
Abstract
Background
The Office of Special Education and Rehabilitative Services (OSERS) outlines provisions states must follow regarding vocational rehabilitation (VR) services. However, states are allowed to develop and implement their own guidance documents.
Objective
Drawing from VR eligibility documents obtained from 20 states, this paper discusses the variations in eligibility criteria across states, VR representatives’ perception of their states’ criteria, and the referral process for individuals with visual impairment (VI) applying for VR.
Methods
This study involved a national online survey and review of state VR agency contacts. In-vivo coding and descriptive statistics (frequency and percentages) were used to summarize survey responses and findings from policy documents.
Results
This study reveals preliminary evidence of interstate and intrastate differences in eligibility criteria for VR services for individuals with VI, variability between special education (school-based) and VR (adult-based) eligibility criteria, as well as variability in the number of referrals VR agencies receive, the ways in which referrals are received, and the time from initial contact to eligibility determination among states.
Conclusion
The findings provide important implications for professionals and policymakers when determining eligibility for adult VR services for individuals with VI. Further research should examine eligibility documents from all U.S. states and territories.
Introduction
State Vocational Rehabilitation (VR) Service Programs are sanctioned through the Rehabilitation Act of 1973, amended by Title IV of the Workforce Innovation and Opportunity Act (WIOA) in 2014. State VR agencies provide services to individuals with disabilities so that they may prepare for and participate in competitive integrated employment with consideration of their unique strengths and abilities (U.S. DOE, 2020). Individuals accessing VR services may be adults with newly acquired disabilities or young adults transitioning from school-age to adult disability services. According to the U.S. Department of Education (DOE)'s Office of Special Education and Rehabilitation Services (OSERS, 2022), 844,426 individuals received VR services under an individualized plan for employment in fiscal year 2020. Included in the population of individuals with disabilities served by VR are individuals with visual impairment (VI), including blindness.
According to recent data from the American Community Survey (ACS) conducted by the United States Census Bureau, there are an estimated 3.7 million people with visual acuity loss or blindness in the United States (National Research and Training Center on Blindness and Visual Impairment (NRTC, 2024). Visual acuity loss is defined as an acuity of 20/40 or worse, and blindness as an acuity of 20/200 or worse in the better eye. Historically, individuals with VI have higher unemployment rates, lower annual earnings, lower annual household incomes, and higher poverty rates in comparison to the general U.S. population (Erickson et al., 2018). Data from multiple sources indicate that approximately 44% of persons with VI are employed, while 10% are unemployed, and 50.9% are not in the labor force at all (McDonnall & Sui, 2019). Other research examining data from the 2019 ACS found that 46.2% of people with VI were employed compared to 78.6% of non-disabled people (McDonnall et al., 2022). Although the percentage of employed persons with VI varies, it is clear that individuals with VI are unemployed at greater rates than persons without disabilities.
Benefits of Access to VR Services for Individuals with VI
Research suggests there may be numerous benefits to accessing VR services. First, three studies from the NTRC found that employers lack knowledge of how individuals with VI perform job tasks and, on average, possess negative attitudes toward employees who are blind or visually impaired (McDonnall et al., 2014, 2015; McDonnall & Cmar, 2022). Data from these three studies suggest that employer communication with VR can improve employer knowledge, hiring, and attitudes toward employees with VI. This is significant because when employers are in contact with VR agencies, they are more likely to know how to support employees with VI.
Second, in another study, Giesen and Hierholzer (2016) studied VR consumers with VI who were social security disability income (SSDI) beneficiaries. Giesen and Hierholzer found that these VR consumers had increased odds of competitive employment when they received job-related services and counseling and guidance from VR. The authors defined job-related services as job placement and search assistance, on-the-job supports, job-readiness training, and on-the-job training. All job-related services, except for job-readiness training, increased recipients’ odds of securing competitive employment. Recipients of job placement and search assistance, on-the-job supports, and on-the-job training experienced increased odds of competitive employment ranging from 78% to 306% depending on the job-related service. Furthermore, recipients of VR counseling and guidance had 32% increased odds of competitive employment compared to those who did not receive these services.
Third, drawing from the U.S. DOE's Rehabilitation Services Administration Case Service Report (RSA-911) database, Cimera et al. (2015) examined 2,543 cases closed by the state-federal VR program in 2012. Each of the cases involved a transition-aged youth (i.e., 16–25 years old) with VI and blindness. One finding that underscored the importance of VR services was that participants who achieved competitive employment received a higher number of VR services than those with unsuccessful employment outcomes.
Inequities in Access to VR Services
Despite the benefits that VR services may supply, several factors may impact an individual's ability to access services. For example, one factor that may impact access is a consumer's race or ethnicity (Capella, 2002; Giesen et al., 2004; Yin et al., 2022). In 1992, Congress amended the Rehabilitation Act of 1973 and acknowledged there were inequities that occurred in the state-federal VR system for traditionally underrepresented populations (Rehabilitation Act, 1992). However, despite the acknowledgment of these inequities, and an amendment to the Rehabilitation Act, 10 years later, Capella (2002) found that minority groups continued to receive VR services at a rate disproportionately lower than individuals who are White. For example, in 2002, White applicants with complex needs were 1.5 times more likely to be accepted for VR services than African American applicants with the same level of education and severity of disability (Capella, 2002). However, around the same time, access percentages for VR services for consumers who were legally blind, were higher for African Americans, lower for White individuals, and about the same for Native Americans, Asian Americans, and Hispanic Americans. These access percentages were proportionate to persons of the same race and ethnicity in the general population with VI (Giesen et al., 2004).
A recent study by Yin et al. (2022) examined racial differences in each step of the VR process—application, eligibility, service provision, and employment outcomes at case closure. Their study analyzed data from multiple sources, focused on individuals ages 15–64 falling into one of six categories representing the individual's “primary impairment at application” (p. 16): hearing, vision, physical, mental, self-care, and independent living limitations. At the application step, White individuals with disabilities were less likely to apply for services than African American, Native American/Alaska Native, and Hispanic individuals, and more likely to apply than Asian individuals. In the remaining three steps of the VR process, White applicants had higher rates of involvement in eligibility, service provision, and employment outcomes at closure than individuals belonging to African American, Native American/Alaska Native, and Hispanic backgrounds, and lower rates than Asian applicants.
Differences in State Eligibility Criteria
OSERS (2024) outlines the provisions states must follow regarding assessment for determining eligibility and priority for VR services, as well as timeliness of evaluation completion for new referrals (34 C.F.R. § 361.41(b)). OSERS mandates that state units providing VR services must have “clear and convincing evidence” before determining that an individual is incapable of benefiting from services regarding an employment outcome. Examples of assessments VR might use to determine eligibility include situational assessments, supported employment assessments, and functional assessments of skill development activities, with necessary supports. Although OSERS requirements are provided for assessment, priority, and the determination of services, states are allowed to develop and enforce their own guidance documents for eligibility determination. That is, there is no universal definition nor qualifications to access VR services across all states in the United States. While general differences between VR agencies have been documented among states (e.g., Cavenaugh, 2010; NRTC, 2024), there has never been an analysis of interstate differences in the interpretation of the outlined VR eligibility requirements for individuals with VI.
Recently, interstate differences in the Individuals with Disabilities Education Improvement Act's (IDEIA, 2004) eligibility criteria for the specific categories of VI, including blindness (Schles & Travers, 2023), and deafblindness (Travers & Schles, 2023) have been published. The results of this work suggest there are large intrastate and interstate variations for children with VI to access school-based services. Given these findings for school-based systems, and the lack of data on VR eligibility criteria for adult service systems, research is needed to understand the current variability in VR eligibility criteria among states for individuals with VI.
To address the knowledge gap surrounding variations in state eligibility criteria for VR services for individuals with VI, including blindness, we asked the following research questions:
How do state eligibility criteria for VR services for individuals with VI vary among states? Are there differences between the eligibility criteria used to determine school-based (special education) and adult-based (VR) services for individuals with VI within each state? What are the perceptions of VR representatives related to their states’ eligibility criteria for VR services for adults with VI? Are there differences in the number of referrals and referral procedures for individuals with VI among states?
Methods
We developed a survey to understand the variability in eligibility criteria for VR consumers with VI across all U.S. states and territories. Eligible survey participants included representatives from U.S. state and territory VR agencies. Participants had the option to either respond to a survey or directly email our research team their state's eligibility criteria policy documents. Our survey was approved by the Institutional Review Board at (Vanderbilt University) and conducted through Research Electronic Data Capture (REDCap; Harris et al., 2009). Data collection ran from October 2023 through January 2024. A copy of the survey is available upon request from the second author.
Recruitment
Recruitment occurred via direct email and phone calls. Initial contact was attempted via email. When the research team was unable to find a direct contact for a state VR agency via a public VR website, other contacts such as Ex Officio Trustees from the American Printing House for the Blind were emailed or called. Calls were made to a general informational phone number for the agency if listed. On average, three follow-up emails were sent, and two follow-up phone calls were made per state (range 1–4). Email recipients were encouraged to share the survey announcement with colleagues in other states.
Survey Instrument Development
The survey tool was collaboratively developed by the study authors. In addition, the Sensory Area Director from the Tennessee Department of Human Services consulted on the development of the survey tool, providing feedback as to how questions regarding job title, caseload size, and consumer connection to VR services should be phrased. We made revisions accordingly with some questions changing from dropdown selections to write-in responses.
The final survey instrument consisted of five overarching themes: information about the person completing the survey (job title and state where from), state determination for eligibility, current services, caseload size, and referrals. Respondents were asked to answer all questions concerning adult VR services only, not Pre-Employment Transition Services (Pre-ETS), as eligibility between these two services may differ.
RQ 1: State Eligibility Criteria
RQ 1 was divided into three parts, A, B, and C. This was necessary as some participants only sent us their state's policy documents regarding eligibility criteria for VR services and others completed the entire survey (including providing their state's policy documents).
RQ 1A: Eligibility Criteria Included in State Policy Documents
RQ 1A examined eligibility criteria for VR services included in state policy documents. To analyze the eligibility criteria, we created twelve variables that fell into four thematic groupings: legal components, qualifying conditions, assessment components, and word choice.
The three remaining variables in this group were coded as categorical. The first related to use of the better eye when determining eligibility. Three codes were developed: N = state eligibility criteria did not base eligibility off functional vision in the better eye, Y = state eligibility was based off functional vision in the better eye, and Y* = state eligibility was based off functional vision in the better eye or total blindness in one eye. The second variable was related to visual acuity thresholds (e.g., acuity must be worse than 20/70). The third documented the specific visual field restriction threshold stated in the policy document (e.g., 20°).
RQ 1B: Eligibility Criteria Reported by VR Representatives
RQ 1B examined VR eligibility criteria provided by survey respondents. We used the same variables listed above for RQ 1A, with the addition of one variable. We added a binary variable to document if respondents reported their state used the Social Security Administration's (SSA) definition of VI including blindness as their eligibility definition. The SSA considers an individual to be blind if “vision can’t be corrected to 20/200 in [the] better eye” or if one's visual field is “20 degrees or less in [the] better eye for a period that lasted or is expected to last at least 12 months” (Social Security Act, 1935).
RQ 1C: Comparison of Eligibility Documents to Representative Reported Criteria
RQ 1C directly compared the state eligibility criteria reported in policy documents (RQ 1A results) to the state eligibility criteria shared by VR representatives in the REDCap survey (RQ 1B results). The analysis involved the variables summarized above in RQ 1A and RQ 1B.
RQ 2: Comparison of School- and Adult-Based Eligibility Criteria
RQ 2 compared the variations in VR eligibility criteria reported in policy documents (RQ 1A) to the variations in school-aged criteria reported by Schles and Travers (2023). Data on progressive conditions was sourced from Schles et al. (2022). Using the thematic categories of qualifying conditions and assessment components as defined above, we were able to create a total of eight variables to directly compare eligibility criteria for school-aged and adult services. Under the theme of qualifying conditions, the four variables were: (1) eligibility was defined as vision in the better eye, (2) visual field restriction or loss qualified an individual, (3) visual acuity threshold, and (4) degree of visual field. Within the category of assessment components, the four variables were: (1) assessments were explicitly used for eligibility, (2) the criteria required an adverse educational impact (for students) or a substantial barrier to employment/ADL (for adults), (3) eye reports were used to determine eligibility, and (4) educational data were used to determine eligibility. Educational data for school-aged services included the use of a functional vision assessment (FVA), a learning media assessment (LMA), or an expanded core curriculum (ECC) assessment. Educational assessments for adult services included an FVA, an LMA, an individualized educational plan (IEP), or an Individualized Transition Plan (ITP).
RQ 3: Survey Respondents’ Perceptions of Referrals
RQ 3 evaluated survey respondents’ perceptions of their state's eligibility criteria and its implications. The three questions we asked were if: (1) they found their state's eligibility criteria for VR services to be inclusive enough so that all persons with VI could receive services, (2) any groups of persons receiving VR services in their state may be underrepresented, and (3) they noted any biases or trends in their state's eligibility process for persons with VI. Each question had an optional write-in response for participants to elaborate.
RQ 4: Number of Referrals and Referral Procedures
RQ 4 included four components gathered from survey responses. First, we asked participants to estimate the number of referrals their agency had received in the last year (listed in 10-person increments) from 0 to 150, with final options of 150 + and “I do not know.” Second, we asked participants to indicate the three most common ways clients were connected to VR services in their state among seven potential options: (1) Doctor/medical center, (2) Veterans’ Administration, (3) School/teacher, (4) Pre-ETS provider, (5) Self-referral /Family member, (6) Unsure/I don’t know, and (7) Other. If participants selected “other” they were asked to write in how clients were connected to VR services in their state. Participants were asked the question 3 times so they could report the first, second, and third most common ways clients were connected to VR services in their state. Third, we asked participants how long on average a case takes from initial contact to eligibility review. Fourth, we asked participants how long it takes, on average, for a VR counselor to be assigned once a client is found eligible for services.
Data Analysis
We used descriptive statistics (e.g., frequency and percentages) to summarize survey responses (RQ 1, RQ 3, RQ 4). For RQ 1B and RQ 2, we used in-vivo coding for qualitative responses to use survey respondents’ exact words/responses as codes (Saldaña, 2016).
Interobserver Agreement (IOA), RQ 1A
The first author, second author, and a research assistant (a special education master's student enrolled in a visual disabilities preparation program) coded all data located in state policy documents. The first author developed a codebook and then all three coders met to train on the codebook and to practice coding on six states. Each coder was required to reach 100% agreement for this initial coding session. Following the initial meeting, all three coders independently coded the remaining 13 states. However, agreement was low due to how different each state's criteria was to interpret (the initial six states were not representative of the dataset because the dataset was so heterogenous). Therefore, the three coders reconvened to revise the codebook and independently recoded all data. After this second round of coding, IOA between all coders was 100%.
Results
Survey Response Rate
Open to all US states and territories, a total of 20 states ultimately participated in this study. The region most represented in this study was the West with seven states. The Midwest and Northeast were equally represented, with a total of five states participating in the study from each region. The least represented region was the South, with three states. See Table 1 for a list of participating states. All survey respondents were VR program administrators, directors, or supervisors. Example titles included: “Program Administrator,” “Bureau Chief,” and “Vocational Rehabilitation Counseling Supervisor.”
A State-by-State Comparison of Qualifying Conditions Used in VR and School-Based Eligibility Criteria.
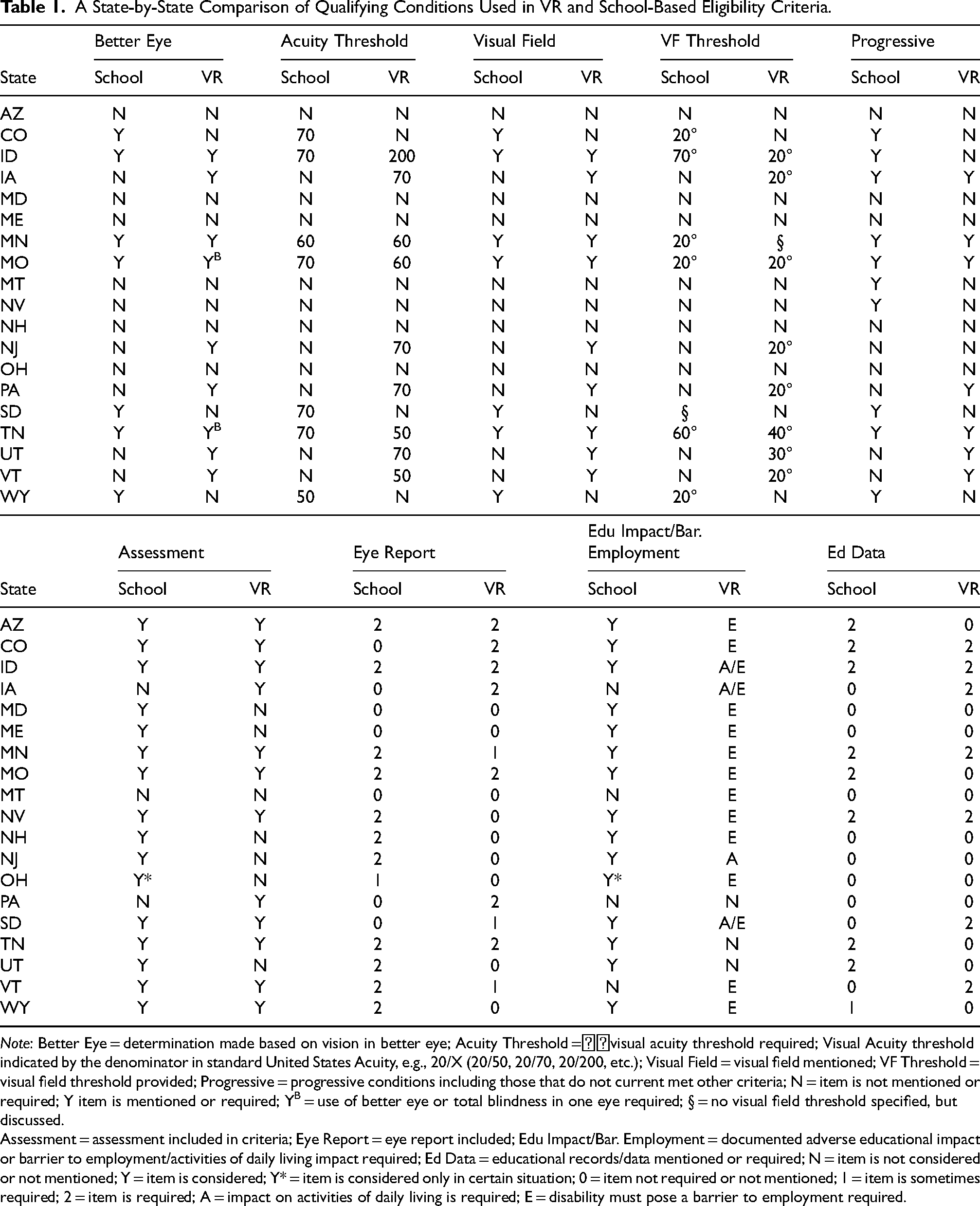
Note: Better Eye = determination made based on vision in better eye; Acuity Threshold =visual acuity threshold required; Visual Acuity threshold indicated by the denominator in standard United States Acuity, e.g., 20/X (20/50, 20/70, 20/200, etc.); Visual Field = visual field mentioned; VF Threshold = visual field threshold provided; Progressive = progressive conditions including those that do not current met other criteria; N = item is not mentioned or required; Y item is mentioned or required; YB = use of better eye or total blindness in one eye required; § = no visual field threshold specified, but discussed.
Assessment = assessment included in criteria; Eye Report = eye report included; Edu Impact/Bar. Employment = documented adverse educational impact or barrier to employment/activities of daily living impact required; Ed Data = educational records/data mentioned or required; N = item is not considered or not mentioned; Y = item is considered; Y* = item is considered only in certain situation; 0 = item not required or not mentioned; 1 = item is sometimes required; 2 = item is required; A = impact on activities of daily living is required; E = disability must pose a barrier to employment required.
RQ 1A: State Eligibility Document Criteria
Respondents from 20 states submitted their VR eligibility criteria documents. However, one state was excluded from the analysis as they uploaded the incorrect eligibility document. Therefore, we reviewed criteria from 19 states. See Table 1 for a state-by-state breakdown of legal components, qualifying conditions, and assessment conditions.
Legal Components
Ten of the 19 states (52.6%) maintained VR eligibility criteria specific to individuals with VI. Only nine states (47.4%) used general VR eligibility criteria, spanning all disability types, with minimal or no specific mention of individuals with VI. However, two states that used general eligibility criteria included terminology specific to individuals with VI.
Qualifying Conditions
Nine states’ (47.4%) eligibility criteria contained visual acuity and visual field thresholds. Visual acuities ranged from 20/50 to 20/200, with 20/70 being the most frequent (n = 4). Nine of the 11 states that had VI-specific criteria mentioned acuity and visual field qualifications. States with general criteria did not include any qualifying conditions. Seven states’ criteria (36.8%) included progressive visual conditions when determining eligibility for services.
Over half (n = 10; 52.7%) of the state eligibility criteria documents did not mention or include use of the better eye when determining eligibility. Seven states included use of the better eye when determining eligibility. Two states required use of the better eye or total blindness in one eye to be eligible for services.
Fifteen states’ (78.9%) eligibility criteria mentioned or required that an applicant's disability pose a barrier to employment to be eligible for services. Only four states (21.1%) mentioned or required that an applicant's disability adversely impact their ADLs to be eligible for services.
Assessment Components
Twelve states’ (63.2%) eligibility criteria required or mentioned some form of assessment for the determination of VR services. Of these 12 states, seven required a medical or eye report, three considered a medical or eye report when available, and two did not require a medical or eye report. The majority of states (n = 12; 63.2%) did not include language around the consideration of educational documents when determining eligibility.
Word Choice
Twelve states’ (63.2%) criteria contained language specific to individuals with VI. A total of eleven different terms were found in states’ eligibility criteria. The most common term was “visual impairment,” used by eight states. “Legal blindness” or “legally blind” were used by seven states. The terms “blindness” or “blind” were used by six states. The term “vision loss” was used by two states. “Visual disability,” “low vision,” “total blindness,” and “functionally blind” were used by one state each.
RQ 1B: Eligibility Criteria Reported by VR Representatives
We received 10 completed surveys and two partially completed surveys. Partial survey responses were retained in RQ 1B analyses, as both respondents answered questions regarding eligibility determination for VR services.
Assessments
All twelve survey respondents reported the use of assessments to determine eligibility. Furthermore, all respondents reported the use of eye reports. Nine survey respondents (75%) reported the consideration of educational data when determining eligibility.
Use of the SSA's Definition
Eight survey respondents (66.7%) indicated their state did not use the SSA's definition of VI to determine eligibility for services. Respondents from three states explained they do not have a state definition of VI or blindness for eligibility determination purposes. Two of these three states reported an applicant must show a need for VR services. The third respondent wrote: “We do not have a state-adopted definition [of VI]. Different programs throughout the state use different definitions.” The remaining five respondents who provided written responses, used broader eligibility criteria than the SSA definition, mentioning progressive visual conditions, lack of binocular vision, low vision, and functional limitations due to a VI.
RQ 1C: Comparison of Eligibility Documents to VR Representative Survey Responses
Eleven states provided both policy documentation and survey responses to be directly compared for analysis. See Table 2 for a summary of the state comparison information.
State-by-State Comparison of Eligibility Criteria from State Documents Versus Criteria Reported by VR Representatives.
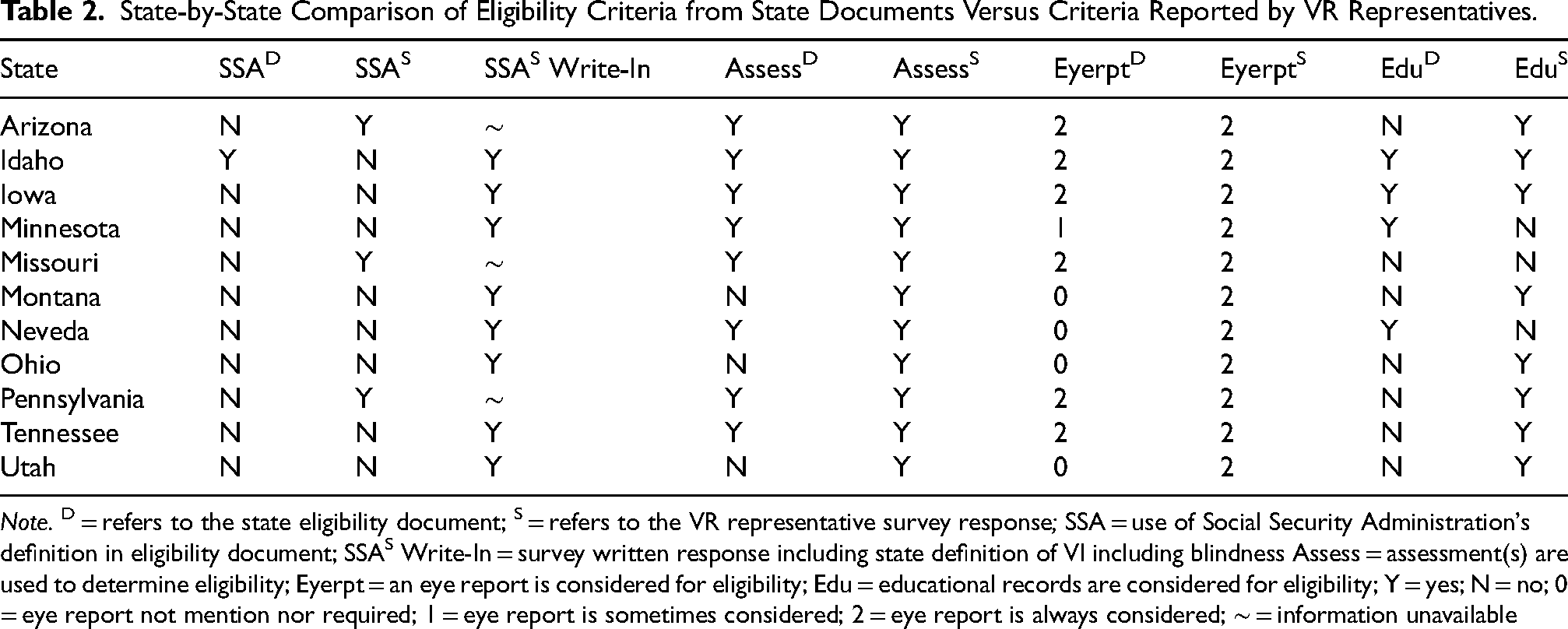
Note. D = refers to the state eligibility document; S = refers to the VR representative survey response; SSA = use of Social Security Administration's definition in eligibility document; SSAS Write-In = survey written response including state definition of VI including blindness Assess = assessment(s) are used to determine eligibility; Eyerpt = an eye report is considered for eligibility; Edu = educational records are considered for eligibility; Y = yes; N = no; 0 = eye report not mention nor required; 1 = eye report is sometimes considered; 2 = eye report is always considered; ∼ = information unavailable
Most Common Referral Methods Reported by Survey Respondents.
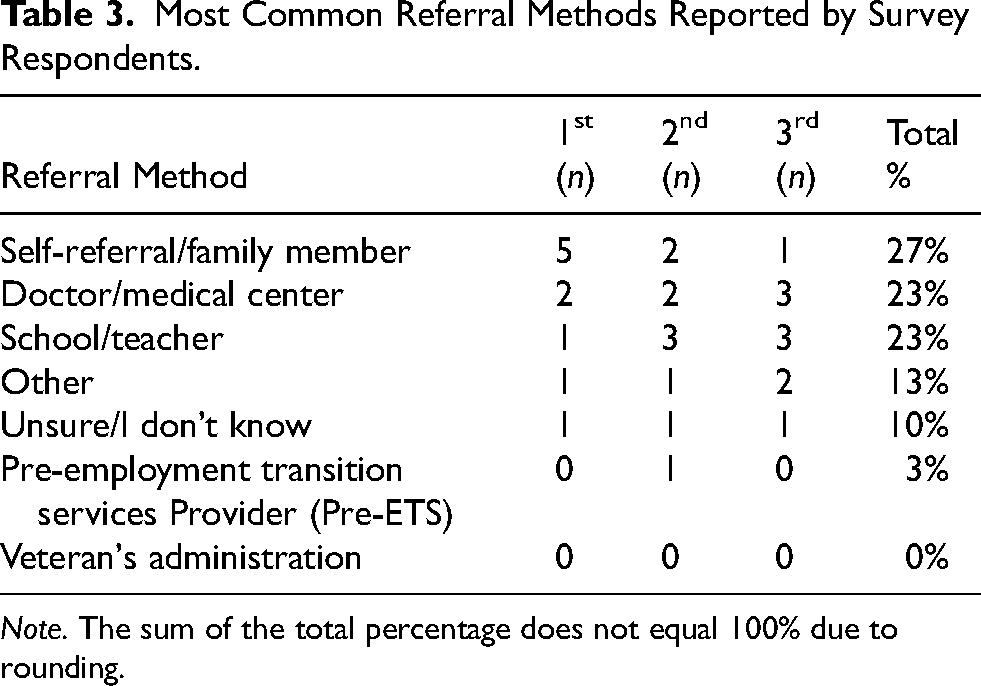
Note. The sum of the total percentage does not equal 100% due to rounding.
Assessments
Eight (72.8%) states’ policy documents indicated that assessments were a required part of the eligibility determination process. Conversely, responses from all eleven survey participants indicated the use of assessments to determine eligibility for services was required. Seven (63.6%) states’ policies sometimes or always considered an eye report when determining eligibility for services. In contrast, all survey respondents reported using an eye report to determine eligibility. Finally, four states (36.4%) referenced the use of educational materials in their eligibility documents. However, eight survey respondents (72.7%) reported the use of educational materials to determine eligibility.
Use of the SSA's Definition
From eligibility document coding, only one state (9.1%) used the SSA definition of VI. However, this same state's representative reported that they did not use the SSA definition. Conversely, three state representatives reported using the SSA definition of VI even though the policy documents did not require this. Regardless of the data source, very few states used the SSA definition of VI as part of their eligibility criteria for VR services (see Tables 1 and 2 for state-specific data).
RQ 2: Comparison of School-Based and Adult-Based Eligibility Criteria
A total of 19 states were included in the comparison of eligibility criteria for special education (school-based) and VR (adult-based) services. States varied in how they quantified thresholds or parameters by which an individual may be found eligible for services, as well as the assessments used to determine eligibility. See Table 1 for a state-by-state breakdown of qualifying conditions and assessment components required for adult- and school-based services, respectively.
Qualifying Conditions
Four states (21.1%) considered use of the better eye when determining eligibility for special education and VR services; seven states (36.8%) did not consider use of the better eye for special education or VR services. The remaining eight states varied in their requirements between special education and VR services. Three states considered use of the better eye for special education services, but not when determining eligibility for VR services. Five states considered use of the better eye when determining eligibility for VR services, but not special education.
Seven states (36.8%) did not include an acuity threshold to determine eligibility for special education or VR services; four states (21.1%) did include this for both special education and VR services. However, of these four states, only one included the same acuity threshold for both special education and VR services (i.e., 20/60). Three states (15.8%) had visual acuity thresholds for the determination of eligibility for special education services but did not have them for VR services. Alternatively, five states (26.3%) had acuity thresholds when determining eligibility for VR services, but not for special education.
Seven states (36.8%) did not include a visual field threshold to determine eligibility for special education or VR services. Four states (21.1%) included visual field thresholds to determine eligibility for both special education and VR services. Only one state had the same visual field threshold when determining eligibility for special education and VR services (i.e., 20o). Considering variations, three states (15.8%) included visual field thresholds for special education, but not VR services. Conversely, five states (26.3%) included visual field thresholds when determining eligibility for VR services, but not special education.
Assessment Components
A majority of states (n = 14, 73.7%) required an assessment when determining eligibility for both special education and VR services. Two states (10.5%) required an assessment for special education, but not VR services. Three states (15.8%) required an assessment when determining eligibility for VR services, but not special education services.
We compared eligibility criteria related to how the visual impairment poses an adverse educational impact or substantial barrier to employment/ADL within each state. Fourteen (73.7%) states required documentation of an adverse educational impact to be found eligible for school-based services. Alternatively, 16 states (84.2%) required documentation of a substantial barrier to employment/ADL to be eligible for adult-based services.
There were variations between the use of eye reports to determine eligibility for special education and VR services. Eleven states (57.9%) required an eye report to determine eligibility for special education services, whereas only seven states (36.8%) required an eye report for VR services. Furthermore, only one state sometimes considered an eye report for special education services, compared to three states that sometimes required an eye report to determine eligibility for VR services.
Finally, there was variability in states’ consideration of educational data/records when determining eligibility. For special education services, educational data included the consideration of an FVA, LMA, and ECC assessment. For VR services, educational data included the consideration of an FVA, LMA, IEP, and ITP. Eight states (42.1%) required educational data for eligibility determination for special education services compared to 10 states (52.6%) for VR services. See Schles and Travers (2023) for specific educational assessments required when determining eligibility for special education services.
RQ 3: Survey Respondents’ Perceptions of State Eligibility Criteria and Referrals
Nine out of 10 survey respondents indicated that their eligibility criteria were inclusive enough so that all interested individuals with VI could receive services. The single respondent who did not feel their criteria were inclusive stated: “We are in the process of updating our eligibility criteria through our rule change. We intend to make it more inclusive to ensure all customers who have barriers to employment based on any kind of vision loss are able to obtain services. For instance, individuals with Cortical Visual Impairments are difficult to determine eligible even though we know they would benefit from services.”
Although the majority of respondents felt their criteria were inclusive, significant underrepresentation was also identified by participants. Seventy percent of respondents reported groups of individuals were broadly underrepresented in their state. Three respondents reported individuals living in rural areas were an underrepresented group. Two survey respondents each identified persons who are deafblind, Asian, Hispanic, and minority populations with vision loss as underrepresented groups receiving services. Finally, individuals with complex needs, individuals with mental health conditions, and Native Americans were each mentioned once. When asked if they noticed any biases or trends in their states’ eligibility process, all ten respondents said no.
RQ 4: Number of Referrals and Referral Procedures
Respondents from 10 states answered our questions about referrals. Four respondents (40%) did not know how many referrals for clients with VI their agency had received in the last year. Three (30%) reported receiving more than 150 referrals, one (10%) reported receiving 41–50 referrals, and two (20%) reported receiving 1–10 referrals.
The most common way respondents reported receiving referrals was through a self-referral/family member, the second most common way was through school/teacher, and the third most common way was through a doctor/medical center. Table 3 summarizes the most common referral methods reported by respondents. Pre-ETS was mentioned by a single respondent as the second most common way clients were connected to VR services. Connection to VR services through the Veteran's Administration was not mentioned by any respondents. Respondents also had the option to select “Other” and write in the method by which clients are connected to VR services. One respondent selected “Other” for all three ways in which clients are connected to VR services and wrote in, “Varies- friends, family, universities, doctors, outreach, etc.” Another respondent selected “Other” regarding the third most common way clients are connected to VR services and wrote, “NFB, AFB, contracted vision provider.”
On average, respondents reported taking between two and four weeks from initial contact to an eligibility review for a client with VI. One respondent indicated an average review time of two months. Two respondents reported that they did not know the duration. Finally, two respondents wrote-in “24” or “45” without indicating a unit of time. Most respondents came from organizations where VR counselors were assigned prior to, or within a day of, an eligibility determination. One respondent each indicated a counselor was on average assigned within either 10 or 38 days. One person did not know how long it took for a counselor to be assigned.
Discussion
The primary purpose of this study was to document interstate variability in eligibility criteria for adult VR services for individuals with VI including blindness. A second purpose of the study was to gather information on state VR representatives’ perceptions of their states’ eligibility criteria and the methods by which clients are connected to VR services. Findings revealed that there is interstate variability in eligibility criteria for VR services. Furthermore, there is some preliminary evidence of intrastate differences in criteria regarding the definition of VI including blindness. Below, we summarize several important findings.
First, although there are similarities in eligibility criteria for VR services between some states, there are also notable differences between others. Several states such as Iowa, Tennessee, and Vermont had similar criteria across eligibility documents. All three states’ criteria were specific to individuals with VI, considered use of the better eye or total blindness in one eye as well as progressive visual conditions, and required some form of assessment when determining eligibility. However, criteria identified in eligibility documents also varied among states. For example, Idaho required a visual acuity of 20/200 or worse and a visual field threshold of 20 degrees or less. However, Utah had different criteria, considering individuals eligible if their acuity was 20/70 or worse and/or a visual field threshold of 30 degrees or less.
Potential VR clients must be made aware of differences in eligibility criteria among states. Given the range of potential eligibility criteria, individuals with VI may choose to live in one state over another, or not be aware of changes in services if they move across state lines. One should not be confined to a particular state due to inequitable eligibility criteria for VR services. As well, these differences are important for VR agencies and counselors to be aware of. When determining eligibility for services, VR counselors must have “clear and convincing evidence” before finding an individual incapable of benefiting from services in terms of an employment outcome (OSERS, 2024). Charged with this responsibility, VR counselors must be familiar with their own states’ eligibility criteria and what constitutes requiring VR services to make an informed decision. Our findings suggest VR representatives may not fully understand the language of their state policy documents. Therefore, it would be reasonable to assume they are not able to communicate clearly with the public about eligibility criteria. It is the responsibility of each VR agency to make their criteria and services clear. A potential solution would be to ensure all VR agencies design their public facing websites to be fully accessible and easy to navigate, including information about who may be eligible for services and what services are available.
Second, we found that there are interstate and intrastate differences between eligibility criteria for special education (school-based) and VR (adult-based) services. We identified differences among both qualifying conditions (e.g., visual acuity, visual field threshold) and assessment components used to determine eligibility. In particular, interstate and intrastate variations in visual acuity thresholds are concerning and may be problematic when determining eligibility for services. Some states did not consider visual acuity thresholds at all, some considered acuity thresholds only when determining eligibility for special education services, and some only when determining eligibility for VR services. Finally, others considered acuity thresholds for special education and VR services, but the threshold was not the same. These differences in visual acuity among states may contribute to some students getting identified for special education services but not VR. Perhaps more shocking, it may also lead to individuals who do not qualify for school-based services but who do qualify for adult services and do not know. Future studies should examine if and how variations in state eligibility criteria for special education and VR services may contribute to differences in the percentages of adults receiving VR services.
Third, variations in requirements around eye reports may contribute to inequities in who is found eligible for VR services. For instance, if an applicant's state requires an eye report to determine eligibility for services, one must then find the means to obtain an eye report. Cost, trust, communication, clinic accessibility (distance/transportation), and doctor-patient relationship have all been identified as barriers to eye care for individuals with high-risk status, those at risk for vision loss/underutilizing eye care, those living in rural areas, or those with low socioeconomic status (Elam & Lee, 2014). Indeed, research has found that variations in state eligibility criteria in school-based settings (e.g., assessment and eye report requirements) correlated to the number of students with VI identified for services (Schles & McCarthy, 2023). More research is needed to determine if the inability to obtain an eye report or other assessment materials used for eligibility purposes creates a barrier for individuals interested in VR services, especially those from rural areas where access to low-vision clinics or specialty medical centers may be particularly limited.
VR representatives in this study did not report any findings of bias or trends in their states’ eligibility process. Nearly all respondents (90%) reported their eligibility criteria to be inclusive enough so all persons with VI could access services. Yet seven (70%) survey respondents reported underrepresentation in groups receiving services in their state (i.e., persons from rural communities, those who are deafblind, Hispanic, Asian, and/or minority groups with vision loss). This finding is consistent with prior research that has shown that there are racial differences within steps of the VR application process, with minority groups having lower rates of eligibility, service, and employment (Yin et al., 2022). More research is needed to identify if variability in criteria impacts acceptance for VR services for individuals with VI belonging to minority groups.
Fourth, Pre-ETS providers were mentioned only once as a common method of referral to adult VR services. This finding was surprising as Pre-ETS providers function as VR staff in school settings. These staff can provide critical linkages for students and families as they transition from school-based to adult service systems (Awsumb et al., 2020). More research is needed to understand how persons with disabilities access adult services, and who is responsible for proactively identifying candidates for VR services in school settings.
Limitations and Future Research
A few limitations should be considered along with the findings of this study. First, the data reported in this study represent only a third (35%; n = 20) of U.S. states and territories. Additionally, we had a smaller response rate, 21% (n = 12), for the survey itself. We could not run statistical analyses because of the small sample size. Future research is needed including a larger sample, ideally the entire country. Although our findings provide early evidence of interstate and intrastate variability, we cannot generalize and make assumptions about the variability between and within the states and territories that were not included. Further, with a larger sample, future work could better examine how variability in eligibility criteria might correlate with the number of VR consumers in each state, and if eligibility criteria varied between combined and vision-specific VR agencies.
The survey did not include questions around the implications or implementation of orders of selection. Future research should include considerations around orders of selection as a state may have more inclusive criteria yet still only serve individuals with the most complex disabilities.
State regulatory and policy documents are subject to change over time. Therefore, the data presented here only capture VR criteria in effect in late 2023/early 2024. Readers should check their state's VR website or contact a representative for the most up-to-date information. Future researchers should ensure they use of current state policy documents in their analyses.
It was difficult to recruit VR professionals given inconsistent and difficult-to-navigate government websites. We recommend future replication studies rely on phone calls over email communication. As well, given that the information gathered from agency representatives did not align with the state policy documents, we would encourage future researchers to continue to collect policy documents in addition to any surveys completed by agency representatives to ensure accuracy of information.
This study combined the two referral methods of self-referral and family member to examine the number of referrals coming from a family unit. VR agencies may not report these two referral methods in the same category as was done in this study. Future research should examine self-referrals, or potential consumer voices, as they stand alone in their importance, separately from referrals made by family members.
Lastly, there is limited knowledge of the number of referrals VR agencies receive and the time from initial contact to eligibility determination, specific to individuals with VI. Findings from our study reflect VR counselors receiving as few as 1–10 referrals to upwards of 150 + . Further research is needed to identify the number of referrals for VR services for consumers with VI, as well as the timeliness of eligibility determination and inequities that may impact the eligibility determination process.
Conclusion
The findings of this study highlight evidence of interstate variability in eligibility criteria for adult VR services. As well, there is evidence of interstate and intrastate variability between special education and VR service eligibility criteria. Finally, early evidence suggests there may be variability in the number of referrals VR agencies receive, the ways in which referrals are received, and the time from initial contact to eligibility determination among states. However, only twenty states participated in this study. Further research should extend these findings and review eligibility documents from all U.S. states and territories. A comprehensive understanding of states’ eligibility criteria for adult VR services is needed to identify inequities more fully within state criteria and VR services. Additionally, there is no single universal definition of VI applied at either the school-age or adult level. Therefore, policymakers should consider how interstate differences may impact how individuals gain access to their state services.
Footnotes
Acknowledgements
The authors declare no acknowledgements.
Ethics Statement
The study was approved by the Vanderbilt University Institutional Review Board (IRB #231171).
Informed Consent
The Vanderbilt University Institutional Review Board determined that the study qualified as an Exempt Study which did not require formal informed consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.