
Abstract
Background
Health professionals living with disabilities are valuable to healthcare due to their dual identity as a clinician and a person living with disability yet remain underrepresented in the workforce. While the barriers to inclusion of clinicians living with disabilities from their own perspective are reported, little is known about peers’ perspectives.
Objective
This study aims to explore the barriers and gaps in knowledge to the inclusion of clinicians living with disabilities from the perspective of colleagues.
Methods
Health professionals and staff (healthcare workers) in a public health authority in Canada responded to a survey consisting of closed and open questions, under 3 subthemes: attitudes, institutional barriers, and gaps in knowledge. Inferential statistics were performed to assess the overall attitudes and differences in perceptions based on types of disability.
Results
Attitudes and barriers varied based on type of disability - clinicians living with physical disabilities were perceived most positively compared to those living with cognitive/learning disabilities. Attitudes also varied based on experience with disability - clinicians with lived experience had more positive attitudes. Gaps in knowledge were found to exist on an individual and organizational level.
Conclusion
The results of this study can open the discussion for rehabilitation and human resource professionals needing to learn about workplace accommodations for health professionals living with disabilities and support addressing attitudes and barriers they face.
Introduction
Individuals living with disabilities represent 20% of Canada's working-age population (Statistics Canada, 2017) but remain underrepresented in most healthcare professions (Bulk et al., 2017; Human Resources and Skills Development Canada, 2010; Nouri et al., 2021). In one exception, a recent report focusing on physicians found that 22% of the participants self-reported living with a disability (Canadian Physician Health Survey, 2021). Work provides individuals living with disabilities a meaningful occupation with numerous benefits, such as improved quality of life and the formation of new relationships (Kocman et al., 2017). It is critical that people living with disabilities are included in healthcare professions not only to provide them with such opportunities, but to ensure the workforce accurately portrays the general population (Bulk et al., 2017). Furthermore, clinicians living with disabilities have a dual identity which provides a unique perspective and has the potential to remove existing attitudinal and organizational barriers (Battalova et al., 2020; Bevan, 2013).
The existing literature on the employment of people living with disabilities is predominantly focused on employment in general sectors of work such as hospitality, trades, and the private sector. Several barriers have been identified in the employment of people living with disabilities including attitudes, organizational practices, and lack of knowledge (Erickson et al., 2013; Nota et al., 2014; Piramanayagam & Seal, 2020). Attitudinal barriers include inaccurate perceptions of the individual's work capabilities and fear of negative perceptions by coworkers and/or clients (Breen et al., 2019; Ju et al., 2013); institutional barriers include legal, financial, and accessibility concerns (Breen et al., 2019; Kocman et al., 2017); and gaps in knowledge include lack of training and/or education in how to facilitate inclusion of individuals living with disabilities in the workplace in addition to suggestions for future steps for such inclusion (Erickson et al., 2013; McDonnall et al., 2014; McDonough et al., 2021). There is limited literature on the specific experience of clinicians living with disabilities, although existing research highlights similar barriers such as negative attitudes from their colleagues and employers, stigma, and devaluation (Bulk et al., 2017; Chacala et al., 2014).
Healthcare workers add a unique perspective to existing literature in having lived experience engaging with individuals living with disabilities and in the benefits to hiring them. In general, employers’ attitudes have been found to differ depending on the individual's type of disability and the employer's previous experience with disability (Andersson et al., 2015; Ju et al., 2013; Kocman et al., 2017; Nota et al., 2014). While healthcare professionals report some discomfort and lack of knowledge in working with individuals living with disabilities, they are shown to develop more positive attitudes than non-healthcare professionals, and the more experience they have working with individuals living with disabilities the more positive attitudes they develop (Satchidanand et al., 2012). Thus, the perceived barriers of colleagues/peers in the healthcare field may add new insight to the existing literature on non-healthcare professions. While research has explored the personal experience of clinicians living with disabilities, there is a literature gap in the employers’ and employes’ perspectives of the barriers to their employment. Due to this gap, it is critical to explore these barriers to educate employers and clinicians, and to create a foundation in which change can be created so that clinicians living with disabilities are no longer underrepresented in the healthcare workforce.
Objective
This study explored barriers and gaps in knowledge of accommodation practices for including healthcare workers living with disabilities from peers’ perspectives. The common barriers and gaps in knowledge identified will allow recommendations for programs or policies to increase the inclusion of clinicians living with disabilities. The following questions were addressed:
What are the overall attitudes toward the employment of clinicians living with disabilities from their peers’ perspective? Will attitudes and barriers toward the employment of clinicians living with disabilities differ based on perceived type of disability? Will attitudes and barriers toward the employment of clinicians living with disabilities vary based on experience or knowledge of working with people living with disabilities?
Methods
Sample Size and Participant Recruitment
A causal-comparative quantitative research design was utilized to better understand and describe current practices in employing clinicians living with disability. The study (H21-02479) was approved by the University of British Columbia's Behavioral Research Ethics Board. Healthcare workers working within various British Columbian (B.C.) health authorities were recruited for this study. Participants were included if they were working as a regulated healthcare employer within the provincial health authorities and had at least one year's experience in their current role. 141 employes working within the provincial health authorities participated in this study. The study's principal investigator contacted various superspreaders (i.e., managers and unions) in three the provincial health authorities - Vancouver Coastal Health, Island Health, and Northern Health - and provided them with the study information. The superspreaders then emailed all prospective candidates the study information including the inclusion and exclusion criteria, purpose of the study, a detailed description on participation in the study, and contact information of the co-investigators should they wish to participate. In addition, a newsletter was sent out within the participating health authorities to the Internal News Page.
Assessment Tools and Data Collection
The informed consent form was provided to participants at the beginning of the survey (via a hyperlink), and consent was confirmed at completion of the survey (via confirmation of survey submission). An online Qualtrics survey was developed based on the literature review. The study utilized pre-existing research tools that were used to explore employers’ perspectives in hiring individuals living with disabilities in general sectors of work (Breen et al., 2019; Erickson et al., 2013; Kocman et al., 2017; Nota et al., 2014), and the researchers modified the questions to fit the target population of clinicians living with disabilities. Some questions in the survey asked participants to distinguish between clinicians living with a physical, mental, or cognitive/learning disability (Andersson et al., 2015; Ju et al., 2013; Kocman et al., 2017; Nota et al., 2014).
The survey was composed of six-point Likert scales and written responses to allow participants to elaborate further. It included 4 subsections covering demographics, attitudes, institutional barriers, and gaps in knowledge.
Demographics. The survey asked for basic information such as age, gender, and ethnicity. Additionally, participants were asked about their professional background including their roles, the settings where they work, and their experience with clinicians with disabilities.
Attitude. In this section, the survey measures participants’ perceptions of working with someone living with disability. Participants were asked to rate on a 6-point scale to what extent they agree on 7 statements presented where 1 point is “strongly disagree,” and 6 is “strongly agree.” Some statements include willingness to work with someone living with disability, their ability to work, and potential benefits and drawbacks. The three types of disability are asked separately for each statement.
Barriers. The survey asks participants to rate how they think each different barrier impact the employment of clinicians living with physical, mental, and cognitive disabilities. Each question is asked on a 6-point Likert scale ranging from “very unlikely” worth 1 point to “very likely” worth 6 points.
Knowledge. The knowledge section has two parts, asking participants what they currently know and what they want to learn. First, participants were asked if their workplace has certain services or programs for clinicians living with disabilities. Participants were given the options of “yes, my workplace has this service”, “no, my workplace does not have this service”, or “unsure”. A response of “unsure” is worth 0 points as it is an indication of no knowledge while “yes” and “no” are both worth 1 point. Then the participants were asked if they want to receive certain training on supporting clinicians living with disabilities. The response options are “yes,” “no,” and “already received”. A response of “no” is worth 0 point indicating no interest in learning while “yes” and “already received” are both worth 1 point indicating interest or having taken actions to learn more.
Procedure
Participants received a recruitment letter which included an introduction to the study purpose, a detailed description of participation in the study, and confidentiality methods. In addition to the link to the informed consent form and the 30-min Qualtrics survey, contact information for the co-investigators was included in the email to provide opportunities to ask additional questions. At the end of the survey, participants were given the option to request the final report. Email reminders were sent out one and two weeks after, and the survey was open for 120 days (about 4 months).
Data Analysis
Like previous research (Breen et al., 2019, Nota et al., 2014), descriptive statistics were used to describe the characteristics of the study population (frequency and percentage) and to summarize the survey data (mean and standard deviation) using SPSS.
Questionnaire Scores Calculations
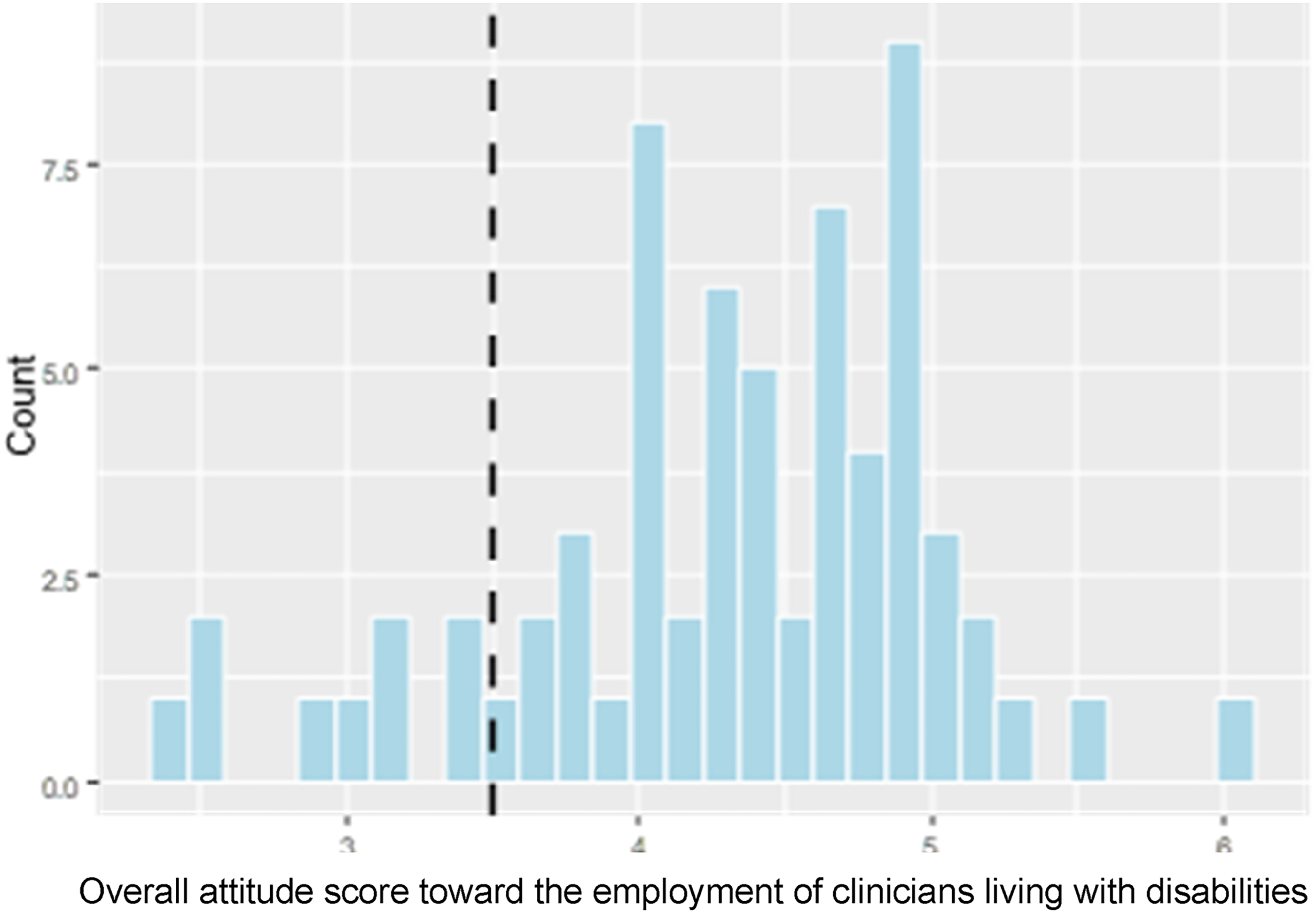
Each participant's overall attitude was calculated by averaging the points on all questions. A separate score for each of the three types of disability was also calculated using the corresponding questions. A score of 3.5 indicates a person has a neutral attitude towards clinicians living with disabilities. A score higher than 3.5 indicates a positive attitude, while a lower score indicates a negative attitude. The distribution of the overall attitude as well as for each subtype is negatively skewed. In this context, the peak of the responses is between 4 and 5 instead of 3.5, the mean of the 6-point scale, as shown in Figure 1.
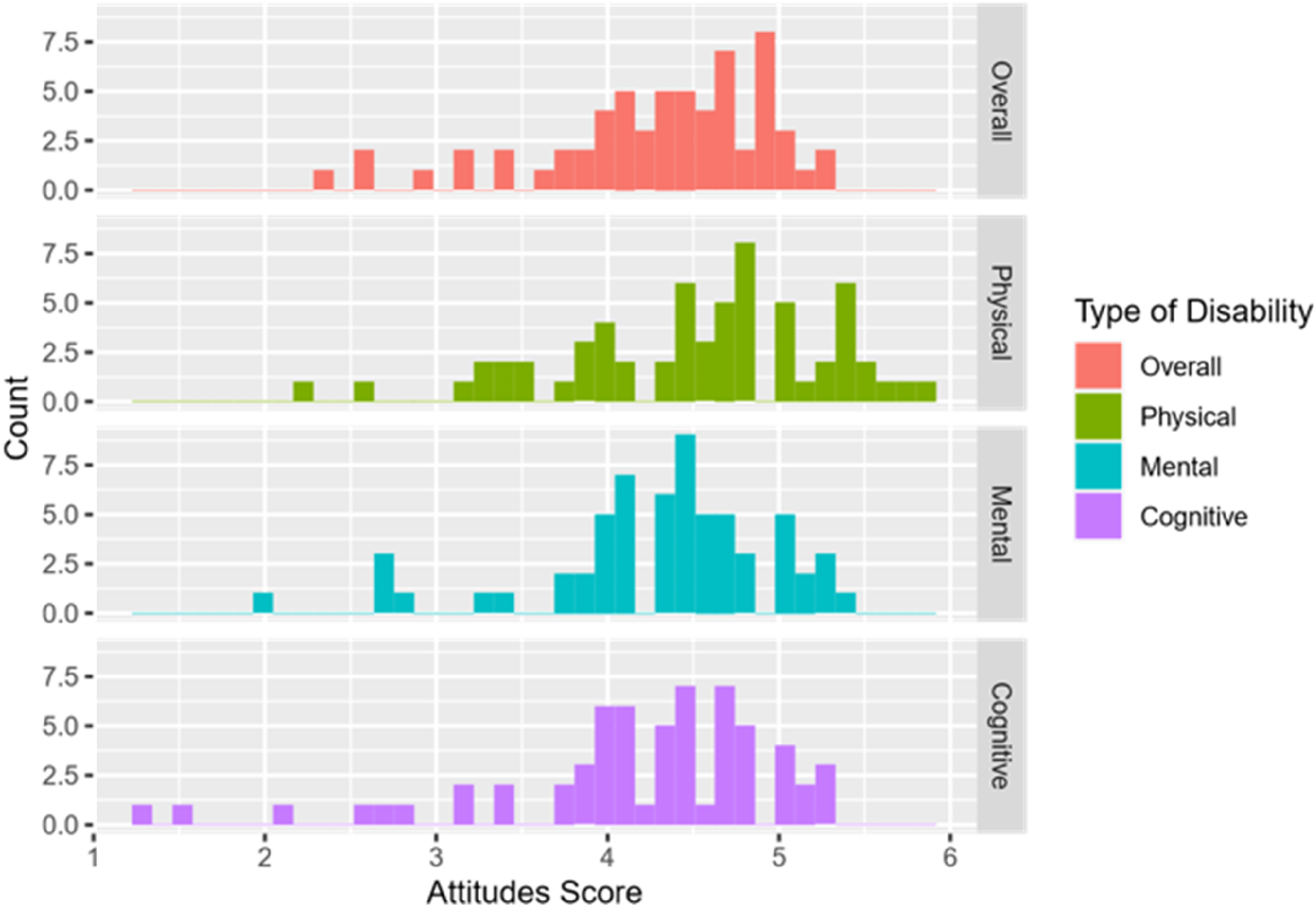
Histogram Showing the Distributions of Attitude Scores for the Employment of Clinicians Living with Different Types of Disability.
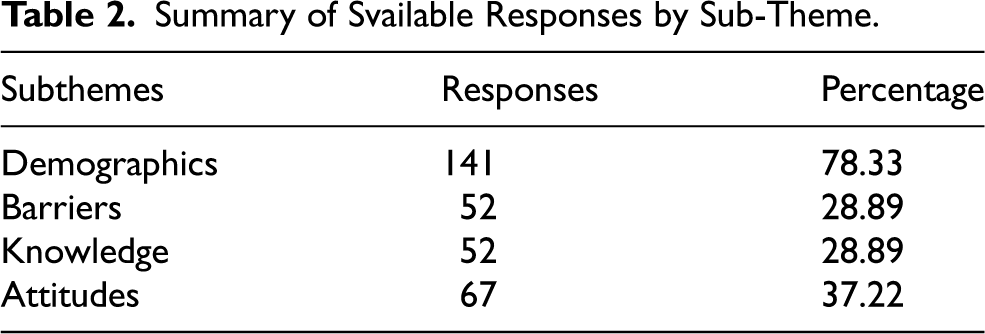
A score of the overall barriers perceived by each participant was calculated by averaging the points on all 15 questions. A separate score for each of the three types of disability was also calculated. The distribution of the overall barriers and for each subtype is negatively skewed (see Figure 2). A total score is calculated for each part of the knowledge section. The maximum score is 6 on knowledge known and 9 on knowledge wanted. Fifty-two responses were collected for this section and the summary is seen in Table 1.
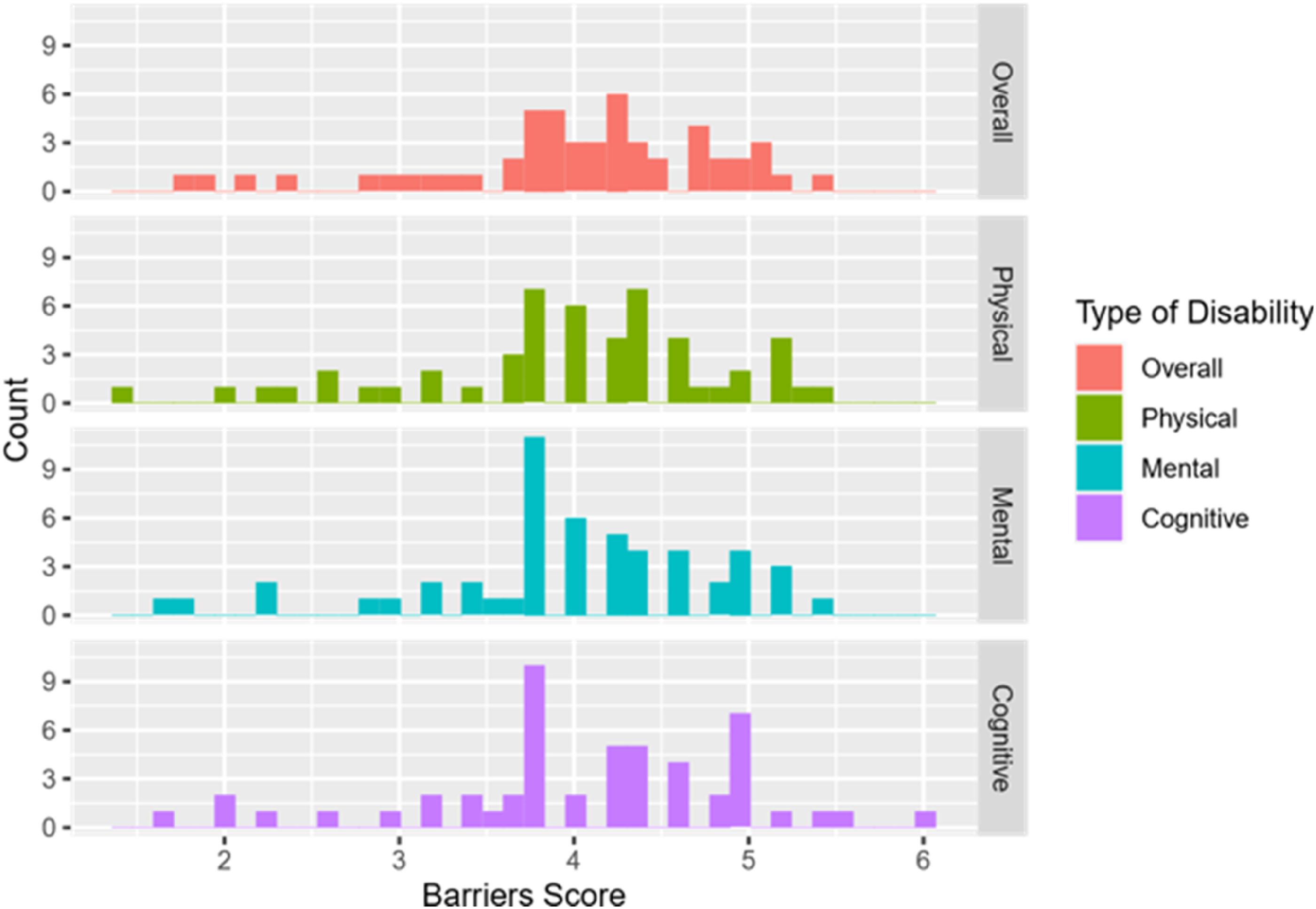
Histogram Shows the Distributions of Barriers Score for the Employment of Clinicians Living with Different Types of Disability.
Sociodemographic Characteristics of Participants.
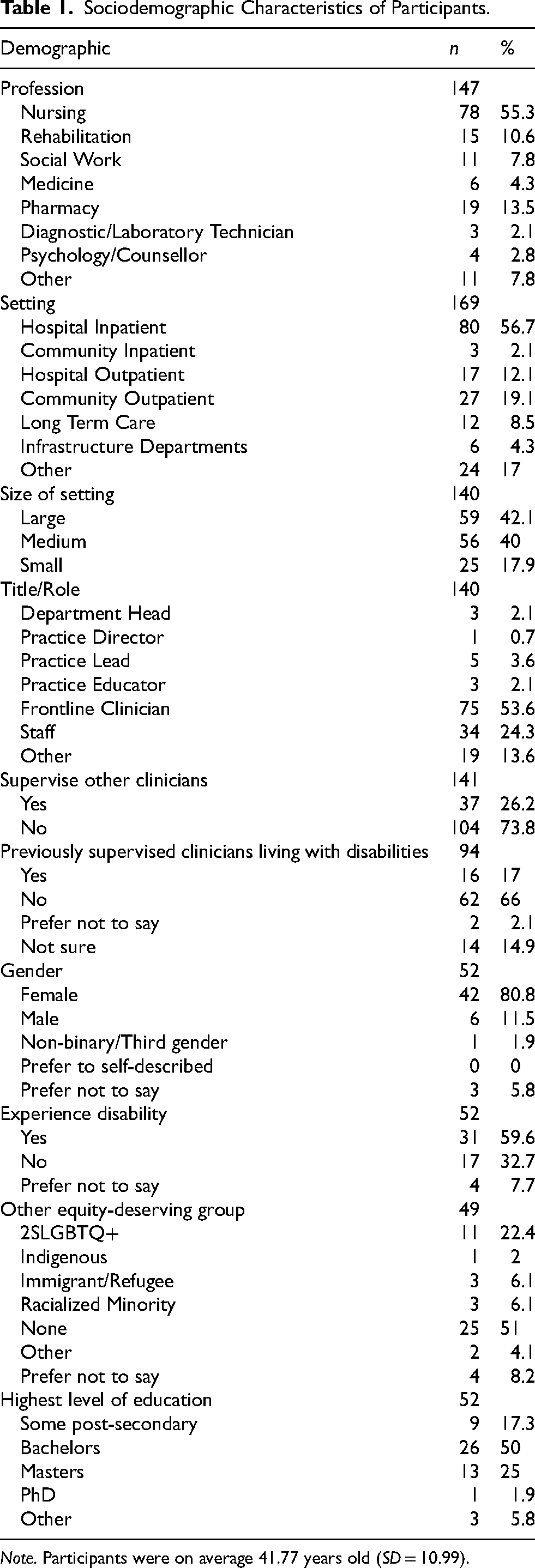
Note. Participants were on average 41.77 years old (SD = 10.99).
Inferential Statistical Analysis
To investigate the 1st hypothesis, the overall attitudes and perceived barriers held by healthcare professionals toward clinicians living with disabilities, a one-sample sign test was performed on the variable of overall attitude and barriers score.
To investigate the 2nd hypothesis: If different types of disability can result in different attitudes toward and perceived barriers to the employment of clinicians living with disabilities a nonparametric Friedman test was used as the distributions of both attitudes and barrier scores towards the three types of disability were not normal (Figures 1 and 2). A post-hoc analysis using the Nemenyi test followed to see if any significant differences between the three types of disability were identified from the Friedman test above.
To investigate the 3rd hypothesis, multiple linear regression was used to see whether attitude and barriers scores each would vary based on knowledge of working with people living with disability. The overall attitude and barriers scores is each regressed against knowledge one currently knows and knowledge one wants to know. In addition, correlations between attitude scores and knowledge scores and between barriers scores and knowledge scores were calculated respectively. A log transformation was performed on both attitude and barriers scores as both data were skewed. Unless specified, all tests use the critical level of 0.05.
Results
Demographics Characteristics
Of those who responded, participants’ age ranged from 24 to 68 with a mean of 43.5 years old. 60.60% identified their title/role as either a front-line clinician or staff member (Table 1). Participants were employed in various healthcare professions, with 53.10% in nursing. 59.60% of participants identified as experiencing disability. Of the 141 participants who participated in the study, 58 participants completed the entire survey. Mann Whitney U tests and Cross Tabulation analysis determined no statistically significant differences between those who completed the entire survey and those who did not, except for work setting size (X2 = 12.94, p = .002). Participants from large settings were more likely to not complete the entire survey when compared to small or medium setting sizes. On a Likert scale from 1 to 6, the mean confidence to accommodate clinicians living with disabilities was 3.23 (SD = 1.18).
Hypothesis Testing
For the 141 participants who responded to the survey, the summary of available responses and their corresponding overall response percentage by section is shown in Table 2.
Summary of Svailable Responses by Sub-Theme.
Research Hypothesis #1
Attitude Scores
The participants have an overall positive attitude towards clinicians living with disabilities. 57 out of 67 respondents have an attitude score of over 3.5 (the neutral point), resulting in a p-value smaller than 0.001 (see Figure 3).
Histogram of Overall Attitude Score with Vertical Line Indicating the Median Score of 3.5.
Furthermore, based on the Wilcoxon rank sum test (W=, p = 0.03), participants who self-identify as living with disability (M = 4.58, SD = 0.64) are more likely to have a positive attitude than participants who do not (M = 3.98, SD = 1.00) (see Figure 4).
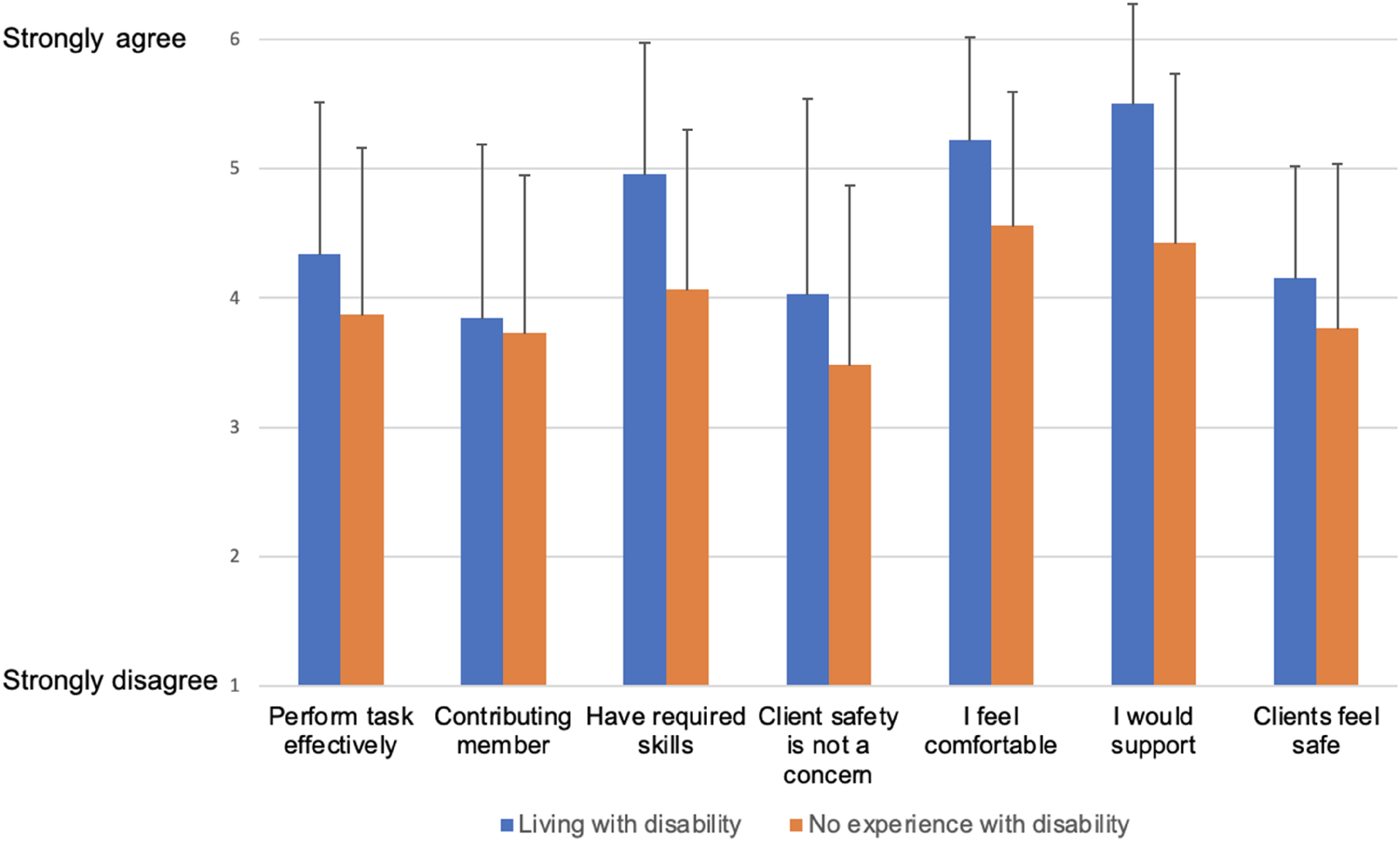
Histogram of mean Attitudes Comparing Participants who Experience Disability vs. Participants Who Do Not.
Institutional Barriers Scores
42 out of 52 respondents have a perceived barrier score of over 3.5, resulting in a p-value smaller than 0.001. This indicates that participants perceived more barriers for clinicians living with disabilities (see Figure 5). Furthermore, based on the Wilcoxon rank sum test result (p = 0.430) there is not enough evidence to conclude that there is a difference between the participants who did (M = 3.97, SD = 0.97) and those who did not (M = 4.06, SD = 0.61) self-identify as living with disabilities in the barriers score.
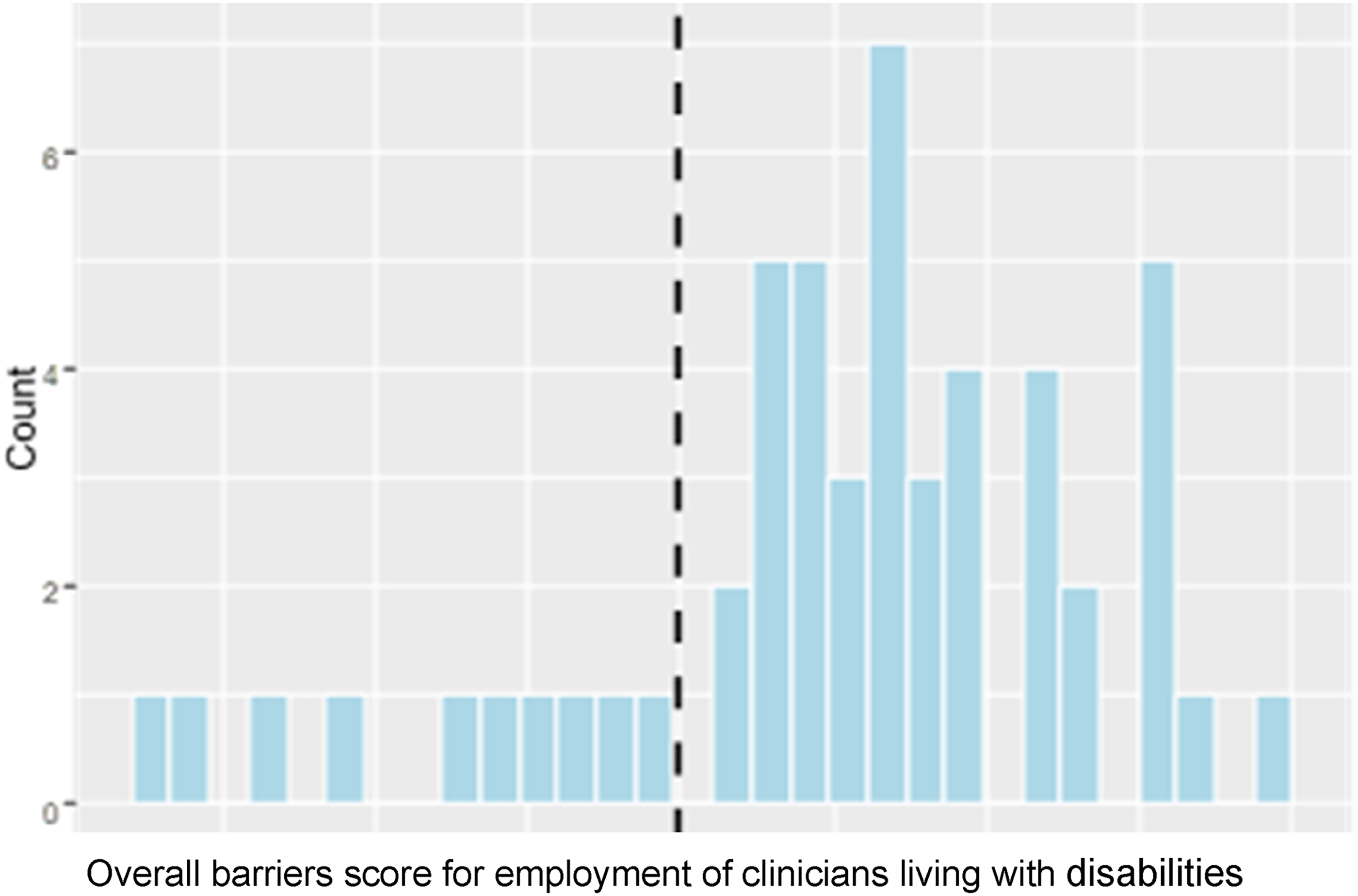
Histogram of Overall Barriers Score with Vertical Line Indicating the Median Sscore of 3.5.
Research Hypothesis #2
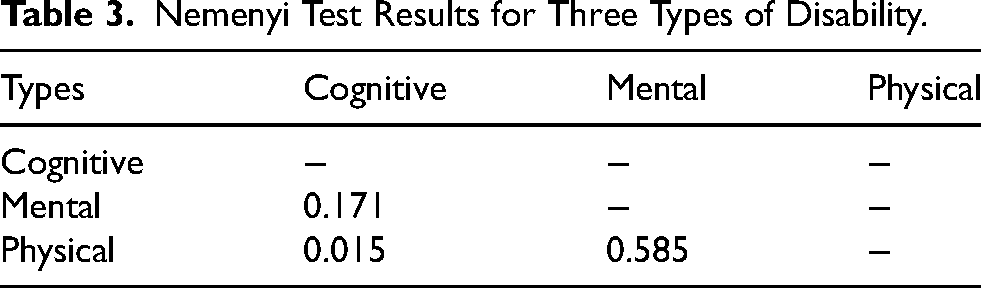
We did not find sufficient evidence shown in the data to conclude that barriers for employment of clinicians living with disabilities differ by type of disability. When comparing barrier scores between the three types of disability, the Friedman tests provide a relatively large p-value of 0.80. On the other hand, attitude scores among the three types of disability were found to be significant at the 5% level (p = 0.009). The result has a small effect size of 0.064 meaning although significant, the result relationship is quite weak. We used the Nemenyi post-hoc pairwise to compare attitude scores among the three types of disabilities. Since attitude scores were simultaneously compared among three groups to control family-wise type one error, the significance level of each comparison was set to .01667 instead. Attitudes toward the employment of clinicians living with physical disabilities (M = 4.59, SD = 0.71) are slightly yet significantly more positive compared to those living with cognitive/learning (M = 4.41, SD = 0.81) disabilities (see Table 3).
Nemenyi Test Results for Three Types of Disability.
In the written responses, it was found that the main barriers to employing clinicians living with mental or cognitive/learning disabilities were related to lack of flexibility of the job (e.g., “No options for flexibility for need for self-care/extra breaks as needed, pressure to work hard, no encouragement for self-pacing”) and time and efforts required to support clinicians (e.g., “We are short staffed and overworked. It's hard to find the time to help someone past learning disabilities”). In comparison, the primary barrier to employment of clinicians living with physical disabilities were related to lack of physical accessibility (e.g., “space - departments are poorly laid out (60's and 70's built) to accommodate”), cost related to facilitating accessibility within the workplace (e.g., “lack of access to resources to support this”), as well the job requirements.
Research Hypothesis #3
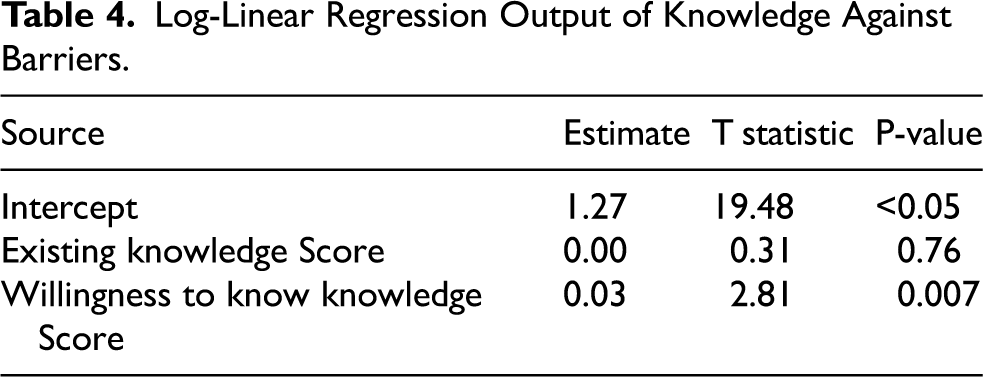
Attitudes toward the employment of clinicians living with disabilities vary based on willingness to learn more about helping colleagues living with disabilities. After fitting linear regressions of attitude scores on knowledge scores and barriers scores on knowledge scores respectively, only the relationship between the attitude score on a log scale and the “willingness to know” score of the knowledge subtheme were significant (Table 4). Figure 6 shows a scatterplot of the attitude scores on a log scale as a function of the score of “willing to learn more” about helping colleagues living with disabilities. More specifically, for every 1-point increase in the “willing to know” score, the attitude score increases by 2.2%. There was not sufficient evidence in the data that shows the variation of barriers to the employment of clinicians living with disabilities based on experience or knowledge of working with people living with disabilities.
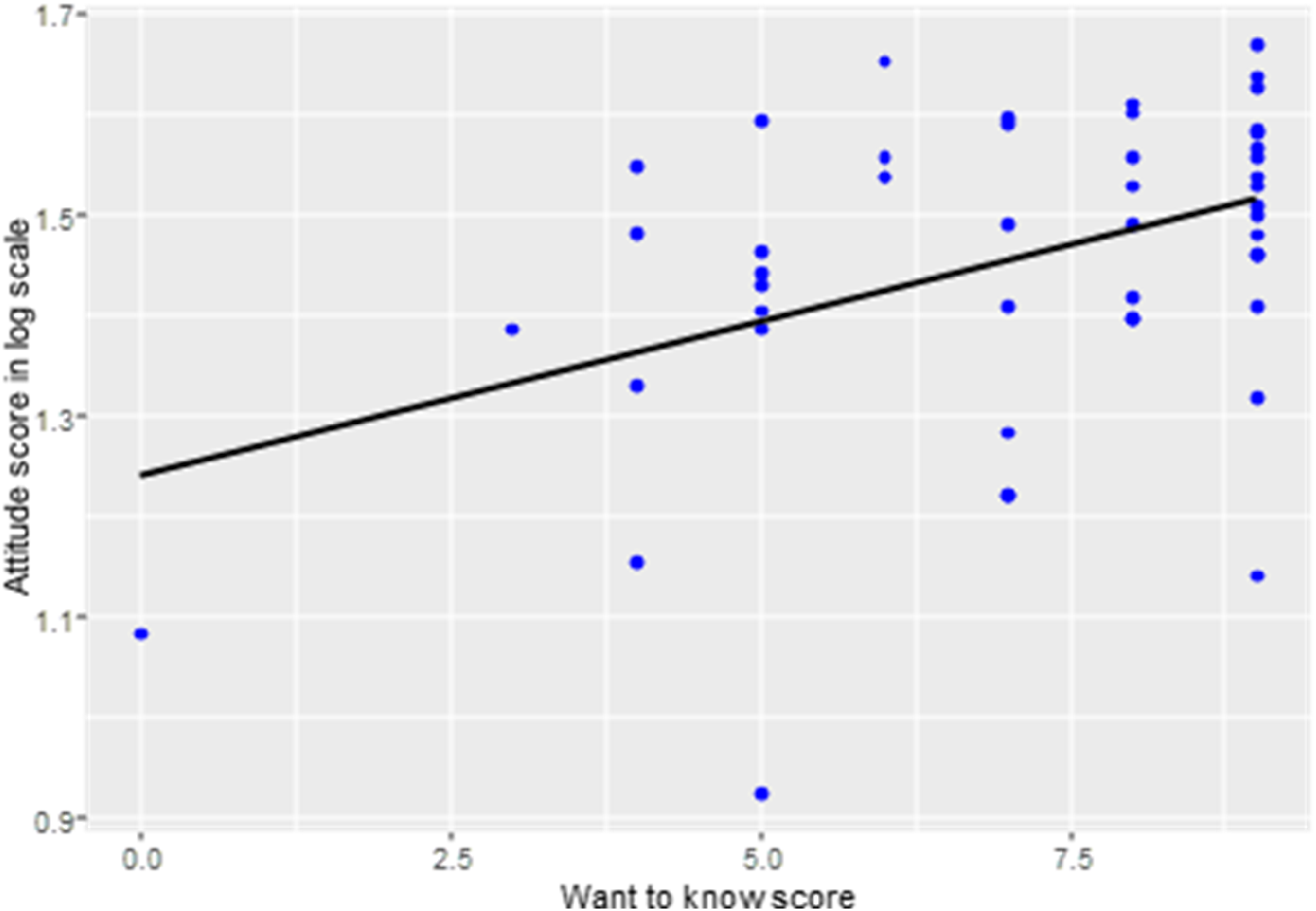
Scatter Plot of Attitude Score on a Log Scale as a Function of Score of Willingness to Learn More About Supporting Clinicians Living With Disabilities.
Log-Linear Regression Output of Knowledge Against Barriers.
Gaps in Knowledge
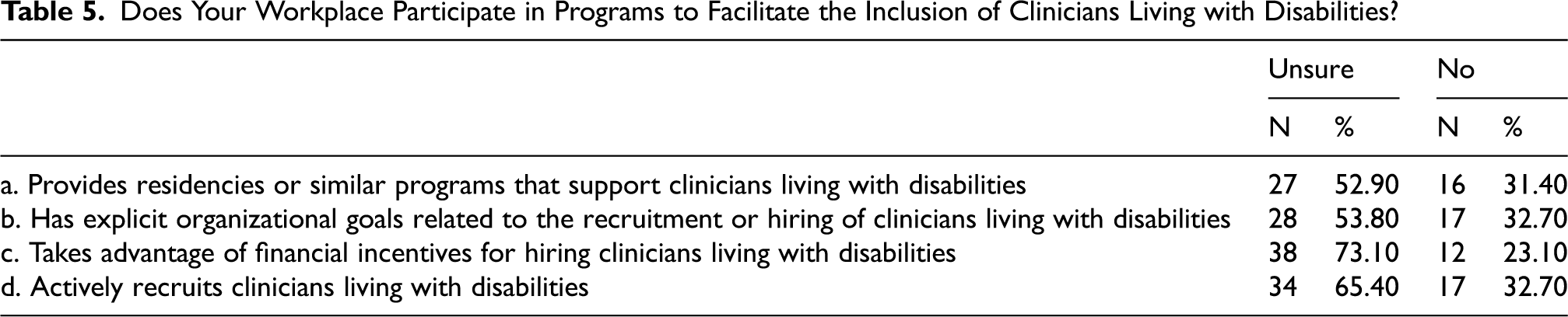
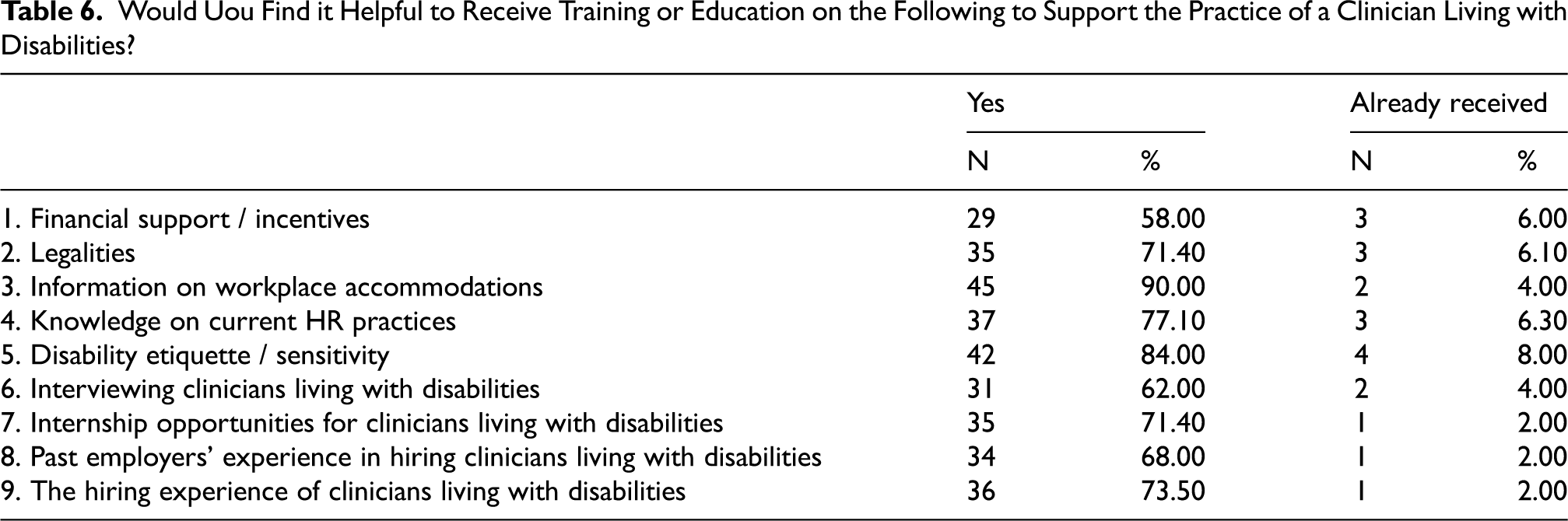
Over 80% of participants reported ‘unsure’ or ‘no’ to if their workplace participates in programs to facilitate the inclusion of clinicians living with disabilities. 66.67% of participants reported that they were unsure if their workplace includes clinicians living with disabilities in their equity, diversion, and inclusion plan. 86.84% of participants also reported that they had never received training or education around employing clinicians living with disability, however 88.89% acknowledged it would be beneficial. Nine examples of educational topics were provided to participants, such as legalities and past employers’ experiences. The majority of participants, ranging from 58–90%, reported that all nine topic examples would be helpful to receive education on (see Tables 5 and 6).
Does Your Workplace Participate in Programs to Facilitate the Inclusion of Clinicians Living with Disabilities?
Would Uou Find it Helpful to Receive Training or Education on the Following to Support the Practice of a Clinician Living with Disabilities?
In addition, gaps in knowledge reported differed based on type of disability. Regarding physical disability, gaps identified were the physical layout of the workspace both inside and outside, as well as the actual job demands. Regarding both mental disability and cognitive/learning disability, gaps identified included scheduling, stigma, and lack of ongoing support. One participant wrote “the management team at my worksite as a whole could benefit from training in workplace accommodation”.
Discussion
Over half of the study population identified as experiencing disability. While limited research has been done across disciplines, a recent report of the Canadian Medical Association reported 22% of participating physicians identify as living with a disability (Canadian Physician Health Survey, 2021). As such, the population of this study may not accurately reflect the attitudes/perceptions of healthcare employers and employes currently in the workforce. The goals of this paper are to drive change by increasing awareness and practicing more inclusive and empathetic leadership. Based on our studies, we will offer a few practical pieces of advice to healthcare leaders to embrace diversity and ensure differences are valued.
Type of Disability Matters
Participants acknowledged both the benefits, and the challenges of having a clinician living with disability on their team. The study's findings overall indicate that the attitudes and barriers to employing clinicians living with disabilities vary based on the perceived type of disability the clinician has. It is important for rehabilitation professionals to realize that addressing these attitudes and barriers not only can increase normalization and the number of healthcare professionals with disabilities but also improve patient experience for those with disabilities seeking assistance.
Attitudes toward the employment of clinicians living with disability were most positive toward those with a physical disability, followed by a mental disability, and finally, clinicians living with a cognitive/learning disability were perceived the most negatively. This pattern of attitudes was expected as it has been maintained in various types of workplaces over the years (Bricout & Bentley, 2000; Ju et al., 2013). Participants reported significantly more negative attitudes toward clinicians living with cognitive/learning disabilities for questions related to comfort of being a colleague, whether clients would feel safe under their care, and whether client safety is a concern. This follows a similar trend to attitudes in general sectors of work (Andersson et al., 2015; Ju et al., 2013; Kocman et al., 2017; Nota et al., 2014). These social attitudes around the perceptions of colleagues, managers, and clients have also been found to impact the employment of individuals living with disabilities in other areas of the workforce (Breen et al., 2019). This negative perception around different types of disability being ‘less than’ is reflected in the study's findings, as well as the continued lack of representation in the workplace.
In the barriers section of the survey, participants identified similar barriers for the employment of clinicians living with a mental disability and a cognitive/learning disability, however participants identified different ones for those living with a physical disability. For example, the location, accessibility, and layout of the workplace were the only barriers perceived to be significantly more likely to impact the employment of clinicians living with a physical disability. The structural barriers identified by healthcare employes and employers are similar to those found by Breen et al. (2019) and Bevan (2013). Also, inadequate accommodations for clinicians living with physical disabilities and the physical requirements of work were mentioned several times. For clinicians living with a mental or a cognitive/learning disability however, barriers of legal issues and additional time and effort on behalf of either colleagues or participants themselves were identified as having significantly more impact on employment. Similar barriers to safety and productivity concerns have been found in systematic reviews looking at employer attitudes toward people living with disabilities (Ju et al., 2013)
Encourage Team Members to Share their Experience with Disability
Significant differences in attitudes were found when comparing participants who identified as experiencing disability (first-hand experience), and those who did not (secondhand experience). Those who experienced disability themselves had significantly more positive attitudes toward the employment of clinicians living with disability on three of the seven attitude questions. In previous literature, negative attitudes are shown to be prevalent due to various factors, such as individuals living with disabilities being perceived to be less capable or skilled (Ju et al., 2013). This was supported by this study's findings - participants who experience disability had significantly more positive attitudes toward whether clinicians living with disabilities have the required skills to work. Evidently, there is a difference in the attitudes and perceptions between healthcare professionals who have first-hand experience, and those who have second-hand experience.
However, overall attitudes toward employing clinicians living with disabilities were still positive on each survey question, for all three types of disability perceived. This study uniquely looked at healthcare employes and employers who are assumed to have some experience working with individuals living with disabilities, which has been shown to result in more positive attitudes (Ju et al., 2013; Satchidanand et al., 2012). Colleagues who have experience with individuals living with disabilities are more likely to have more accurate views and positive attitudes (Elahdi & Alnahdi, 2022).
Educate Leaders to Dupport team Members to Ducceed in their Roles and Advocate for Policy Changes
Less than 20% of participants had received training on workplace accommodations or legislation, however, the majority reported that such would be helpful to support the inclusion of clinicians living with disabilities in the workplace. Several participants reported stigma and lack of understanding as a barrier to employing clinicians living with disabilities and alluded to a lack of knowledge by others within the workplace. A brief education session providing accurate information around the employment and inclusion of individuals living with disabilities has been shown to result in more positive attitudes of employers (Papakonstantinou & Papadopoulos, 2017). In the current study, participants identified various topics to be helpful for the hiring process, such as past employers’ experience, disability sensitivity, and information on legislation. Providing employers with similar types of education has been found to result in higher interest in the hiring of individuals living with disabilities (Andersson et al., 2015). Furthermore, employers’ attitudes toward accommodations have been found to be more positive if they have been provided with education around legislation (Mutchnick & Blount, 1996). Thus, changes in attitudes and perceptions toward clinicians living with disabilities can be achieved at the individual level.
However, gaps were also found at the organizational level. Most participants reported that their workplace either does not participate, or that they were unsure if they participated, in various programs that facilitate the inclusion of clinicians living with disabilities. For example, they noted that there is a minimal to zero presence of personnel that can assist clinicians living with disabilities such as occupational therapists or counselors. One participant stated in an open-ended question that “clinicians with disabilities are not on the radar of my worksite”. Results of this study can open the discussion for rehabilitation and human resource professionals needing to learn the kinds of workplace accommodations for healthcare professionals with disabilities. This organizational gap in knowledge can also be considered within the education system, where disability competence is not well-versed in university programs. It has been found that students in healthcare professions, such as nursing, hold negative attitudes toward colleagues living with disabilities (Shpigelman et al., 2016). This indicates that education around facilitating the inclusion of clinicians living with disabilities needs to begin prior to individuals even entering the workforce.
Limitations
It must be noted that the study's sample population was limited to employers and employes working within the public health authorities. This may have resulted in missing additional, and potentially different perspectives of healthcare professionals in private practice. However, as Canada's healthcare system is primarily publicly funded, it is important that research captures these perspectives to begin with (Lee et al., 2021).
Another limitation of the study was that the population was composed of a high percentage of healthcare workers who experience disability themselves, which may have resulted in more positive attitudes. 59.6% of participants self-identified as experiencing disability which is likely to be higher than the actual percentage of the population of clinicians living with disabilities. The Wilcoxon rank sum test revealed that the attitude score of people experiencing disability is significantly higher than people not living with disability. This concludes that people who have overall positive attitudes towards clinicians living with disabilities are likely biased, and it is uncertain whether the results can be applied to the general population.
Another limitation was the study's sample size. Although 141 responses were received, the actual responses used in the statistical analysis are only around a third of that number. The low response rate suggests that a more effective way of recruiting participants may need to be considered. One possible improvement of the survey is to make all questions mandatory to answer but provide the option of “prefer not to answer”. In that case, while respondents still have the freedom of not answering the questions, they need to put some indication, which might prompt them to answer the survey more carefully.
Furthermore, due to time constraints the study's methods were limited to only completing a survey. The survey was also not standardized, so the study cannot ascertain that construct validity exists. However, this tool was not only based on a literature review, but reviewed by the expert team and the Action Research Group (ARG) composed of clinicians living with disabilities, health professional employers, and researchers.
Lastly, over half of the study population did not complete the entire survey. When comparing those who completed the survey and those who partially completed the survey, no significant differences were found in the demographics except for workplace setting size. Participants who identified as working in large settings were significantly more likely to only complete part of the survey, when compared to those who identified as working in small or medium sized settings. This may be due to healthcare professionals in larger hospitals or clinics having a heavier caseload or being in a louder environment. These participants may have been interrupted by colleagues or clients more frequently while trying to do the survey, and therefore did not complete it.
Conclusion
In conclusion, the attitude of employers and employes has a powerful effect on perceptions (stereotypical or inclusive) toward individuals living with disabilities in the general workforce (Nelissen et al., 2015). In the current study, it was found that overall healthcare workers’ attitudes were positive. This could reflect the uniqueness of their experience working with people living with disabilities, or because of the study's significant percentage of participants who experience disability themselves. It was also found that participants who had “first-hand” experience of disability reported more positive attitudes than those with “second-hand” experience. However, attitudes and barriers significantly differed based on perceived type of disability, with the most negative perceptions toward clinicians living with cognitive/learning disabilities. While negative attitudes and barriers evidently exist in healthcare, our respondents reported a lack of education around accommodation practices to facilitate the inclusion of clinicians living with disabilities both at the individual level, as well as at the health authority level.
For B.C.'s public hospitals to accurately reflect the diverse population and improve the quality of client care, changes to the inclusion practices of clinicians living with disabilities in the workplace must occur at multiple systemic levels. Next steps to facilitate this include developing education programs on disability inclusion and ableism with mandatory completion for employers and employes.
Footnotes
Acknowledgements
The authors have no acknowledgements.
Ethical considerations
Ethics approval was provided by UBC Behavioural Research Ethics Board, H21-02479.
Informed consent
The informed consent form was provided to participants at the beginning of the survey (via a hyperlink), and consent was confirmed at completion of the survey.
Funding
The dissemination of this study was supported through the SoTL Linkage Grants F23-03269.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.