
Abstract
Background
Health professionals are at increased breast cancer(BC) risk. Occupational factors are likely contributory, especially nightwork. Return to work for women with BC has received much attention. However, systematic review of return-to-work among health professionals with BC is lacking.
Objective
To perform systematized review of the return-to-work literature on health professionals with BC.
Methods
PRISMA and ENTREQ guidelines were followed, searching PUBMED, CINAHL, PsycINFO and Web-of-Science.
Results
From 2242 publications, 33 primarily qualitative studies addressed return-to-work among health professionals with BC. Fourteen return-to-work studies included some health professionals with BC. Ten studies addressed return-to-work among health professionals with cancer; 264 of whom had BC. Of nine case-studies/self-reports of health professionals with BC, seven worked within oncology. Occasionally-mentioned baseline working conditions included long workhours, nightshifts and busy schedules/multi-tasking. Particular concerns regarding chemotherapy for health professionals were infection risk, fatigue, cognitive function and appearance, the latter often impacting BC disclosure to patients. Emotional burdens when confronting patients’ health problems while afflicted with BC were highlighted. Occasionally-implemented modifications with return-to-work were shortened workhours, nightwork elimination, modified duties or job change. Salutogenic developments with return-to-work included emotional rewards: feeling needed and enhanced sensitivity/empathy for patients with cancer. Issues surrounding the initial BC diagnosis were very delicate for health professionals. Three oncology nurses with BC were diagnosed with post-traumatic stress disorder.
Conclusions
Much more attention should be directed to the occupational needs as well as potential contributions of health professionals with BC. Participatory action research should guide intervention studies aimed at identifying the healthiest RTW options for this special cohort.
Keywords
Introduction
Health professionals are at increased risk of breast cancer (BC).1,2 A number of occupational exposures may heighten their BC risk. Among these are ionizing radiation and nightshift work; for example, investigations conducted primarily among nurses indicate a significant association between prolonged exposure to nightshift work and BC risk.3,4 For nurses who were overweight or had work-related effort reward imbalance (ERI), years of nightshift work were linked to increased age acceleration. 5 The latter has been related to elevated BC risk. 6 Compared to nurses working only day shifts, those who permanently worked nightshifts were found to have shorter sleep duration and greater sleep debt. 7
The emotional burden experienced by health professionals, as well as ERI, deleteriously impact sleep. 8 Among physicians, the total work stressor burden, as assessed by the Occupational Stressor Index (OSI), has been significantly associated with poor overall sleep quality (Pittsburgh Sleep Quality Index ≥ 6). 9 There is some evidence that short sleep duration, as well as poor or irregular sleep, are linked to heightened BC risk.10,11
As the most frequently-diagnosed malignancy among women worldwide, 12 BC is often detected and treated during paid-employment years. 13 Overall, continued employment appears to favorably impact well-being among women who have been diagnosed with BC.14–16 Return to work (RTW) for women with BC has received much attention.13–30
Among the abiding themes that arise in relation to RTW for women with BC is the apparent benefit of implementing at least one modification in working conditions, with decrease with work hours being most frequent. 21 On the other hand, heavy self-rated workload is reportedly a negative predictor of RTW during BC treatment. 18 Knowledge regarding employment rights and entitlements, as well as social support have been emphasized as important for women with BC.16,24–26 Cognitive limitations, fatigue and changes in appearance are particularly important RTW issues during and after BC treatment.13,24,25,31 A pilot randomized controlled trial from Scotland indicates that case management vocational rehabilitation was associated with 53 fewer days of sick leave during the first 6 months after BC surgery for seven women compared to 11 women who did not receive this service. 17 In studies among patients treated for BC as well as other malignancies, the importance of supervisors’ support for promoting sustainable, satisfying RTW experiences has been demonstrated. 32
Notwithstanding helpful insights such as these, Porro and colleagues 33 emphasize the need for “a better understanding of the RTW process…in order to propose appropriate interventions aimed at facilitating the RTW of [survivors of BC] and its sustainability” (p. 591). According to the Expert Panel tackling this question, a detailed consideration of the work environment, including professional status is essential. 33 In light of their heightened risk, the question arises: What is the state of the knowledge regarding RTW among health professionals with BC? We aim herein to systematically address this question. This becomes a particularly urgent priority given the stressful work conditions faced by health professionals.
Methods
The Preferred Reporting Items for Systematic reviews and Meta-Analyses literature search extension (PRISMA-S) 34 guidelines were followed, with further insights gleaned regarding qualitative studies via ENTREQ (Enhancing transparency in reporting the synthesis of qualitative research) 35 and regarding systematized review via Ref. 36 Ethics committee approval was not required since the present study is a systematized review of published material.
Eligibility criteria
Studies addressing RTW among women with BC were potentially eligible, insofar as health professionals of any profile were explicitly included. Breast cancer could have been at any stage and with any treatment. Return-to-work needed to have been addressed in some way in the publication. There was no restriction as to research design; narrative studies, including case- or self-reports were considered. Only full length publications (journal articles or books) were included, with no limitations regarding date of publication nor language.
Search strategy
Comprehensive searches of the literature were carried out between mid-December 2024 and mid-March 2025 by the first author, with replication by the second author. The authors consulted librarian experts in systematic reviews at their institutions regarding the choice of search terms and strategy. The data bases used for the searches were: PUBMED, CINAHL, PsycINFO and Web of Science. Three search strategies were employed:
(Physicians OR Doctors OR Clinicians OR Nurses OR Physical Therapists OR Occupational Therapists OR Midwives OR Respiratory Therapists OR Health Professionals) AND (breast cancer) AND (self-disclosure) AND (work) (Physicians OR Doctors OR Clinicians OR Nurses OR Physical Therapists OR Occupational Therapists OR Midwives OR Respiratory Therapists OR Health Professionals) AND (breast cancer) AND (return to work) (Physicians OR Doctors OR Clinicians OR Nurses OR Physical Therapists OR Occupational Therapists OR Midwives OR Respiratory Therapists OR Health Professionals) AND (breast cancer) AND (work conditions)
The authors’ own reference lists and other sources, including within the identified references, were also examined.
Screening procedure/inclusion
All procedures were performed directly by the authors without any extrinsic software. After omission of duplicates, the title and then abstract of each reference were examined to assess whether or not BC and RTW were likely to have been addressed. After excluding studies that did not fulfill these criteria, the entire full text of each reference was scrutinized. This procedure was detailed, multi-faceted and iterative. The key was to identify studies in which health professionals were explicitly included as patients with BC, i.e., not only care providers. The entire full text of each reference was examined independently, at least twice. Next, the empirical publications on BC and RTW that included health professionals as patients were further scrutinized at least twice. At that step, the question was whether or not there was actual information about the included health professionals. Studies were excluded insofar as work-related information (other than the most basic, such as job category or job title) was lacking about the health professionals.
Approach to evaluating the included studies
The focal point for all the included studies was to glean as much information and insight as possible about the health professionals with BC, emphasizing work-related issues, within a clinical framework. This too was an iterative process, by which three study categories were first distinguished. These were: (1) Publications addressing RTW after BC in which some of the participants were health professionals, (2) Publications addressing RTW among health professionals with BC or other malignancies and (3) Case reports/ self-reports of health professionals with BC.
For all three study categories the following data were extracted. Firstly, publication year and country in which the investigation was performed were recorded. Next, the available oncologic data were compiled. Baseline work conditions/job stressors were reviewed when available, followed by issues of direct relevance to RTW. Then the actual data regarding RTW, especially the timing vis-à-vis initial BC diagnosis were noted. In relation to RTW, it was also noted whether or not the health professional(s) disclosed their BC diagnosis. Issues related to disclosure (or non-disclosure) were indicated, as well. Next, from the actual description, and sometimes inferentially from the narratives, we strove to assess the job stressor status with RTW, including eventual modifications in work conditions. Psychological and lifestyle issues were also evaluated as they related to BC diagnosis, treatment and rehabilitation. Further comments were made about each of the studies. The latter emphasized overriding conclusions, underscoring both the strengths as well as methodologic challenges.
Some of the steps in the data extraction procedure required adaptation according to the study category. The study design was indicated for the 1st two study categories. Self-reports versus case reports were distinguished for category 3. For reports in which there were participants other than health professionals with BC (category 1), further salient findings for the entire study group were identified. For category 2, relevant insights from health professionals with other malignancies were noted. Information regarding initial BC detection were available for categories 2 and 3. Self-treatment was described in some of the Category 2 studies of health professionals. Information about how the initial BC diagnosis was conveyed was available only among some of the self-reports (Category 3).
The authors independently evaluated each of the included studies. Areas of disagreement were resolved by in-depth discussion.
Results
As summarized in the flow chart, Figure 1, altogether 2242 publications were identified via the above-described search strategies. After removing 1042 duplicates, 1200 references were screened by title, 625 of which were deemed sufficiently relevant to review the abstract. From these abstracts, 218 references were found in which BC and RTW were addressed and whose full text was then reviewed. These are listed in alphabetical order in the Supplement. Fifty empirical publications were identified in which health professionals with BC were included as patients and RTW issues were addressed. Eleven of the 50 publications lacked any further information about the health professionals and were excluded. Each of the 11 excluded papers is marked in the Supplement.
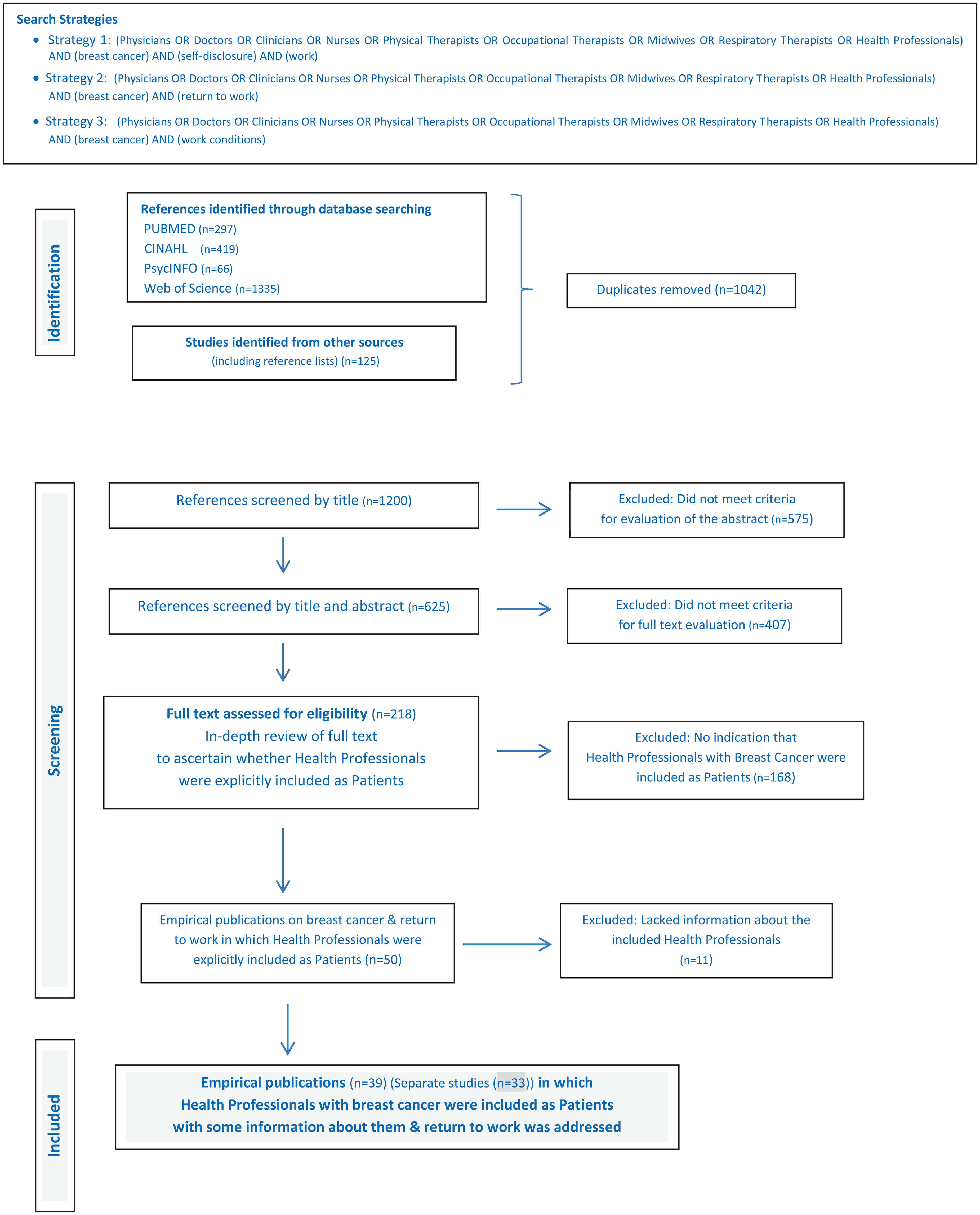
PRISMA flow chart for selection of studies addressing return to work among health professionals with breast cancer.
Altogether 39 publications from 33 separate studies were identified in which RTW among health professionals with BC were explicitly included, with at least some information about the health professionals and their work-related issues. These are divided into three tables, each arranged in chronological order. Table 1 contains publications in which health professionals were participants in a larger study addressing RTW after BC. Publications explicitly focusing on health professionals with cancer including BC, are presented Table 2, while case studies and self-reports of health professionals with BC are in Table 3.
Studies of return to work for patients with breast cancer in which health professionals are explicitly included among the care recipients.
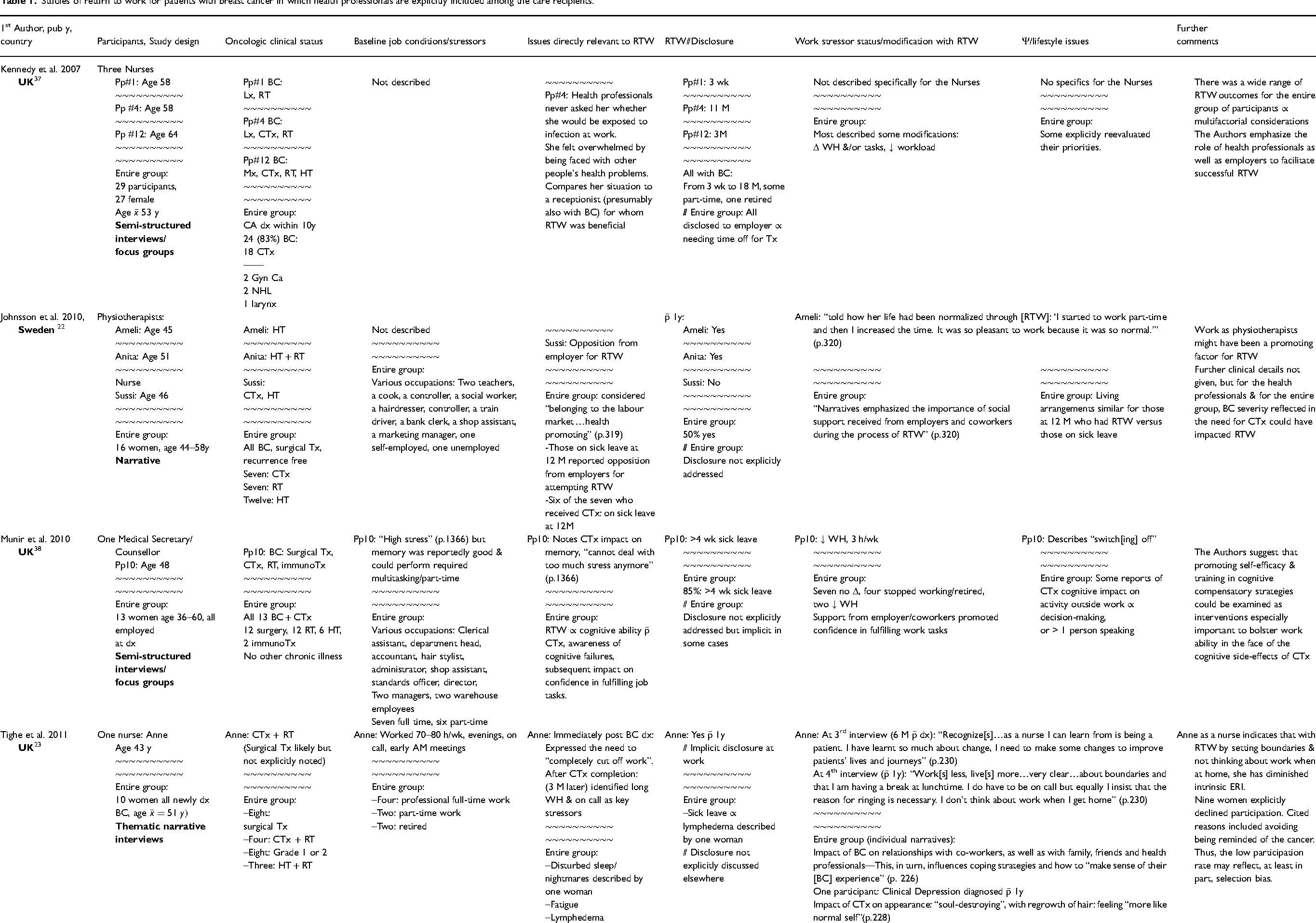
BC = breast cancer, CA = cancer, CRC = colorectal cancer, CTx = chemotherapy, D = day(s), DAL = dominant arm lymphedema, DASH = Disabilities of the Arm, Shoulder and Hand, dx = diagnosis/diagnosed, ERI = effort reward imbalance, Gyn = gynecologic, h = hours, HCW = Health Care Worker, HT = hormonal therapy, hx = history, immunoTx = immunotherapy, IQR = interquartile range, Lx = lumpectomy, M = month(s), MD = physician, MET = metastatic disease, Mx = mastectomy, Neoadj = neoadjuvant, NHL = non-Hodgkin's lymphoma, NL = Netherlands, Pp = participant, pub = publication, ROM-T = range of motion test, RT = radiation therapy, RTW = return to work, SE = side effects, Tx = treatment/treating, UK = United Kingdom, U.S. = United States of America, WH = work hours, wk = week(s), y = year(s),
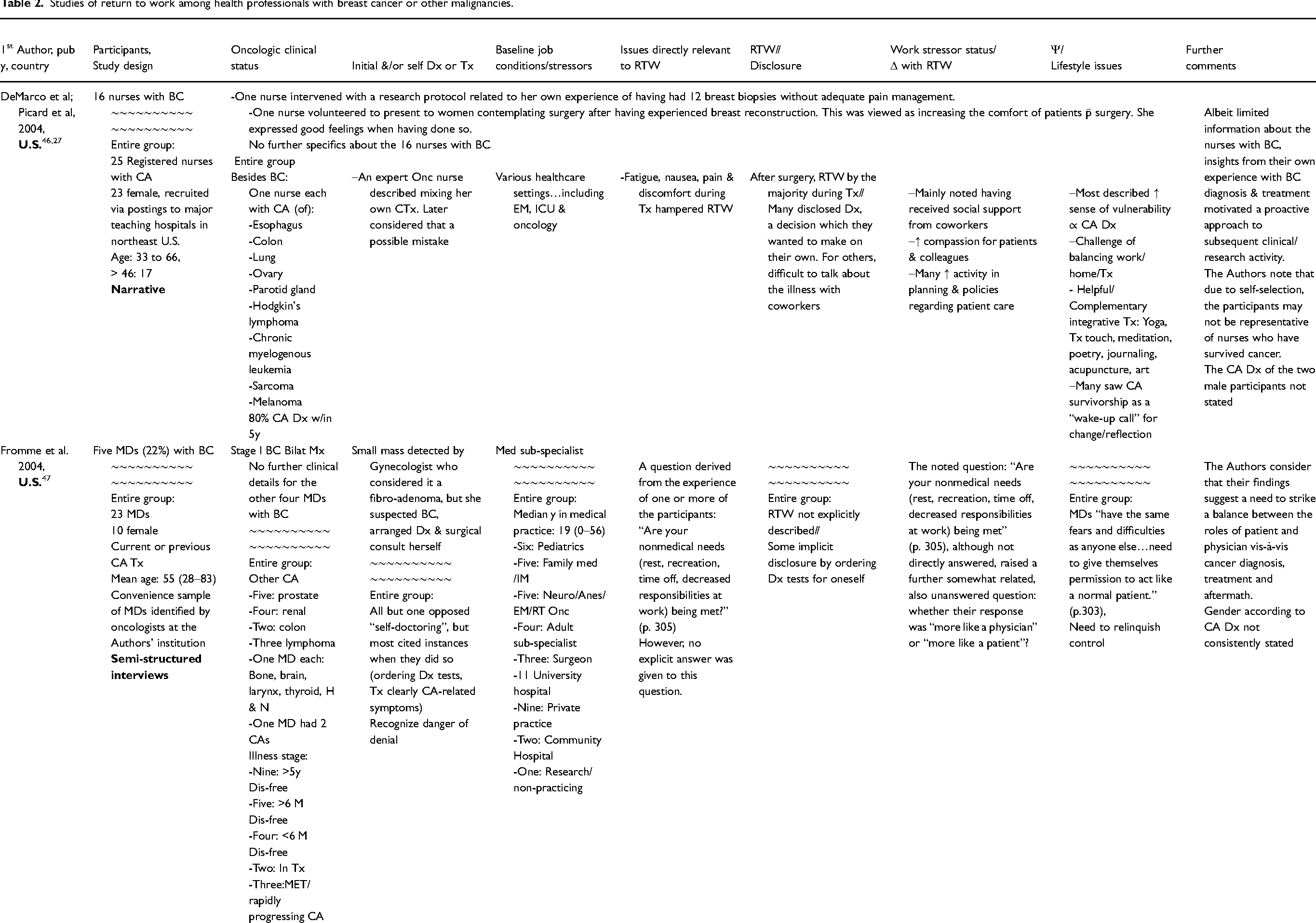
Studies of return to work among health professionals with breast cancer or other malignancies.
Statistical significance * p < 0.05, ** p < 0.01*** p < 0.001.
Anes = Anesthesia, BC = breast cancer, Bilat = bilateral, CA = cancer, CRC = colorectal cancer, CTx = chemotherapy, Dis = disease, Dx = diagnosis, diagnosed, EM = emergency medicine, Gyn = gynecologic, HCW = health care workers, H & N = head & neck, HT = hormonal therapy, ICU = intensive care unit, IM = internal medicine, LE = lymphedema, Lx = lumpectomy, M = month, MD = physician, Med = Medicine/medical, MET = metastatic disease, MM = mammogram, Mx = mastectomy, Neuro = Neurology, NHS = National health service (UK), NS = statistically non-significant, OH = occupational health, Onc = oncology, P = participant, QNWL = quality of nursing work life, RT = radiation therapy, RTW = return to work, SE = side effect, Tx = treatment/treating, UE = upper extremity, UK = United Kingdom, U.S. = United States of America, WE = work environment, WH = work hours, y = year, Δ = change, Ψ = psychological,
Case reports & self-reports of health professionals with breast cancer.
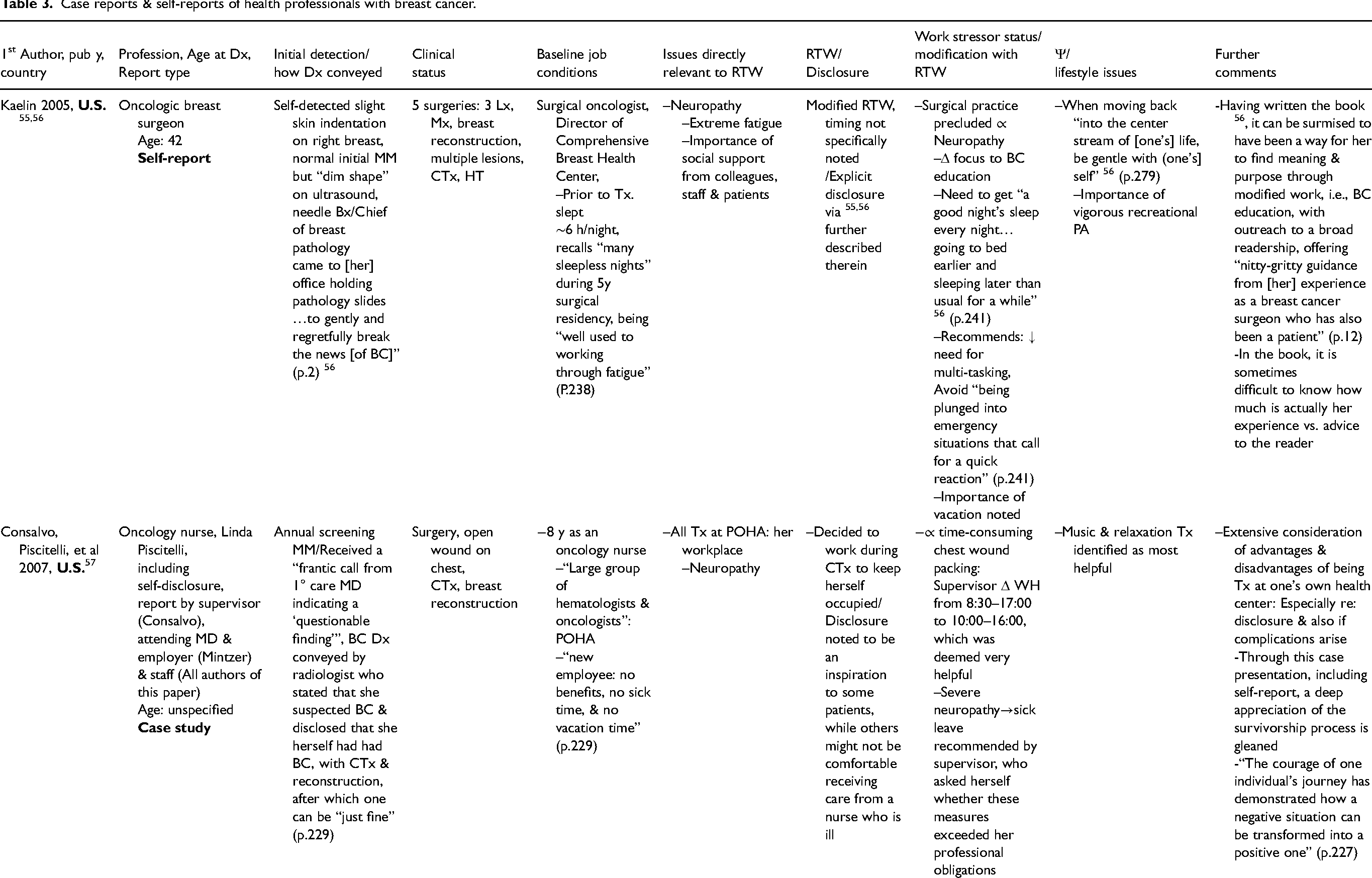
Admin = administrative, BC = breast cancer, Bilat = bilateral, BMI = body mass index, Bx = biopsy, CA = cancer, CBT = Cognitive/behavioral therapy, CTx = chemotherapy, Dx = diagnosis, EM = emergency medicine, ERI = effort-reward imbalance, exam = examination, FHx = family history, f/u = follow-up, HT = hormonal therapy, Hx = hysterectomy, ICU = intensive care unit, LE = lymphedema, Lx = lumpectomy, MD = physician, MET = metastatic disease, MM = mammography, Mx = mastectomy, OSI = Occupational Stressor Index, PA = physical activity, PMHx = past medical history, POHA = Pennsylvania Oncology Hematology Associates, PTSD = post-traumatic stress disorder, recur = recurrence, RT = radiation therapy, RTW = return to work, STAR = Survivorship Training and Rehabilitation, TAV = threat avoidant vigilance, Tx = treatment/treating, U.S. = United States of America, WH = work hours, w/in = within, wk = week(s), y = year(s), Δ = change, Ψ = psychological,
Studies of RTW among women with breast cancer, of various occupational profiles, including health professionals
Table 1 presents the 14 separate studies of RTW among women with BC, in which some of the participants were health professionals.16,22–26,37–45 Most of these studies were various types of small-scale narrative interviews, in which nurses, physiotherapists, physicians and/or health professionals of other (or undefined) profiles were included. Oncologic treatment of the interviewed health professionals was varied, but, in addition to surgery, many received chemotherapy. Relatively little was reported regarding their baseline working conditions, except occasional mention of work hours (often long), nightshift work and busy schedules/need for multi-tasking.23,24,38,41,42 Particular concerns for health professionals vis-à-vis RTW that arose regarding chemotherapy included infection risk, 37 fatigue,41,43 impact upon cognitive function24,38 and upon appearance.25,42 The latter was a sensitive issue often linked to disclosure of BC, especially to patients. 25 Shorter work hours, nightshift work and/or taking proper breaks for meals became explicit issues with RTW for some of the nurses23,24,39,41 and one of the physicians. 26 The emotional burden of dealing with patients’ health problems while being afflicted with BC was also poignantly expressed. 37
Some salutogenic developments could also be identified among the health professionals with RTW. These included asking colleagues for help e.g., with challenging clinical procedures. 25 One nurse stated that she had learned a great deal by being a patient. With RTW, she was better able to set boundaries, avoiding over-involvement outside work hours, i.e., reducing intrinsic ERI. 23 One physiotherapist considered gradually implemented RTW as having helped normalize her life. 22 Presumably BC had been detected at an early stage for this physiotherapist, since besides surgery, she received only hormonal therapy. However, further clinical details were not described in her case. Both physiotherapists participating in 22 resumed work at 12 months. Satisfaction associated with their specific job profile may have helped promote RTW.
For all the participants included in these studies, a key finding regarding RTW was the importance of work-place social support. Both instrumental and emotional support from supervisors and co-workers were repeatedly cited. Concordant with that support was the implementation of various workplace modifications. The most frequent of these were changes in job tasks and work hours/schedule. Of particular importance, often in direct relation to the latter, was the allocation of needed time for treatment/medical appointments. Some specific ergonomic modifications were described,26,44 especially in relation to special needs. Among these were work station adaptations, reportedly associated with high satisfaction for women with upper limb lymphedema. 44
Among 73 women whose BC treatment included axillary lymph node dissection and mastectomy, RTW at three months was reported to be nearly 50%. However, the percentage was notably lower among the “care workers” (36%). 45 The impact of upper limb lymphedema on work-related activity was substantial for many health professionals, especially if the dominant arm was involved. 44
Studies of health professionals with breast cancer and other malignancies
Ten separate studies were identified addressing RTW among a series of health professionals with cancer and in which BC was the diagnosis for at least some of the participants 27–29,46–54 (Table 2). Of these, BC was the sole diagnosis in three publications.28,52,54 In the following studies: 27,29,4650,–53 only nurses were included, whereas only physicians were included in reference. 47 Nurses and physicians were participants in, 54 whereas various categories of health professionals were listed in.28,48,49 Most of the studies were of female health professionals exclusively, whereas the majority of the participants were male physicians in. 47 Two male nurses with malignancies other than BC were included in.27,46
Altogether, 264 health professionals with BC were participants in the studies summarized in Table 2. Limited oncologic detail can be gleaned about them. Lumpectomy was the cited surgical treatment for two nurses, 29 while ten physicians and 14 nurses had undergone mastectomy.47,52,54 Explicitly, four health professionals had Stage 1 BC, four had Stage 2 and three had Stage 3 BC.47,49 Distant metastases (Stage 4) were documented among 11 of the 117 health professionals with BC included in. 28 Chemotherapy was received by 82 (70%) of the participants in 28 and four of the five nurses with BC in. 52
The initial BC diagnosis can be particularly sensitive for health professionals. This issue and related topics are addressed in column 4 of Table 2. Three nurses were directly informed by a physician,29,52 with an emotional reaction described in one case. 52 Another health professional self-detected nipple indentation, but due to denial, delayed the actual BC diagnosis. 48 On the other hand, a medical sub-specialist who was told by her colleague that a small breast mass was benign, pursued the subsequent diagnostic workup herself. She underwent bilateral mastectomy for Stage I BC. 47 A radiologist reportedly examined the film herself, noting that the Stage I BC was associated with a very favorable prognosis. 49
Small-scale narrative interviews predominated for the studies included in Table 2, as was the case for those in Table 1. Except for some mention of job title, length of employment and setting, compared to the studies presented in Table 1, even less was reported about the baseline working conditions of the health professionals with BC or other malignancies. Only one study 53 referred to nightshift work at baseline, noting that this was the case for some of the 17 nurses with various malignancies. Nearly 100% RTW, sometimes gradual, was reported in the three studies28,52,54 in which only health professionals with BC were included. In the two of those publications based on qualitative analysis,52,54 fatigue and cognitive deficits were major concerns, while social support as well as financial considerations reportedly promoted RTW.
Some changes in work conditions with RTW were reported in,28,52–54 most frequently shortened workhours, elimination of night work and change in duties, with actual change in jobs occasionally reported. While colleagues covered for difficult tasks, they sometimes complained about the extra burden. 52 In a larger study from South Korea, the overall quality of nursing working life after RTW was reportedly the lowest among nurses with BC compared to nurses with other malignancies.50,51 Concern about workplace exposure to COVID-19 was noted in the most recent studies.52–54
Upper extremity problems were cited in,28,48,52 with the need to wear an elastic glove, necessitating BC disclosure to patients. 52 A health professional with BC and lymphedema in the UK study 48 reportedly faced job loss since long sleeves were not permitted, while restricted arm stretch impacted her ability to place a drip bag for intravenous treatment.
Among the emotional rewards of RTW for health professionals with BC were the feeling of being needed and enhanced sensitivity/empathy for patients with cancer.29,49,54 A patient's explicit expression of gladness when a nurse with BC returned was particularly poignant. 52 Deeper insights and appreciation of the potential contribution to helping patients with cancer was likewise reflected among the health professionals with various malignancies.27,46,48,49,53 However, further work with patients afflicted with cancer, particularly end-stage disease, could also trigger adverse emotional responses.48,49,53 Disclosure of a cancer diagnosis to patients, coworkers and supervisors was a very personal decision, as well as being impacted by cultural considerations, with some health professionals opting to refrain.27,29,46,48–51,53 In some cases, the latter precluded implementation of needed workplace modifications. 29
Case studies/self-reports of health professionals with breast cancer
Nine published case studies/self-reports of female health professionals with BC were found.30,55–65 Among these, seven health professionals worked within some aspect of clinical oncology,55–62,64,65 including surgery,55,56 rehabilitation61,62 and primary care of patients with cancer 64,65 (Table 3). Six of these reports were from nurses,30,57–60, 63 while three were from physicians.55,56,61,62,64,65
The three physicians55,56,61,62,64,65 and one of the nurses 63 initially self-detected a breast change, whereas BC was found during screening mammography for two oncology nurses.57,60 While the initial diagnosis of BI-RADS V (Breast imaging-reporting and data system) was conveyed in a sealed envelope for one of the nurses, 63 personal communication was reported for the BC surgeon 56 and for one of the oncology nurses. 57 In the latter case, 57 a radiologist who, herself, had undergone extensive treatment for BC provided explicit encouragement that after treatment one can be “just fine” (p.229).
Although the full clinical details were not usually reported, all but two of the cases involved health professionals with BC who had undergone mastectomy and/or chemotherapy.60,64,65 Upper extremity complications were described in three cases: axillary web syndrome 64 and upper arm lymphedema.30,59 In addition to BC, one of the oncology nurses was also treated for ovarian cancer. 58 She, as well as two of the other oncology nurses,59,60 reportedly suffered Post-traumatic stress disorder (PTSD) in association with the BC diagnosis and treatment. The physician rehabilitation specialist reported disturbed sleep, but not full-blown PTSD. 62
Overall, there is rather limited information about the baseline job conditions in most of these case/self-reports. Exposure to nightshift work is explicitly noted by the oncologic breast surgeon 56 and for one of the oncology nurses. 60 Another oncology nurse 57 as a new employee lacked benefits, including sickleave and vacation time. Besides clinical work, four of the health professionals also had academic and/or leadership responsibilities.55,56,58,61–63 A detailed assessment of baseline job stressors was provided for one of the oncology nurses. 60 Notwithstanding a healthy social climate at the cancer hospital where she had worked for 30 years, high demands, lifting patients, heavy threat avoidant vigilance burden, as well as some conflict and effort-reward imbalance, ERI, contributed to a total Occupational Stressor Index, OSI score of 85. The latter is nearly at the level for which urgent intervention is needed, and, as mentioned, is associated with poor sleep quality. 9
All of the health professionals returned to work in some capacity, mainly after treatment,58,59,61–63 although one oncology nurse chose to work during chemotherapy in order to keep herself occupied. 57 Extreme fatigue and/or neuropathy were reported by nearly all the health professionals who had undergone chemotherapy,55–59,61,62 while cognitive dysfunction was also reported by the oncology nurse who had incurred ovarian cancer as well as PTSD. 58
The oncologic breast surgeon,55,56 the rehabilitation physician61,62 and one of the oncology nurses 57 described some favorable aspects of disclosure to colleagues, staff and patients. This included social support.55,56 However, the need to be selective was also emphasized.57,60,64,65
For several of the health professionals, major work modifications were made in association with RTW. Due to chemotherapy-induced neuropathy, the oncologic breast surgeon was obliged to refocus her professional efforts towards BC education.55,56 An oncology nurse who had endured PTSD received help to diminish administrative tasks. Notwithstanding the gratification of helping patients with cancer, she found that listening to patients’ problems could also be overwhelming. 59 The oncology nurse who had suffered ovarian cancer as well as PTSD in addition to BC, resigned from clinical practice, turning instead to academic pursuits, although those were frequently overwhelming for her. 58 In contrast, another nurse not only returned full-time to clinical practice, but also pursued a Master's degree focusing on nurses with cancer. 63 After RTW, the primary care physician increased the number of patients with BC in her clinical practice.64,65 Several workplace modifications were made for the third oncology nurse who had suffered PTSD, lowering the total OSI score by 12.3 points. Among these modifications were a negotiated pay increase, allowing her to quit her 2nd job, thereby reducing workhours, elimination of nightshift work and diminishing administrative tasks. In addition, the occupational neuropsychiatrist recommended that she avoid working with patients suffering end-stage disease. These work-related interventions, together with cognitive behavioral therapy, reducing job over-commitment and dance as recreational physical activity plus healthy social interaction, were associated with an overall favorable outcome. She thereby garnered renewed élan towards her “lifelong commitment to fight against the scourge of cancer” 60 (pp. 214–5). The importance of attention to psychological/lifestyle issues is underscored for all the case reports of health professionals presented in this section.
Discussion
Integrative review—synthesis of the findings
In contrast to the plethora of studies on RTW among women with BC, relatively few explicitly included health professionals with BC. Regarding the latter, based on the present searches, the largest number of RTW publications were those in which some of the participants with BC were health professionals. However, this was often with little or no further information about the latter. For the 14 identified studies carried out among various occupational profiles, altogether there were at least 122 health professionals with BC about whom some work-related information could be gleaned. Regarding the 10 studies exclusively focused on health professionals, 264 participants had BC. These were among a substantially larger group of health professionals who had been afflicted with malignancies other than BC. Both males and females were included in some publications. In addition, nine case studies/self-reports of health professionals with BC were identified. For the publications devoted explicitly to health professionals with BC or other cancers, insights were limited regarding their work conditions prior to, during and after BC treatment.
Notwithstanding the lack of complete clinical data, it can be concluded that besides surgical intervention, a sizable percentage of the health professionals with BC included in this review had received chemotherapy. Major issues that arose in relation to chemotherapy included extreme fatigue, neuropathy, infection risk, cognitive dysfunction and impact on appearance. The latter was particularly delicate vis-à-vis disclosure to patients and to others in the healthcare work environment. With RTW numerous shorter and longer-term modifications were made due to chemotherapy. Perhaps the most dramatic was the need to completely redirect clinical practice from surgery to medical education because of chemotherapy-induced neuropathy.55,56 Physiotherapy and other non-pharmacologic strategies are being investigated to counter chemotherapy-induced peripheral neuropathy 66,67. If successful, such measures could help preserve the work capacity of affected health professionals, especially nurses, surgeons and other physicians who perform invasive procedures.
Lymphedema and/or other upper arm problems were also an issue specifically for the health professionals with BC in many of the studies.23,28,30,44,45,48,52,59,64,65 On the one hand, work-station modifications were reported to be helpful for employed women with BC-related upper arm lymphedema.26,44 On the other hand, lack of appreciation of the special RTW needs of nurses associated with this BC-related complication was also reported.30,48 A particular challenge was related to the increasingly-applied “bare below the elbow” (BBE) policy, aimed at reducing nosocomial infections. 68 Efforts are ongoing to find solutions for health professionals who for cultural-religious reasons are conflicted by BBE policy. 69 Such solutions could be helpful, as well, for health professionals with upper arm lymphedema. At the same time, strides made to optimize axillary management hold promise to minimize upper arm lymphedema as well as BC recurrence. 70
The 24-year “journey” traversed by a nurse with BC-related lymphedema provides further insights into this complex problem. 30 Her working conditions at baseline had been intense. As a school nurse and counselor, she was responsible for up to 100 children per day, with many additional duties. Apparently, she continued to work in that capacity for some time after the occurrence of lymphedema, although several subsequent job changes were also described. 30
With a few other exceptions, very limited information is available concerning the baseline working conditions of the health professionals with BC. This hinders adequate assessment of RTW, including considerations of job stressors that may have contributed not only to the increased BC risk at that time, but that may also impact risk of BC recurrence. A particular weakness was the lack of attention to nightshift work. Altogether only seven of the 33 separate studies included in this review addressed diminution or avoidance of nightshift work with RTW in some way.24,50–54,56,60
As noted, a link between nightshift work and sleep deficiency has been demonstrated among nurses. 7 The prevalence of severe insomnia, as well as overall PTSD symptoms, was substantial among health professionals working nightshifts in a study carried out in public hospitals during the COVID-19 pandemic. 71 The relation between PTSD and the cancer experience is well-recognized. 58 These considerations warrant attention for health professionals with BC, who may well be vulnerable to PTSD, and for whom attention to nightshift work could be an important component of interventions aimed specifically at improved sleep with RTW.
Another stressor, particularly salient for clinical work within oncology, is the emotional challenge of providing care for patients with advanced and/or endstage disease. 72 Distress in this regard was articulated by health professionals in some of the studies included in this review.48,49,60 For one of the oncology nurses, 60 given the presence of PTSD, including recurrent nightmares about patients with metastatic and terminal outcomes, the occupational neuropsychiatrist recommended that she avoid work with patients suffering endstage malignancy. Such an intervention could be an option, at least temporarily, in selected cases.
Post-traumatic stress disorder was explicitly diagnosed only in three of the case studies included in this review.58–60 More attention to the possibility of PTSD is warranted among health professionals with BC or other malignancies who provide care within oncology. Their emotions can be triggered as they over-empathize with patients who have similar cancer experiences.
On the other hand, continued clinical work, including within cancer care, was often a source of gratification. Many of the health professionals gleaned new-found insights from their own BC experience, with deepened empathy which could be of benefit to their patients.23,27,29,46,49,53–57,59–65 This was also poignantly illustrated by the manner in which the radiologist who herself had undergone major BC treatment, conveyed the initial BC diagnosis to an oncology nurse. 57
In sharp contrast, was the nurse who described the “total shock” of receiving a diagnosis of BI-RADS V in “a sealed white envelope” 63 (pp. 291–292). A comparably devastating manner of receiving a diagnosis of a highly malignant tumor is described by Dr Karla Castro-Frenzel, anesthesiologist, who was informed by a surgeon via “a gut-wrenching Monday-morning phone call at work after anesthetizing [her] first patient” 73 (p. 2303). Conveying a diagnosis of BC or other malignancy to any patient is obviously exceedingly delicate, requiring the utmost sensitivity and skill. 74 At the very least, such sensitivity and skill should be applied when the recipient of the “bad news” is a health professional. It could, in fact, be that health professionals have special needs in this regard. If these are not taken into account, untoward consequences may result. Among these could even be avoidance of BC screening. Of the limited published data on this topic, it appears that health professionals are underscreened for BC.75,76 These considerations become highly salient regarding adherence to needed follow-up. As noted, fear of recurrence was expressed by a number of the health professionals with BC,49,54 particularly those working within oncology.
Dr Castro-Frenzel eloquently describes the “distinct strengths and vulnerabilities” of physicians when they become patients…due to the “inside knowledge and ability to better navigate the medical system [while also being] uniquely positioned to act as the greatest adversaries to [their] own patient-selves” 73 (p.2303). She sees “serving others” as the “most powerful strength” whereby “work can be restorative not only to patients but to our own patient-selves” 73 (p.2304). These observations would seem to apply, at least in part, to other health professionals. In terms of practical implications, one of the major themes of this review is that continuing to work can provide a vital source of meaning. Yet, the work conditions should be adapted to the needs of health professionals who have been afflicted with BC.
A particularly promising avenue could well be rehabilitation per se as part of the RTW trajectory. Several examples from the present review support this contention. Namely, the two physiotherapists with BC, Ameli and Anita, returned to their rehabilitation-related work, which was described as “pleasant…because it was so normal” 22 (p.320). Concordantly, after completing BC therapy, Dr Julie Silver resuming her work as a rehabilitation specialist, developed a program dedicated to cancer survivorship and wrote a book on that very topic. 62 Therein, Dr Silver describes the STAR program, an acronym for “Survivorship Training and Rehabilitation”, in which health professionals are appropriately trained to provide cancer survivorship care, as a “best-practices model” (p.11). 62 The importance of a multi-disciplinary team oriented to the specific vocational needs of women with BC has been underscored. Supportive services can be provided by a range of rehabilitation specialists, including physiotherapists, occupational therapists, occupational health physicians and nurses, and psychological counselors. 17 Within the rehabilitation framework, the focus could be to explore how health providers as health recipients could best return to healthier work.
An important component of such a framework should certainly be improving work-life balance, to ameliorate ERI, effort-reward imbalance. Indeed, ERI could be most clearly seen in the baseline work conditions of two of the health professionals included in this review.23,60 The intrinsic component of ERI, overcommitment, if pronounced, has been associated with increased oxidative stress markers among nurses. 77 These markers, in turn, are associated with age acceleration, 78 which, as noted, is linked to heightened BC risk. 6 Singh and colleagues 77 emphasize that in order to reduce the associated health risks among nurses, there is a “need for targeted interventions to address this intrinsic stressor, [which is] characterized by difficulty detaching from work and constant rumination” (p.6). As noted for one of the case studies, 60 shortened workhours, thereby providing more time for recreational physical activity and other healthy social interactions, were key practical ways for the oncology nurse to reduce job overcommitment, while enhancing the meaningfulness/personal rewards of her work. Concordantly, two nurses with BC who participated in a formal exercise program both returned to work. The benefits of the program in promoting RTW were acclaimed by most of the participants in the study. 39
A participatory action research (PAR) approach has been advocated to design and implement RTW interventions that are both realistic and concordant with the needs of women after BC treatment 79 . It has been emphasized that via PAR, “useful and precise knowledge” can be generated which could inform studies that are both appropriate for the target group and “logistically realistic” (p.3). Indeed, PAR would be particularly appropriate for health professionals with BC.
In examining the studies included in this review in relation to PAR, preliminary suggestions for interventions emerge. Some are based on reported individual experience. For example, from the in-depth follow-up of the 43-year-old nurse, during the course of her treatment and RTW, 23 a sharp contrast is seen. She describes the pre-BC work conditions: long workhours (70–80 h/week), night call and early morning meetings. With RTW, besides reducing workhours, she explicitly set boundaries, including the need for proper restbreaks for meals, free from unnecessary disturbances. Inadequate, interrupted restbreaks, have been shown to be associated with burnout and poor sleep among health professionals. 9 Moreover, sufficient, genuine restbreaks are among the most feasible interventions and can be coupled with health-promoting practices. 9
Reducing workhours and/or diminishing or eliminating nightshift work with RTW were reported to have been requested and/or implemented by several of the health professionals.26,28,38,52,54–57,60 Since prolonged exposure to nightshift work has been associated with BC risk among health professionals,3,4 the latter intervention warrants particular attention.
A few of the health professionals requested that other colleagues and staff “step in” with administrative and/or challenging tasks.25,52,59,60 Although sometimes eliciting complaints, 52 overall a spirit of solidarity and support was thereby promoted, an essential component of successful RTW. The special measures needed with lymphedema and other upper arm problems also merit further attention.30,44,45
Increased activity within planning, education and policies was quite often reported.27,46,54–56 This could help minimize direct contact with patients afflicted with end-stage disease, and could be particularly well integrated within the outlined rehabilitation framework.
Limitations
Nearly all the studies included in this review were observational, mainly narrative. Substantial insights can be gleaned thereby regarding RTW for health professionals with BC. However, robust conclusions cannot be made as to which RTW strategies are most effective and beneficial for this cohort.
A major challenge in conducting this review is the lack of systematic attention to the RTW needs of health professionals with BC. On the other hand, health professionals as care providers have been included in numerous studies on RTW for women with BC. These two roles needed to be “untangled”, via a multi-faceted search strategy and exhaustive examination of a plethora of publications, to finally identify a relatively small number of papers in which at least some information could be garnered on the topic.
The formalities of a systematic review could not be fully implemented. In particular, quality assessment of each study was not a suitable option. Firstly, given that the studies included in this review were primarily qualitative, as pointed out by Tong et al. 35 “Quality assessment of qualitative research is challenging and contentious” (p.6). More fundamentally, the focus of our review, especially in relation to the RTW studies included in Table 1 differed substantially from the overall aims of those studies. Thus, it would not be appropriate to formally criticize those studies for their lack attention to the specific working conditions and needs of health professionals with BC. Instead, we opted in Table 1 to glean and present the maximal amount of information about those health professionals, and also to indicate where the needed information was lacking. The larger, quantitative studies Refs.40,44,45 in Table 1, notwithstanding appropriate statistical analysis and overall methodologic rigor, generally provided even less insight into the specific situation of the health professionals with BC. There were also substantial gaps in the information provided by larger, quantitative publications included in Table 2: Refs.28,50,51 addressing RTW among health professionals with various malignancies. On the other hand, rich, multi-faceted insights were provided by many of the qualitative studies in Table 2, as well as in the case studies in Table 3. Taken together, the present review cannot fully meet the requirements of a systematic review, since formal quality appraisal cannot be carried out. The term “systematized review” is therefore more appropriate.
In the present review, none of the health professionals with BC were noted as male. Although primarily a disease of women, a small, yet growing percentage of BC occurs in men. 80 Obesity as well as occupational exposure to ionizing radiation are among the implicated risk factors for male BC. 80 A few of the studies in this review included men with malignancies other than BC,27,39,41,42,46,47 and from whom some further salient insights can be gleaned. Perhaps most notable was the overriding importance of RTW for preserving their self-image. 41
The studies that included series of patients with BC were carried out in various countries in Europe, the Middle East, the Far East and Oceania, as well as the U.S. In contrast, however, of the nine cases of female health professionals with BC, all but two explicitly worked in the U.S. Consequently, the generalizability of these case studies is limited.
Notwithstanding these challenges, the present review can be a springboard to inform further efforts to address the special needs, as well as the potentially special contributions of health providers who have been faced with breast cancer when returning to their work.
Conclusions
Insufficient attention has been given to health professionals who have been afflicted with breast cancer, BC. Special issues arise regarding their returning to work, RTW. Guidelines are vital to help oncologists, oncology nurses, occupational health physicians, occupational therapists, physiotherapists and others, who as health providers address the needs of their colleagues with BC. Job stressors that may contribute to increased BC risk warrant particular scrutiny with RTW for this cohort. A participatory action research, PAR, framework has been advocated to guide RTW strategies for patients with BC. 79 Such a PAR framework would be particularly suitable to guide intervention studies aimed at identifying the healthiest RTW options for this special cohort.
Supplemental Material
sj-docx-1-wor-10.1177_10519815251410109 - Supplemental material for Return to work for health professionals with breast cancer as health recipients: A systematized review
Supplemental material, sj-docx-1-wor-10.1177_10519815251410109 for Return to work for health professionals with breast cancer as health recipients: A systematized review by Karen Belkić and Brigitte Wilczek in WORK
Footnotes
List of acronyms
Acknowledgements
Discussions regarding search strategies and help in tracking down references were provided by Librarians at the Karolinska Institute Library and Claremont Graduate University. Special thanks to Dr Katie Kohn, PhD, STEM Librarian at the Claremont Colleges Library for her expert advice.
Ethical approval
This study was performed in accordance with the principles of the Declaration of Helsinki. Ethical approval is not required for a systematic review of published materials. No informed consent was needed to carry out this study.
Author contributions
The first author (Dr Karen Belkić) initiated the study, conceptualized the study design, performed the systematized review, interpreted the results, wrote the manuscript, approved the submitted manuscript and agrees to be accountable for all aspects of the work. The second author (Dr Brigitte Wilczek) helped initiate the study, contributed to conceptualizing the study design, independently performed the systematized review, interpreted the results, approved the submitted manuscript and agrees to be accountable for all aspects of the work. Both authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Open Access is provided by the first institute of the first author. Dr Karen Belkić has received support for her research activity from King Gustav the Fifth's Jubilee Foundation and Stockholm County Council.
Stiftelsen Jubileumsklinikens Forskningsfond mot Cancer, Stockholm läns landsting,
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets generated and/or analyzed for this study are available from the corresponding author upon reasonable request.
Dedication
The authors would like to dedicate this manuscript to our colleagues and all health professionals.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.