
Abstract
Background
Burnout is becoming increasingly prevalent among healthcare professionals where it impacts quality of care and staff turnover, especially in the wake of the COVID-19 pandemic. One promising strategy to reduce burnout is the use of mindfulness-based programs, which may aid allied health professionals (AHPs).
Objective
To explore the usefulness of a 10-week mindfulness program on reducing burnout symptoms in AHPs in Singapore, as well as to identify AHPs’ attitudes and perceptions towards adopting mindfulness in practice.
Methods
In this mixed methods study, a purposive sample (n = 8) of physiotherapists, occupational therapists, and therapy assistants were recruited. Participants underwent a mindfulness program, comprising 5 face-to-face sessions every other week for 10 weeks. Quantitative data were collected at pre- and post-intervention stages using a survey on participant characteristics and the Maslach Burnout Inventory – Human Services Survey for Medical Personnel to assess burnout symptoms. Qualitative data were collected through semi-structured interviews.
Results
There was a decrease in emotional exhaustion scores (34.50 to 25.50, p = 0.012) while depersonalization (p = 0.107) and personal accomplishment (p = 0.062) scores showed no significant changes. Qualitative benefits reported include increased introspection, improved emotional regulation and communication, and fostering of supportive workplace culture. Advocacy from superiors and the perceived effectiveness of mindfulness techniques can facilitate the adoption of the mindfulness program.
Conclusion
A 10-week mindfulness program reduced burnout symptoms, specifically emotional exhaustion, among AHPs. Future studies should explore the application of the program within a larger participant sample to develop an optimal model for feasible and pragmatic adoption within the clinical setting.
Introduction
Burnout can be understood as a psychological state of exhaustion that stems from persistent exposure to work-related stressors while lacking sufficient resources to efficiently cope with these stressors. 1 However, there has yet to be a universal definition of burnout due to the lack of conceptual clarity surrounding the term.1,2 Although burnout was first defined in the 1970s as a single dimension construct involving exhaustion, 3 burnout is now widely understood to be a multi-dimensional construct involving the combination of three distinct yet interrelated components: (1) emotional exhaustion, (2) depersonalization, and (3) a sense of reduced personal accomplishment. 4
Emotional exhaustion among healthcare professionals is characterized by a reduced capacity to experience emotions related to work, often leaving professionals feeling drained and “used up” at the end of the workday. 5 On the other hand, the second component—depersonalization—refers to feelings of treating patients as objects rather than human beings and becoming more callous towards patients. 5 The third component which constitutes a sense of reduced personal accomplishment includes feelings of ineffectiveness in helping patients with their problems and the lack of experiencing professional achievements.4,5 The relative contribution from each dimension to the development of burnout is varied and complex across individuals and thus, burnout is challenging to identify in the workplace. Importantly, if unaddressed, chronic burnout can diminish job performance and impair mental and physical health. 6
Internationally, the issue of burnout is becoming increasingly prevalent among healthcare professionals. Across Asia, Europe and the United States of America, the prevalence of burnout among physicians has been reported to be as high as 67%. 7 Aside from physicians, burnout prevalence is equally significant among other healthcare workers including nurses and allied health professionals (AHPs). 8 A meta-analysis paper reported that burnout affects around one-tenth of the global nurse population. 9 Due to the nature of their work and the clinical environment, healthcare professionals face numerous pressures including the challenges of clinical work, time constraints, competing demands, the lack of control over work processes and scheduling, and their conflicting roles and relationships with leadership. 10 These pressures were exacerbated during the COVID-19 pandemic due to an increase in workload and total working hours.11,12 As a result, healthcare professionals often experience numerous undesired consequences which include lower patient satisfaction, reduced quality of care, higher risk of medical errors, decreased mental well-being, intents to leave the profession and even suicidal thoughts.11,13–16
A prominent and effective strategy to ameliorate burnout is the use of mindfulness-based programs to reduce burnout symptoms.4,17 Mindfulness is most frequently defined as the awareness that emerges through intentionally and non-judgmentally paying attention to the experiences of the present moment. 18 Many studies have found that regular mindfulness practice helps to reduce mental health issues, and improve well-being related outcomes, emotional regulation, and relationships.19,20 However, such studies examining the impact of mindfulness have most frequently targeted nurses and physicians and have rarely targeted other healthcare professionals.17,21,22
In Singapore, a recent study indicated that healthcare workers were more stressed and burnt out during the pandemic. 12 Among the AHPs in a tertiary hospital in Singapore, 67.4% of them has reported to have experienced burnout. 8 Despite AHPs being an integral part of the Singapore healthcare system, there is currently a lack of studies that examine the use of mindfulness as a strategy to reduce or manage burnout in AHPs. Therefore, this study aims to explore the usefulness of a brief 10-week mindfulness program on a pilot group of AHPs, as well as to identify AHPs’ attitudes and perceptions towards the adoption of mindfulness in practice.
Methods
Study design
This study used a mixed method, convergent design with purposive sampling. 23 Ethical approval was obtained from Singapore Institution of Technology Institutional Review Board, Reference No. 2022043. Participants provided their written informed consent prior to the commencement of the study. Participants also provided verbal consent for the interviews to be audio recorded via the Zoom teleconferencing platform.
Participants
The target sample was identified to be a group of healthcare professionals (n = 8) from SATA CommHealth (a local community healthcare institution), comprising physiotherapists, occupational therapists, and therapy assistants in the outpatient rehabilitation department. The selected sample was heterogenous in terms of age, ethnicity, religion, educational level, work roles, and the number of years of working experience, which facilitated the collection of inclusive data. These participants were purposively selected to form a pilot group representative of the AHP population in Singapore (Table 1).
Demographic characteristics of sample.
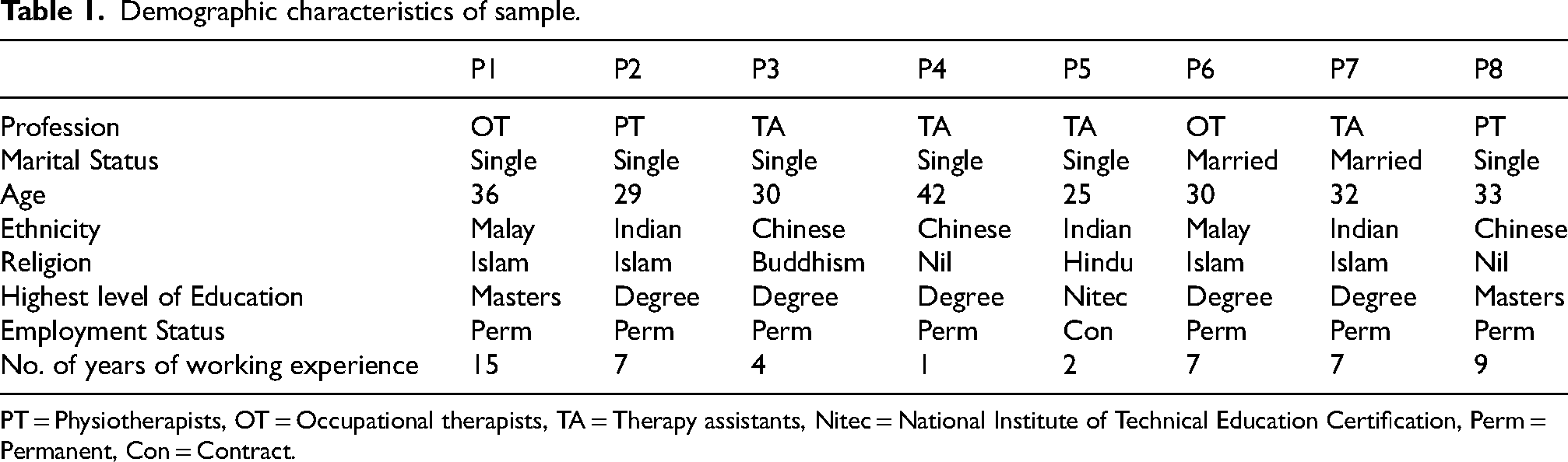
PT = Physiotherapists, OT = Occupational therapists, TA = Therapy assistants, Nitec = National Institute of Technical Education Certification, Perm = Permanent, Con = Contract.
Intervention
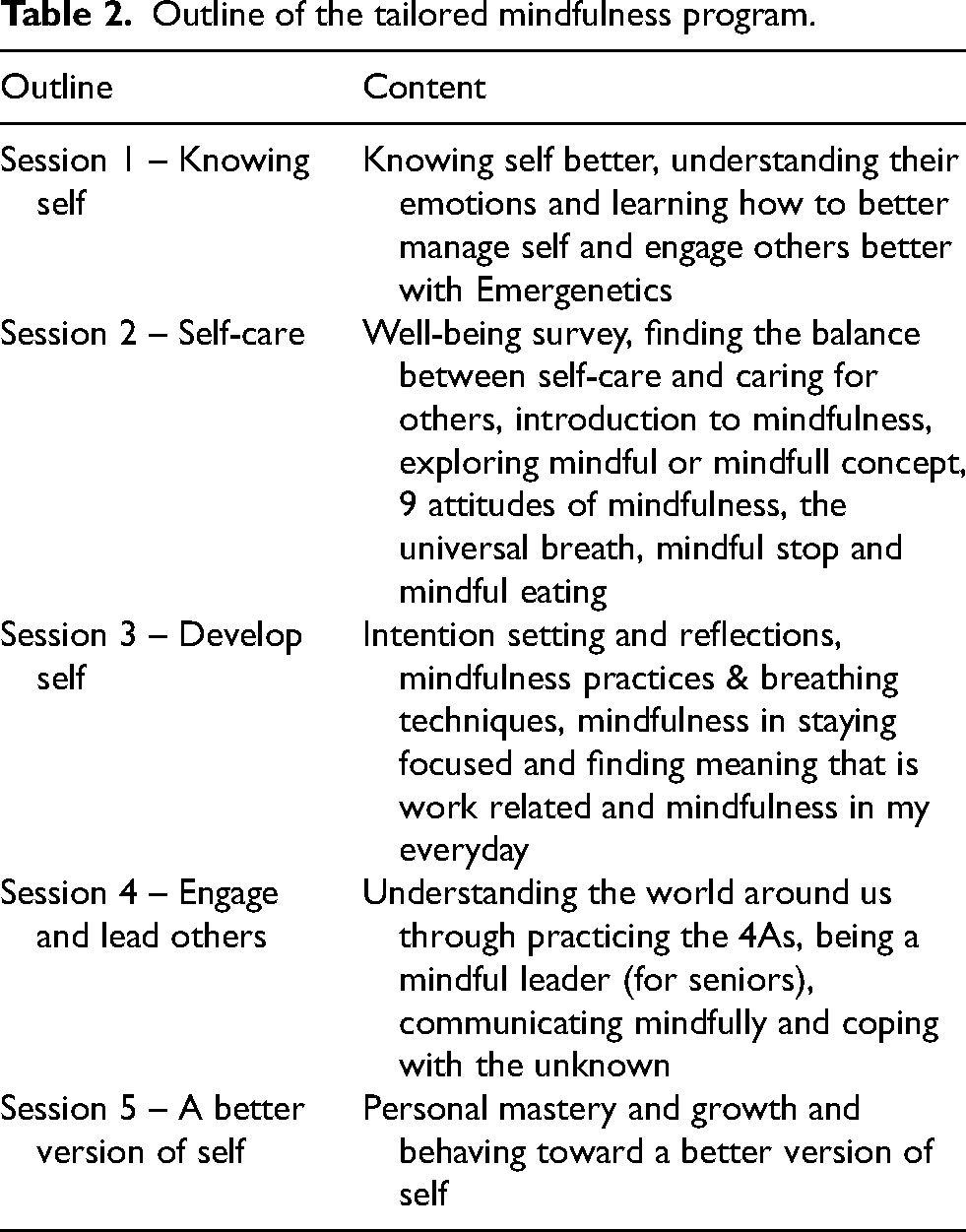
Participants underwent a mindfulness program specifically designed for rehabilitation staff and facilitated by a qualified external trainer. The program consisted of 5 face-to-face sessions conducted every other week over the course of 10 weeks. The specific topics covered during each session are outlined in Table 2. The first session was designed to be 4 h, and it utilized the Emergenetics psychometric tool (https://www.profileassessments.com/emergenetics/) to facilitate an understanding of self and others. The duration of each subsequent sessions was 3 h and participants were instructed on the concepts of mindfulness as well as mindfulness practices such as the universal breath, mindful stop and meditation. Participants were assigned into groups after each session to encourage and support one another during the program. In addition, participants were encouraged to apply mindfulness techniques in their daily lives.
Outline of the tailored mindfulness program.
Data analysis
Quantitative data
A Qualtrics survey was used to gather participant demographics and their individual responses to the Maslach Burnout Inventory - Human Services Survey for Medical Personnel (MBI-HSS-MP). MBI-HSS-MP is a validated instrument with a verified three-factor structure for assessing burnout dimensions and it has acceptable internal consistency (Cronbach's α: 0.73–0.84; McDonald's ω: 0.75–0.85) and satisfactory test-retest reliability (values between 0.70 and 0.92). 24 This survey was distributed via email to participants prior to the start of the program and immediately after the program. The main outcome measures were the changes in scores for the three MBI-HSS-MP subscales: emotional exhaustion (EE), depersonalization (DE), and personal accomplishment (PA). There are nine items under emotional exhaustion (EE), five items under depersonalization (DE), and eight items under personal accomplishment (PA). These items are rated on a Likert scale of 0 (never) to 6 (every day) on how often participants experienced symptoms. This study adopted the cut-off score to define burnout levels as EE score ≥ 27, DE score ≥ 10, and PA score ≤ 33. 7 Data were analysed using Statistical Package for Social Sciences (Version 28.0). Wilcoxon signed rank test was used as the non-parametric statistical test to compare pre- and post-intervention MBI-HSS-MP scores.
Qualitative data
Participants were notified of their allocated interview time slots after the completion of the mindfulness program. Depending on each participant's availability, either online Zoom or physical interviews were conducted. Physical interviews were held within an enclosed private meeting room in SATA CommHealth. Interviews were conducted with two researchers and one participant present. Each researcher directed the interview using a predefined topic guide throughout the interview. The topic guide (refer to Supplementary S1) covered: (1) experience and perception of mindfulness, (2) program structure and details, (3) attitude on adopting mindfulness as a coping strategy, and (4) perception on burnout, where the key content was based upon existing relevant studies on mindfulness.25–28
Interviews were audio recorded, transcribed, and analysed via thematic analysis. A combination of inductive and deductive approach was used to derive the codes and themes from the data. 29 The first author independently read and coded the transcribed text of each interview. Subsequently, these codes were grouped into potential themes based upon observations of word repetitions, consensus in perceptions and emerging patterns or constructs (e.g., introspection) across participants’ quotes through iterative comparisons. Subsequently, the themes/subthemes were discussed and reviewed amongst all the researchers until mutual agreement on their naming and descriptors was achieved.
Results
MBI-HSS-MP score
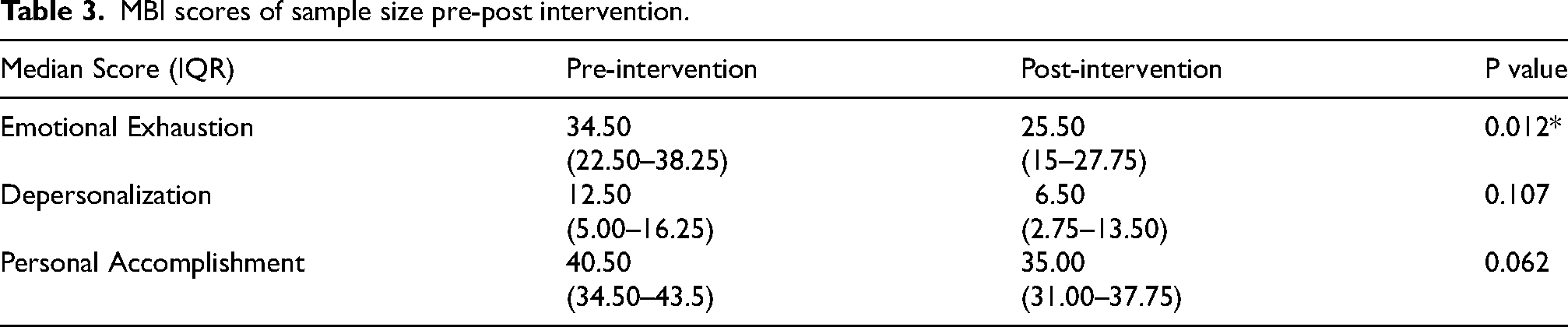
Participants had high levels of EE, DE, and PA prior to the start of the mindfulness program, indicating that they were in a burnout state (Table 3). After the program, the levels of EE, DE, and PA decreased, with only EE revealing a significant change (p = 0.012) post-program.
MBI scores of sample size pre-post intervention.
Semi-structured interview responses
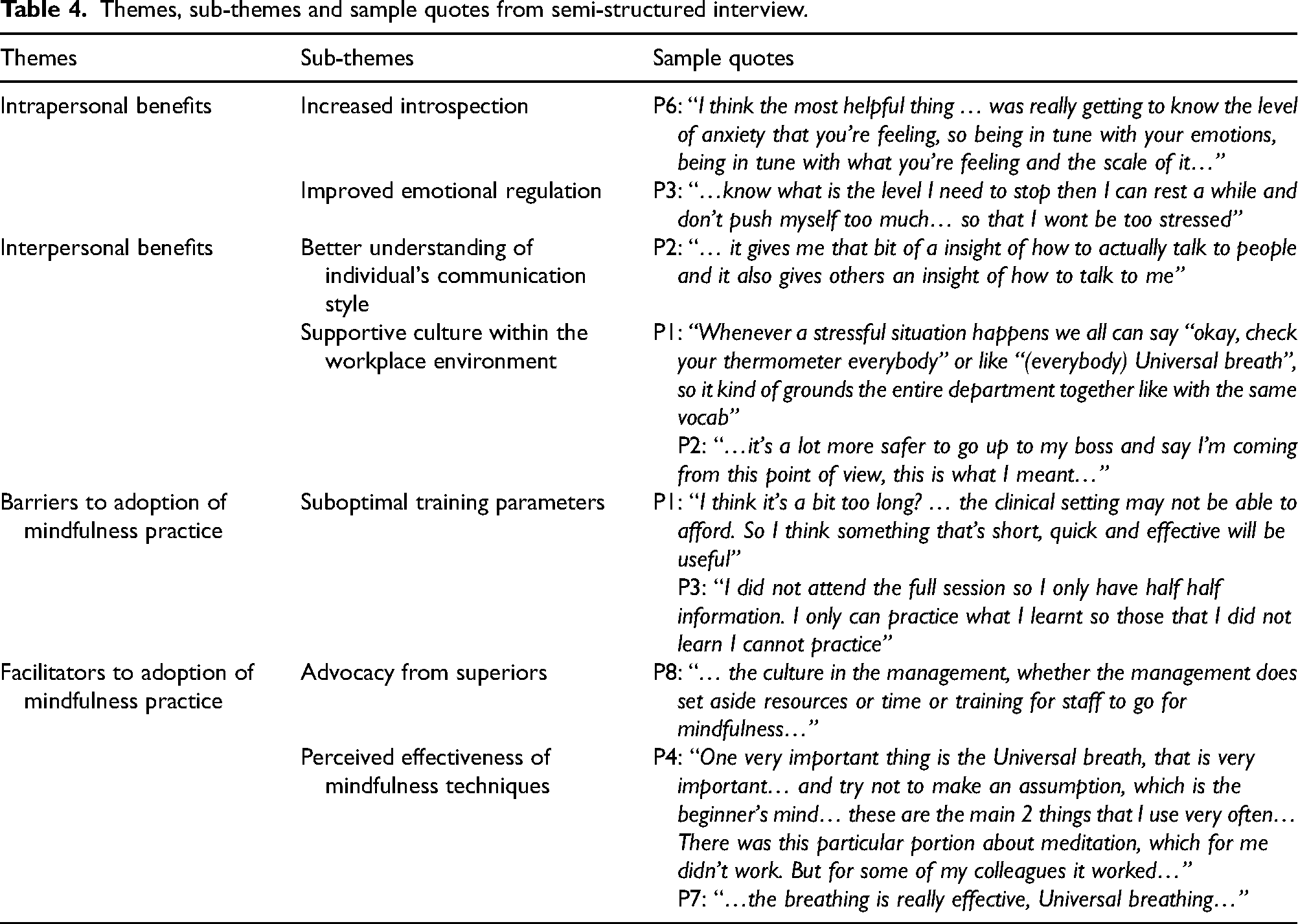
Four main themes were identified from participants’ responses during interviews: (1) intrapersonal benefits, (2) interpersonal benefits, (3) barriers to adoption of mindfulness practice, and (4) facilitators to adoption of mindfulness practice. The themes and subthemes are compiled and shown in Table 4.
Themes, sub-themes and sample quotes from semi-structured interview.
Intrapersonal benefits
All participants shared that they became more aware of the emotions present within themselves which includes emotions such as anxiety, stress and frustration. The increased ability to introspect resulted in a better awareness and understanding that their emotions have an influence on their experience at work. Moreover, 6 out of 8 participants (P1, P2, P3, P4, P5 and P7) shared that there was an improvement in their ability to regulate stress. They described that they had a better understanding of their own capacity for stress and their stress limit as the mindfulness session promoted greater introspection and self-awareness of emotions. This allowed them to have greater confidence in emotional regulation in unexpected situations or situations that arise from interactions with superiors or patients.
Interpersonal benefits
Participants shared that the results from the Emergenetics psychometric tool allowed them to understand their own and colleagues’ communication styles better. They were able to refine their own communication skills through adjusting and being mindful of their own responses. Through the mindfulness training, a supportive culture within the workplace environment was created. The participants were encouraged to work together in smaller groups during the sessions and their interactions were maintained and sustained on a group chat. One participant (P1) has shared that regular check ins with each other during working hours were beneficial in encouraging further interaction and active application of learnt mindfulness techniques. With the creation of a supportive workplace environment, the participants shared that they were more willing to be vulnerable with their supervisors. Therefore, the mindfulness training strengthened their communication skills, advocated workplace empathy and a supportive culture among the healthcare professionals which led to improved interpersonal relationships.
Barriers to adoption of mindfulness practice
There were mixed responses regarding the total training duration, the interval span between each session and the length of each session. Three participants (P1, P2, and P4) felt that the program could be condensed into shorter version with more pertinent content and fewer sessions. Another participant (P6) shared similar sentiments, indicating that they experienced mental saturation due to the length of the session. However, participants who found the length of each session to be acceptable described that the content covered and the interactions between participants as facilitating deeper understanding, thereby warranting the duration of the program.
With regards to the interval between each session, three participants (P2, P4, and P7) shared that sessions were too widely spaced, and they had difficulty remembering the content taught as a result. On the other hand, the rest of the participants who felt that the intervals between sessions were appropriate shared that it helped to pace and plan their work demands and allowed time to consolidate what they learned during the sessions. Three participants (P2, P3 and P7) did not complete all sessions due to unavailability. They shared that they had an incomplete understanding of mindfulness which limited their individual practice of mindfulness techniques.
Facilitators to adoption of mindfulness practice
Some participants (P1, P5 and P8) shared about how an organization treats and values their employees has the potential to influence one's working experience. Participants (P1, P4, P5 and P8) agreed that a supportive organization that looks out for the well-being of their staff and understands the challenges within the clinical setting serves as a facilitator to the adoption of mindfulness.
The mindfulness techniques which all participants found particularly useful were the beginner's mind, universal breath, and the thermometer. One participant (P6) shared that these strategies were largely applied within one's mind facilitating the practice of these techniques anywhere once it is understood. However, other techniques such as meditation were found to be less useful, thus influencing their subsequent practice.
Discussion
The present study sought to investigate the usefulness of a mindfulness program on AHPs and to identify AHPs’ attitudes and perceptions towards the adoption of mindfulness practice. Our findings demonstrate that after a short mindfulness program, participants experienced increased introspection, improved emotional regulation and interpersonal relationships, which likely led to the reduction in emotional exhaustion.
Improved emotional regulation and interpersonal relationships
After the training, the participants were more aware of their own emotions, and there was improved emotional regulation, especially relating to the self-management of stress. This was consistent with other qualitative studies21,30 that revealed similar experiences of improvements in attention and self-awareness to identity their emotional state, thoughts, and behaviours. Importantly, this result also aligns with other quantitative studies that reported lower stress levels among healthcare professionals after mindfulness practice.20,22 In addition, stress is found to be positively correlated to burnout. 31 Therefore, regular mindfulness practice may reduce levels of EE and overall burnout through the self-management of stress.
The above hypothesis can be substantiated through the concept of emotional regulation. It was described by Fasbinder et al. (2020) as a construct of 4 defining attributes: (1) self-awareness, (2) self-control, (3) emotional expression, and (4) active thinking. 32 These attributes influence one's perception of the antecedents which contributes to how one responds to a given situation. Hence, there appears to be a correlation between attentiveness to one's experienced emotions, emotional regulation, and stress, which influences the level of burnout an individual experiences. 33 Based upon the 5-stage symptomatology model of burnout, a job begins with a honeymoon phase characterized by enthusiasm, followed by the onset of stress (a stage of stagnation with neglected symptoms) before progressing to chronic stress, burnout and ultimately, habitual burnout. 13 The process of experiencing burnout begins if effective coping mechanisms were not used to manage job-related stressors. 13 Therefore, improved emotional regulation would allow AHPs to manage work-related stressors during the onset of the stress phase, which prevents progression to the next phase of burnout.
Another benefit experienced by participants was improved interpersonal relationships or understanding between colleagues and supervisors. The mindfulness program involved the creation of three smaller groups within the larger group of participants to facilitate discussion about the content taught during the session. Participants’ interactions were further enhanced when they were assigned into specific groups after each session to encourage and remind each other to apply mindfulness in their daily lives. Considering that AHPs generally work in teams, the element of teamwork and communication embedded within a mindfulness program could be useful in reducing burnout. This notion is supported by a study by Wang et al. (2022) where increased teamwork quality was found to reduce burnout in the healthcare setting. 34 Furthermore, difficult communication, isolation, and having low levels of social ties within the work environment exert a negative influence on healthcare worker's burnout and health.35,36
Barriers and facilitators for mindfulness practice
Due to the diverse nature of the workplace environment across occupations, there are currently no standardized mindfulness training models in the work setting. 37 The perceived barriers and facilitators to the adoption of mindfulness practice observed in the present study provide insights on the limitation of our tailored mindfulness program. Therefore, these perspectives can inform future modifications to derive an optimal mindfulness training model to be used within the clinical setting.
The overall sentiment felt by the participants was that the mindfulness program was quite lengthy, and some did not manage to attend all the sessions. Findings from other studies revealed a similar pattern of dropout rates among healthcare professionals attending the Mindfulness Based Stress Reduction (MBSR) program. 38 Although the MBSR program is an evidence-based program that consists of 8 weekly sessions that are 2.5 h long and includes a day of silent retreat,21,30,39 it is not always feasible to adopt this program in the AHPs’ work environment. One study elaborates that 40% of healthcare professionals dropping out from the program was due to the lack of time and increased work responsibilities. 40 Consequently, there have been various tailored mindfulness programs used among healthcare professionals that showed promising levels of attendance. One study that adopted a variation of MBSR where its duration was reduced to 1 h per week and another study that evaluated the efficacy of a 4-session long mindfulness-based intervention revealed a retention rate of 97% and 93.1% among participants, respectively.41,42 Therefore, given the practical difficulties of AHPs’ workload and time constraints, a reduced session duration would likely have been better received.
Despite the varied participation rates, all participants experienced significant improvements in the EE subscale of the MBI-HSS-MP. This improvement in EE corresponded to one participant's sharing that there were several mindfulness techniques such as the beginner's mind, universal breath, and the thermometer that were perceived to provide greater effectiveness compared to others (e.g., meditation). Additionally, it corroborates with the findings from a study that examined the transfer of mindfulness training to the work setting. 43 The study has suggested that the value ascribed to the mindfulness strategies relates to an individual's perceived skillfulness and effectiveness in bringing about intrapersonal benefits. In other words, mindfulness strategies that are convenient and useful increase motivation for individuals to implement the strategies in their daily lives.
Limitations and future directions
The findings of the current study must be interpreted within the context of some limitations. Firstly, this study recruited a small sample size due to purposive sampling in a fixed setting, thus limiting the capacity to generalize the results to a larger population. Relatedly, the selected participants may hold preconceived notions towards the outcome of mindfulness as they may be aware of the intention for program implementation. Future studies should investigate the impact of mindfulness in a larger AHP population.
Secondly, there was difficulty in ensuring the full adherence of participants to the program due to unexpected personal and workload demands. This might have influenced participants’ experiences and their overall perception and effectiveness of mindfulness. In order to ensure maximum participation and successful implementation, a pivotal facilitator would be the presence of organizational support. 44 Furthermore, introducing a shorter and more condensed program that accommodates to the clinical work environment would reduce barriers to participation. Therefore, future programs performed with considerations of time commitment and organizational support such as resources, time or incentives would encourage program adherence among AHPs.
Lastly, the burnout symptoms of participants in this study were only assessed via MBI-HSS-MP. For future studies that aim to evaluate the impact of mindfulness on reducing burnout, there is value in including other outcome measures to provide a more holistic view of burnout. One example is the Copenhagen Burnout Inventory 45 that measures burnout on a personal, work-related, and client-related scale and outcome measures that includes job satisfaction and engagement.
Conclusion
A 10-week tailored mindfulness program reduced burnout symptoms, specifically EE, among AHPs. Mindfulness practice facilitated the ability to introspect and regulate emotions, and improved interpersonal communication and relationships which enhance teamwork quality. Collectively, this reduces the likelihood of burnout in the healthcare settings. Future studies should investigate the efficacy of mindfulness intervention in a larger AHP cohort. Key factors such as advocacy from superiors and organisational support, including time allocation and resource investment, should be considered in future programs to facilitate successful adoption of mindfulness among AHPs in a clinical setting.
Supplemental Material
sj-docx-1-wor-10.1177_10519815241313115 - Supplemental material for Exploring the use of mindfulness for prevention of burnout in allied health professionals in Singapore
Supplemental material, sj-docx-1-wor-10.1177_10519815241313115 for Exploring the use of mindfulness for prevention of burnout in allied health professionals in Singapore by Shun Hwa Yap, Liyana Nabilah Bte Zainal, Siti Zubaidah Binte Yusoff and Xiang Ren Tan in WORK
Footnotes
Acknowledgements
We would like to thank the participants from SATA CommHealth for their participation in this study. We would also like to appreciate our research partner - Nicholas for his contributions in the data collection process.
Ethical review
Ethical approval was obtained from Singapore Institution of Technology Institutional Review Board, Reference No. 2022043.
Informed consent
Participants provided written informed consent prior to the commencement of the study and verbal consent for the interviews to be audio recorded.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by funding from SATA CommHealth.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.