
Abstract
Background:
Macro-thyrotropin (TSH) is a high molecular weight complex of TSH associated with apparently elevated levels of serum TSH, which can lead to an incorrect diagnosis of subclinical hypothyroidism. Given that levothyroxine (LT4) replacement is unnecessary in such cases, the accurate identification of macro-TSH based on clinical and laboratory findings is of particular importance. We aimed to determine the prevalence and clinical features of macro-TSH in patients with subclinical hypothyroidism evaluated after the introduction of TSH harmonization.
Patients and Methods:
Between August and November 2023, we included 1599 consecutive patients with subclinical hypothyroidism (TSH > 4.23 mIU/L with normal fT4 levels) who were either untreated or receiving LT4 replacement monotherapy. Polyethylene glycol (PEG) precipitation was performed in all cases. Patients with TSH recovery of <20% underwent further evaluation, including gel filtration chromatography under neutral and acidic conditions, protein G and Jacalin precipitation assays, and a comprehensive battery of interference tests.
Results:
Four patients (0.25%) showed high molecular-weight TSH peaks (>150 kDa) under neutral conditions that disappeared under acidic conditions, with a shift to the native molecular weight (approximately 28 kDa), indicating the initial presence of macro-TSH. The TSH complex was detected in peaks corresponding to IgG, IgA, and IgM. These findings were verified using Protein G and Jacalin precipitation assays, with no evidence of assay interference. Reevaluation of TSH recovery following PEG precipitation showed substantial variation in two patients who had abundant monomeric TSH compared with the high-molecular complex. All four patients with macro-TSH had previously received LT4 therapy, which resulted in a modest reduction in TSH levels, with three of these patients testing positive for TgAb and/or TPOAb.
Conclusions:
Macro-TSH complexes comprise several immunoglobulin isotypes. In cases with low antibody-TSH binding affinity and positive antithyroid autoantibodies, TSH levels may fluctuate during the clinical course, thereby complicating diagnosis and management.
Keywords
Introduction
Macro-thyrotropin (TSH) is a high molecular weight complex (>150 kDa) of TSH. It is characterized by elevated TSH levels with normal thyroid hormone concentrations, likely owing to reduced renal clearance and low biological activity. The presence of macro-TSH can give the false impression that TSH levels are elevated. However, thyroid hormone replacement therapy is not required in patients with macro-TSH who present with subclinical hypothyroidism. Therefore, after excluding other sources of assay interference, accurate identification of macro-TSH is essential to avoid unnecessary treatment. In this regard, gel filtration chromatography (GFC) is considered the diagnostic gold standard for elucidating the molecular size of macro-TSH. However, polyethylene glycol precipitation (PEG) is more accessible as an initial screening approach, along with being comparatively inexpensive. 1
Although in recent clinical practice, thyroid function has been evaluated using different types of high-sensitivity automated immunoassays, inter-assay variability has emerged as a significant issue. To address these discrepancies, the International Federation of Clinical Chemistry and Laboratory Medicine Committee for Standardization of Thyroid Function Testing has developed a global harmonization approach for TSH measurements. 2 As a result, TSH harmonization has been introduced with an assay reference interval of 0.61–4.23 mIU/L in Japan. 3
In large cohorts of patients with subclinical hypothyroidism, the prevalence of macro-TSH is estimated to be between 0.6% and 1.6%.4–6 Although markedly elevated TSH levels have often been reported in patients with macro-TSH, 1 TSH levels as low as 4 mIU/L have also been observed. 7 To accurately identify patients with macro-TSH, some groups have proposed that isolated TSH elevation with thyroid hormone in the upper half of the reference interval, or the use of TSH cut-off values stratified according to fT4 levels, may have diagnostic value.8,9 However, previous studies have employed diverse measurement methods, while some have also included patients receiving levothyroxine (LT4) replacement therapy for subclinical hypothyroidism. Therefore, the distribution of TSH levels in patients with macro-TSH among those with subclinical hypothyroidism encountered in current clinical practice remains unclear. Compared with other forms of assay interference, macro-TSH is particularly difficult to detect using routine laboratory testing. 10 Therefore, physicians should be aware of potential discrepancies between laboratory data and clinical findings, such as when TSH levels do not fully normalize despite an increased LT4 dose or when adverse clinical signs appear.
In this study, using a commercially available Roche electrochemiluminescence immunoassay (ECLIA), we sought to determine the prevalence and clinical features of macro-TSH in patients with subclinical hypothyroidism who were evaluated after the introduction of TSH harmonization.
Methods
Patients
Between August and November 2023, we enrolled 1948 patients at Kuma Hospital who underwent thyroid function tests using the ECLIA method for the evaluation of different thyroid diseases and who were found to have subclinical hypothyroidism (TSH > 4.23 IU/mL and fT4 levels within the reference interval). Their median age (378 males and 1570 females) was 56 years (range: 19–80 years). We reviewed their clinical findings and medications by referring to their medical records. Of these 1948 patients, 941 had received no treatment. Among the remaining 1007, there were 658 who had received only LT4, while 349 were treated either with thiamazole, propylthiouracil, or potassium iodide. We finally included 1599 patients who were either untreated or receiving LT4 replacement monotherapy in this study (Fig. 1). This study was approved by the Ethics Committee of Kuma Hospital (approval number: 20230720-1). Since the research involved the use of preexisting clinical data and blood samples without freeze-thaw cycles before reassay stocked at –80°C, the need for individual informed consent was waived and an opt-out consent process was implemented.
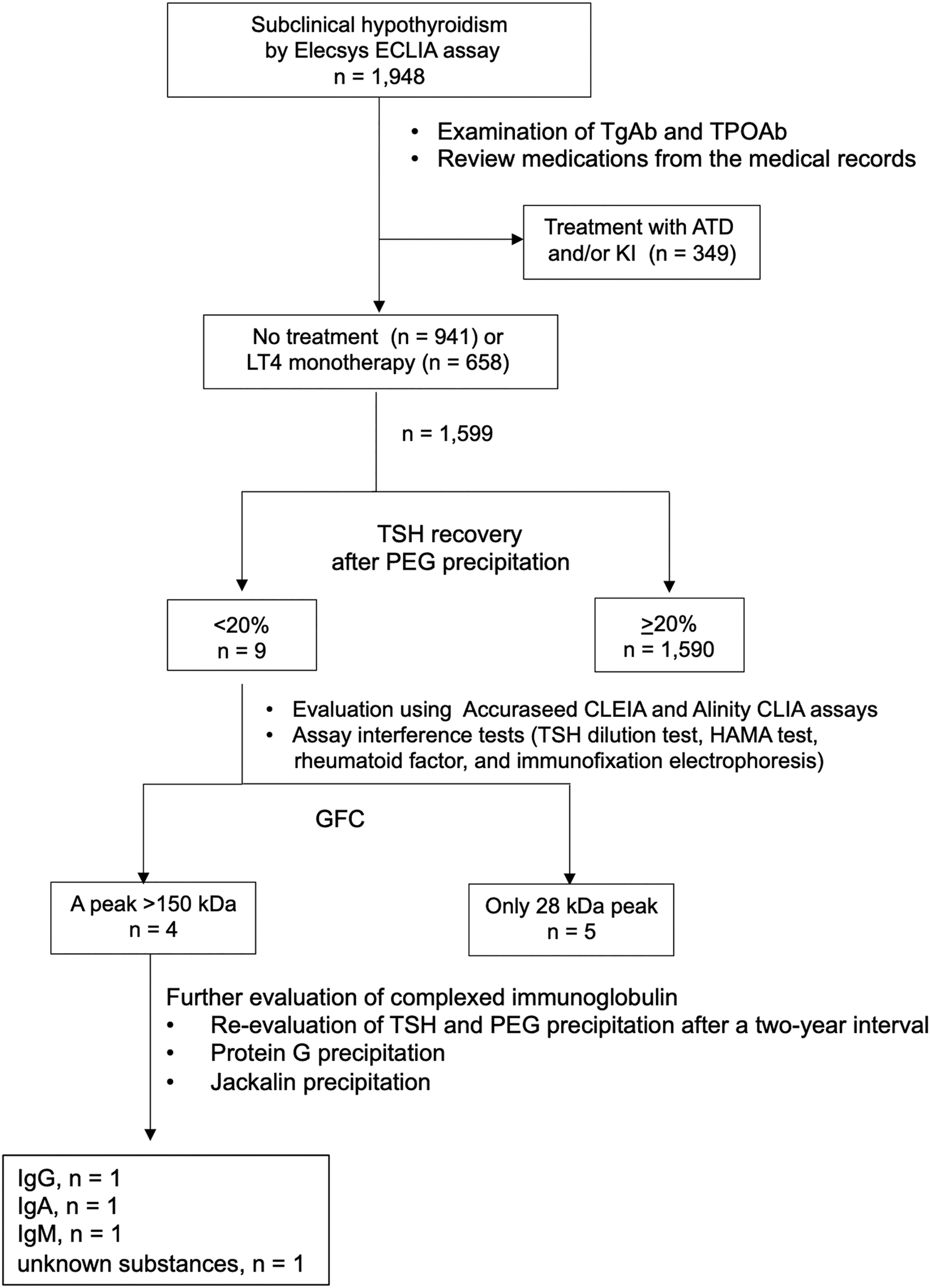
Flow chart showing the detection of macro-TSH and final selection of patients with subclinical hypothyroidism in the study. ATD, thiamazole and propylthiouracil; GFC, gel filtration chromatography; HAMA, human anti-mouse antibody absorption; KI, potassium iodide; LT4, levothyroxine; PEG, polyethylene glycol precipitation; TgAb, anti-thyroglobulin antibodies; TPOAb, anti-thyroid peroxidase antibodies.
Thyroid function tests
Routine measurements of TSH, free thyroxine (fT4), and free triiodothyronine (fT3) were performed using an Elecsys ECLIA assay (
Polyethylene glycol precipitation
Equal volumes (300 µL) of 25% PEG-6000 (FUJIFILM Wako Pure Chemicals) were added to samples obtained from patients and control individuals. This was followed by vortex mixing for 10 seconds, incubation for 30 minutes at 20–25°C and subsequent centrifugation at 12,100 × g for 10 minutes. Finally, the supernatant was measured to determine the rate of TSH recovery, using the following equation:

The reference range [99% confidence interval (CI)] for TSH was 20–65%.
TSH dilution test
Samples were diluted 2-, 5-, and 10-fold, and TSH levels were measured using the Roche ECLIA assay at Kuma Hospital, with TSH recovery (%) being determined using the following equation:

The presence or absence of dilution linearity was also evaluated, with the limit of quantitation ranging from 0.005 to 100 mIU/L and intra-assay coefficients of variation of ≤10% for TSH assays.
Gel filtration chromatography
GFC analyses under neutral (pH 7.2) and acidic (pH 3.0) conditions were performed using Shodex Protein KW-804 columns (Resonac Corporation, Tokyo, Japan). The flow rate was 0.75 mL/min, and the fractionation time was 35 minutes. Initially, 200 μL samples obtained from patients and healthy control group were eluted under neutral conditions (pH 7.2) using a mobile phase (150 mM sodium chloride and 50 mM Tris buffer). TSH and immunoglobulin concentrations were measured in each GFC fraction. Subsequently, fractions corresponding to high-molecular-weight TSH peaks were directly reinjected into the column using a mobile phase adjusted to pH 3.0 to assess whether macro-TSH complexes dissociated under acidic conditions. TSH concentrations in each GFC fraction were measured without prior neutralization.10,11
Agarose bead protein G precipitation
To evaluate the potential interference due to immunoglobulin G, we used Protein G agarose beads (Code No. 11243233001; Sigma-Aldrich). Equal volumes (200 µL) of protein G were added to patient and control samples, followed by incubation for 3 hours at 4°C and subsequent centrifugation at 12,100 × g for 5 minutes. Finally, the supernatant was collected to determine the rate of TSH recovery using the following equation:

Samples that deviated by 15% or more from the rate of recovery of the concurrently measured control sample were considered positive.
Heterophilic antibody blocking tube treatment
To evaluate interference caused by heterophilic antibodies, we used heterophilic blocking tubes (HBT, product code 3IX762; Scantibodies Laboratory). Patient and control samples (200 µL) were added to these tubes, followed by mixing five times by inversion and incubation at room temperature for 1 hour. Having thereafter mixed several times by pipetting, the samples were analyzed, with TSH recovery being calculated using the following equation:

Samples that deviated by 15% or more from the recovery rate of the concurrently measured control sample were considered positive.
Jacalin precipitation test
Jacalin is an alpha-

Samples that deviated by 15% or more from the recovery of the concurrently measured control sample were considered positive.
Human anti-mouse antibody absorption
Human anti-mouse antibody absorption (HAMA) analyses were performed using IIR (BioIVT, Westbury, NY, USA). A 20 mg/mL stock solution of IIR (0.1 mL) was diluted with 0.075 M phosphate-buffered saline (PBS) to final concentrations of 10 and 2.5 mg/mL, with a 0 mg/mL solution consisting of 0.075 M PBS alone serving as a negative control. Samples were mixed with the different concentrations of IIR solution at a 9:1 ratio (135 µL:15 µL; total volume: 150 µL) and vortexed gently for 5 seconds. The mixtures were incubated at 4°C for 16 hours with agitation on a rotator, after which they were centrifuged for 5 minutes at 12,100 × g, with 150 µL of the resulting supernatant being transferred to a micro-sample cup. For determinations of the rates of TSH recovery, the TSH concentration in each sample treated with 0 mg/mL IIR (PBS only) was defined as 100%. Recoveries were calculated as the percentage of the TSH concentration measured after the addition of IIR at final concentrations of 0.25 and 1 mg/mL IIR relative to the baseline value.
Rheumatoid factor
Interference from the rheumatoid factor was evaluated based on latex agglutination turbidimetric immunoassays. In these assays, the rheumatoid factor within samples reacts with human-denatured gamma globulin-sensitized latex to initiate an antigen–antibody reaction, resulting in agglutination. The degree of agglutination in the reaction solution, and hence the concentration of the rheumatoid factor in the sample, was determined based on a change in absorbance.
Immunofixation electrophoresis
Evaluation of monoclonal protein (M protein) in serum was outsourced and performed using immunofixation electrophoresis according to the manufacturer’s protocols.
Results
Of the 1599 patients presenting with subclinical hypothyroidism who were either untreated or receiving LT4 replacement monotherapy, 909 and 690 were established to be positive and negative for TgAb and/or TPOAb, respectively. As shown in Figure 1, a comprehensive battery of examinations was performed to identify patients with macro-TSH. Nine patients showed a TSH recovery of <20% in response to PEG precipitation (Table 1). Of these, all nine and seven showed linearity in the TSH dilution test evaluated using the Elecsys ECLIA method and elevated TSH levels using both the Accuraseed CLEIA and Alinity CLIA methods, respectively (Table 2). Although one of these patients tested positive for rheumatoid factor, none showed evidence of interference with HAMA or M protein (Table 2).
Nine Patients with Significant Reductions in the Rate of PEG Recovery

Bold characters indicate values outside of the reference intervals.
F, female; PEG, polyethylene glycol.
Evaluation of Measurement Interference and GFC Testing in Cases of Reduced PEG Recovery
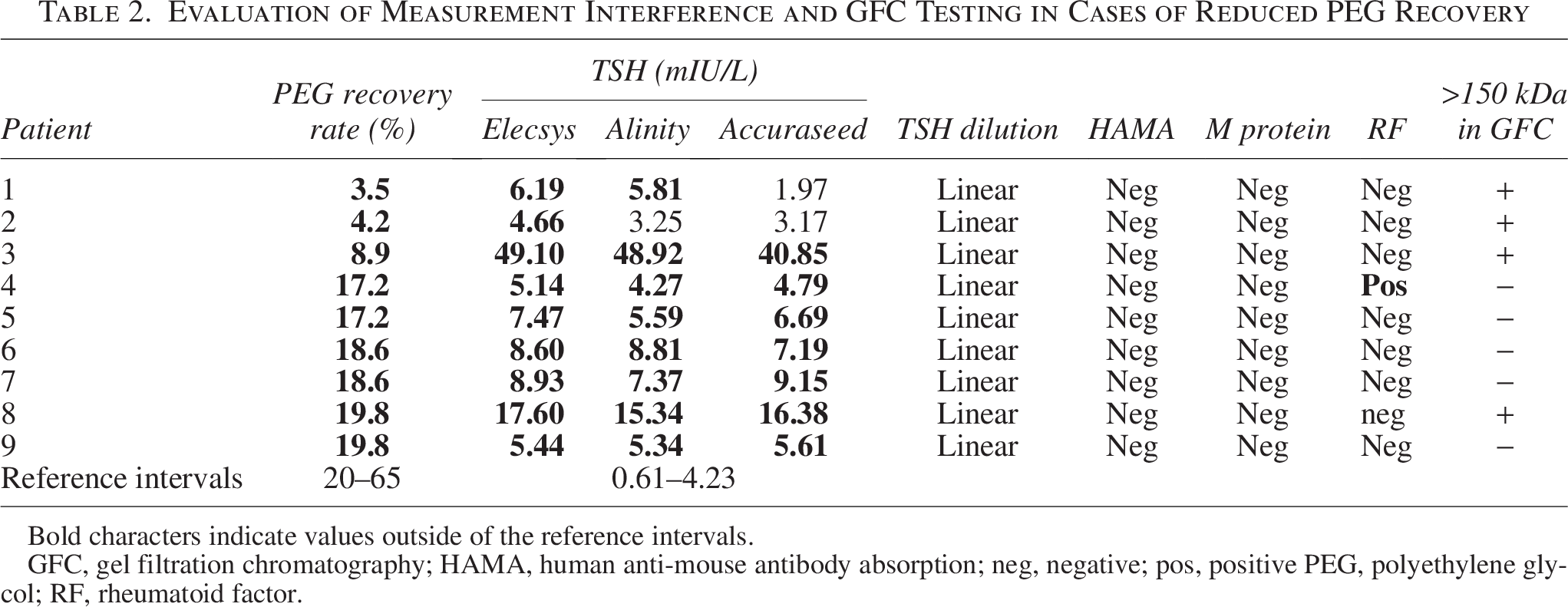
Bold characters indicate values outside of the reference intervals.
GFC, gel filtration chromatography; HAMA, human anti-mouse antibody absorption; neg, negative; pos, positive PEG, polyethylene glycol; RF, rheumatoid factor.
Of the nine patients for whom there was a TSH recovery of <20% on PEG precipitation, GFC revealed that four (#1, #2, #3, and #8) were characterized by peaks in fractions of high molecular weight TSH (>150 kDa) in neutral elution buffer (pH 7.2). However, acid elution buffer (pH 3.0) was found to promote a dissociation of these TSH complexes, resulting in the disappearance of the high molecular weight peak and a shift toward the native molecular weight (approximately 28 kDa) (Fig. 2). These peak shifts provided definitive evidence that the elevated levels of TSH were attributable to the presence of macro-TSH. The timing of elution of the TSH peak fractions in patients #1 (26.5 minutes), #2 (27.5 minutes), and #3 (20.0 minutes) was consistent with molecular weights slightly higher than those obtained for the peaks of IgA, IgG, and IgM, respectively (Fig. 2 and Supplementary Fig. S1). However, the timing of elution of the TSH peak fraction in patient #8 (24.0 minutes) indicated an absence of binding to any specific subclass of immunoglobulin. Consistent with these findings, the low rate of TSH recovery following Jacalin precipitation in patient #1 and after protein G precipitation in patient #2 indicated IgA-bound and IgG-bound macro-TSH, respectively (Table 3). Reevaluation of the rate of TSH recovery following PEG precipitation, performed after a 2-year interval, revealed marked changes in patients #3 and #8 (Table 3). Initial GFC analysis for these patients had indicated a higher abundance of monomeric TSH (28 kDa) when compared with the high molecular weight TSH complex (Fig. 2).
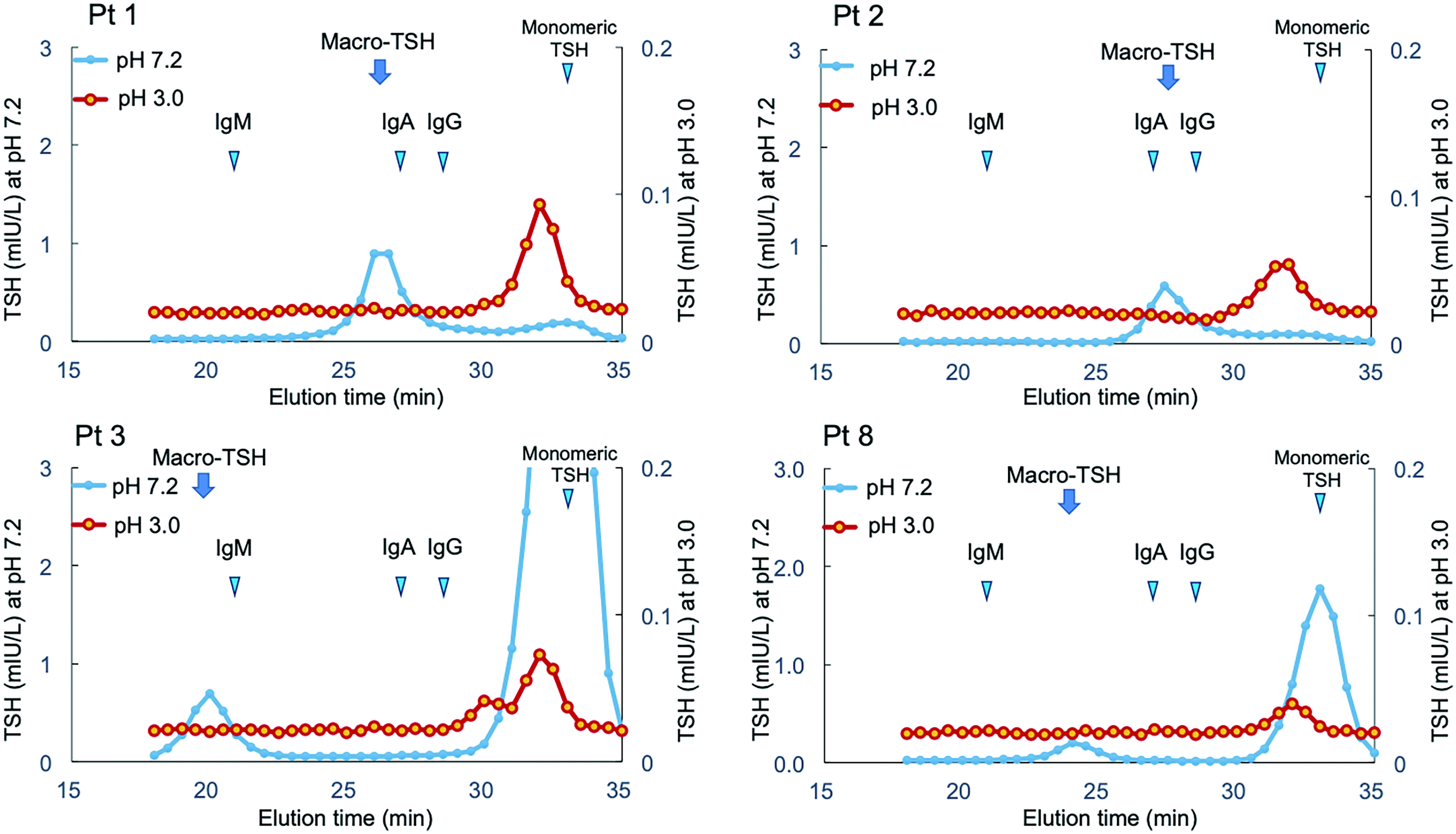
GFC analysis under neutral and acidic conditions. Pt 1, patient #1; Pt 2, patient #2; Pt 3, patient #3; Pt 8, patient #8. The elution times of IgM (21.0 minutes), IgA (27.0 minutes), IgG (28.5 minutes), and monomeric TSH (33.0 minutes) in neutral buffer (pH 7.2) are indicated by arrowheads. The levels of macro-TSH are indicated by arrows. GFC, gel filtration chromatography; IgM, immunoglobulin M; IgA, immunoglobulin A; IgG, immunoglobulin G; TSH, thyrotropin.
Laboratory Evaluation and Thyroid Volume of the Four Patients with macro-TSH

Thyroid volume was measured by ultrasonography and calculated using the following equation: thyroid volume = 0.7 × (length × height × width) in both lobes of thyroid gland.
Bold characters indicate values outside of the reference intervals.
2-year interval between the 1st and 2nd examination.
GFC, gel filtration chromatography; HBT, heterophilic antibody blocking tube; NT, not tested; PEG, polyethylene glycol; TgAb, anti-thyroglobulin antibodies; TPOAb, anti-thyroid peroxidase antibodies.
The volume of the thyroid gland in the four patients with macro-TSH (ages: 27–47, TSH levels at the first and second examinations: 4.6–49.1 mIU/L) had almost normal proportions. Three of these patients were positive for TgAb and/or TPOAb (Table 3). All four patients had received LT4 replacement therapy during their clinical course, which contributed to slight reductions in their TSH levels (Fig. 3). Of the four patients (#4, #5, #6, and #9) with low TSH recovery (<20%) on PEG precipitation whose macro-TSH status was not confirmed by GFC, two patients (#5 and #6) showed persistently elevated TSH levels at the 2-year interval (Supplementary Table S1). Other clinical characteristics, including thyroid volume, positivity for TgAb and/or TPOAb, and dose of LT4 replacement during their clinical courses, were similar to those observed in the four patients (#1, #2, #3, and #8) with definitive macro-TSH (Table 3, Supplementary Table S1, and Fig. 3).
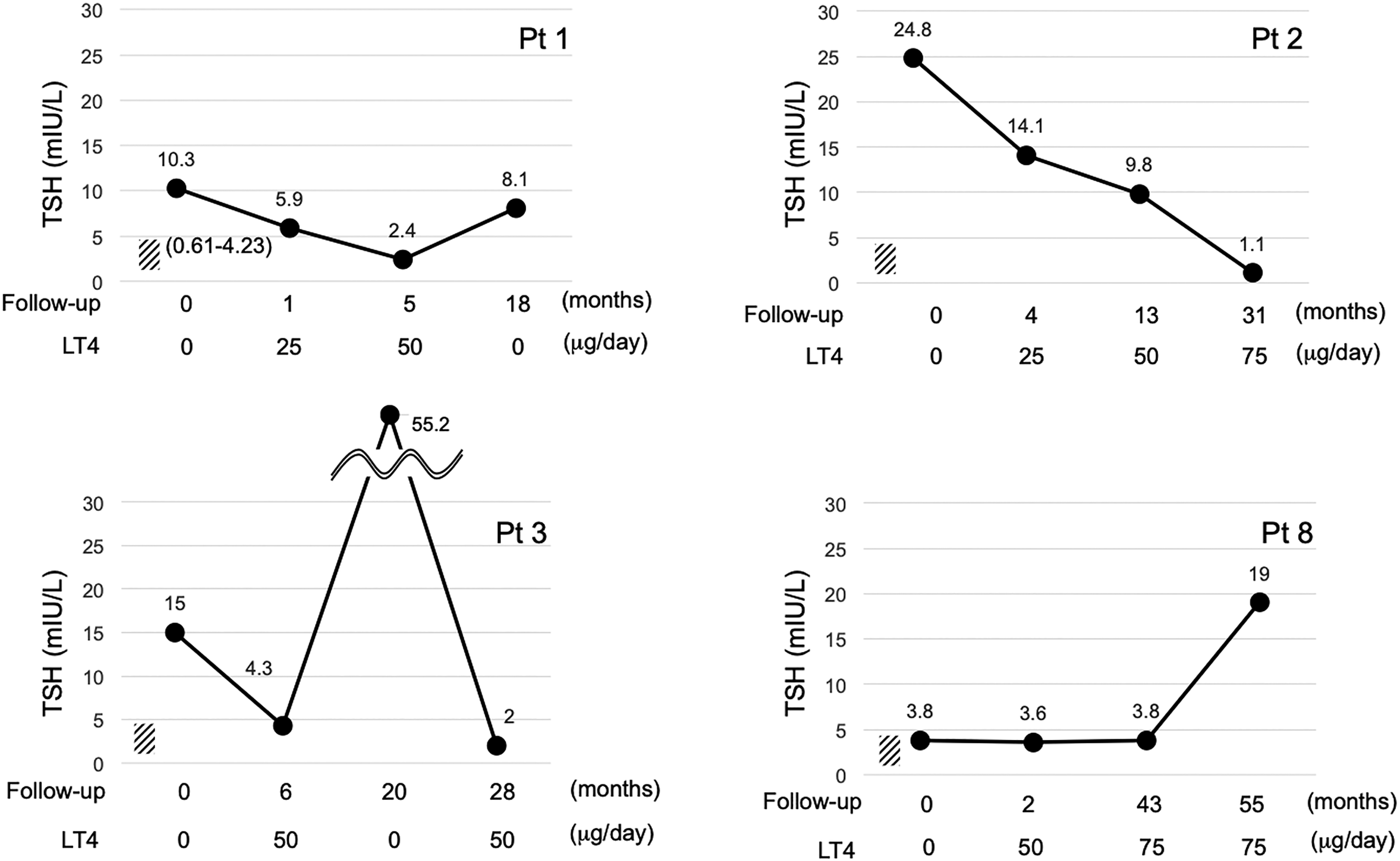
TSH levels in patients with macro-TSH with or without LT4 replacement therapy. Pt 1, patient #1; Pt 2, patient #2; Pt 3, patient #3; Pt 8, patient #8. Four representative time points are shown during the clinical course of each patient, at which thyroid function had stabilized either during LT4 replacement therapy or without treatment. The horizontal axis represents the time course (months) with the dose of LT4 replacement. LT4, levothyroxine; TSH, thyrotropin.
Discussion
In this study, we recorded a macro-TSH prevalence of 0.25% (4/1599) in patients with subclinical hypothyroidism who were either untreated or receiving LT4 replacement monotherapy, which is somewhat lower than previously reported levels (0.6–1.6%).4–6 To date, there have been 10 observational studies that have investigated suspected macro-TSH in patients with subclinical hypothyroidism. 1 Only one of these has examined a cohort exceeding 1000 individuals. 6 In this regard, studies often apply a TSH cutoff value higher than 10 mIU/L to enroll individuals with subclinical hypothyroidism. Several studies have focused on evaluations using assay methods developed for research purposes rather than those that are commercially available.5,6,12 For the purposes of the present study, we included consecutive patients with laboratory findings of subclinical hypothyroidism (TSH > 4.23 mIU/L with normal fT4) measured using the commercially available Roche ECLIA, which is widely used in clinical practice under TSH-harmonized conditions. Macro-TSH was diagnosed based on multiple analyses, including PEG, GFC, immunoglobulin precipitation, and verification of measurement interference. We suspect that discrepancies in prevalences reported in previous studies may be due to inter-study differences with respect to patient selection, assay platforms, diagnostic criteria, and cut-off TSH levels, since earlier studies were conducted prior to TSH harmonization and were dependent on assay-specific reference intervals.
A key finding of this study was the heterogeneity of the molecular weights of the detected TSH complexes. In the four patients with macro-TSH, we identified diverse complexes associated with immunoglobulins, including IgG, IgA, and IgM, along with undetermined substances (Fig. 2 and Table 3). In this regard, although PEG has been established as being highly effective in precipitating IgG and IgM, it tends to be less effective in the case of IgA, with only approximately 50% of IgA being precipitable. 11 IgG-bound TSH has been considered the predominant form of macro-TSH.1,4,5 However, the findings of the present study provided evidence to indicate that macro-TSH potentially comprises diverse immune complexes.
A further notable observation was the temporal variability in macro-TSH, with marked differences detected in the ratios of concomitant monomeric TSH to macro-TSH complex. For example, for two of the patients (#1 and #2) with macro-TSH, the observed rates of TSH recovery during PEG precipitation were persistently low and characterized by a predominantly high molecular weight TSH peak, implying stable immunoglobulin associations (Fig. 2 and Table 3). In the other two patients (#3 and #8), the rate of TSH recovery was found to fluctuate considerably between the two examinations (Table 3). These latter patients had a relatively higher proportion of monomeric TSH (Fig. 2), indicating the presence of low-affinity, unstable TSH complexes or fluctuating binding-antibody levels. Similar longitudinal fluctuations in macro-TSH and serum TSH levels have been reported previously, 12 indicating that macro-TSH is not static and may evolve over time.
Our findings have several important implications with respect to further research. Macro-TSH should be considered not only in patients with marked TSH elevation but also in those with mild or fluctuating TSH increases and normal fT4 levels. Linearity in TSH dilution testing and consistency among different immunoassay platforms do not necessarily exclude the presence of macro-TSH, thereby emphasizing the need for targeted screening using PEG precipitation in conjunction with confirmatory GFC when suspicion persists. Among the five PEG-suspected but GFC-negative patients, some may represent labile macro-TSH or partially dissociated complexes. This possibility is supported by the findings that ancillary interference tests were negative in all but one case and that GFC-negative patients showed clinical characteristics similar to those with definitive macro-TSH (Tables 2 and 3, Supplementary Table S1, and Fig. 3). PEG precipitation alone therefore remains an important screening method for macro-TSH and may have diagnostic value in the appropriate clinical contexts. However, it is not realistic, from a cost-effectiveness perspective, for all patients with subclinical hypothyroidism to undergo PEG precipitation testing to identify the rare cases of macro-TSH. Current clinical guidelines do not actively recommend LT4 replacement for older adults with subclinical hypothyroidism, given the physiological age-related increase in TSH levels. 13 In the present study, all four patients with macro-TSH were relatively young women (27–47 years old) and had no goiter. Therefore, a more practical approach would be to target non-elderly women, particularly those with discrepancies between laboratory findings and clinical presentation, 10 in order to avoid unnecessary thyroid hormone treatment.
All patients with macro-TSH received LT4 therapy during their clinical course, which led to a modest or inconsistent reduction in TSH levels (Fig. 3). In addition, three of the four patients with macro-TSH were established to be positive for TgAb and/or TPOAb (Table 3). Although thyroid hormone replacement is generally not required for patients with laboratory-determined subclinical hypothyroidism attributable to macro-TSH, it is typically difficult to ascertain whether LT4 therapy has a detrimental effect on patients with this background.
This study has some limitations. First, this was a single-center study, in which most patients had thyroid disease and many were receiving LT4. It is thus conceivable that TSH levels, including macro-TSH, may have been modified in response to this treatment. Consequently, the generalizability of the findings to the wider population may be limited. Second, GFC was performed only for patients with a PEG recovery of <20%. Therefore, atypical macro-TSH complexes evading PEG detection may have been missed.1,5,11 Third, the macro-TSH complexes may have been weakly bound and dissociated during the GFC process, leading to potential underestimations.
In conclusion, macro-TSH is a rare, albeit clinically relevant, cause of subclinical hypothyroidism in the era of TSH harmonization. We have demonstrated that macro-TSH can be characterized by immunoglobulin heterogeneity and temporal variability, particularly in patients with autoimmune thyroid disease. A heightened awareness and appropriate confirmatory testing are essential to prevent misdiagnoses and the unnecessary administration of LT4 replacement therapy.
Data Statement
The original data generated and analyzed during this study are included in this published article.
Ethical Approval
This study was approved by the Ethics Committee of Kuma Hospital (approval number: 20230720-1).
Consent to Participate
Given that the research involved the use of preexisting clinical data and blood samples without freeze-thaw cycles before reassay stocked at −80°C, the need for individual informed consent was waived, and an opt-out consent process was implemented.
Authors’ Contributions
E.N.: Conceptualization (lead), data collection (equal), data analysis (lead), methodology (equal), writing—original draft (lead), and writing—review and editing (equal). S.F.: Conceptualization (supporting), data collection (equal), and writing—review and editing (equal). C.I.: Data collection (equal), methodology (equal), and writing—review and editing (equal). M.I.: Data collection (equal) and writing—review and editing (equal). M.N.: Data collection (equal) and writing—review and editing (equal). A.M.: Supervision (equal) and writing—review and editing (equal). T.A.: Supervision (equal) and writing—review and editing (equal).
Footnotes
Acknowledgments
The authors express our sincere gratitude to Satoru Tachibana, Keisuke Sugano, and Nonoka Tsukada for their assistance in collecting the details of clinical cases for use in this study. The authors thank Roche Diagnostics K.K. (Tokyo, Japan) for their contribution to this study and also thank Editage for English-language editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was partially supported by a research grant from Roche Diagnostics K.K. (Tokyo, Japan). The sponsor had no role in study design, data collection, analysis, interpretation, article preparation, or the decision to submit for publication. Eijun Nishihara received no individual funding for this work. Shuji Fukata received no individual funding for this work. Chisako Imamura received no individual funding for this work. Mitsuru Ito received no individual funding for this work. Mitsushige Nishikawa received no individual funding for this work. Akira Miyauchi received no individual funding for this work. Takashi Akamizu received no individual funding for this work.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.