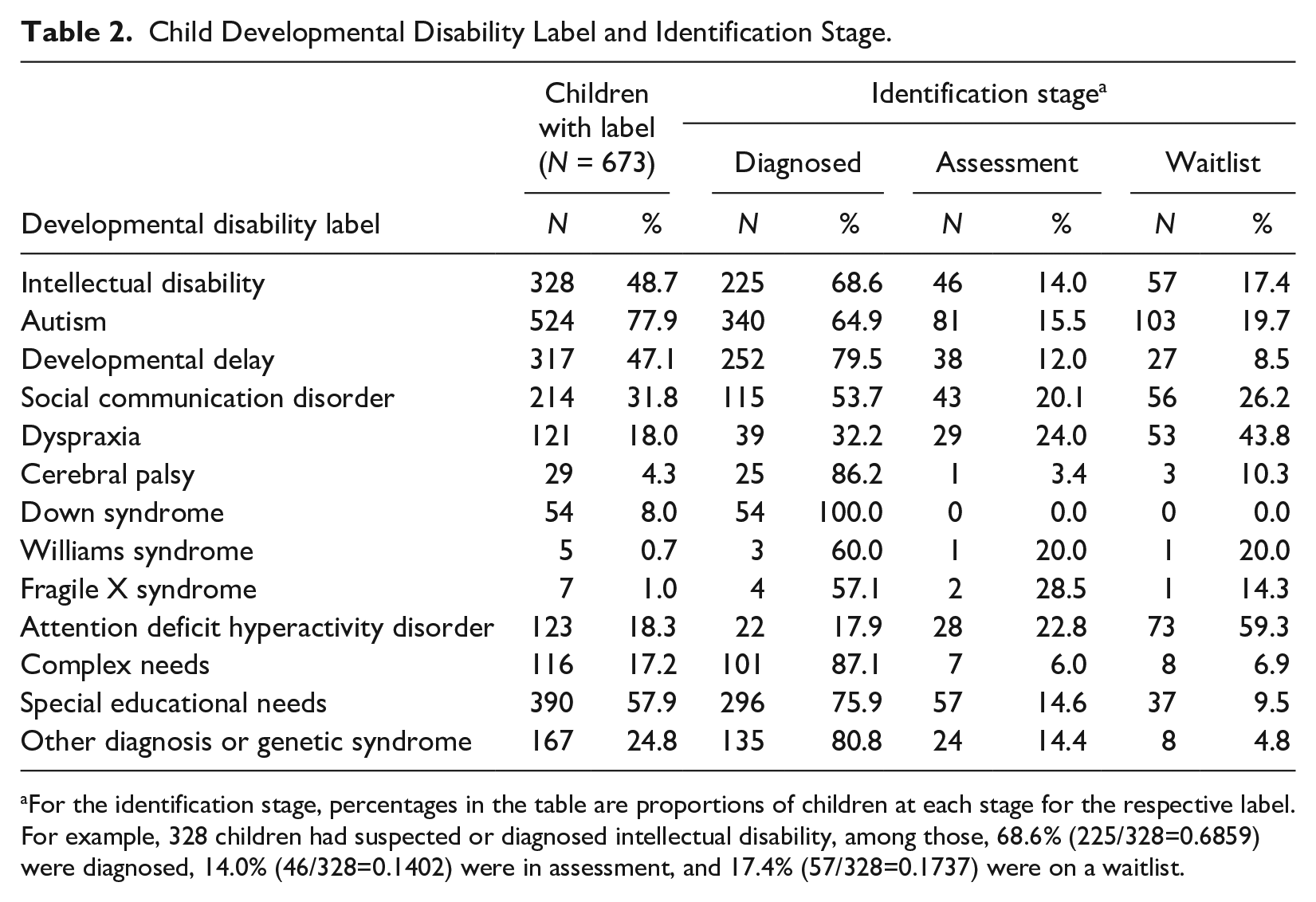
For the identification stage, percentages in the table are proportions of children at each stage for the respective label. For example, 328 children had suspected or diagnosed intellectual disability, among those, 68.6% (225/328=0.6859) were diagnosed, 14.0% (46/328=0.1402) were in assessment, and 17.4% (57/328=0.1737) were on a waitlist.
Procedure
Ethical approval was granted by the University of Warwick’s Humanities and Social Sciences Research Ethics Committee (reference 57/17–18). Between September 2018 and May 2019, UK parental caregivers of children aged 0 to 6 years (from birth until the day before their seventh birthday) with suspected or diagnosed DD (developmental delay, ID, and/or autism) were invited to complete the survey anonymously. As there can be long delays to receive a DD diagnosis (especially autism diagnosis, e.g., Crane et al., 2016), parental caregivers of children with suspected DD were included. Prior research indicates parents often were the first to identify developmental delays and were generally correct in their assessment (e.g., Bellman et al., 2013). The child age range of 0 to 6 years was selected, consistent with our conceptualization of EI as the provision of formal support across service systems during early childhood (i.e., 0–6 years). Furthermore, this age range captured children whose DD was recognized following contact with education services, as in the UK it is only compulsory for children to begin full-time education following their fifth birthday.
Participants were recruited via social media and distribution via several UK organizations that worked with families of children with DD, such as charities, independent service providers, and specialist schools. The survey took approximately 30 minutes to complete and was available online (hosted by SnapTM Surveys) or by surface mail, according to participant preference. In the online survey, all questions were optional except for “child age.” The survey was available in the English language only. As the survey was shared widely (social media and various organizations) and participation was both anonymous and voluntary, it was not possible to ascertain the survey response rate. Participation was anonymous to reduce potential concerns regarding support from services being impacted by participation. No incentives were provided for participation or survey completion.
Survey Development and Measures
Data on access to EI supports and child and family characteristics were collected in the survey. The survey was developed by the authors with input from a group of key stakeholders, including parental caregivers of children with DD, EI professionals, and charity organizations that worked with families. Prior to distribution, the survey was piloted with four parental caregivers of children with DD and adapted based on their feedback (e.g., the terminology used, clarity of questions, length). Parental caregivers who piloted the survey were specifically recruited through a charity organization for this purpose, as they had young children with DD and experience of access to EI supports in the United Kingdom. A copy of the survey is available from the first author on request.
Access to support
Access to support was measured in several ways to capture access to various EI supports (e.g., professionals, services, interventions). A comprehensive list of 49 EI support sources was included in the survey. The list was developed with input from a group of key stakeholders (see above) and described professionals and services in the UK context at the time of data collection. EI support sources were presented in three groups. The first group included 27 key professionals across health, education, and social care services, such as general medical practitioner (i.e., a community-based medical doctor that specialized in general practice and the treatment of common medical conditions in primary care), occupational therapist, school staff, social worker, and respite carer (see Table S1 in the Supplemental Materials available online). The second group included 10 additional health specialists, such as neurologist, ophthalmologist, and podiatrist (see Table S2 in the Supplemental Materials available online). The third group included 12 other supports, such as parent groups, telephone helplines, websites, and children’s centers (see Table S2).
Participants reported their family’s contact with each of the 27 key professionals (yes/no/on a waitlist/not sure) in the preceding 12 months. For the 10 additional health specialists and 12 other supports, participants only reported whether their family had been in contact with these in the preceding 12 months.
If the participant reported they had not accessed support from any of the 27 key professionals in the past 12 months, they were later asked if they had wanted support from that professional (yes/no). Unmet need was defined as support wanted but not accessed (i.e., if the participant reported they had not accessed support from the professional and wanted support from the professional). A total count of unmet need for supports was the sum of professionals the participant wanted but had not accessed (possible range 0–27).
If a participant reported they had accessed support from any of the 27 key professionals in the past 12 months, they were later asked to rate the ease of access to that professional on a 5-point Likert-type scale, where 1 was “very difficult” and 5 was “very easy.”
Participants were also asked if, in the past 12 months, their child had received any interventions to support their development or they themselves had received interventions to support them as parental caregivers (yes/no). A few interventions were listed as examples to help participants complete the question (e.g., Early Bird, Hanen®, Incredible Years®, Triple PTM, Applied Behavior Analysis [ABA], SCERTS®, TEACCH®, therapy, counseling). If a participant responded “yes,” they were asked to list interventions received in a free-text response box. These responses were analyzed to identify whether the intervention mentioned was a packaged intervention program that was additional to the 49 EI supports covered in the quantitative part of the survey (see below, Analysis).
Participants were also asked to describe up to three things that had made it difficult for their family to access support (i.e., barriers) and up to three things that had helped their family access support (i.e., facilitators). These responses were analyzed to identify barriers and facilitators of access to EI (see below, Analysis).
Child and family characteristics
Data were gathered in the survey on the variables reported in Table 1. For child DD, participants identified any DD labels professionals had told them their child had (or might have had) from a list of 12 (see Table 2). In addition, there was a free-text response box where participants reported any other diagnoses or genetic syndromes. Participants also reported on the identification stage of applicable DD labels (i.e., if they were waiting for an assessment, going through an assessment, or had received the diagnosis).
A self-identification measure of ethnicity recommended by the UK ONS was used, comprised of 18 responses across five ethnicity groups (Asian, Black/African/Caribbean, Mixed/Multiple, White, and Other; Potter-Collins, 2011). Family income was equivalized using the modified Organization for Economic Co-operation and Development (OECD, n.d.) scale. Income poverty was measured using the OECD’s definition: families with an income below 60% of the UK median equivalized income (£28,400 at the time of data collection; ONS, 2019) were classified as living in poverty. Using zip codes, neighborhood deprivation was ascertained from the UK Indices of Multiple Deprivation (IMD) scores, comprised of seven deprivation domains (income, employment, education, health, crime, housing, and living environment; UK Government, 2019). Neighborhood deprivation was dichotomized to identify participants who lived in the 20% most deprived areas of their UK country (i.e., IMD deciles 1–2) versus participants who lived in less deprived areas (i.e., IMD deciles 3–10).
Analysis
Data from online and hard-copy surveys were collated into a single database. Descriptive statistics were calculated for quantitative data. Free-text responses on interventions accessed were analyzed to identify participants who had accessed a packaged intervention, defined as a multi-session support package. Inclusion criteria for responses to be coded as a packaged intervention were: (a) specific intervention program named (e.g., “Triple P Stepping Stones” “SCERTS” “Incredible Years Course” “ABA 12 week program” “Funded and did the TEACCH train program myself” “PECS [Picture Exchange Communication System]”) or (b) clear indication of multiple-session support additional to those covered in the quantitative part of the survey (e.g., “Play therapy sessions” “Art therapy” “Counselling for Carers. . .10 sessions” “Two sessions with a family therapist”).
Exclusion criteria for responses to be coded as a packaged intervention were: (a) multiple-session support covered in the quantitative part of the survey, where there was no indication of an additional packaged intervention (e.g., “Speech and language therapy” “Portage” “Physiotherapy” “Occupational therapy” “Sure start”), (b) single session or one-off support (e.g., “EHCP [education, health and care plan, i.e., statutory statement of SEN in England] Workshop” “Sleep Training Study day” “Sensory Workshop” “Specialist teacher came in to give advice about what to put in place”), (c) support provided without the mediation or involvement of a service or professional (e.g., “I did a lot of work unsupported by professionals by reading books and watching videos online and then used this to help my daughter. . .Hanen’s Talkability for Verbal Autistic Children”), and (d) no intervention program named or vague response (e.g., “At school only” “Behavior support”).
Framework analysis, a rigorous and systematic qualitative analysis approach comprised of several distinct but interrelated stages (i.e., familiarization, identifying a framework, indexing and charting data, mapping, and interpretation; Ritchie & Spencer, 1994; Ward et al., 2013), was used to explore barriers and facilitators of EI access. The first step, familiarization with the data, involved reading all responses. Next, a framework was identified, namely, our existing framework of factors influencing access to EI (Sapiets et al., 2021), to organize the data in a meaningful and manageable way. Subsequently, data were charted according to the type of effect (barrier or facilitator) and the factor level (family, service, intersection, or contextual; see above, Introduction; Sapiets et al., 2021). Prior to analysis, the first author developed a comprehensive a priori coding scheme based on the framework of factors influencing access to EI (Sapiets et al., 2021) to identify barriers and facilitators of access across factor levels. A bottom-up approach was then used to code the charted data; the authors delineated prominent barriers and facilitators that emerged from the data. During data analysis, the coding scheme was iteratively reviewed and revised by the authors. Where similar barriers or facilitators emerged, codes were merged into an overarching barrier or facilitator code, if appropriate. For example, “knowledgeable professionals” and “positive engagement with professionals” codes were integrated into an overarching “supportive and competent professionals” facilitator code.
We counted the frequency of mentions of barrier or facilitator codes by participants rather than the frequency of participants who reported the code, as this captured instances where participants described multiple things that impacted their access related to one overarching barrier or facilitator. For example, one participant reported “Waiting lists” and “Long forms to fill in” were barriers of access, which were both coded as service-level barriers (i.e., reflected
A subset of the data (N = 80 participants, 11.9%) was independently coded by two of the authors, and interrater reliability was calculated based on the percentage of agreement for the codes identified and Cohen’s κ (Cohen, 1960). There was substantial interrater reliability for the codes identified (mean agreement 87.2%, range 84.5–90.3%, mean κ = 0.74, range 0.49–0.93).
Results
Access to EI Support Sources
All participants provided data on their family’s access to a range of EI support sources, including access to professionals, services, and interventions.
Access to interventions
Less than one-third of participants (N = 197, 29.3%) reported they or their child had received an intervention in the preceding 12 months, either to support child development or the participant in their role as parental caregiver.
Using our coding scheme (see above, Analysis), free text responses from less than one-fifth of participants (N = 127, 18.9%) described access to a packaged intervention, supplemental to contact with the 49 formal support sources (i.e., professionals and services) described below. A wide range of packaged interventions were reported by participants. The most frequently reported packaged interventions were: Early Bird, ABA, Hanen Programs®, Triple PTM Parenting Programs, TEACCH®, Incredible Years®, See and LearnTM, SCERTS ®, and talking therapy or counseling (see Table S3 in the Supplemental Materials available online).
Access to professionals and services
Of the 49 formal EI support sources listed in the survey (i.e., professionals, services), supports accessed by the highest proportion of participants were pediatrician (N = 569, 84.5% of participants accessed), speech and language therapist (N = 567, 84.2%), general medical practitioner (N = 530, 78.8%), dentist (N = 511, 75.9%), and school staff (N = 482, 71.6%). Supports accessed by the smallest proportion of participants were: foster carer (N = 7, 1.0%), podiatrist (N = 26, 3.9%), endocrinologist (N = 26, 3.9%), support to manage direct payments independent from the local (government) authority (N = 38, 5.6%), and independent support advisor (N = 40, 5.9%). Data on participants’ access to the 49 support sources are presented in full in Tables S1 and S2 in the Supplemental Materials available online.
Waitlist to access professionals
Approximately one-third of participants (N = 221, 32.8%) were on a waitlist for at least one of the 27 key professionals (M = 0.6 key professionals, SD = 1.1, range 0–11; Table S1). Professionals with the highest proportion of participants on a waitlist to access were: occupational therapist (N = 47, 7.0%), educational psychologist (N = 46, 6.8%), staff from a team or service responsible for assessing SEN (N = 30, 4.5%), mental health professional (N = 30, 4.5%), and sleep practitioner (N = 23, 3.4%).
Unsure of access to professionals
Almost one-quarter of participants (N = 162, 24.1%) were “not sure” if they had accessed support from at least one of the 27 key professionals. Professionals with the highest proportion of participants unsure of access were: family support worker (N = 28, 4.2%), staff from a team or service responsible for assessing SEN (N = 27, 4.0%), behavior specialist (N = 27, 4.0%), advocate (N = 21, 3.1%), and independent support advisor (N = 21, 3.1%).
Unmet Need for EI Supports
More than three-quarters of participants (N = 508, 75.5%) reported a perceived unmet need for at least 1 of the 27 key professionals (M = 3.2 key professionals, SD = 3.2, range 0–17; Table S1). Of participants who had not accessed the respective professional (not the total sample), professionals associated with the highest perceived levels of unmet need were: occupational therapist (N = 136, 52.9% of participants who had not accessed an occupational therapist), educational psychologist (N = 131, 52.8%), staff from a team or service responsible for assessing SEN (N = 83, 52.2%), behavior specialist (N = 232, 43.0%), and pediatrician (N = 28, 40.0%).
Ease of Access to EI Supports
Mean ease of access ratings for the 27 key professionals were between 2.3 and 3.8 (possible range 1–5; Table S1). Professionals with the highest ease of access ratings were: foster carer (M = 3.8, SD = 1.0), dentist (M = 3.8, SD = 1.0), charity worker (M = 3.7, SD = 1.1), optician (M = 3.7, SD = 1.0), and advocate (M = 3.6, SD = 1.2). Professionals rated the least easy to access were: mental health professional (M = 2.3, SD = 1.3), social worker (M =2.4, SD = 1.3), staff from a team or service responsible for assessing SEN (M = 2.6, SD = 1.2), home support staff (M = 2.6, SD = 1.3), and behavior specialist (M = 2.6, SD = 1.3).
Barriers and Facilitators of Access to EI
Barriers to EI access were identified from participants’ descriptions of things that made it difficult for their family to access support. Facilitators of access to EI were identified from participants’ descriptions of things that helped their family access support.
Barriers
Six overarching barriers were identified (see Table S4 in the Supplemental Materials available online), which covered service, family, and intersection factor levels. Barriers with the highest count of mentions by participants were: service-level barriers (e.g., insufficient resources and capacity, adverse or inflexible service features, and lack of continuity; N = 711 mentions), unhelpful professionals (e.g., negative engagement styles, obstructive actions, limited knowledge; N = 225), complex service system (e.g., lack of service coordination or collaboration, absence of information on services; N = 190), and parental caregiver barriers (e.g., limited knowledge, other responsibilities, time constraints, lack of resources or support from family and peers; N = 133; Table S4). A small group of participants (N = 64, 9.5%) reported no barriers of access to EI.
Facilitators
Seven overarching facilitators were identified (see Table S5 in the Supplemental Materials available online), which covered service, family, and intersection factor levels. Facilitators with the highest count of mentions by participants were: supportive and competent professionals (e.g., positive attitudes and engagement styles, proactive support, knowledgeable; N = 151 mentions), empowered parental caregivers (e.g., resources, skills, proactive behaviors, knowledge; N = 133), peer and family support (N = 127), and accessible services (e.g., accessible features of service delivery, flexibility, provision of resources, availability, continuity; N = 119; Table S5). More than one-fifth of participants (N = 154, 22.9%) did not identify any facilitators of access to EI.
Discussion
The present study provides comprehensive data on current levels of access to EI and supports among a large sample of families of young children with suspected or diagnosed DD in the UK. Our findings show families of young children with DD access support from a diverse array of professionals and services across education, health, and social care (similar to Maltais et al., 2020). However, only a small proportion of families access packaged interventions that are generally considered internationally to constitute the core of EI provision. There was also variation in families’ access to support.
Access to primary health services (i.e., general medical practitioner, health visitor, dentist, and optician) was high. There was a low proportion of participants on a waitlist for primary health services and unmet need for these services was low. Primary health services were also rated easy to access. These findings may reflect the fact that primary health services are universally free in the UK. Moreover, these services do not require a referral to access and are community-based (i.e., provided in local settings, including at home). High levels of primary health service access may also reflect the increased prevalence of health conditions among children with DD (Allerton et al., 2011). In addition, primary health services in the UK are a gateway to more specialist services, as referrals from primary care are often required to access specialist services. Therefore, repeated contact with primary care services may be a necessity for families to obtain referrals to diagnostic or other specialized services (e.g., Crane et al., 2016; Zuckerman et al., 2015).
Access to specialized health services was less straightforward, which may reflect the diverse range of specialized supports covered in our survey and the variety of settings in which these can be delivered (e.g., community, hospitals, and specialist centers). Pediatrics and speech and language were accessed by the highest proportion of families, which is likely due to their key roles in DD assessment and EI provision in the UK. Previous research indicates communication development concerns facilitate both parental support seeking and professional referral to EI (Sapiets et al., 2021). Furthermore, communication delays are reported as the most common reason for entry into EI programs (Sapiets et al., 2021), which may explain the high access to speech and language in our study. This may also be due to the high proportion of children with suspected or diagnosed autism in our sample, as speech and language therapy is one of the most common intervention approaches for children with autism in the UK (Denne et al., 2018). Furthermore, several packaged interventions reported by participants in the present study were predominantly communication-focused (e.g., Early Bird, Hanen Programs®, TEACCH®, See and LearnTM, SCERTS®, MakatonTM courses for caregivers, Pediatric/Pre-school Autism Communication Therapy, PECS®). Despite high access, pediatrics and speech and language were rated as being relatively difficult to access, which potentially reflects a high demand for these services or difficulty obtaining a referral to them. The importance of speech and language support emerged in participants’ free-text responses, as several reported paying for private services or access through other services (e.g., children’s center, school). In addition, several participants reported limited capacity (or complete absence) of publicly funded speech and language services was a barrier, which may be suggestive of variation in public speech and language service provision.
Educational psychology and occupational therapy were accessed by around half of the participants. In comparison to other professionals, there was a high proportion of participants both on a waitlist and reporting an unmet need for these. Educational psychologists in the UK generally assess children’s learning and development using psychological approaches and techniques, in addition to supporting children, their families, and schools to promote children’s emotional and social wellbeing. The role of educational psychologists in the UK is similar to that of school psychologists in other countries, but they are not typically school-based in the UK. Instead, educational psychologists are positioned at the level of the local educational authority and require a referral to access their services. It is likely these supports are in high demand for families of children with DD, due to the nature of the difficulties associated with DD. However, our findings highlight potential failures across UK service delivery to meet these needs. Similar to speech and language, participants reported limited capacity (or absence) of publicly funded educational psychology or occupational therapy was a barrier, in addition to difficulties obtaining referrals and inflexible entry criteria (e.g., age, diagnosis, catchment area). In contrast, participants reported their ability to fund these services privately was a facilitator.
Access to mental health and sleep practitioners was low, and there was a moderately high waitlist plus relatively high level of unmet need reported for these. This finding is consistent with previous UK research (Bromley et al., 2004; Toms et al., 2015). Of all professionals listed in the survey, mental health professionals were rated the most difficult to access. Difficulties accessing these services may reflect the complex, multifactorial nature of mental health and sleep disorders in children with DD and a general lack of knowledge of this among professionals, which is further confounded by a limited capacity of specialist services (Read & Schofield, 2010; Royal College of Psychiatrists [RCP], 2016; Sutton et al., 2019). Previous research demonstrates an inadequate capacity of mental health services to serve children with or without DD (Toms et al., 2015). In the UK, children may be excluded from mainstream mental health services due to the presence of DD or challenging behavior; or excluded from DD services if they do not have the “right” diagnosis (RCP, 2016). Conflict between services regarding entry criteria, terminology, or provision can result in “families being left stranded between services” (RCP, 2016, p. 14).
Access to education was generally high. Equally, access to teams in services that are responsible for assessing SEN was high, but these also had a high proportion on a waitlist and high levels of unmet need. Formal identification of SEN is often a requirement to access specialist EI support in the UK, and so these services are often crucial. Barriers of access to teams that assess SEN reported by participants included: insufficiently resourced services, complex processes, extensive delays and waiting times, unsupportive or obstructive professionals, and having to “fight” to access support (e.g., parents’ commented “Cuts in SEN” “waiting times for the EHC [education health and care needs] assessment and draft and communication from the LA [local (government) authority] is appalling”). Similar barriers of access to SEN assessment and subsequent provision in England were found by Cullen and Lindsay (2019).
In the United States, early childhood special education is a key aspect of EI provision (Reichow et al., 2016). While some educational supports in the UK are similar (e.g., Portage, specialist educational provision, educational psychology, educational interventions), there is no direct comparison. Therefore, there may be scope to expand early childhood special education in the UK. The majority of children in the present study attended a mainstream educational setting, rather than a specialist school or SEN unit within a mainstream school. While this is promising in terms of inclusion, it may indicate limited educational support if the mainstream provision has insufficient resources or expertise (e.g., parents’ reported “Lack of funding at schools to provide additional support while waiting for a diagnosis” “Lack of understanding at first mainstream primary school”). Participants free-text responses on interventions accessed indicated that several children had accessed these at school (e.g., parents’ reported “School do TEACCH and other specialist interventions” “ABA therapy, speech therapy and play therapy—all at special school” “We managed to get our child in a school that has taken on the Hanen method, is also taking on SCERTS”). While this demonstrates the potential importance of school for access to intervention programs, it also highlights a potential gap in provision for younger children. This finding needs to be interpreted with caution as participants were not directly asked to specify where EI support sources were accessed.
Services offering support for families appeared to be a challenge to access, which may represent a key gap in provision in comparison to services directly focused on children (cf. Turnbull et al., 2007). Access to home support, respite, and family support workers was low, and around one-fifth of the total sample perceived these as an unmet need. This is likely an underrepresentation, as families are often not aware of the availability or importance of family-focused supports in comparison to child-focused supports (Harbin et al., 2000; Turnbull et al., 2007). As social workers typically link families to family-focused services (or act as gatekeepers), these findings may in part be explained by the low rate of access to (and reported difficulty of accessing) social workers in our sample. This is supported by previous evidence of an association between a lack of contact with a social worker and lower awareness of respite services among parental caregivers of children with ID in the UK (Chadwick et al., 2002).
Similarly, access to social work for families of children with DD has been reported as problematic by practitioners (Okumura et al., 2018). Participants in the current study reported limited capacity of and increasing thresholds to access family-focused supports were barriers (e.g., one parent reported “Told we didn’t need [respite and personal budget] as we are not in crisis and doing very well”), which contradicts the very principles of EI (i.e., preventive support). Low rates of access to family-focused EI support are especially concerning, considering the provision of child-focused supports alone may not be as effective at improving child development.
Access to interventions, especially packaged interventions, was considerably low. Furthermore, there was substantial variation in the interventions reported by participants, which covered a range of child-focused (e.g., ABA, SCERTS®), parent-focused (e.g., parenting courses, counseling), and family-focused (e.g., family therapy) supports. This may partly be due to the question used to capture intervention access; the question was intentionally broad to capture the wide range of interventions that can be provided to children with DD and their families. Our findings may not thoroughly reflect participants’ levels of access to packaged interventions, as participants were required to name interventions their family had accessed in a free-text response box. This relied on participants being aware of (and able to recall) interventions. Eight of the most frequently reported packaged interventions were included as examples listed in the question (Early Bird, ABA, Hanen Programs®, Triple PTM, TEACCH®, Incredible Years®, SCERTS®, and talking therapy or counseling), although other examples listed were not reported by any participants (Early Intensive Behavioral Intervention, Parents Plus Early Years Program, and CAN parent). Nonetheless, a considerable number of additional packaged interventions were reported by participants (e.g., See and LearnTM, Cygnets, Pediatric/Pre-school Autism Communication Therapy), which gives some confidence in the validity of data gathered using this free-text approach.
Significant levels of unmet need for support in the early years are highlighted in our findings, as more than three-quarters of families perceived an unmet need for at least one EI support. Prominent areas of perceived unmet need included: (a) assessment and/or provision of supports for DD and associated needs (e.g., occupational therapy, educational psychology, SEN assessment, behavior support, speech and language therapy, sleep support), (b) provision of family-focused supports (e.g., respite, family support work), and (c) general health services (e.g., pediatrics, dentistry). Our findings indicate a potential mismatch between the availability and capacity of services to support children with DD and the demand for support (i.e., number of families perceiving the need for support), which may be related to austerity policies and higher prevalence of some DD diagnoses (e.g., autism; Chiarotti & Venerosi, 2020). It is not unusual for families to report wanting more services than they receive (e.g., Harbin et al., 2000), particularly if they perceive access to more specialized supports will lead to better child outcomes (McWilliam et al., 1995). However, as access to more services or professionals can be negative for families (McWilliam, 2016), the perceived unmet need for support from specialized services may instead reflect a lack of understanding or expertise of DD in nonspecialized services.
A crucial finding in our study is the identification of the complexity of the EI system in the UK as a barrier of access, in addition to a disjointed approach to the provision of support across services. In addition, participants reported collaboration and communication between EI professionals and services was a facilitator of access (cf. Atkins et al., 2020). For the past four decades there have been significant developments moving away from fragmented service systems (i.e., with multiple agencies working autonomously) toward achieving a more comprehensive and coordinated service system for EI in the United States (Harbin et al., 2000). Despite progress toward this goal, Harbin et al. (2000) highlight interagency coordination is complex and nuanced, with service delivery models being influenced by an ecological cluster of interacting factors, and “the enactment of legislation and the implementation of that legislation are very different processes” (p. 387). While similar efforts have also been made in the UK, for example, the Children and Families Act in 2014 and the SEN and Disability Code of Practice in 2014, it is clear there is still a long way to go to achieve a cohesive service delivery system for families. There was also a recurring rhetoric of families having to “fight” to access various supports in our study (cf. McWilliam et al., 1995), due to (at least in part) the inadequate capacity of services to serve families of children with DD. This suggests access is based on parents’ ability to advocate for support, raising concerns regarding equity.
Implications for Policy, Practice, and Future Research
Several implications can be drawn from our findings which can inform initiatives to improve access to EI for families of children with DD.
Policy and practice
It is important for policy and public health to acknowledge and address the high level of unmet need. In terms of practical implications, improving professionals’ engagement styles and understanding of both family needs and available services is key to facilitating access, which will enable professionals to more effectively support families. Change at a wider systemic level is also needed, such as simplifying processes, coordinating support services, examining service coverage and requirements (i.e., age, diagnosis) to ensure no families fall through the net, and increasing government investment in EI support services.
Existing initiatives to improve the provision of EI in other contexts could be adapted to improve access to EI in the UK, such as service coordination under Part C of IDEA in the United States (Harbin et al., 2000; McWilliam, 2016). This is a coordinated approach to provision across a comprehensive service system, which incorporates individualization, family-centered focus, integration of therapies, and inclusion (see Harbin et al., 2000; McWilliam, 2016). As these characteristics appear congruent with the barriers and facilitators of access to EI raised by families in the present study, implementation of service coordination for EI in the UK. context may be beneficial. A shift away from medical-model and therapist-orientated approaches would be facilitated by enhancing caregiver-oriented support and recognizing caregivers as equal partners in EI.
It may also be beneficial to draw on NHS England’s keyworker pilot, which is currently targeting children and young people with ID and/or autism who are inpatients in (or at risk of being admitted to) a mental health hospital (NHS England, n.d.). If successful, the keyworker model could be expanded to support all children with suspected or diagnosed DD and their families, in addition to those perceived to have “the most complex needs,” thus ensuring a more proactive approach to supporting children and families to “get the right support at the right time” (NHS England, n.d.).
Future research
Future research on families’ access to EI will be beneficial, especially population-based studies. The development of comprehensive quantitative measures of access to interventions will also be advantageous. In addition to the areas covered in the present study, collecting data on the: (a) location of support provision (e.g., family home, community service, school, and hospital), (b) funding (public, private, or other), (c) orientation (therapist or caregiver-oriented), (d) focus of support (child, parental caregiver, and family-focused), (e) resources required to access (e.g., service costs, travel, and time), and (f) flexibility of support (i.e., ability to tailor to individual and family needs or highly specified curriculum to follow) will be helpful to further understand families’ experiences of access to EI. In addition, future research should capture data from a range of EI stakeholders (children and adults with DD, parental caregivers and families, professionals working across education, health, social care, and other services, service providers, commissioners of services, etc.). Last but not least, to ensure equitable access to EI for all families, future research should identify interacting factors linked to variation in levels of access across families.
Limitations
Although our findings highlight key issues regarding access to early years support, as we used a convenience sample there is a potential risk of bias and therefore generalizability to all families of children with DD in the United Kingdom is limited. Participants were recruited primarily through third-sector DD organizations and social media. Consequently, families not in contact with these networks or social media platforms may be underrepresented in our sample. A few autism-focused charities supported recruitment, which may explain the high proportion of children with (suspected or diagnosed) autism in our sample. While the study included a diverse sample in relation to socioeconomic indicators, for example, income poverty (58.4% of participants, compared with 32% of U.K. households in 2020; Department for Work and Pensions, 2021) and unemployment (18.4% of participants, compared with 13.4% of U.K. households in 2021; ONS, 2021), there was an overrepresentation of White participants (N = 618, 91.8% of participants; compared with 86.0% of census) and underrepresentation of other ethnicity groups in our sample compared with population data for England and Wales (see above, Participants; ONS, 2018). Future research could address this by designing accessible studies (culturally, linguistically, etc.) and targeting recruitment to promote participation from families typically underrepresented in research. Despite these limitations, reasonable confidence can be placed in the descriptive statistics reported due to the large sample size (N = 673).
As our measurement of unmet need for EI supports was based on parental caregivers’ perspectives of “wanted support” from professionals they had not accessed, it is possible participants may not have known what support these professionals provide or if their family needed their support. However, it does provide insight into parental caregivers’ perspectives of unmet need for EI support which are part of the standard education, health, and social care system across the UK. While parental caregivers’ experiences and perceptions of access to EI are extremely informative, our study lacked perspectives of professionals and services within the EI system. However, similar findings have emerged in studies of professionals within the EI system. For example, in Mazurek et al. (2020), primary care providers reported their lack of knowledge and insufficient resources were barriers to the provision of support for families of children with DD.
Conclusion
This study provided critical information on access to various EI supports for families of children with suspected or diagnosed DD across the UK. Our findings clearly indicate access to support is not straightforward and there is variation in levels of access to various EI supports. Furthermore, there was significant unmet need for EI supports and several common barriers and facilitators of access perceived by families. We hope the findings of our study will help inform initiatives to improve access to EI supports for families of children with suspected or diagnosed DD across the UK, such as improving professionals’ engagement with this group, in addition to increasing their understanding of family needs and services that are available to support them.
Supplemental Material
sj-docx-1-jei-10.1177_10538151221083984 – Supplemental material for Families’ Access to Early Intervention and Supports for Children With Developmental Disabilities
Supplemental material, sj-docx-1-jei-10.1177_10538151221083984 for Families’ Access to Early Intervention and Supports for Children With Developmental Disabilities by Suzi J. Sapiets, Richard P. Hastings, Catherine Stanford and Vasiliki Totsika in Journal of Early Intervention
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Warwick Collaborative Postgraduate Research Scholarship, Cerebra, Mencap and Ambitious about Autism.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.