
Abstract
Mental health challenges among students remain a complex and widespread problem facing school leaders. Though schools are a front-line pathway for providing mental health services, many struggling youth are not receiving the professional help they need (Atkins, Hoagwood, Kutash, & Seidman, 2010; Findlay, 2017). Creative and collaborative solutions are needed to bridge the mental health gap. School leader support is essential to the successful implementation of mental health interventions (Forman, Olin, Hoagwood, Crowe, & Saka, 2009). This paper summarizes the novel approach taken by school and community leaders in one rural Ontario community who jointly piloted a school-based social worker (SBSW) role to support secondary schools in two districts. Interviews with five district leaders (four involved in designing the intervention and the SBSW who piloted the role) reveal conditions necessary for the pilot to take place, as well as leader involvement in setting up, supporting, monitoring the new role. Interviews highlighted multiple ways which the pilot improved student mental well-ness: one-on-one and group counselling sessions, charting fresh pathways networks of support available to students, creating a safe space for student and staff drop-ins, among other benefits to schools and stakeholders involved in the pilot. Results also detail three challenges leaders encountered along the way: stakeholder agreement, role clarity, and the temporary design of the role. Findings underscore how school-based social workers show promise in addressing rising mental health challenges.
Keywords
Introduction
Mental health challenges remain a serious, sometimes deadly, issue facing children and adolescents (Canadian Mental Health Associate, 2021; Mental Health Commission of Canada, 2021). One in ten youth are predicted to experience depression, and one in seven are predicted to experience suicidal ideation (Findlay, 2017). In Ontario, between 2006 and 2017, youth emergency department visits for anxiety and mood disorders spiked by 89% (Chiu et al., 2020). Many mental health challenges that youth are facing, especially panic and posttraumatic stress, have been exacerbated by the Covid-19 pandemic (Hill et al., 2021; Leeb et al., 2020). Schools are recognized as offering frontline opportunities to respond to youth mental health concerns due to the number of caring professionals accessible and services available (Atkins et al., 2010). Our paper shows that stemming the tide of mental health challenges recognized pre-pandemic and, on the rise post-pandemic, requires solutions that leverage a full complement of school and community support. Our data emphasize school leaders’ willingness to guide much needed collaborative and innovative solutions to respond to rising student mental health concerns.
Mental Health Need ‘Outstripping’ Supports
Most youth who receive support for mental health challenges typically access services through their schools (Substance Abuse and Mental Health Services Administration, 2020). The sheer scale of current mental health demands depletes resources schools have available to cultivate mental wellness (Atkins et al., 2010). Although schools are one of the most common entry points for youth to access services, most youth with mental health challenges are not receiving the professional help they need (e.g., Findlay, 2017). In Ontario, Canada, it is estimated that more than one third of adolescent students have an unmet need for mental health support (Boak et al., 2016). The results of one mental health survey conducted in 643 schools across Canada suggests that 80% of educational leaders feel the need to address unmet student mental health needs within their schools (School-Based Mental Health Substance Abuse Consortium, 2013). What is more, Canadian provincial Ministries of Education have recently increased funding to support student mental wellness. In 2019, Ontario’s Ministry of Education increased mental health support funds by $27 million annually over the next 10 years (Ontario Ministry of Health, 2019). Despite the infusion of funding and support from government-level directives, difficulties persist for youth with mental health challenges.
The Covid-19 pandemic has intensified some of these mental health challenges for youth. Studies have predicted increasing student experiences of stress and anxiety relating to Covid-19 (Orgiles et al., 2021; Xie et al., 2020). Impacts on youth mental health have “the potential to become a greater problem than the virus itself” (Harris & Jones, 2020, p. 243). The experiences of students returning to school in September 2020 in Alberta indicated that Covid-19 is recognized as a risk to health and social relationships, particularly for female students and older students who report higher negative affect and cognitive/attention scores on the Behavioral Concern Scales (Schwartz et al., 2021). School-based mental health professionals will be critical to support students in dealing with anxiety, social adjustment, and other unanticipated mental health concerns related to the Covid-19 pandemic (Weisbrot & Ryst, 2020). Leaders remain challenged to find pathways to youth mental health and well-being (MHWB) supports.
School-based Social Workers Bridging the Mental Health Service Gap
Having school-based social workers (SBSWs) is one potential way to address youth MHWB concerns. Initially, SBSWs acted as liaisons to connect students to community resources. Some districts have increased access into in-house support with additional SBSWs, as there has been a shift to recognizing the value of increased access and more comprehensive “wrap-around” services and programs to support more holistic MHWB for students and families (Ouellette et al., 2004). Sherman (2016) describes the current SBSW role as a “mental health practitioner” within schools (p. 148). SBSWs act in multiple capacities in supporting student MHWB. Providing front-line mental health support, such as crisis intervention, is seen as one of the biggest benefits of SBSWs (Bye et al., 2009). SBSWs also provide follow-up services, like one-on-one and group counselling (Allen-Meares et al., 2013). SBSWs can forge connections among students, families, school staff, and outside organizations (Berzin et al., 2011). In this way, SBSWs are in a prime position to match student needs with appropriate supports and following up with service pathways (Kelly et al., 2015). Further, given the many roles of SBSWs, they are uniquely positioned to stretch to address rising mental challenges by broadening their scope of practice across multiple levels of support to meet student needs (O’Brien et al., 2011).
Beyond providing day-to-day support to students, SBSWs take a leadership role in addressing rising mental health challenges. SBSWs have expertise in resolving complex needs through multiple channels of support, making them key voices in navigating the rise in mental health challenges (Sherman, 2016). Taking the lead to understand school-wide trends in MHWB and making recommendations to improve the mental health climate within schools are ways SBSWs leverage their experience (Hopson & Lawson, 2011). Improving collaboration between SBSWs and administration, as well as people in and outside of the school community, is a crucial step toward expanding SBSWs’ MHWB impact (Sherman, 2016).
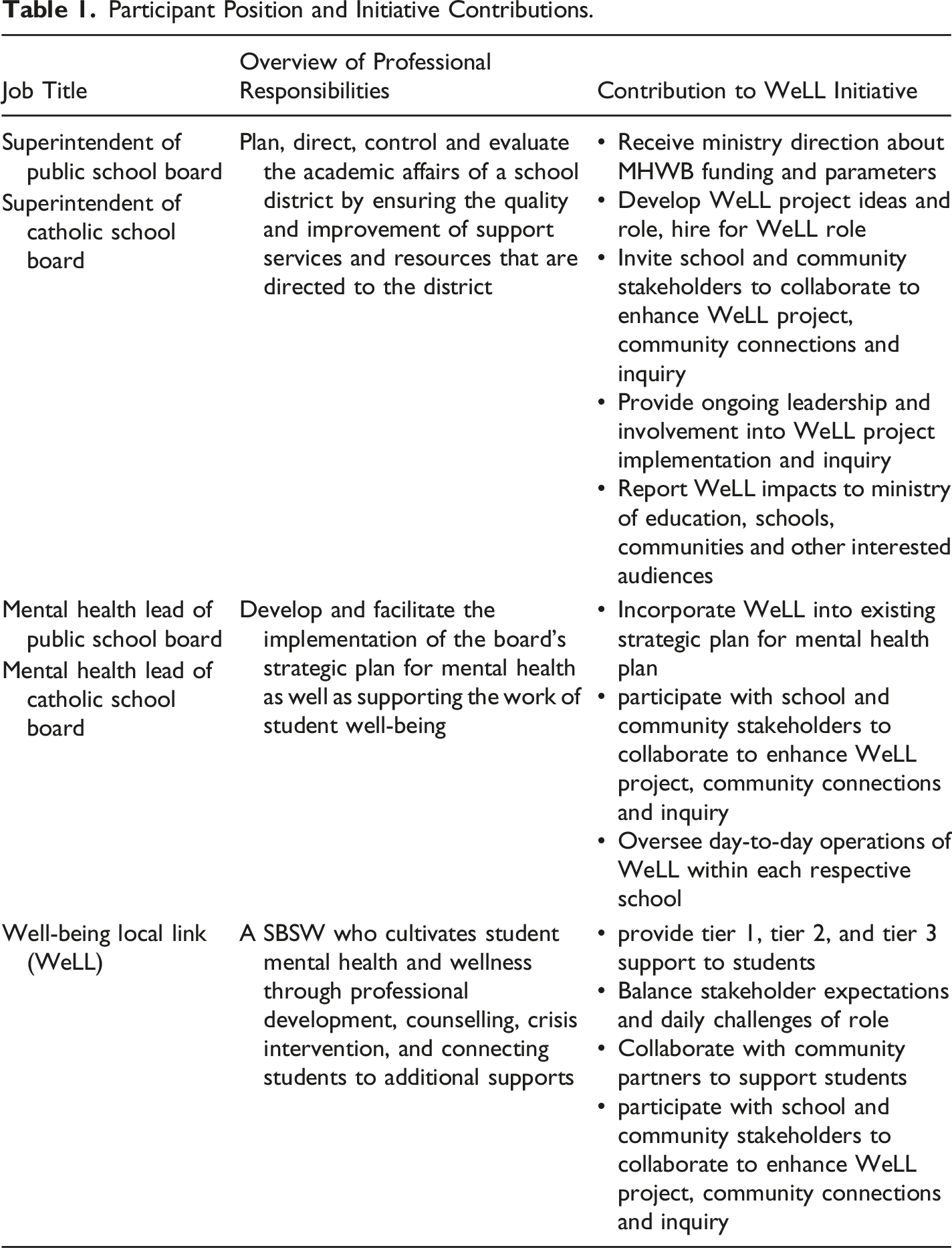
Participant Position and Initiative Contributions.
Literature Review
Principal and administrator support has been identified as essential to implementation of MHWB intervention (Forman et al., 2009; Langley et al., 2010). Beyond the rollout of the intervention, school leadership was viewed as a major factor in an intervention’s long-term sustainability or, if lacking, was positioned as a barrier to success. The centrality of school leadership in maximizing influence on teachers and students is well established (Huber & Muijs, 2010). Creating and maintaining processes for monitoring and sustaining mental health interventions is critical to the implementation of long-term interventions (Fazel et al., 2014). Additionally, developing and nurturing longstanding collaborations with community-based partners that are oriented to a shared wellness agenda grows available resources and caters to sustained impact (Andis et al., 2002; Webb, 2018). These multifaceted concepts operate within dynamic contexts and are worthy of examination.
Leader Support Vital to School Well-being
School leader ownership of supporting students’ MHWB is an essential starting point to cultivating positive mental health (Andis et al., 2002). Committed school leaders can foster improved student MHWB by participating in conversations on key issues and by seeking expert counsel to address mental challenges (Short, 2016). Evidence-based mental health interventions consider school leaders to be key champions of successful implementation (Forman et al., 2009). Their ongoing and visible involvement in MHWB is essential to embedding wellness into the “fabric of a school’s life” (Askell-Williams, 2017, p. 149).
Leveraging existing resources and prioritizing them around mental health needs is one step leaders can take to boost available resources (Atkins et al., 2010). Need continues to “outstrip” available school support, beckoning leaders to consider new partnerships that bring fresh resources to address student needs (Andis et al., 2002). Parents wonder whether schools will be adequately equipped to support the rise in mental health challenges as schools reopen after the Covid-19 pandemic (Fontenelle-Tereshchuk, 2021). Developing a shared vision with stakeholders is paramount to supporting mental well-being; community partners are often cited as key people in decision making (Andis et al., 2002). As research shows, schools are well positioned to pilot new, collaborative MHWB initiatives that leverage community resources and services (Caparelli, 2012). New partnerships can take many forms: other school districts; local community programs (Adelman & Taylor, 1999; Blank et al., 2012; Power, 2003); and linkages with university researchers (Hooper & Britnell, 2012). Leaders are encouraged to “map out” student needs, potential supports and then align community resources to wellness challenges (Atkins et al., 2010). Put simply, meeting complex youth mental health needs requires the “weaving together of school and community resources” (Adelman & Taylor, 1999, p. 158).
Collaboration Critical to Intervention Success
Community partnerships who provide care beyond the school setting are key to successfully implementing mental health interventions, and community organizations can be important champions for successful evidence-based mental health interventions (Mei et al., 2020). Counselling and therapy practices, healthcare centers, and case-management services are examples of wrap-around services (Burns & Hoagwood, 2002). Funding agencies, local businesses, mental health advocacy organizations, and cultural or religious centers can also act in a community capacity.
Forman et al. (2009) and Langley et al. (2010) interviewed school administrators who successfully or unsuccessfully implemented one such evidence-based mental health program, Cognitive Behavioral Intervention for Trauma in Schools (CBITS: Jaycox, 2004). Administrators who partnered with community-based agencies were more successful than those in schools that relied solely on school-based resources. MHWB initiatives flourish when services and organizations are brought together to cultivate positive wellness climates and address student mental health problems (School Mental Health-Assist, 2013). Researchers found the joint resources and expertise generated through school and community partnerships create the conditions to overcome implementation and monitoring challenges. Investigating research practice partnerships continues to be an important area for inquiry in educational research (Coburn et al., 2021; Wiens et al., 2020).
The Pilot in Review
In response to mounting MHWB challenges in rural southwestern Ontario leaders from a Catholic school board, public school board, and community non-profit convened in 2018 to address youth mental health challenges. Leaders decided to pilot and jointly fund a SBSW position, referred to here as the Well-Being Local Link (WeLL). 1 The WeLL initiative represented an expansion of current support and the first formalized collaboration between these partners. The role aimed to realize the value of employing a SBSW skillset and expertise to meet student MHWB needs.
Fostering mental wellness was central to the joint WeLL intervention school leaders designed. Multiple definitions of ‘mental wellness’ exist; drawing from the Canadian Mental Health Association’s (2021) conceptualization, school leaders settled on the following framework to ground the WeLL’s purpose: An emotional and psychological state of well-being in which students can realize their potential, cope with the normal stresses of life, work productively, and make a contribution to their community. The WeLL role was built around the School Mental Health Ontario (2023) three-tier service model. While some of the WeLL’s responsibilities would reach all students (i.e., tier 1), most responsibilities would serve students with significant mental health needs requiring additional or individualized support (i.e., tiers 2 and 3). Tier 1 supports can include the development and support of social-emotional learning (SEL) integration in the classroom, which affords students application of their skills in realistic contexts and interactions (Bobek, et al., 2021). Tiered MHWB programs are more likely to be effective when school and community partners work together as part of the system of care scaffolding universal supports (i.e., tier 1 supports), integration into the learning environment and targeted supportive structures (i.e., tier 2 and tier 3 supports) for connecting with the home environment (Clarke et al., 2021).
Context for WeLL Initiative
In 2018, the Ontario Ministry of Education directed funding for MHWB initiatives and required inquiry into the effectiveness of these initiatives. The external research team engaged in systematic inquiry throughout the role creation and first year of implementation to examine the impact of this new mental health worker role (the WeLL, filled by a SBSW). The WeLL initiative was jointly piloted by two rural school districts who share an overlapping geographical area. The WeLL role was created by school and community leaders to boost available mental health support to students. Both school districts serve rural agricultural communities and small towns with more than 30 elementary schools and more than two high schools per district. Each district includes approximately 2000 leaders, educators, and support staff. A variety of community-based mental health and wellness agencies exist in the district catchment areas. The leading addiction and mental health agency in the region has served over 2500 clients (citation removed to protect anonymity of the districts).
The creation of the role was aided by school-wide student survey data which alerted district leaders to increasing reports of depression, anxiety, and substance use. As a certified social worker with experience working with youth, the WeLL was initially provided with policy-focused orientation by district leaders and later received specific MHWB training to align with district initiatives. Additional guidance about implementing the role in school settings was provided by school leaders, in-school guidance counsellors, and other staff as needed.
From the outset, leaders set ambitious goals for the WeLL position. To highlight just a few of the responsibilities, the WeLL would respond to crises, provide ongoing counselling, devise professional development for staff, collaborate with school boards and community, and aid in facilitating the school boards’ mental health plans. Additionally, the person in the WeLL position, who was new to working in education, needed to be responsive to different contexts emerging across schools, school systems, and in a rural community.
The hiring of the WeLL role coincided with the start of the school year. School district leaders and the WeLL worked in the first few months to increase awareness about the new role and to establish pathways for student referrals. The WeLL position was split between two secondary schools, one in each district. The role supported students directly by developing caseloads and offering supports for each school concurrently. Students were referred to the WeLL by others (e.g., teachers, school leaders, parents), or could request an appointment directly. Teacher monitoring of student MHWB and referral to the WeLL were key, although district leaders also sought to encourage direct student access through announcements and classroom visits by the WeLL. Simultaneously, the district promoted the role to educators and the broader school communities through district communications. Over the school year, those involved in the role and role creation met monthly to discuss the implementation and monitoring.
To improve the likelihood of a successful pilot, school superintendents invited collaboration from community and school leaders (i.e., principals and vice principals). School leaders provided important context pertinent to tailoring the WeLL to meet unique mental health challenges and mesh within the school communities. Community members volunteered additional funding to monitor the success of the initiative and to reinforce connections to community MHWB services. District leaders leveraged an existing collaboration with an external team of educational researchers, the authors of this paper, to work with community to inquire into this new role. The external research team was comprised of five researchers from three universities guided by the principles outlined in Collaborative Approaches to Evaluation (Shulha et al., 2016). These principles directed the inquiry and were also used as a way to foster reflection during the inquiry. District leaders wanted to know to what extent a SBSW could enact a WeLL role to improve student MHWB services from within the schools as well as connecting students with surrounding community resources.
This paper explores the WeLL role and district-level school leaders’ perspectives of engaging in an innovative collaboration to support student MHWB. We focus on three key questions: (1) What is the utility of a SBSW in the WeLL role? (2) How does the WeLL role contribute to MHWB in the student population? (3) What are the facilitators and barriers to implementing this WeLL role? We draw from multiple sources generated throughout the inquiry including interviews with leaders held 1 year after the role was initiated. Data show that a collaborative leader-driven approach in piloting a SBSW role has promise to support complex student MHWB in schools.
Method
Stake’s (1995) qualitative case study methodology, as characterized by the study of a naturally occurring phenomenon, in this case the WeLL pilot, with a focus on depth and accuracy of information, namely to understand the leaders’ perspectives in regards to the three research questions, was employed. The unique features of the MHWB initiative, and the collaborative approach taken by the district leaders, the WeLL, community partners, and the external research team created an ideal setting for a clear and deep understanding of a real-world case (Yin & Davis, 2007). To tap into descriptive insights about intention, implementation, and influence of this initiative, we interviewed the program champions involved in the role (Forman et al., 2009). Ethical approval was obtained through the Research Ethics Board at [Unnamed] University.
Participants
As part of the qualitative case study methodology, the five program champions completed one-on-one semi-structured interviews with the external research team in June 2019. Participants included two school superintendents (one from each district), two mental health leads (one from each district), and the WeLL. Superintendents and mental health leads had significant experience in education, with more than 5 years working with the specified district and some of them having held multiple roles (e.g., teacher, school leader, program leader). Collectively, these participants offer a strategically rounded perspective about the initiative (see Table 1).
Instruments and Data Collection
We used the research questions as well as project implementation sources to develop a semi-structured interview guide to investigate leader perspectives (see Appendix A). We anticipated leaders were an excellent source of data to provide information about the WeLL role, inquiry and impact. Semi-structured interviews permitted us to gather open-ended perspectives around focused implementation inquiries, while also allowing us to probe nuances and particulars in real time (Patton, 2002). Questions focused on the impact of the WeLL role on different groups of people in the school and community and about supports and barriers to the implementation of the role. Interviewers recorded and kept detailed verbatim notes throughout the 45–60-minute interviews. Detailed researcher notes and transcriptions were used to support analysis. Follow up conversations with interviewees were held to gather additional data and to clarify understanding as needed. To situate the participants’ perspectives while protecting their anonymity, participants are referred to by their role throughout this paper.
We used work products created throughout the inquiry to strengthen our understanding of the participant perspectives and to expand on the ideas expressed by participants in their interviews. These work products included the inquiry plan, copies of all minutes from meeting notes, email communications with program champions, and two reports (an interim report and the summative report). Document review is a common starting point in educational research as a way of strengthening and supporting the research (Bowen, 2009). We used work products to chronologically revisit the inquiry process as part of conceptualizing this research, by looking for details pertinent to our research questions we systematically traced actions and learning about the WeLL role while identifying areas for further learning.
Data Analysis
Figure 1 provides an overview of the analysis process. Prior to analyzing the data, the inquiry work products, transcripts, and verbatim notes were read repeatedly by two coders to develop familiarity with the data (Burnard, 1991; Patton, 2002). Researcher notes capturing early impressions and potential codes and themes were recorded in document margins (Burnard, 1991). While reading data, coders created a non-exhaustive preliminary list of codes. The first coder (i.e., the first author) then consulted with a second coder (the fifth author) to compare earmarked statements, what codes seemed to repeat, and triangulate how emerging codes might point to larger themes. ATLAS.ti (2018) was used to identify significant statements about the process of role implementation through a deductive (i.e., codes agreed upon in consultation with the second coder) and emergent coding process. Open and “in vivo” codes were used for sections of transcripts that surpassed the scope of the coding framework discussed with the secondary coder (Creswell, 2013). Significant statements were then organized into salient sub-themes, which were then bundled into four overarching categories (Patton, 2002; Saldana, 2009). The results section is structured around the findings from this integrative process. Data Analysis Flow.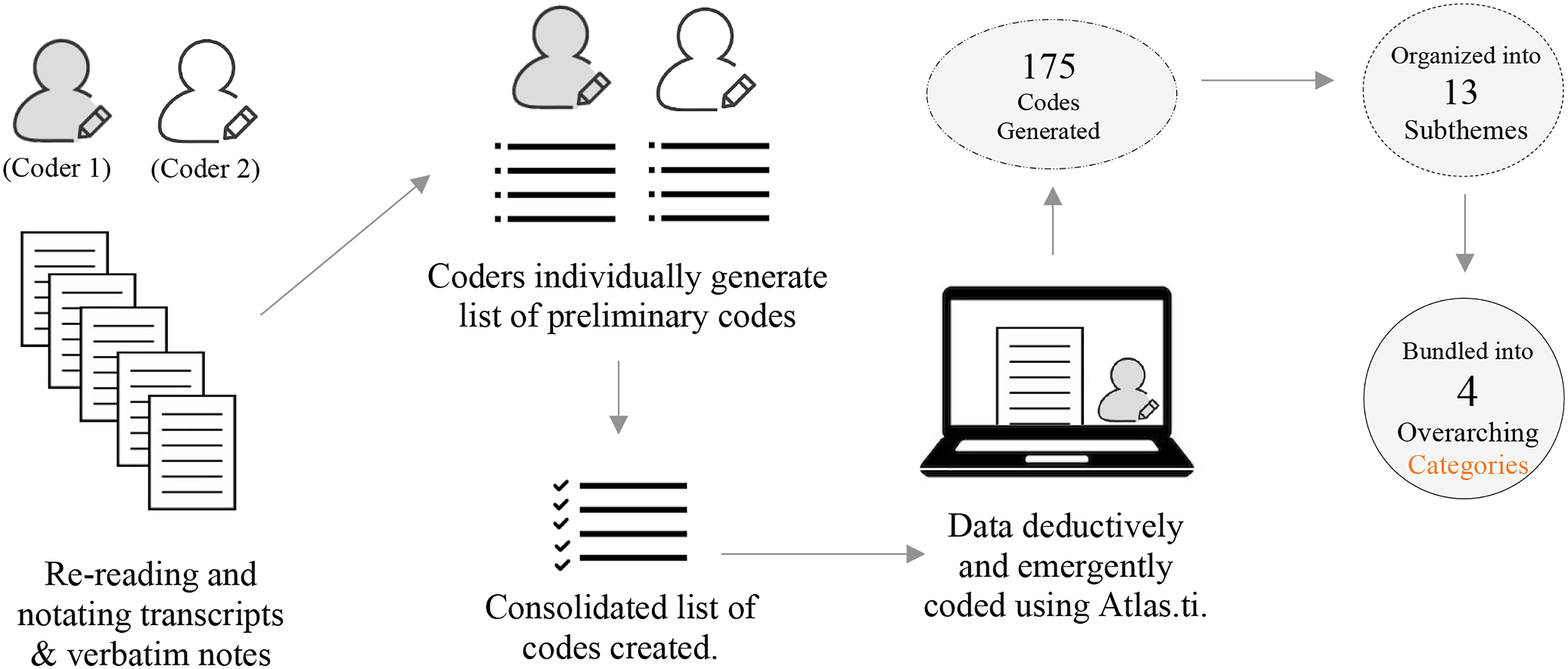
To ensure data collected was reported accurately throughout the inquiry and case study, work products created were reviewed in an iterative manner by program champions. Feedback provided to the research team was considered, and adjustments were made as needed. Throughout the individual interviews, clarification was sought to ensure information was being shared in an accurate manner. In the data analysis process, triangulation occurred through the coding of interviews (i.e., investigator triangulation) and through follow up conversations with the participants to promote credibility of the data (Stahl & King, 2020).
Results
Interviews with program champions yielded a rich understanding of a collaborative and innovative solution to pervasive mental health challenges. Four key findings emerged: leader involvement, benefits of the WeLL role, implementation challenges, and future considerations (see Figure 2). Framing these key findings around the three driving research questions of this work: Benefits of the WeLL role and future considerations address the utility of an SBSW in a WeLL role (i.e., question 1); benefits of the WeLL role also seek to understand how the WeLL role contributes to student MHWB (i.e., question 2); finally, leader involvement and implementation challenges explore facilitators and barriers to implementing the WeLL role (i.e., question 3). A Thematic Guide of Findings. Notes. This figure provides a visual framework for conceptualizing how key themes fit together. The right-pointing arrows denote the unfolding process of the WeLL role implementation. The plus signs inside the large arrow represent the increasing benefits on MHWB over the pilot. The dotted lines in the middle of the large arrow signify the disruptions, or challenges encountered during WeLL implementation. Since leaders’ efforts undergirded the pilot process, the leader involvement theme is visually placed underneath the overall process (i.e., larger arrow).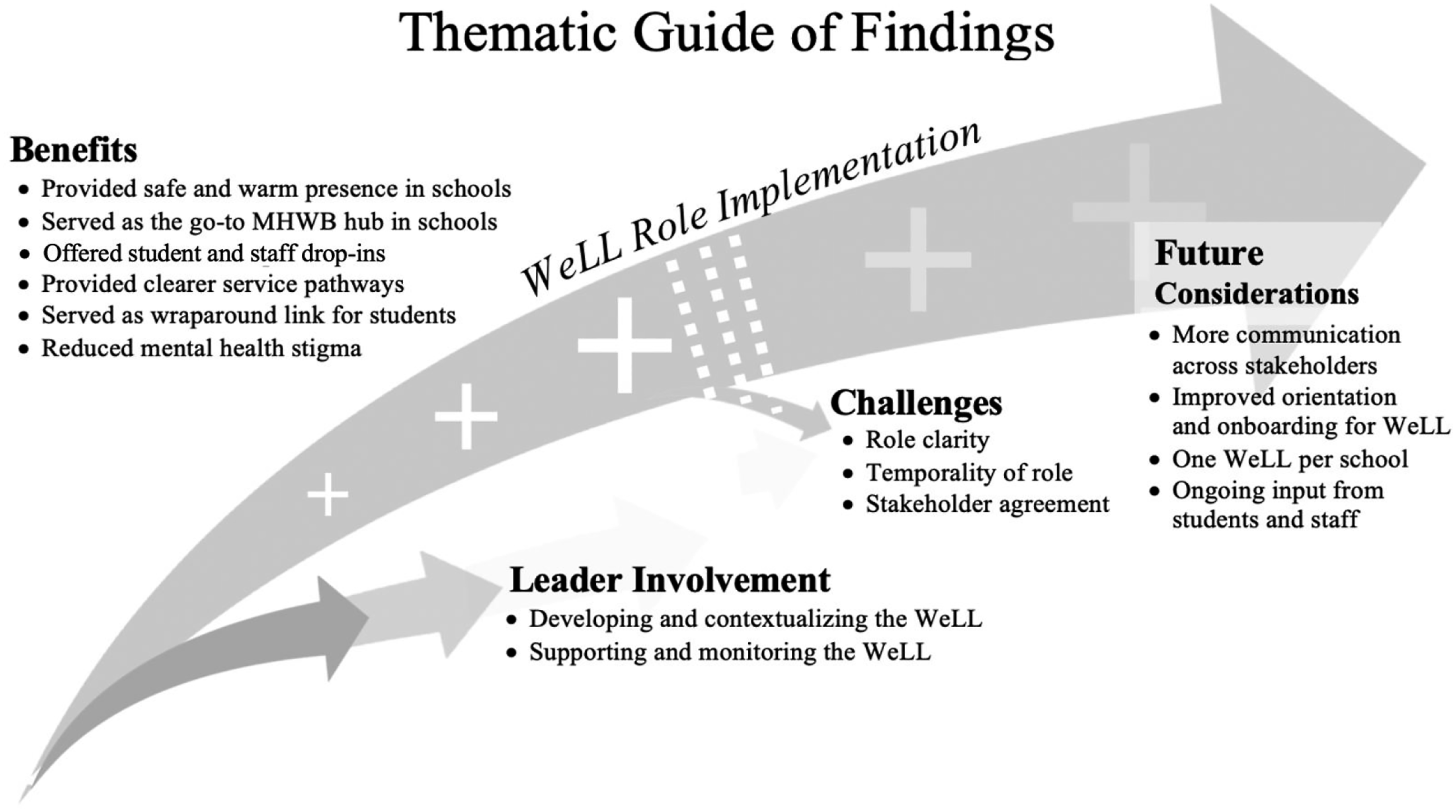
Leader involvement is addressed first to provide a backdrop and insight into the creation and implementation of the WeLL role. Next, the benefits to students, school, staff, and the broader school community are examined, followed by a review of the challenges encountered during role implementation. Finally, the next steps and goals regarding the future of student MHWB are considered.
Leader Involvement
School and district leaders involved with the WeLL role influence the implementation and mental health landscape through the mental wellness context, the set-up, supporting the WeLL role, and monitoring the role’s implementation.
Mental Wellness Context
The WeLL role was introduced as one part of the participating school districts’ broader mental health strategies. All interviewed leaders wanted to improve the mental health climate of the schools involved in this initiative by reducing the stigma of mental illness, prioritizing student crises, fostering belonging, and equipping students to respond to peer mental health problems. The external research team observed that the district leaders were focused on being responsive to the perceived needs of the students and others in the school environment. Superintendents also respected that school leaders already had a number of MHWB initiatives planned or underway in their school buildings and that the capacity for additional emphasis in this area needed to be carefully woven into the school environment. District leaders were eager to collaborate with an external research team to monitor the implementation of the newly created WeLL role and its efficacy in positively impacting student MHWB.
Prior to the WeLL role, the mental health leads annually convened a mental health fair of community supports for students and parents. Still, superintendents noticed that students needing targeted intensive or individualized care (i.e., tier 2 and 3 interventions) were not receiving the desired level of needed supports. One mental health lead likened the need for additional personnel inside the school to a stream: “Here’s the stream; who else is along that riverbank to support and build up the riverbank, build up, you know, shore up some of those resources so that there are fewer kids [heading downstream].” Prior to the start of the WeLL role, school and district leaders were well positioned to create a support that was responsive to student MHWB because they had a keen awareness of mental health problems facing students, access to additional funding resources, existing relationships to build from, and a shared vision for an inquiry that included the value of bringing in additional personnel to support student MHWB.
Set-up
Both superintendents and one mental health lead said that the timing of role implementation was “right” to create the WeLL role. The district had maintained an increased focus on wellness for some time so there were enough people involved to accept the risk and support the new role. Superintendents and one mental health lead also cited the benefit of working with the external team. When first conceptualizing the role, superintendents considered two key questions: what complex mental health and substance-use needs faced their community and how might a SBSW address those concerns? Mental health leads also saw the pilot’s MHWB focus as a path to promote academic achievement.
Over the course of multiple collaborative working sessions, leaders and the inquiry team reviewed district data from 5 years’ worth of MHWB surveys and a literature review of SBSWs’ responsibilities to draft a broad vision for the WeLL position. Evidence from meeting minutes shows that school and district leaders reflected on how the role would integrate with existing school staff and community networks. The layers of leadership engaged throughout the initiative show that leaders thought and acted strategically to leverage the benefits of a SBSW across schools, families, and community organizations. One mental health lead explained it this way: [I think about] support to the person in the role around navigating within the building, within the community, amongst people. . . I mean, clinically, I think about it as use of self; I mean, how do you use yourself strategically as a social worker in a school, clinically [for] the students but also in the team.
District leaders recognized the need for collaboration with community to strengthen the network of WeLL supports to operate cohesively for students. “In order to work together with people, we need opportunities to come together around a common purpose,” explained one mental health lead. District leaders identified several larger motivations for collaboration: rallying behind student wellness, building meaningful relationships, and shining a light on the broader mental health services available to students. At an early working session, community partners indicated their desire to strengthen school-based programming and create bridges to services outside of school. The collaborative approach provided opportunities to come together and build a network focused on student MHWB that might not otherwise have been assembled.
Supporting the WeLL Role
Leaders demonstrated ongoing involvement in supporting the new WeLL role throughout the pilot year. As one superintendent described, the WeLL was “intentionally onboarded” into school communities. One mental health lead described a two-fold approach to supporting the WeLL: “[It]’s really important to support the person in the role but also to support the implementation of the position.” Leaders oriented the newly hired WeLL to “the building, within the community, [and the] people” (mental health lead). One superintendent expressed how finding a “keen core group of engaged staff” was key to ushering in the new role. When program staff are supportive of a new role, they can act as program champions who assist with the implementation of the role and act as support for the person in the role. Leaders held regular check-ins to troubleshoot clinical and logistical issues. One mental health lead outlined her perspective on supporting the WeLL: “Let’s talk about cases, let’s talk about the work, let’s talk about how you see yourself in this position.” To further establish the WeLL role within participating schools, leaders communicated the role’s purpose and scope of practice to school personnel and community mental health resources. The final inquiry report noted that, in its first year, both the role and the person in the role required support from different levels of leadership to facilitate smooth transitions for members of each of the school communities as the role was implemented.
Monitoring Role Implementation
We used several ways to monitor the WeLL pilot as it was implemented: planning sessions, recordings of meeting minutes, sharing meeting summaries, interim and final initiative reports, and informal conversations with all participants. Leaders saw a multifaceted approach to ongoing reflection about the role as key to implementation. For example, one of the mental health leads interviewed commented, “I think [we need to] continu [e] to review. . . The feasibility of a position that’s spanned not just two schools but two boards. Looking at the benefits, looking at the challenges. . . In the view of what do we need to have in place to ensure success.”
Choosing to work with an external research team helped scaffold a process for meaningful reflection. In the words of one mental health lead, the reflective process “facilitated opportunities to think out loud about what we do, how we are doing it, and why we are doing it.” By maintaining regular communication with principals, community, superintendents, and mental health leads over the course of the pilot year, the external research team was able to flag emerging issues and bridge gaps in understanding among leaders. During several inquiry meetings, the research team provided leaders with a synthesis of WeLL progress and implementation challenges to consider and address. Leaders also listened to student voices regarding the WeLL’s impact on MHWB in the form of individual and collective arts-informed perspectives (e.g., students’ photographed, painted, written reflections). Feedback generated by ongoing inquiry activities including regular check-ins with the WeLL enabled leaders to make informed decisions around how the role fits within broader mental health strategies, what job responsibilities should be prioritized, and how to balance the role’s presence across schools and community sites.
Benefits of Role
The presence of the WeLL role, within the schools and for those involved in the collaboration, were identified through interviews as being particular benefits of the WeLL role. Each of the main groups benefited is explored in the following sections.
Within Schools
Over the course of the pilot year, the WeLL became a hub of mental health support to students. Mental health leads commented on the WeLL’s physical and warm presence as an important aspect of cultivating rapport and a sense of safety among students. Students were comfortable dropping in to converse with the WeLL about health-related issues, or even to talk about their day, without having an appointment. The WeLL conducted regular one-on-one and group counselling sessions for students with a range of mental health challenges. One superintendent explained that school staff initially saw the role’s primary focus as front-line support within schools. The WeLL described staff reliance on her when facing uncertainties regarding mental health needs: “[They] would say, ‘I have this student, I’m not quite sure what I should say or what I should do.’” Later on, staff realized the role had a wider scope and impact, including the reduction of mental health stigma and community connectedness.
The WeLL added a “deeper level of support for more complex needs” (superintendent) by making service pathways clearer to students while enhancing students’ access to mental health resources. This superintendent further commented, “There are more community service supports available than we realized.” Mental health leads mentioned multiple ways that the WeLL served as a wraparound service link for students: offering to place phone calls for students to community resources, keeping detailed case notes on which students were connected with what resources, and following up with community resources after a student accessed their services.
Overall, data from the inquiry process shows that staff valued the WeLL. One mental health lead explained, “The staff really have embraced having [her]…she’s one of them and they feel supported… They don’t want to lose her, for sure.” District leaders reported that staff found it was calming to have the WeLL present during difficult conversations about students. The WeLL recalled several challenging meetings where she kept the conversation focused on student needs. During the inquiry, one mental health lead noted that having a WeLL role made a difference in the overall levels of support available in the school. Similarly, one superintendent conveyed how easily the role liaised with school staff; several staff members even had regular drop-ins with the WeLL. The WeLL provided staff with updates on student well-being and offered timely strategies to support students: “I supported [staff] in their time of need so that they have a better capacity to feel more able to help [students] in a good way.” Guidance counsellors communicated to one mental health lead their sense of relief that the WeLL had become the go-to mental health resource in the school. One superintendent and a mental health lead attributed the success of role integration within school communities to the WeLL herself and her intentional effort to connect with staff. The WeLL and a mental health lead noticed an increase in school-wide motivation for supporting students since the start of the role.
Collaboration
One of the greatest benefits of role implementation cited by leaders was that it created a reason to meet with others involved with greater regularity. “We have never had the need to work closely together to support [each other] so, this year, we were in more frequent contact around that,” expressed one mental health lead. Including the WeLL at meetings added a holistic frame to think about student wellness from a social worker perspective. During meetings, partners had more “opportunities to learn about each other that they normally would not have” (mental health lead). Community-based partners learned more about the complexities of the education system. From working with community agencies and social workers (i.e., people with a master’s degree in social work [MSW]), we learned some of the challenges faced and overcome in creating referral processes, following up with students, and receiving consent. Despite the logistical challenges in collaborating, one mental health lead reported greater motivation to work together in the future.
Challenges
In addition to the benefits of the WeLL role, challenges existed. The most prominent challenges were obtaining agreement, role clarity, and coping with the temporary nature of the role.
Leader Agreement
Interviewed leaders said the biggest challenge to WeLL implementation was determining and communicating the direction of the role. One mental health lead described the ambitious role design: “The position initially was sort of this big vision of what somebody in this role could maybe do and what this role could do.” During the role creation and implementation processes, those involved held competing expectations for role execution. The WeLL’s feedback about how the position was unfolding was seen by one leader as an additional challenge: “There was a bit of a rub with someone new coming into our world and someone telling us what we are doing wrong.” Sharing the role between two school districts that lacked collaborative infrastructure further complicated role development. One mental health lead put it this way, “You get [competing expectations] between two schools but that may be potentially more pronounced between two boards.” The WeLL called attention to another layer of role shaping tension, culture: “Not only [are] the cultures of the two schools different, the culture of the two boards are different, [which] adds a complicating factor.”
Role Clarity
Early on in the role, the WeLL quickly found herself balancing the day-to-day needs of students with leader expectations. Because multiple people oversaw role implementation, it was difficult for the WeLL to obtain quick feedback about role priorities: “It’s harder for me to actually do [anything] without everyone accepting that’s happening.” One superintendent estimated that it took about 4 months to establish the WeLL role. Despite regular check-ins with mental health leads and multiple meetings, the WeLL reported inconsistent messaging: “In my opinion, the job hasn’t become more clear as we went on...what is my silo, so to speak? Like, what do I do, what can I do, and where does that end?” One superintendent echoed this concern, explaining how the WeLL’s role raised practical questions about existing caseloads at schools and the responsibilities of other staff who also support mental health. Mental health leads cited referral processes and crisis procedures as areas needing to be updated to include the new role.
Temporary Nature of the Role
Because the WeLL role was a pilot initiative, school communities were unclear how long the WeLL would be present. Students reported to one mental health lead that recent educational cuts have them questioning what supports will be available to them in upcoming semesters, which impacted the extent to which students felt comfortable building relationships with the WeLL: “We didn’t know until [the second semester], if [the WeLL] would survive…Students really are aware of the educational cuts…[no one knows] how that’s all going to fall out.” One superintendent said the prospect of a new SBSW in the WeLL role would be a big hurdle for student mental health: “[The WeLL] leaving will be a step backwards, a detour that will effect [existing supports]; rebuilding will be needed.”
Future Considerations
Leaders acknowledged the need for improved role clarity and communication with the WeLL. For one mental health lead, a next step is revisiting the vision and description for the role. Streamlining the goals, plans, and tasks of the role were listed by the WeLL as necessary to facilitate working across two school boards. From the WeLL’s perspective, role agreement between superintendents and principals is imperative before hiring a new WeLL or other MHWB support staff: “Who decides what I get to do? Do the principals get to decide, or is it upper management? There are very different directions from all [around] what my time use should be.” One superintendent thought the role was too complicated for two boards to handle at once: “One WeLL between two boards likely won’t continue, it’s too complex.” They recommended the WeLL be housed in one district, at one school. Regardless of whether the role is full- or part-time in their district, the other superintendent expressed a desire to be more active in onboarding future WeLL roles in schools. One mental health lead thought that hiring a manager to oversee the logistics of the position might optimize the WeLL’s presence: “Other places have a manager to upkeep [case infrastructure], like when files come in.” The WeLL emphasized drawing boundaries around the role’s involvement with student affairs as a key next step: “[Setting] clear expectations, clear guidelines [around] what they want this role to be. Making sure that [I’m] the best person to be taking on that [need].” Specifically, the WeLL cited not getting pulled into conversations around discipline as a necessary boundary, which could compromise critical rapport that facilitates access to services: “I want to make it so [students] can still reach out to me if they need to.” In addition to shaping the WeLL or other future SBSW roles, one superintendent expressed a desire to leverage the momentum sparked by the pilot. Specifically, they want to grow mental health supports by creating mental health teams that would include both students and staff. These teams would have three goals: promoting connectedness among the school community, breaking down mental health stigma, and gathering student voices around MHWB.
Discussion
Creating the WeLL role showcased how schools, districts, and researchers collaborate to assemble the leadership and resources that boost wellness supports to address complex mental health issues (Atkins et al., 2010). Leaders agreed that the WeLL improved mental health supports for students. Echoing the success of other multi-tiered mental health school supports, the WeLL underscored how SBSWs are valuable for “establish [ing] a continuum of mental health services for students” (Marsh & Mathur, 2020, p. 71). Students received front-line supports for mental health challenges (e.g., drop-in accessibility, counselling sessions, advocacy during difficult meetings) and accessed a wider array of resources (i.e., wrap-around supports) made visible by the WeLL’s guidance (Kelly et al., 2015). These findings show that SBSWs possess key skills that school communities might otherwise be lacking (e.g., Berzin et al., 2011). To be sure, the WeLL did not fulfill every capacity initially envisioned for the role. The WeLL role did enable a cross-district collaboration that strengthened MHWB supports and positioned districts with evidence to support re-imagining of roles for SBSWs.
Leaders expressed strong support for funding the WeLL for another year: “[the WeLL] really enhanced legitimacy for a social worker mental health position in [our] school” (mental health lead). Noting its overall success, one mental health lead saw opportunities to create similar roles in other schools: “I see [potential] spin-off to the development and implementation of other roles, either in another school, be it secondary or even at the elementary level, as we continue to imagine what a mental health service delivery model might look like.” Honing a SBSW’s skillsets to one school community keeps workload in balance and increases the focus and multi-tier impact of interventions (Kelly et al., 2015).
In concert with leader-supported intervention literature (Forman et al., 2009; Langley et al., 2010), the WeLL role would not have happened without the buy-in and support of school- and community-based leaders. Leaders attributed working through a formal inquiry process as a valuable way to manage difficult conversations. With no single person available to provide immediate role clarity, decisions during the implementation were sometimes inconsistent and unclear. The inquiry provided a structured opportunity for leaders to come together early, conceptualize the WeLL role, ask specific questions about its implementation, and identify learning from other SBSWs, which leaders reported may not have happened in the same way without the inquiry.
The pilot demonstrated swift uptake by participating schools. Staff were relieved to have access to a dedicated school-based mental health resource; demand for student services quickly filled the WeLL’s caseload. Overburdening SBSWs with responsibilities continues to be a major hurdle for advancing MHWB programs in schools (Teasley, 2018). To support the supervision of caseloads, the WeLL advised, “Clear communication around the purpose of the role [and] ongoing support are really important.” Designing and shaping the role to meet the needs of those involved from two school districts and outside community organizations was the chief obstacle. Communicating ambitious role expectations, understanding the range of school climates, and handling daily complex MHWB challenges at each school generated a misalignment between the role vision and day-to-day practice (Sherman, 2016). True to the experience of other SBSWs with newly assigned roles, the WeLL’s responsibilities shifted with the demands of the school community (Phillippo et al., 2017). The pilot was a catalyst for discussions on MHWB. Additionally, the pilot represents an important cross-district and community collaboration which can be established as an ongoing effort.
Implications for Research and Practice
By gathering varied perspectives, this study provides a glimpse into the benefits and possibilities of leveraging the skill sets of a SBSW. A limitation is the small group of participants. Richer insights await if more perspectives from local school leadership, such as principals, administration, staff, and community are added. Additionally, future research with an established SBSW role, with defined and manageable expectations could offer more insight into the benefits and challenges associated with the ways in which the role operates in a school-based setting and its impact on student MHWB. Due to the early stage in implementation of the WeLL role, these questions were outside the scope of this inquiry. In this inquiry, hearing from the program champions behind the WeLL pilot frame a good starting point for understanding the embedded supports and challenges that are a part of implementing a novel MHWB support in schools. “We have not done enough with helping kids. . .We have to do more” (superintendent). In other words, the WeLL moved the needle of student wellness, but leaders are committed to making greater strides in meeting mental health challenges. “[This is just the] beginning of our conversation around mental health” (superintendent).
For those who want to start a conversation around improving mental health in schools and create a role similar to the WeLL, interviewed leaders’ reflections offer a window into district-level and school-level steps to be taken. As seen through this pilot, district leadership play a pivotal role in onboarding community and school involvement to support, take on risks, and shape the vision. Although collaborating between districts aided in bringing together the necessary resources together to pilot the WeLL, developing such a role within one school, or at least within one district, is advised. Preceding or concurrent to assembling partners, there is an opportunity at the school level to assemble a mental health team, comprised of students and staff, to identify MHWB challenges and provide perspective on how a new role might fill gaps in services. Incorporating district and school leaders in the onboarding of a newly created role will help with apt acclamation of a new role and swift role uptake within a school community. To maximize role impact while ensuring role clarity, consider appointing someone within a school to manage the day-to-day logistics of the SBSW role, creating a direct collaborative channel between the role and district leaders (Sherman, 2016), and scaffolding a formal inquiry process to monitor and advance progress. Given the unique mental health climate and demographics inherent to each school, it is expected that novel SBSWs roles will take on a unique subset of responsibilities, some similar and others different to the WeLL. The suggestions noted through this section — embedding SBSWs in single schools or districts, establishing a team for MHWB, onboarding SBSWs in meaningful ways, and delegating some of the associated administrative work — would also be important considerations in the scaling up of similar initiatives (e.g., to district-wide supports).
Concluding Thoughts
School leaders can still make progress towards addressing student MHWB needs even without taking steps to create a role like the WeLL. The results of this study show that advancing three points of view, each a distillation from interviewed leaders’ insights, can improve mental health outcomes in schools. First, understanding the need for agility in responding to mental health challenges is paramount. One key to unlocking agile solutions is leader understanding that appropriate MHWB responses change according to time, context, and student need. Second, leaders must also adopt an openness and a willingness to take risks to support novel approaches. Partnerships with community agencies offer opportunities for MHWB support that may go beyond those that can be organized, staffed, or funded by school districts themselves. Finally, maintaining a longitudinal approach to mental wellness allows leaders to align interventions undertaken with overriding objectives. For example, leader recognition that impacts of MHWB supports exist in the short-, medium-, and long-term frame expectations and next steps; while some benefits may be realized quickly, others may take significant time and energy to be realized. Together, these perspectives will help school leaders navigate complex mental health challenges and better support student well-being.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.