
Abstract
Background
Healthcare professionals are frequently exposed to intense emotional demands that may lead to compassion fatigue. Challenges in maintaining work–life balance also play a significant role in shaping life satisfaction. Yet, studies examining their combined effects on healthcare professionals’ life satisfaction remain limited.
Objective
This study aims to examine the impact of compassion fatigue and work-life balance on the life satisfaction of healthcare professionals.
Methods
This cross-sectional quantitative study collected data from 301 healthcare workers at Kahramanmaraş Sütçü İmam University Hospital in Türkiye, using validated psychometric scales. Analyses included reliability testing, normality assessment, confirmatory factor analysis, and structural equation modeling.
Results
Changes in life satisfaction were 11% attributable to compassion fatigue (R2 = 0.115). The occupational burnout subdimension negatively affected life satisfaction (ß = −0.363; t = −4.060; p < 0.001), with each unit increase resulting in a 0.175-point decrease in life satisfaction. Nine percent of the variation in life satisfaction (R2 = 0.099) was explained by the positive impact of work on life (ß = 0.190; t = 2.739; p = 0.007) and the positive impact of life on work (ß = 0.155; t = 2.377; p = 0.018). However, the negative impact of work on life caused a 0.132-point reduction in life satisfaction (ß = −0.151; t = −2.385; p = 0.018). Overall, compassion fatigue and work-life balance together explained 12% of the variation in life satisfaction (R2 = 0.125; F = 21.332; p < 0.001).
Conclusion
Findings underscore the importance of alleviating emotional burden and implementing institutional policies that support work–life balance to enhance healthcare professionals’ life satisfaction. However, because this study was conducted in a single hospital and employed a convenience sampling method, generalizability of the results is limited.
Introduction
The healthcare sector is a complex and dynamic field that challenges the physical, emotional, and mental boundaries of its workforce. Healthcare professionals frequently face long working hours, heavy workloads, and emotionally demanding interactions. This reality impacts not only the individual well-being of healthcare professionals but also the efficiency of healthcare services and the quality of patient care.1,2 Improving the quality of life for healthcare professionals positively influences life satisfaction on an individual level, while also enhancing patient satisfaction and the sustainability of healthcare services at an institutional level.3,4 In this context, quality of life is a multidimensional concept that holistically reflects an individual's physical, environmental, social, and psychological condition, whereas life satisfaction is a psychological indicator that expresses the individual's subjective level of contentment with their life.5–7 In this study, life satisfaction is considered the subjective component of quality of life and is addressed as a significant construct reflecting an individual's overall well-being. However, to achieve these goals, it is essential to conduct a detailed examination of the critical factors that negatively affect the life satisfaction of healthcare workers. Considering that individuals working in help-oriented professions are constantly engaged in meeting others’ needs and providing emotional support, it is evident that these processes may eventually lead to emotional exhaustion.8–10 At this point, compassion fatigue, an important concept for understanding the emotional burdens of healthcare workers, holds critical significance for individual well-being and professional sustainability.
Compassion fatigue is defined as a state of emotional and cognitive exhaustion arising from the professional roles of healthcare professionals. Figley (2002) describes compassion fatigue as the emotional depletion and reduced capacity for empathy resulting from prolonged exposure to the traumatic experiences of others. 11 This phenomenon is commonly observed in professions where professionals witness patients’ suffering and share their traumatic experiences. Compassion fatigue can lead to negative outcomes such as secondary traumatic stress and burnout, adversely affecting both professional performance and individual quality of life. 12 Secondary traumatic stress refers to the emotional responses elicited by exposure to others’ traumatic events, while burnout results from the prolonged demands of professional roles, leading to physical and mental exhaustion. 13 In this context, compassion fatigue emerges as a factor that threatens not only individual well-being but also the quality of patient care. 14
To better understand the effects of compassion fatigue, it is essential to consider its relationship with work-life balance. Work-life balance refers to the harmonious integration of work and personal life, allowing individuals to derive satisfaction from both domains. 15 For healthcare professionals, achieving work-life balance not only fosters individual satisfaction but also enhances professional sustainability. However, the demanding nature of the healthcare sector often disrupts this balance, leading to increased levels of burnout and compassion fatigue, and consequently, decreased life satisfaction. 16 Mitigating work-related strain and fostering the enriching effects of personal life can have the positive contributions for enhancing the well-being of healthcare professionals 17
The intricate interaction between work-life balance and compassion fatigue becomes even more significant in terms of its effects on healthcare professionals’ life satisfaction. Life satisfaction refers to an individual's overall sense of contentment with life and is closely linked to physical, emotional, and social well-being. 7 Healthcare professionals’ life satisfaction is profoundly influenced by variables such as work-life balance and compassion fatigue.17,18 The literature highlights that low life satisfaction among individuals is associated with decreased job satisfaction, which negatively impacts the quality of healthcare services.19,20 This underscores the need to develop individual and institutional strategies to enhance healthcare professionals’ life satisfaction. 21
Previous research has mainly examined compassion fatigue, work-life balance, and life satisfaction either independently or in pairs. For example, Jeong and Jung (2020) investigated work-life balance, compassion satisfaction, compassion fatigue, and burnout among clinical nurses, but did not assess life satisfaction. 22 Cetrano et al. (2017) examined the effects of compassion fatigue, burnout, and compassion satisfaction on the quality of working life among mental health professionals but did not include work-life balance or life satisfaction. 16 Ruiz-Fernandez et al. (2020) analyzed quality of life in relation to socio-demographic variables, burnout, fatigue, and compassion satisfaction, but did not jointly assess work-life balance and compassion fatigue. 18
Similarly, Milutinovic et al. (2023) explored the effects of compassion satisfaction and compassion fatigue on nurses’ life satisfaction, but did not consider work-life balance. 17 Yaman and Özdelikara (2023) examined the impact of compassion fatigue on job and life satisfaction among oncology and palliative care nurses, but did not include work-life balance. 23 Öztürk and Karabulutlu (2021) investigated the relationship between compassion fatigue and life satisfaction in midwives, but excluded other variables. 24 Bae et al. (2020) studied the association between compassion satisfaction and work-life balance, but did not address life satisfaction. 25 Al-Otaibi and Kerari (2025) assessed the relationship between quality of working life, compassion fatigue, and self-efficacy among nurses, but did not examine work-life balance or life satisfaction. 26 Finally, Mitra et al. (2024) published an editorial that contributed to the discussion in this field but did not provide empirical data. 27
In our comprehensive literature search, no study was identified that simultaneously examined compassion fatigue, work-life balance, and life satisfaction within the same model among healthcare professionals. Therefore, the present study aims to address this important gap by evaluating these three variables together in a general sample of healthcare professionals. In doing so, it provides a more comprehensive perspective on the factors influencing healthcare professionals’ life satisfaction.
Materials and methods
This study was conducted to examine the effects of compassion fatigue and work-life balance on life satisfaction among healthcare workers, and it adopts a cross-sectional and quantitative research design. Quantitative research aims to obtain objective and generalizable results based on numerical data.28,29 In this context, the methodology section of the study provides detailed information on the population and sample, data collection tools, study limitations, and ethical considerations
Population and sample
The population of this study consisted of healthcare workers employed at Kahramanmaraş Sütçü İmam University Health Practice and Research Hospital. In this research, the term “healthcare worker” refers both to individuals directly involved in patient care (e.g., nurses, health technicians, and physicians) and to those with professional healthcare qualifications who serve in administrative roles. Employes in administrative positions are medically trained professionals who take on managerial or supportive roles within the hospital's operations. Therefore, all individuals included in the sample group were professionally qualified personnel in the field of healthcare. However, detailed data regarding the occupational distribution of the participants could not be obtained, and this is acknowledged as a limitation of this study.
Data were collected between February and April 2024 through face-to-face survey administration at the specified hospital by the researchers. The survey forms were administered to participants via one-on-one interviews, and written informed consent was obtained from healthcare workers who agreed to participate in the study. Participants were selected on a voluntary basis, and the data collection process was carried out with the approval of the hospital administration and the ethics committee.
The sample was determined using a convenience sampling method. This technique, which allows researchers to collect data from individuals who are accessible and willing to participate, is a practical non-probability sampling method preferred for its efficiency in terms of time and cost. Convenience sampling is a technique widely used in business and management research, largely due to its practical advantages. 30 As one of the non-probability sampling methods, convenience sampling offers a practical alternative that allows researchers to collect contextually useful data under practical constraints. 30 The use of non-probability sampling methods in quantitative studies is an increasingly common norm. A careful analysis of some high-level quantitative articles shows us that quantitative researchers frequently use at least five different non-probability sampling methods. 31 When used transparently and with appropriate justification and considering the good reputation of many studies that use this method, it can be said that the use of non-probability sampling in quantitative designs is acceptable and inevitable. 30 However, convenience sampling has certain limitations compared to probability-based methods.30,31 Particularly due to disadvantages regarding representativeness, the findings obtained through this method may have limited generalizability to the broader population of healthcare workers. Furthermore, the convenience sampling method weakens your ability to establish causal relationships between variables and make causal inferences, the results of this study should be interpreted within the institutional context in which the research was conducted.
A total of 301 healthcare workers who agreed to complete the survey form fully during the data collection process participated in this study. The adequacy of the sample size was evaluated based on the total number of scale items used in the research. The literature suggests that an appropriate sample size is three to ten times the number of scale items. 32 Accordingly, considering that the scales used in the study consisted of 37 items, the achieved sample size of 301 participants was deemed appropriate and sufficient.
Data collection tools
A questionnaire consisting of four sections was used in this study. The first section of the questionnaire included demographic characteristics of the participants, such as age, gender, marital status, education level, years of professional experience, weekly working hours, and the unit in which they work. The second, third, and fourth sections respectively employed the Short Compassion Fatigue Scale (SCFS), the Work-Life Balance Scale (WLBS), and the Satisfaction with Life Scale (SWLS). The characteristics of the scales are presented below:
Demographic characteristics
The first section of the questionnaire included demographic information about healthcare professionals, such as age, gender, marital status, educational level, years of professional experience, weekly working hours, and department of employment.
Compassion fatigue short scale (CFSS)
Developed by Adams et al. (2006) and adapted into Turkish by Dinç and Ekinci (2019), this scale consists of a total of 13 items and is structured as a five-point Likert-type scale (1 = Strongly disagree, 5 = Strongly agree).33,34 The scale comprises two sub-dimensions: “secondary trauma” and “occupational burnout.” For example, items such as “I have suddenly and involuntarily recalled a terrible experience while working with a patient” and “I feel worthless, disappointed, or angry about my work” reflect these two dimensions. A higher score on the scale indicates a higher level of compassion fatigue. In this study, the Cronbach's alpha coefficient of the scale was calculated as 0.92, indicating a high level of internal consistency. The data are normally distributed, with skewness and kurtosis values of 0.386 and −0.069, respectively. Normal distribution was assumed based on the criterion that skewness and kurtosis values fall within the range of −1.5 to +1.5. 35
Developed by Fisher, Bulger, and Smith (2009) and adapted into Turkish by Ekinci and Sabancı (2021), this scale consists of a total of 17 items.36,37 It comprises four sub-dimensions: negative work-to-life impact, negative life-to-work impact, positive work-to-life impact, and positive life-to-work impact. The scale is scored using a five-point Likert scale. A high score indicates a positive work-life balance. For example, the item “My job makes it difficult to maintain the kind of personal life I would like” reflects the negative work-to-life dimension, while the item “My personal life helps me relax and feel ready for the next day's work” represents the positive life-to-work dimension. In this study, the Cronbach's alpha coefficient for the scale was 0.889. The skewness (0.191) and kurtosis (0.103) values fall within the acceptable range for normal distribution. Since the values are within the range of −1.5 to +1.5, the dataset is considered to be normally distributed. 35
Satisfaction with life scale (LS)
Developed by Diener et al. (1985) and adapted into Turkish by Dağlı and Baysal (2016), this scale consists of 5 items.38,39 It is rated on a 5-point Likert scale, with higher scores indicating greater life satisfaction. For example, the items “My life conditions are excellent” and “I am satisfied with my life” directly reflect the individual's perception of life satisfaction. In our study, the Cronbach's alpha coefficient for this scale was calculated as 0.913. The skewness (0.121) and kurtosis (–0.366) values also fall within the acceptable range for normal distribution. Accordingly, the data were considered to be normally distributed. 35
Data analysis
The data obtained within the scope of the research were analyzed using SPSS (Statistical Package for the Social Sciences) and AMOS (Analysis of Moment Structures) software. First, descriptive statistics and demographic distributions were presented; then, the structural validity of each scale was tested through confirmatory factor analysis (CFA). In the final stage, multiple regression was conducted to evaluate the effects of compassion fatigue and work-life balance on life satisfaction. Reliability and normality analyses of the scales have been detailed in the relevant sections above.
Ethical considerations
Ethical approval for this study was obtained from the Social and Humanities Ethics Committee of Kahramanmaraş Sütçü İmam University Rectorate (Report No. E-282439. dated 26.01.2024). Additionally, permission was obtained from the Chief Physician of the Healthcare Practice and Research Hospital to conduct the study.
Results
The demographic variables of the participants, psychometric analyses, confirmatory factor analyses of the scales, as well as correlation and regression analyses, were examined in detail to provide a comprehensive understanding of the relationships among the study variables and the reliability and validity of the measurement tools used.
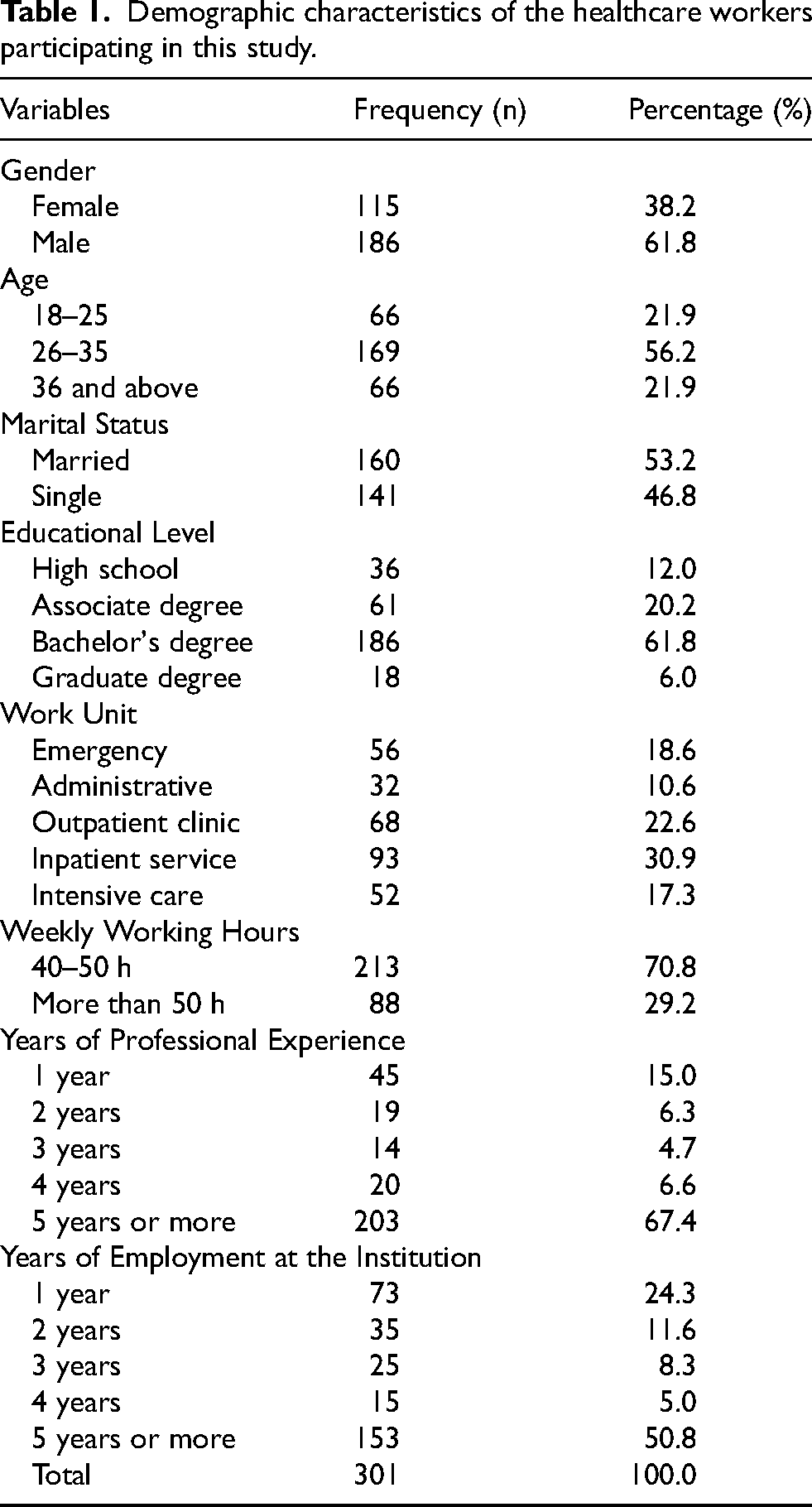
Table 1 presents the demographic characteristics of the healthcare workers who participated in the study. The majority of participants were male (61.8%), and the most represented age group was 26–35 years, accounting for 56.2% of the sample. In terms of marital status, 53.2% of the participants were married. Regarding education level, a large majority (61.8%) held a bachelor's degree. Among the units where participants worked, inpatient wards (30.9%) and outpatient clinics (22.6%) were the most common. Most participants reported working 40–50 hours per week (70.8%), and 67.4% had five or more years of professional experience. Approximately half of the participants (50.8%) had been working at the institution where this study was conducted for five years or more. This demographic distribution provides important insight into the representativeness of the sample among healthcare workers and reflects a diversity of professional experience.
Demographic characteristics of the healthcare workers participating in this study.
Psychometric properties
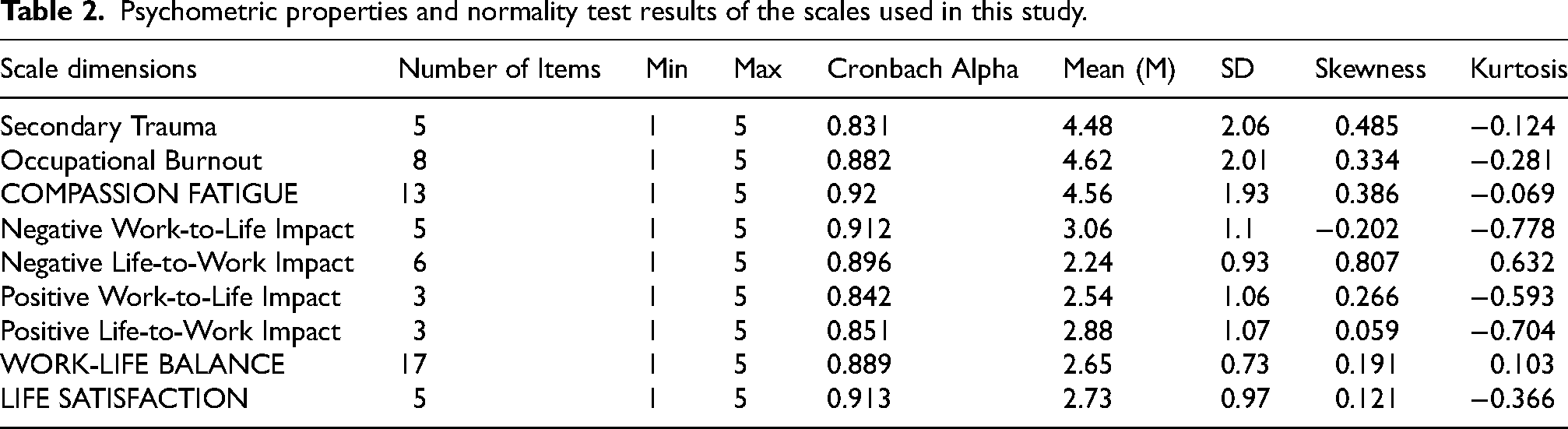
The psychometric analysis results presented in Table 2 indicate that the scales used in the study are adequate in terms of reliability and validity. The Cronbach's alpha coefficients demonstrate high internal consistency for all scales and their subdimensions, ranging from 0.831 to 0.920. Furthermore, the skewness and kurtosis values fall within the acceptable range of −1 to +1, indicating that the data conform to normal distribution. These results support the validity and reliability of the measurements of compassion fatigue, work-life balance, and life satisfaction.
Psychometric properties and normality test results of the scales used in this study.
Confirmatory factor analysis results and model fit
Compassion fatigue scale
The path diagram presented in Figure 1 illustrates the effects of the two subdimensions—Secondary Trauma and Occupational Burnout—on the corresponding items of the scale. The factor loadings range from 0.50 to 0.88, indicating that all items are significantly associated with their respective factors. A strong positive correlation (r = 0.93) was also observed between the two subdimensions.
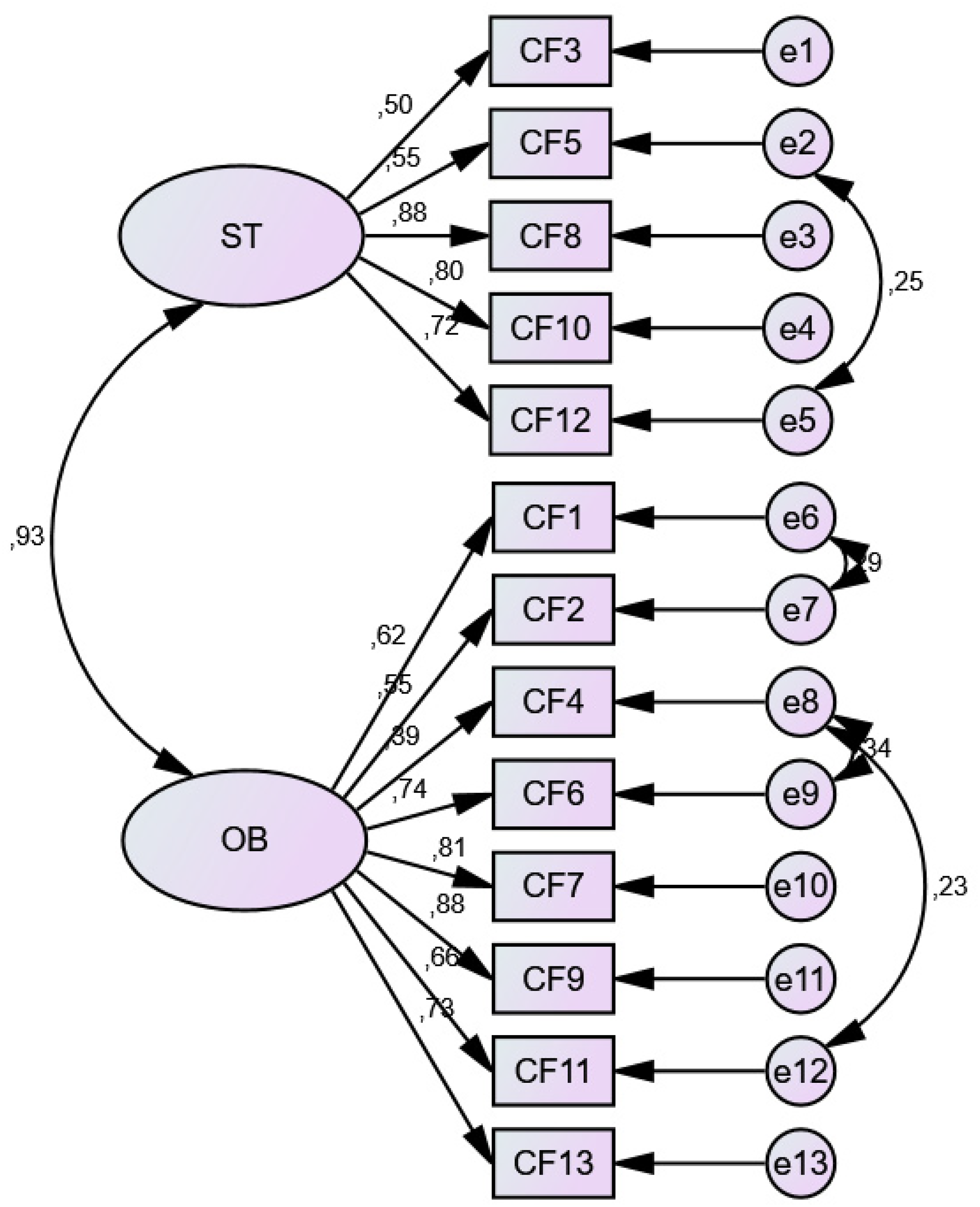
Path diagram of the confirmatory factor analysis for the compassion fatigue scale (ST: secondary trauma, OB: occupational burnout).
The model fit indices (χ2/df = 3.659; GFI = 0.904; CFI = 0.926; RMSEA = 0.079) demonstrate a good fit between the model and the data, supporting the structural validity of the scale at an acceptable level. 40 These results indicate that the Compassion Fatigue Scale is a reliable and valid measurement tool for assessing compassion fatigue among healthcare workers.
Table 3 presents the regression weights obtained from the confirmatory factor analysis for the two subdimensions of the Compassion Fatigue Scale: Secondary Trauma and Occupational Burnout. The standardized factor loadings range from 0.501 to 0.878 for the Secondary Trauma subdimension and from 0.391 to 0.881 for the Occupational Burnout subdimension. The fact that all item loadings exceed 0.30 indicates that the items are significantly associated with their respective factors.
Regression weights of the confirmatory factor analysis for the compassion fatigue scale.
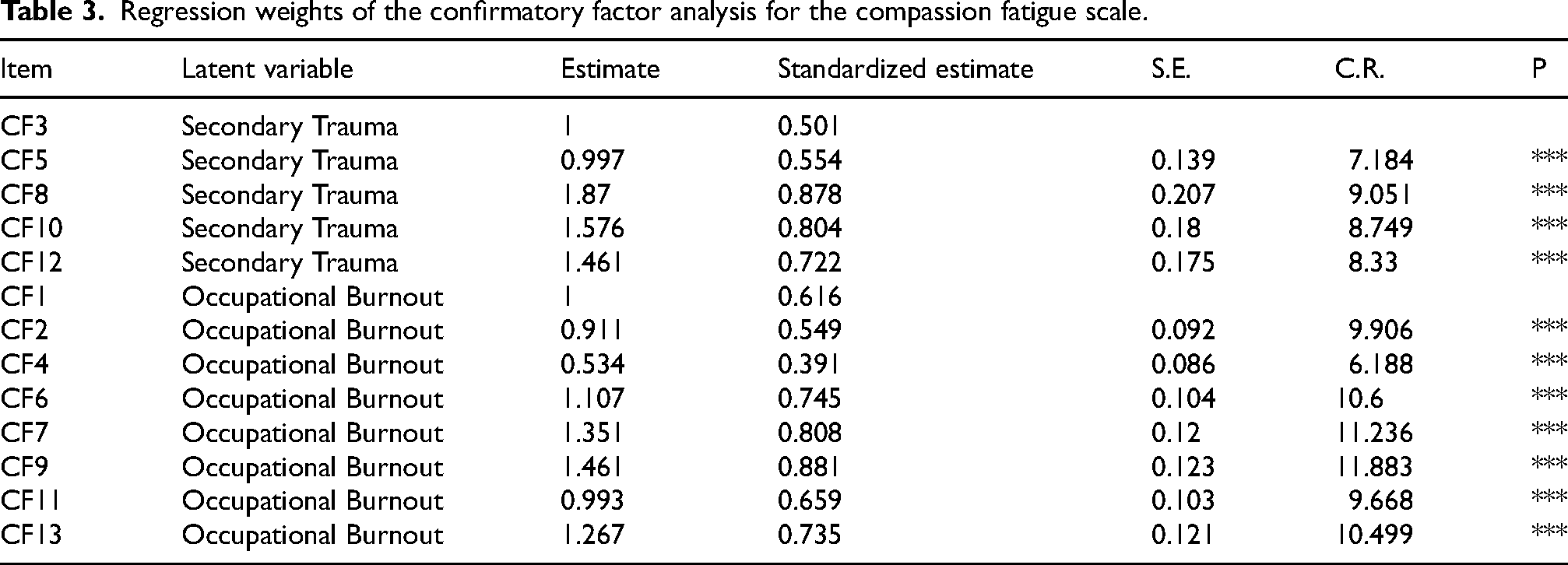
Moreover, the high critical ratio (C.R.) values and statistically significant p-values (p < 0.001) further support the reliability of the model. These results demonstrate strong construct validity for the scale and confirm that the subdimensions are effective in measuring compassion fatigue among healthcare workers
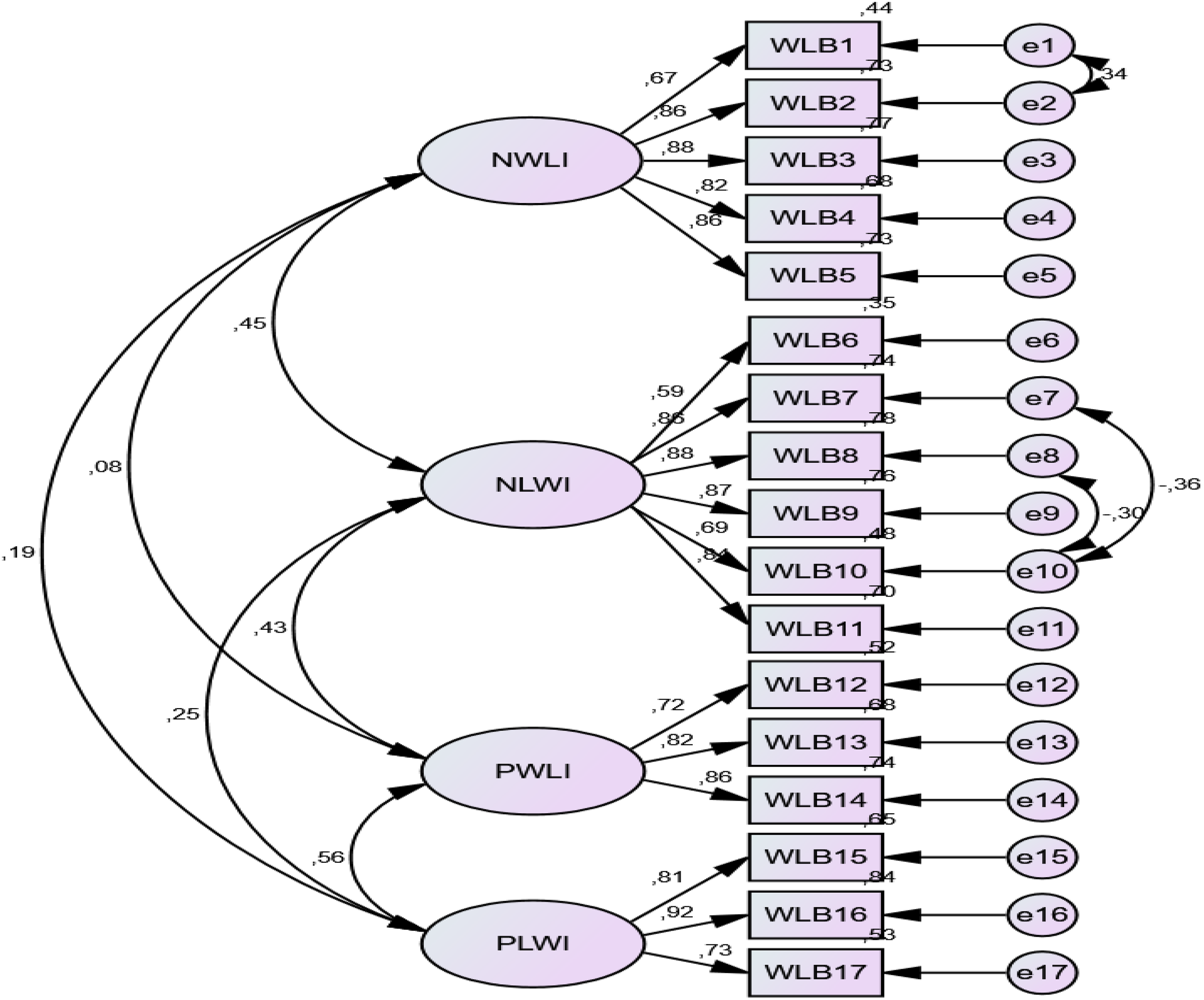
Path diagram of the confirmatory factor analysis for the work-life balance scale. (NWLI: Negative Work-to-Life Impact, NLWI: Negative Life-to-Work Impact, PWLI: Positive Work-to-Life Impact, PLWI: Positive Life-to-Work Impact).
Work-life balance scale
Figure 2 illustrates the confirmatory factor analysis model of the Work-Life Balance scale. Balance scale, illustrating its four subdimensions: negative work-to-life impact, negative life-to-work impact, positive work-to-life impact, and positive life-to-work impact. The standardized factor loadings range from 0.592 to 0.917, indicating strong associations between each item and its corresponding subdimension. Additionally, following covariance modifications in the model, the fit indices were at acceptable levels (χ2/df = 2.754, GFI = 0.904, CFI = 0.943, RMSEA = 0.076). This indicates that the goodness-of-fit values are within the acceptable range of the scale.40–42 These results demonstrate that the model is structurally valid within the sample of healthcare workers.
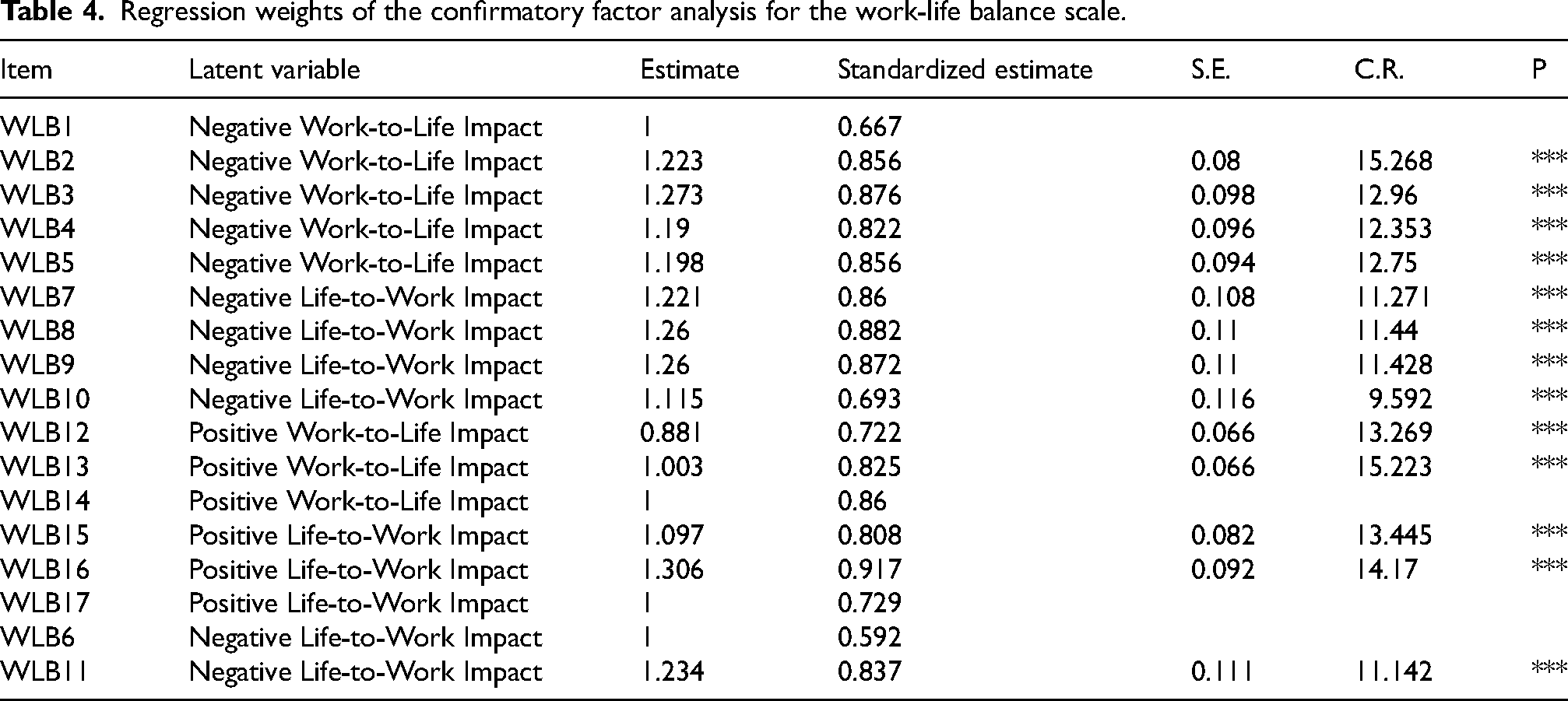
Table 4 presents the detailed regression weights for the items of the Work-Life Balance Scale. The standardized factor loadings range from 0.592 to 0.917, indicating that each item has a strong and significant relationship with its respective subdimension. All items demonstrated high C.R. values and statistically significant p-values (p < 0.001). These findings support the strong validity and reliability of the scale within the sample of healthcare workers.
Regression weights of the confirmatory factor analysis for the work-life balance scale.
Satisfaction with life scale
Figure 3 presents the path diagram of the Confirmatory Factor Analysis (CFA) for the Satisfaction with Life Scale. To improve the model fit indices, a covariance was added between item 4 and item 5. As a result of the covariance analysis, the model fit indices were as follows: χ2/df = 1.569, GFI = 0.991, AGFI = 0.968, CFI = 0.998, RMSEA = 0.044, RMR = 0.013, SRMR = 0.0101. These values indicate that the model demonstrates a good fit and falls within acceptable limits.40–42 The regression weights for this model are detailed in Table 5.
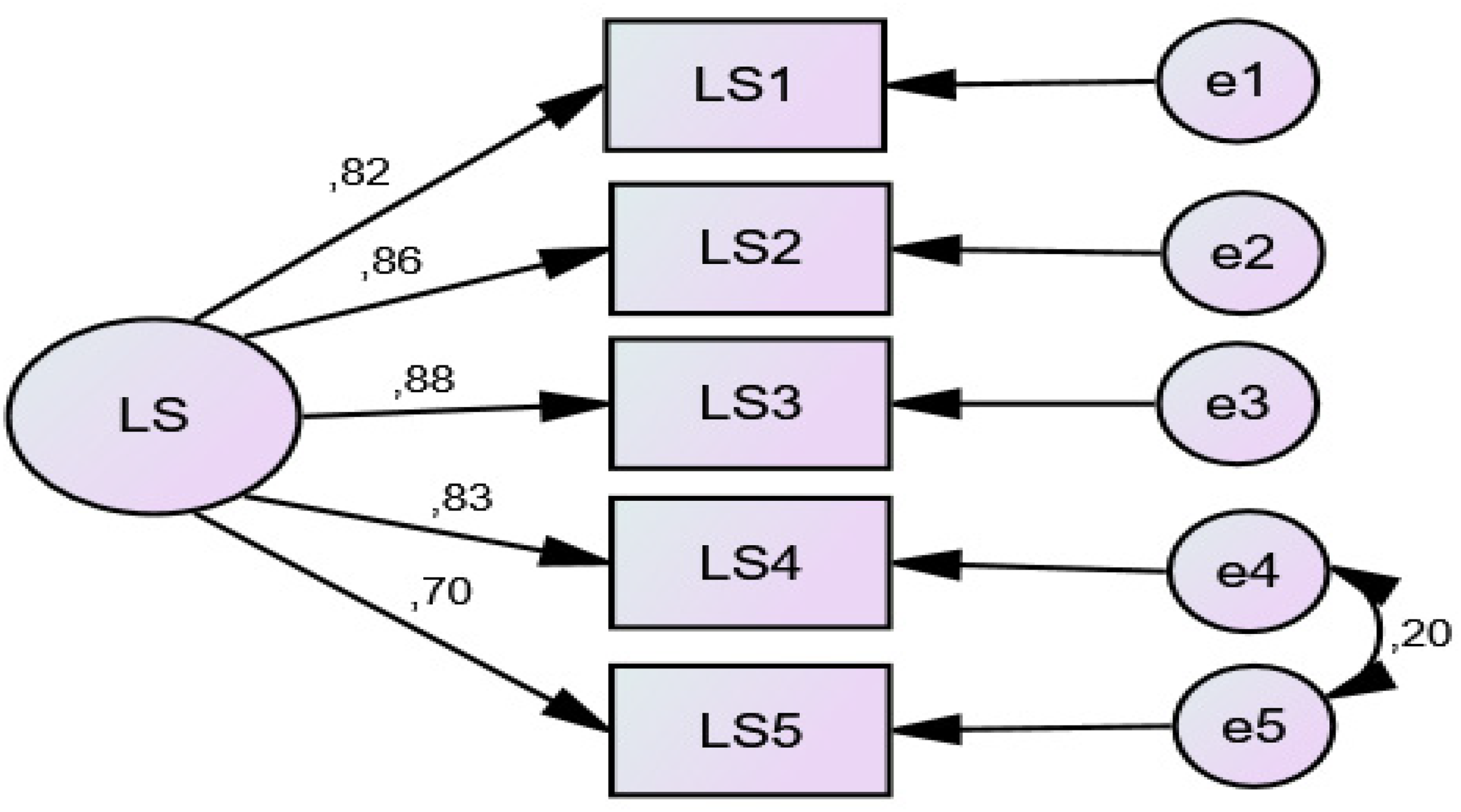
Path diagram of the confirmatory factor analysis for the satisfaction with life scale (LS: Life Satisfaction).
Regression weights of the confirmatory factor analysis for the satisfaction with life scale.

Table 5 presents the results of the confirmatory factor analysis for the five items of the Satisfaction with Life Scale. The standardized factor loadings range from 0.696 to 0.885, indicating that all items have a strong relationship with the corresponding factor. Additionally, all p-values were statistically significant (p < 0.001). These findings demonstrate that the Satisfaction with Life Scale consistently and validly represents the construct being measured and supports the high construct validity of the scale among healthcare workers.
Overall model fit evaluation
The model fit indices from the confirmatory factor analyses of the Compassion Fatigue, Work-Life Balance, and Satisfaction with Life scales fall within the threshold values accepted in the literature, indicating that the models exhibit a good fit with the data. 40 In particular, RMSEA values below 0.08 and CFI and GFI indices above 0.90 support the structural validity of the scales.41,42
Regression analysis results
Effect of compassion fatigue on life satisfaction
Table 6 presents the results of the regression analysis showing the effects of the subdimensions of the Compassion Fatigue Scale on life satisfaction. According to the analysis, 11% of the variance in life satisfaction (R2 = 0.115) is explained by the independent variables, secondary trauma and occupational burnout. The overall explanatory power of the model was significant (F = 19.372; p < 0.001). Among the subdimensions, occupational burnout has a statistically significant negative effect on life satisfaction (ß = –0.363; t = –4.060; p < 0.001). A negative relationship has been identified between occupational burnout and life satisfaction; as occupational burnout decreases, life satisfaction increases (ß = −0.363). Furthermore, the regression coefficient of the model falls between −0.259 and −0.090 at a 95% confidence interval (B = −0.175). This result indicates that a one-unit increase in occupational burnout leads to an approximate decrease of B = −0.175 units in life satisfaction scores. In contrast, the effect of secondary trauma on life satisfaction was not significant (p = 0.730). The Durbin-Watson value was 1.758, indicating no autocorrelation issue in the model. The Variance Inflation Factor (VIF) values of the model variables were found to be below 10, indicating that there was no multicollinearity among the variables. The standardized residuals of the model ranged between −3.29 and +3.29 (Std. Residual = −2.522 and 2.630), suggesting the absence of outliers in the model. The 95% confidence intervals of the model coefficients were as follows: ST = −0.068 to 0.098 and OB = −0.259 to −0.090.
Regression results of the subdimensions of compassion fatigue on life satisfaction.

Durbin Watson: 1.758, Std. Residual = −2.522 and 2.630.
Effect of work-life balance on life satisfaction
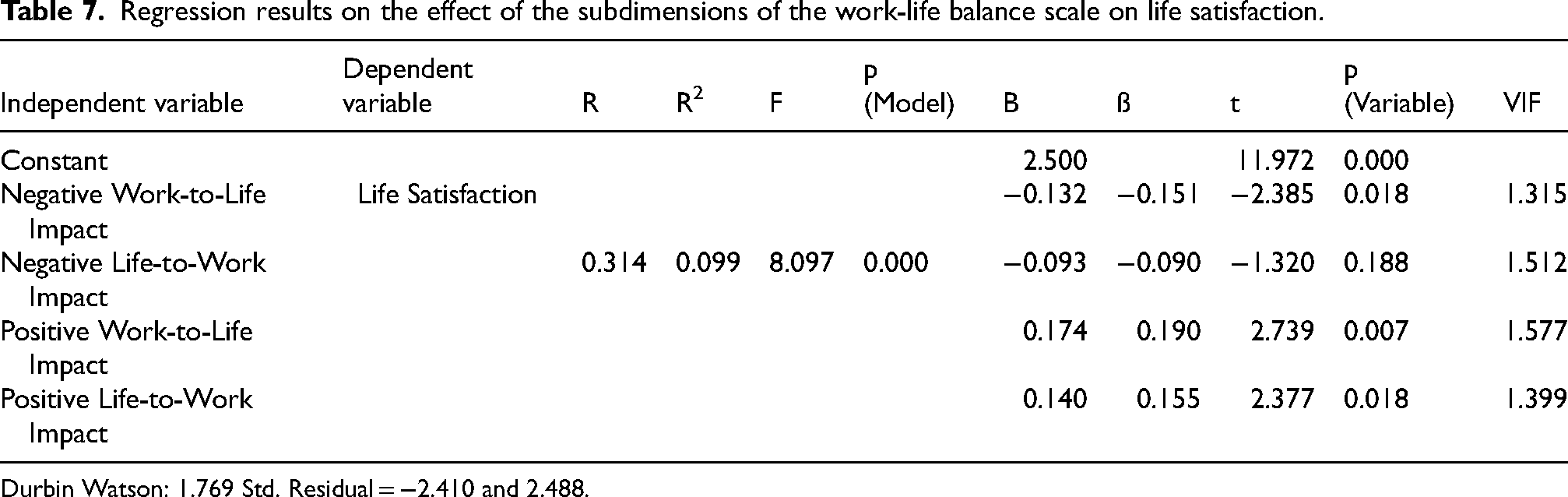
Table 7 presents the effects of the subdimensions of the Work-Life Balance Scale on life satisfaction. According to the analysis results, 9% of the variance in life satisfaction (R2 = 0.099) is explained by the subdimensions: negative work-to-life impact, negative life-to-work impact, positive work-to-life impact, and positive life-to-work impact. The overall explanatory power of the model (F = 8.097; p < 0.001) is statistically significant, and there is no model fit problem. The fact that the VIF values of the model variables are below 10 indicates that there is no multicollinearity among the variables. The standardized residuals of the model were found to range between −3.29 and +3.29 (Std. Residual = −2.410 and 2.488), indicating the absence of outliers. The 95% confidence intervals of the model coefficients were as follows: NWLI = −0.241 to −0.023, NLWI = −0.232 to 0.046, PWLI = 0.049 to 0.299, and PLWI = 0.024 to 0.256.
Regression results on the effect of the subdimensions of the work-life balance scale on life satisfaction.
Durbin Watson: 1.769 Std. Residual = −2.410 and 2.488.
Among the independent variables, negative work-to-life impact has a statistically significant negative effect on life satisfaction (ß = –0.151; t = –2.385; p = 0.018). A negative relationship has been identified between the negative impact of work on life and life satisfaction; as the negative impact of work on life increases, life satisfaction decreases (ß = −0.151). Furthermore, the regression coefficient of the model falls between −0.241 and −0.023 at a 95% confidence interval (B = −0.132). A one-unit increase in negative work-to-life impact leads to a decrease of B = –0.132 in life satisfaction scores.
In contrast, positive work-to-life impact (ß = 0.190; t = 2.739; p = 0.007) and positive life-to-work impact (ß = 0.155; t = 2.377; p = 0.018) significantly increase life satisfaction in a positive direction. As the positive impact of work on life increases, life satisfaction also increases (ß=0.190). Furthermore, the regression coefficient of the model falls between 0.049 and 0.299 at a 95% confidence interval (B = −0.175). A positive relationship was found between the positive impact of life on work and life satisfaction; as the positive impact of life on work increases, life satisfaction also increases (ß=0.155). The model's regression coefficient lies between 0.024 and 0.256 at a 95% confidence interval. A one-unit increase in positive work-to-life impact results in an approximately 0.174-unit increase in life satisfaction, while a one-unit increase in positive life-to-work impact leads to an approximately 0.140-unit increase. The Durbin-Watson value was 1.769, indicating no autocorrelation in the model.
Effects of compassion fatigue and work-life balance on life satisfaction
Table 8 presents the regression analysis results showing the effect of the Compassion Fatigue Scale and the Work-Life Balance Scale on life satisfaction. According to the findings, 12.5% of the variance in life satisfaction (R2=0.125) is explained by the independent variables, compassion fatigue and work-life balance. The explanatory power of the model (F = 21.332; p < 0.000) is statistically significant, and no fit issues were identified within the model. The fact that the VIF values of the model variables are below 10 indicates that there is no multicollinearity among the variables. The standardized residuals of the model were found to range between −3.29 and +3.29 (Std. Residual = −2.269 and 2.659), demonstrating that there are no outliers in the model. The 95% confidence intervals for the model coefficients were as follows: CF = −0.246 to −0.132 and WLB = 0.053 to 0.355. Compassion fatigue has a statistically significant negative effect on life satisfaction (ß = –0.376; t = –6.517; p < 0.001). This finding indicates that a one-unit increase in compassion fatigue results in an approximate decrease of 0.189 units in life satisfaction scores. A negative relationship has been found between compassion fatigue and life satisfaction (ß = −0.376). As compassion fatigue increases, life satisfaction decreases. The regression coefficient of the model falls between −0.246 and −0.132 at a 95% confidence interval.
Regression results on the effects of compassion fatigue and work-life balance scales on life satisfaction.

Durbin Watson: 1.781 Std. Residual = −2.269 and 2.659.
On the other hand, work-life balance significantly increases life satisfaction in a positive direction (ß = 0.153; t = 2.659; p = 0.008). A one-unit increase in work-life balance leads to an approximate increase of 0.204 units in life satisfaction scores. A low positive correlation was found between compassion fatigue and work-life balance (ß=0.153). The regression coefficient of the model falls between 0.053 and 0.355 at a 95% confidence interval. The Durbin-Watson value was 1.781, indicating no autocorrelation issue in this model.
Discussion
This study provides significant insights into the relationships between compassion fatigue, work-life balance, and life satisfaction among healthcare professionals, illuminating the professional and emotional challenges they encounter. The findings indicate that compassion fatigue negatively impacts life satisfaction, while components of work-life balance have both positive and negative effects on life satisfaction. Specifically, the subdimensions of compassion fatigue—secondary trauma and occupational burnout—have emerged as critical factors affecting the life satisfaction of healthcare workers.
Secondary trauma arises when individuals in empathy-driven professions internalize the traumas of those they serve, leading to emotional exhaustion.40,41 It has also been concluded that secondary trauma reduces life satisfaction.17,18 However, contrary to the general trend in the literature, this study did not find a significant relationship between secondary trauma and life satisfaction. The absence of a significant effect of secondary trauma on life satisfaction in this study may be explained by both sample characteristics and cultural-contextual factors. A considerable proportion of the participants had a university education, most had more than five years of professional experience, and the majority were concentrated in the 26–35 age group. These characteristics may have contributed to perceiving traumatic events as an inherent aspect of the profession and to the development of more effective coping strategies. In addition, the fact that more than half of the participants were married may have strengthened family support, thereby helping to maintain life satisfaction. In the Turkish context, strong family ties, robust social support networks, and the role of spiritual values in coping processes, together with collegial solidarity among healthcare professionals, can be considered cultural and contextual protective factors that limit the negative impact of secondary trauma on life satisfaction.
On the other hand, occupational burnout has emerged as another important factor negatively affecting life satisfaction. This study demonstrated that occupational burnout adversely impacts the life satisfaction of healthcare workers. In a study conducted by Uchmanowicz et al. (2019) on nurses and midwives, it was noted that life satisfaction prevented participants from experiencing occupational burnout. 9 In another study conducted with nurses, participants with moderate levels of life satisfaction were reported to have high levels of occupational burnout. 42 A study conducted with healthcare workers indicated a negative relationship between life satisfaction and burnout. 43 Similar to the results of this study, the general trend in the literature suggests that occupational burnout reduces life satisfaction.44,45
In line with our research findings, the study conducted by Yaman and Özdelikara (2023) with oncology and palliative care nurses revealed a negative relationship between compassion fatigue and life satisfaction. 23 Similarly, the study by Yılmaz and Üstün (2018) indicated that compassion fatigue emerged as a critical factor affecting the life satisfaction of healthcare workers. 46 However, some studies have concluded no significant relationship between compassion fatigue and life satisfaction. 24
Work-life balance was another variable examined about life satisfaction. The positive relationship between work-life balance and life satisfaction emerged as a significant finding. Subdimensions such as positive work-to-life impact and positive life-to-work impact were observed to enhance life satisfaction, while negative work-to-life impact decreased it.
A wide array of studies in the literature support our research findings. In the study conducted by Milutinovic et al. (2022), it was stated that the negative aspects of work life influence life satisfaction. 17 Similarly, Johar (2023), in his study with employes in the education sector, emphasized a significant and positive relationship between work-life balance and life satisfaction. 47 The study by Cain et al. (2018) also revealed that the presence of a positive work-life balance plays a critical role in achieving life satisfaction. 48 Noda's (2020) research conducted in OECD countries showed that work-life balance contributes to improving life satisfaction. 49 Similarly, Best and Chinta (2021) identified work-life balance as an important predictor of life satisfaction.50,51 The study by Khurshid et al. (2023) also highlighted the impact of work-life balance on life satisfaction.52,53 Additionally, the results of the study conducted by Diani and colleagues (2024) showed that individuals with high work-life balance also had high levels of life satisfaction.54,55 In the current study, the model explained 12.5% of the variance in life satisfaction (R2 = 0.125), which indicates a relatively modest explanatory power. Thus, while the findings are statistically significant, they should be interpreted with caution, and future research should consider additional factors that may more comprehensively account for life satisfaction.
These findings indicate that individuals who achieve a balance between work and personal life tend to have higher levels of overall happiness. The overall findings of the study highlight the necessity of interventions at both individual and institutional levels to enhance the life satisfaction of healthcare workers. Developing targeted programs to manage compassion fatigue and work-life balance is a critical need in this context. Future research is recommended to support the relationships among these variables through larger sample sizes and longitudinal designs. Additionally, conducting similar analyses across different professional groups would increase the generalizability of the findings. By examining compassion fatigue and work–life balance within a unified framework, this study uniquely contributes to understanding the determinants of healthcare professionals’ life satisfaction.
Limitations
The use of a convenience sampling method in this study introduces certain limitations. Since the participants were selected on a voluntary basis from a single university hospital, the generalizability of the findings to other healthcare institutions or different regional contexts is limited. Additionally, the sample group included both clinical staff directly involved in patient care (e.g., nurses, physicians, health technicians) and healthcare professionals with the same qualifications who serve in administrative roles within the hospital. Although these individuals possess medical knowledge and experience, the stressors and workload associated with administrative positions may differ from those experienced by clinical staff due to the nature of their job responsibilities. This variation may lead to non-homogeneous effects on the studied variables, and therefore, the findings should be interpreted with caution. Another limitation concerns the explanatory power of the model. Although the model revealed statistically significant results, it accounted for only 12.5% of the variance in life satisfaction (R2 = 0.125), indicating a modest level of explanatory capacity. This suggests that additional psychological, organizational, and contextual factors not included in the present model may also influence life satisfaction. It is recommended that future research utilize probability sampling methods covering broader and more diverse healthcare institutions. The lack of occupational distribution data in the study constitutes another limitation of the research. The inability to collect this data has made it impossible to compare variables such as compassion fatigue, work-life balance, and life satisfaction according to occupation. It is known that the compassion fatigue variable is significantly influenced by the individual's occupation. Moreover, an individual's profession has the potential to positively or negatively affect their life satisfaction and work-life balance.
Conclusion
This study reveals that compassion fatigue and occupational burnout significantly diminish life satisfaction among healthcare workers, while work-life balance contributes positively.
To enhance employe well-being and care quality, organizations should:
Implement emotional support and stress management programs, Offer flexible and balanced work arrangements, Strengthen social support systems in the workplace.
These targeted interventions can help promote a healthier, more sustainable working environment in healthcare settings.
Footnotes
Author note
This manuscript has undergone professional English language editing to improve fluency and clarity.
Acknowledgements
List all contributors who do not meet the criteria for authorship, such as technical assistants, writing assistants or head of department who provided only general support.
Ethical considerations
Ethical approval for this study was obtained from the Social and Humanities Ethics Committee of Kahramanmaraş Sütçü İmam Universtity Rectorate (Report No. E-282439. dated 26.01.2024). Additionally, permission was obtained from the Chief Physician of the Healthcare Practice and Research Hospital to conduct the study.
Informed consent
Prior to data collection, all participants were verbally informed about the purpose, scope, and procedures of the research during face-to-face interactions. Additionally, a written information statement was provided on the first page of the questionnaire. Participants proceeded with the survey only after confirming their willingness to participate, and informed consent was obtained accordingly.
Authors contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data collected in this study were analyzed in accordance with ethical approval and with full protection of participant confidentiality. The data were systematically gathered to support the study's findings and have been used solely for scientific purposes. If necessary or upon request, the data can be shared with the editor and/or reviewers. Such sharing will be conducted strictly within the scope of the academic review process and in compliance with data confidentiality principles.