
Abstract
Objective
The objective of this article is to analyze the features of headache attributed to hypothyroidism (HAH), evaluate the differences between groups with and without HAH, between “overt” and “subclinical” hypothyroidism groups, and evaluate outcomes after levothyroxine treatment.
Methods
Patients with hypothyroidism were selected in a cross-sectional study, followed prospectively for 12 months, and classified as subclinical or overt hypothyroidism. The patients were divided into two groups: with and without HAH.
Results
HAH was reported by 73/213 (34%) patients, involving the following areas: fronto-orbital (49%), temporal (37%), and posterior part of the head (15%). The HAH features were as follows: pulsatile (63%), four to 72 hours’ duration (78%), unilateral (47%), nausea/vomiting (60%), and moderate-severe intensity (72%). Hypothyroidism symptomatology was similar in both groups, except for a greater frequency of hoarseness in the group with HAH. Migraine history was more frequent in the patients with HAH (53% vs 38%, p < 0.05). The frequency of HAH was similar both in overt and subclinical hypothyroidism. After levothyroxine treatment 78% reported a decrease in HAH frequency. Subclinical and overt hypothyroid patients reported a similar alleviation of their headaches.
Conclusion
Patients with HAH may present with unilateral, pulsatile, episodic pattern, and nausea/vomiting, which is at odds with the criteria for HAH established by ICHD 3 beta. Not all individuals responded to levothyroxine, and patients with the subclinical form of hypothyroidism benefit from this treatment.
Keywords
Introduction
Headache and hypothyroidism are clinical conditions that cause a significant impact on the quality of life, and it is well established that both are more frequent among women (1–3). The association between headache and hypothyroidism has been known for more than 60 years (4–13).
Hypothyroidism is clinically recognized as a complex syndrome with signs and symptoms, including neuropsychiatric symptomatology, affecting most, if not all, systems of the body. It is considered a common disease, e.g. in the United Kingdom the incidence of clinical hypothyroidism was estimated at 40/10,000 women/year and 6/10,000 men/year and the prevalence was 9.3% in women and 1.3% in men (2). The disease is even more prevalent in the elderly; Sawin and colleagues (14) studied relatively healthy people between 60 and 89 years of age and found high thyroid-stimulating hormone (TSH) levels in 7% of women and 3% of men, respectively.
ICHD 3 beta criteria for headache attributed to hypothyroidism.

ICHD 3 beta: International Classification of Headache Disorders, third edition beta.
Another important study (12) reported that “new daily persistent headache” (NDPH) also seems to be associated with hypothyroidism. In a retrospective study (16), the authors pointed out that the endocrinologists failed to attach due importance to the headache in hypothyroid patients, reinforcing its importance in this still poorly understood, albeit frequent type of headache.
The aim of this study was to observe the frequency of HAH among a group of hypothyroid patients, analyze its features, taking into consideration the criteria established in ICHD 3 beta, evaluate the differences in clinical presentation between the groups with and without headache, between the “overt hypothyroidism” and “subclinical hypothyroidism” groups, and assess outcomes after the hypothyroid condition has been controlled with levothyroxine.
Methods
Between October 2008 and September 2013 consecutive patients with primary hypothyroidism, recently diagnosed at an endocrine outpatient clinic (Centro de Saúde Ana Rodrigues) in Caruaru, Brazil, were included in a cross-sectional study. After the clinical and laboratorial diagnosis the patients were prospectively followed for 12 months. To classify the patients as having HAH the following criteria were used: (i) a new headache starting in a close relation to the other symptoms of hypothyroidism or (ii) a previous primary headache, the recent worsening of which was closely related to the onset of hypothyroidism symptomatology. The ICHD 2 (2004) criteria were not used for recruiting patients. The patients’ recollection of a clear increase in frequency of their headache attacks was interpreted as the worsening of a previous primary headache. For comparative analysis the patients were divided into two groups: (1) group with HAH (GH) and (2) group without HAH (GWoH). The patients from GH were invited to describe their headache characteristics.
Migraine and probable migraine were considered as migraine and, when the patient reported the presence of both (1) headache with features of tension-type headache (including probable) and (2) migraine, he or she was considered to be a migraineur (15). The primary headaches were classified as migraine or nonmigraine using the respective ICHD 3 beta criteria.
All the patients were followed up by one of the authors (MFLC, endocrinologist with training in headache medicine) for a period of 12 months, which included visits to the clinic with new laboratory tests of their thyroid function (TSH and free T4) and thyroid antibodies, such as anti-thyroid peroxidase (anti-TPO) antibody and an evaluation to check all clinical manifestations of hypothyroidism, including the frequency, intensity and other features of the HAH for the GH after treatment with levothyroxine (dosage of 50–100 µg/day).
For the diagnosis of hypothyroidism a TSH cutoff of 5.0 mIU/l, whether or not associated with low levels of free T4 (<0.7 ng/dl), was adopted. Patients with high levels of TSH and a normal range of free T4 were classified as individuals with subclinical hypothyroidism. Patients below the age of 14 years and those with mental illness, neurologic diseases or unable to answer the anamnesis alone were excluded from the study.
Information on previous illnesses including primary headaches, family history of thyroid disease, and use of medications was added to the patient’s files. On the basis of calculated body mass index (BMI) the patients were classified into four groups: low weight (<20), normal weight (20–24), overweight (25–29) and obese (>29).
Qualitative variables were expressed through relative frequency (percentage) and absolute (n), and for the quantitative ones we used mean and standard deviation. Fisher’s exact test was applied to compare groups in their qualitative variables. Student’s t test was performed on the numerical variables age and free T4 and for the variable TSH nonparametric Mann–Whitney test was chosen when there was no normality in the distribution (Kolmogorov-Smirnov test). Statistics were performed using the Biostat program, version 5.0, and the significance level assumed was 0.05.
This study was approved by the Ethics in Research Involving Human Subjects Committee of the Federal University of Pernambuco, Brazil, protocol number 261/08. All patients were required to sign the informed consent.
Results
Baseline clinical and laboratorial features of both groups: with headache and without headache.
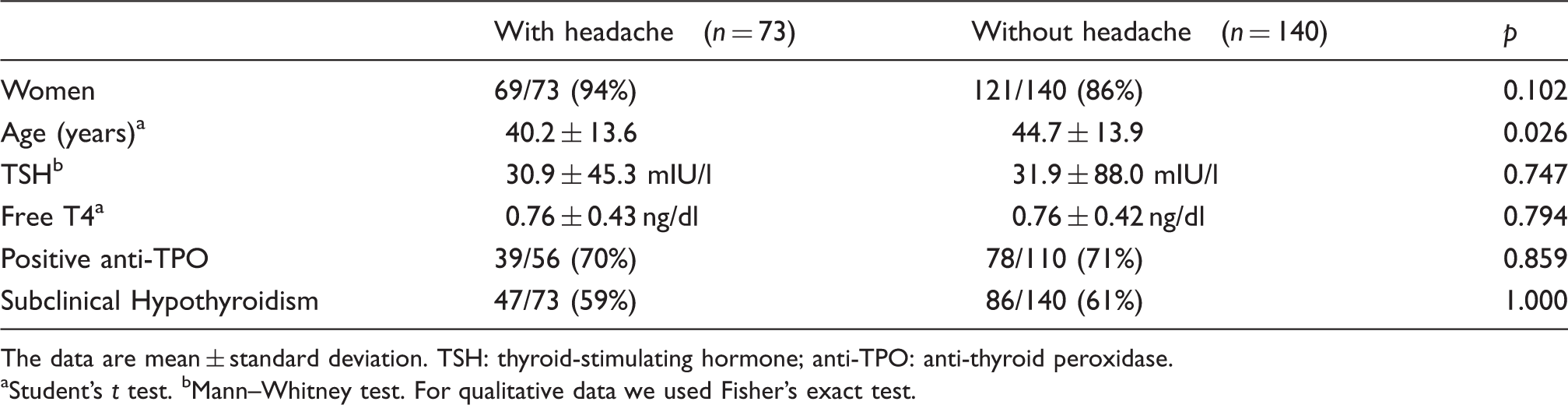
The data are mean ± standard deviation. TSH: thyroid-stimulating hormone; anti-TPO: anti-thyroid peroxidase.
Student’s t test. bMann–Whitney test. For qualitative data we used Fisher’s exact test.
The frequency (number of days with headache during the previous 28 days) before the onset of the treatment with levothyroxine was 10 ± 11 days (median 4, 1–28 days).
Demographic data of groups with headache and without headache.
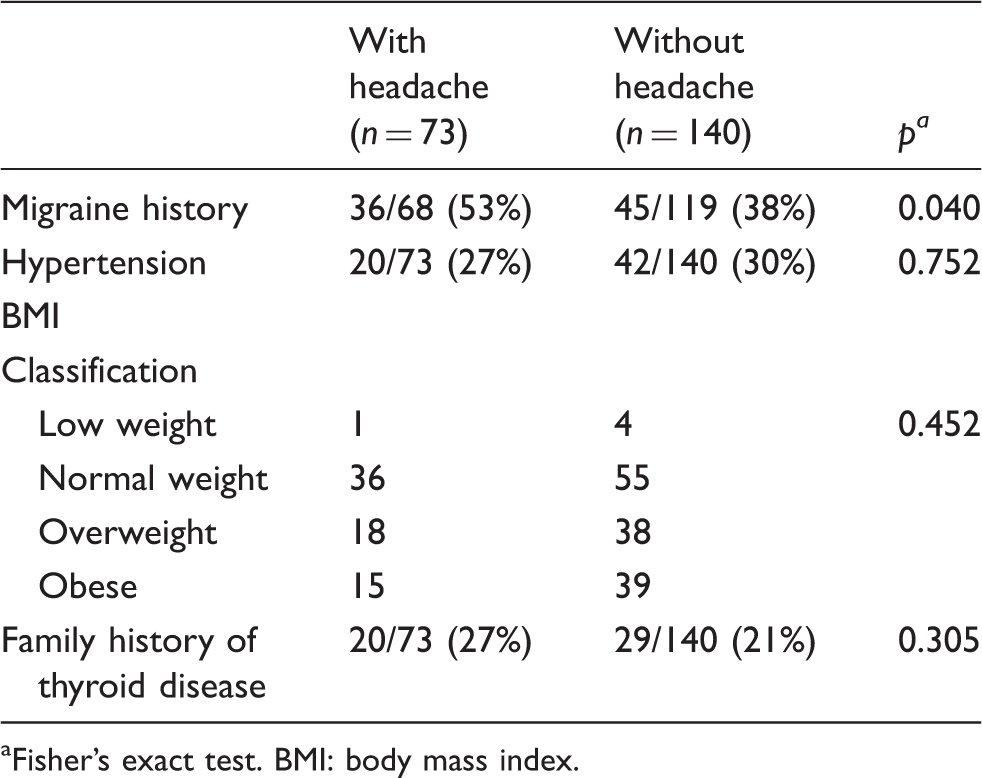
Fisher’s exact test. BMI: body mass index.
Signs and symptoms of hypothyroidism in the groups with headache and without headache.

Fisher’s exact test.
When compared with the overt hypothyroid patients, those with the subclinical form had a very similar frequency of headache (32% vs 35%, respectively; p > 0.05).
Headache features reported by patients (n = 64) with headache attributed to hypothyroidism of recent onset.

Only 64 patients completed the 12-month follow-up period.
Of the 73 patients with HAH, 64 participated in the entire 12-month follow-up, of whom 50 (78%) reported a decrease in headache frequency (more than half the days of the month) or complete remission of their headache, including an alleviation in terms of intensity, with the use of levothyroxine. Even after control of the hypothyroidism, confirmed by hormonal evaluation, 14 HAH patients did not report any relief in their headache attacks. “Subclinical” as well as “overt hypothyroid” patients reported alleviation of the headache in 37/45 (82%) and in 13/19 (68%) cases, respectively (p = 0.320).
Discussion
In assessing the importance of headache in a series of patients with hypothyroidism, our study demonstrated that approximately one-third of the patients evaluated reported HAH. This confirms what had been previously described by Moreau and colleagues (7). The ICHD 3 beta (15) has included the criteria for “headache attributed to hypothyroidism” as a secondary type of headache, probably based on the findings of Moreau et al. (7).
Nevertheless, we would like to comment on a few points raised by Moreau et al. (7) in 1998, when they evaluated 102 patients with hypothyroidism of recent onset and reported that 31 of them described a headache that was attributed to a hypothyroid condition. A history of migraine was particularly frequent in that group (i.e. 12/31, 40%), but lower than that reported by our hypothyroid patients (58%) (7). In the discussion they (7) pointed out that this type of headache (1) “begins 2 months after the onset of hypothyroidism. It is a slight but continuous, bilateral, non-pulsatile headache” and (2) “under thyroid hormonal replacement therapy, this nonmigrainous headache tends to disappear.” When we compared our findings with those of Moreau and colleagues (7), major differences can be observed, such as non-pulsatile quality (37% vs 90%), duration of four to 72 hours (78% vs 18%), unilateral location (47% vs 20%), nausea or vomiting (60% vs 0%), and mild (“slight”) intensity (28% vs 89%). To the best of our knowledge, after the publication of Moreau et al. (7), no other study involving a series of cases with hypothyroidism and HAH was published, reinforcing the importance of conducting new studies.
Another point that may be misinterpreted is the use of terms such as “continuous duration without any paroxysmal attacks” (7) and “constant over time” (15). None of the individuals evaluated in the present study reported an unremitting continuous form of headache. Hypothyroid patients may develop headache with features similar to those observed in the relatively rare primary headache known as “new daily persistent headache” (NDPH), the definition of which is also, in our view, vague (“daily from its onset, which is clearly remembered…pain becoming continuous and unremitting within 24 hours,” ICHD 3 beta) (8,11,12). Thus, without determining the duration of a continuous pain it is difficult or even impossible to establish a clear criterion. Furthermore, NDPH rarely improves with treatment, which makes some experts doubt the existence of a relationship with hypothyroidism. Furthermore, there is a discrepancy between the text and the results shown in Table 2 by Moreau and colleagues (7) regarding headache attack duration: The text states that its duration was less than 72 hours in 82% of the cases, whereas Table 2 showed the inverse. That said, the criterion 3C “Constant over time” is vague regarding duration, and is not supported by any scientific evidence and should therefore be deleted from the HAH diagnostic criteria. Similar concerns must be considered in relation to other features used as criteria by the ICHD 3 beta. For example, based on complaints reported by the present series of hypothyroid patients with HAH, the following features were observed: (1) pulsatile quality, (2) almost half of our patients reported unilateral pain, (3) it is an episodic type of headache with duration of pain < 72 hours, (4) nausea or vomiting is usually present and (5) in the majority of cases the headache is of moderate to severe intensity.
The ICHD 2 (2004) criteria for HAH were commented on by Tepper and colleagues (8): “(A) at least one of the following characteristics: continuous, bilateral, and nonpulsatile; B. Hypothyroidism is documented by appropriate tests; C. The headache begins within 2 months after the onset of hypothyroidism; D. Headache lasts < 3 months after effective treatment of hypothyroidism.” Items C and D are also included in some of the criteria established by ICHD 3 beta for “headache attributed to other disorder of homoeostasis” (10.7).
The vast majority of patients reported an improvement in their headaches within the two first months following hypothyroidism treatment.
On the other hand, the reason why not all patients with hypothyroidism of recent onset develop headache remains unknown. The rationale for comparing “headache” and “no headache” groups was to identify possible factors linked to hypothyroid patients who do develop headache. Except for a slight statistical difference in age, our results were similar between groups regarding sex, etiology and hormone levels. When taking into account their past medical history, there were no differences between groups in terms of prevalence of hypertension or a family history of thyroid disease. Considering that obesity itself is a risk factor for increased headache frequency and that patients with hypothyroidism may progress with weight gain, the two groups—GH and GWoH—had very similar BMI profiles.
In recent years the medical community has begun to pay more attention to subclinical hypothyroidism, also known as mild thyroid failure. Despite the fact that subclinical hypothyroidism is a less symptomatic disease, this condition may increase mortality (17,18). To grasp the magnitude of the problem, in the general population 3%–8% may present with subclinical hypothyroidism (19). Our data demonstrated a similar frequency of subclinical hypothyroid among patients in GH and GWoH. Moreover, with regard to HAH, both groups, subclinical and overt hypothyroid, responded similarly to the treatment with levothyroxine. The fact that patients with subclinical hypothyroidism may present with HAH and respond to levothyroxine is of major importance, demonstrating that subclinical hypothyroidism may substantially impair the quality of life of those patients. Currently, there are still arguments against the treatment of subclinical hypothyroidism. We strongly suggest treating patients with HAH. In this context, it was reported (20) previously that subclinical hypothyroidism was associated with a higher frequency of neuropsychiatric symptomatology, although hormone treatment was unable to reverse these symptoms, particularly anxiety (21).
Moreau and colleagues (7) also drew attention to the fact that the headache decreased in intensity and duration within two weeks following the start of treatment with levothyroxine in 18/31 patients and disappeared in 13/31 of the patients during the 12-month follow-up. However, these authors did not indicate whether the same participant could be in both groups.
We wish to emphasize that 38% of patients without HAH (GWoH) reported a previous history of migraine. We therefore presume that hypothyroidism did not influence the frequency or intensity of the previous usual manifestations of migraine, at least in these patients. On the other hand, a previous history of migraine was more prevalent in the “headache group,” which is in accordance with the ICHD 3 beta (15). Headache attributed to hypothyroidism may indeed occur in patients with previous migraine if one accepts the definition of HAH as an exacerbation of the migraine attacks (9).
In general, as seen in headaches attributed to other disorders of homoeostasis, improvement or complete relief of symptoms is to be expected for the majority of such patients, following appropriate treatment of the underlying disease (15). An improvement in the headache was observed in more than two-thirds of patients after treatment, which suggests that thyroid disease may play an important role in the nociceptive mechanism of pain deflagration. Regarding the lack of response to treatment of hypothyroidism after levothyroxine observed in a few of the patients with HAH, even after a 12-month follow-up period, we recognize that this may have occurred, in part, because of the relatively high prevalence of migraine sufferers among our HAH patients, which may have changed the profile of migrainous characteristics. Spontaneous oscillations in the profile with changes in frequency or transformation from an episodic form to a chronic one are by no means rare in migraineurs. Considering the idea that HAH promptly responds to the treatment of hypothyroidism with levothyroxine, the use of classical preventive drugs in these patients is not required. But, based on our data showing that one-third of patients failed to respond to levothyroxine treatment, the authors suggest that, if the headache persists after three months of levothyroxine administration, a combination of preventive drugs be used with levothyroxine.
We still do not know whether a longer period of treatment is required in order to obtain a satisfactory relief of the HAH. In such cases, when there is a failure after hormone replacement and the headache persists, we recommend further investigation, including evaluation with neuroimaging in order to rule out other possible secondary causes, such as pituitary adenoma (22), cerebral venous thrombosis (23), among other conditions, that might coexist with low levels of thyroid hormones. Even the treatment with levothyroxine may be a cause of headache: The development of pseudotumor cerebri associated with levothyroxine administration has been reported (24).
Some patients with HAH, particularly children or adolescents, may be misdiagnosed as having a pituitary TSH- or prolactin-secreting adenoma (25–28). In this connection, serum prolactin concentration may rise during a hypothyroidism state and patients with “pseudoprolactinoma” due to primary hypothyroidism have been operated on mistakenly (28). Chan and colleagues (28) recommend that thyroid tests be performed in all patients with pituitary enlargement prior to a surgical procedure in order to exclude hypothyroidism-induced pituitary swelling. Lee et al. (29) observed a rapid progression of hypothyroidism-related pituitary hyperplasia within a four-week interval in a 10-year-old girl who demonstrated a rapid progression in her gland enlargement due to low levels of thyroid hormones. On the other hand, Kocova et al. (30) reported the case of a girl, at an early stage of puberty, with primary hypothyroidism, a high TSH concentration and hyperprolactinemia. A large intrasellar mass expanding beyond the sella, indicative of a dramatic pituitary hyperplasia, was found. A resolution of the pituitary hyperplasia was observed within 40 days after levothyroxine treatment. This is similar to the period in which a response is expected to be observed in patients with HAH (30).
A case of a 43-year-old man with a three-year history of headache and delayed puberty was also reported (31). Congenital hypothyroidism was diagnosed and a giant sellar pseudotumor with suprasellar extension causing cerebrospinal fluid obstruction and hydrocephalus was demonstrated. After hormone replacement therapy a significant decrease in the size of the mass was observed, with resolution of the hydrocephalus. These examples clearly demonstrate that the headache or its resolution may be caused by, respectively, the growth of a pituitary gland or to its reduction after treatment.
With regard to the patients with HAH who fulfilled the criteria for migraine but with no previous history of migraine, we believe that such patients may not have a true migraine, but rather, a headache triggered by thyroid dysfunction, in other words, an HAH with migraine-like characteristics.
The pathophysiology of the HAH remains largely unknown. We will discuss some lines of evidence that may explain, at least in part, the mechanism involved in the genesis of the HAH. Pituitary growth associated with high TSH levels and a possible “mass effect” (compression of painful intrasellar structures) have been proposed and mentioned above as one of the mechanisms of HAH (32). Hypothyroid patients may also present with high prolactinemia, and prolactin itself has been implicated as an adjunctive headache-worsening factor (33). Interestingly, the ICHD 3 beta has included headache secondary to pituitary adenoma and hypo- or hypersecretion of the gland, which may cause the “mass effect” (15). Moreover, the clinical criteria (e.g. evidence of improvement in parallel with the control of hormone (TSH and/or prolactin) levels) account for the characteristic pattern in HAH, as the appropriate treatment would cause a reduction in the volume of the previously enlarged pituitary gland, resulting in a clinical improvement in the pain. Levy and colleagues (34), however, have suggested that pituitary volume may be less important than genetic factors and hormone function. Further studies should be conducted in order to evaluate the relationship between the pituitary gland and the volume of the intrasellar compartment in patients with HAH. The hypothesis is that patients with hypothyroidism who do not develop HAH have an intrasellar volume larger than that of an enlarged pituitary gland, if this is indeed the mechanism involved in the genesis of HAH.
In addition, the nociceptive threshold was, in one study, proved to be strangely higher in hypothyroid patients when compared with healthy control individuals, returning to normal six weeks after treatment of the thyroid insufficiency with thyroxine (35). Other authors have mentioned the possibility of thyroxine antinociceptive effects through the elevation of platelet serotonin, prostacyclin metabolism or vasomotor activity following treatment with levothyroxine (7), which could also contribute to an excellent outcome, at least regarding migrainous features. The involvement of purinergic transmission has also been postulated (8,36).
Hypothyroidism and headache are conditions frequently associated with each other. Nonetheless, a routine trial of TSH in headache patients has still not been established, although this has been suggested in relation to migraineur children (9). Since hypothyroidism is particularly frequent among women (prevalence up to 8%–20% depending on the age group), the present authors recommend routine evaluation of TSH and free T4 in adult women with headache, particularly those with episodic migraine that has progressed to a chronic migraine or individuals with headache of recent onset (e.g. NDPH) (12).
It is not possible to determine whether a hypothyroid individual will or will not have headache on the basis of the variables investigated in our study. Migraine history is a frequent finding in patients with headache and hypothyroidism. Some hypothyroid patients may report headache features other than those described for HAH by ICHD 3 beta, or we may even encounter, in some cases, some features attributed to HAH overlapping with those of primary headache such as migraine.
Although hypothyroidism has been considered a migraine comorbidity (37), Amy (38) did not find any case of hypothyroidism among 21 chronic headache patients, and Hagen and colleagues (39) found a low headache prevalence among women with high TSH values. Regarding limitations of our study, we would like to comment that a large amount of data was based on patient recall. Without using the tension-type headache ICHD 3 beta criteria, we classified primary headache as migraine or non-migraine. No cluster headache patient was included in this series, although patients with primary stabbing headache are very probably present in our study population.
In conclusion, as demonstrated in the present study, the International Headache Society criteria should be refined regarding the HAH features presented in this paper. Patients with or without a previous history of migraine may present with a unilateral, pulsatile, episodic pattern, nausea and vomiting, which is at odds with the criteria for HAH established by ICHD 3 beta. The question remains as to whether migraineurs with hypothyroidism have a “true” HAH or whether their migraine attacks worsened with this new hormonal dysfunction.
Clinical implications
Headache attributed to hypothyroidism (HAH) is a common complaint among hypothyroid patients. It is still not possible to determine who is more susceptible to suffer from HAH among hypothyroid patients. Treatment of the basal condition is effective in the relief or remission of headache in the majority of hypothyroid patients with HAH. Patients with HAH may present with a unilateral, pulsatile, episodic pattern, and nausea and vomiting, thereby contradicting the criteria for HAH established by the International Classification of Headache Disorders, third edition beta.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.