
Abstract
Background
Many studies exist outlining poor outcomes related to cardiopulmonary resuscitation (CPR) administered to patients who are elderly and/or have comorbid medical conditions with sudden cardiac arrest. Patients with asystole or pulseless electrical activity have worse outcomes. Studies show only 10% of patients with out-of-hospital cardiac arrest and initial asystole survive until they reach the hospital. Less than 5% survive until hospital discharge with good neurologic function.
Research Question
Given these poor outcomes, the question arises: what are the impacts on the healthcare personnel providing this type of aggressive intervention?
Study Design and Methods
The study design was a cross-sectional, mixed-methods anonymous online survey of hospital personnel in one large academic setting. The survey included demographic questions and 6 questions regarding feelings around the use of CPR. Descriptive statistics were used to report on respondents and their responses. Thematic qualitative analysis of free-text responses was completed.
Results
One-hundred fifty-four people of 780 (20%) responded to an anonymous survey sent to hospital personnel. Ninety-four percent of respondents were involved in a hospital code experience; 87% surveyed had performed CPR on an individual knowing there was a low likelihood of survival. Eight themes with subthemes were identified in the data. Participants primarily had challenging emotions associated with taking part in CPR including sadness and frustration.
Conclusions
A large majority of healthcare workers surveyed in a single hospital system reported performing CPR on patients knowing there was a low likelihood of survival. Many respondents reported emotional effects.
Keywords
Background
Myriad studies exist outlining poor outcomes as they relate to cardiopulmonary resuscitation (CPR) administered to patients who are elderly and have multiple comorbid conditions after sudden cardiac arrest (SCA). Those that present to the hospital with asystole or pulseless electrical activity (PEA) have the worst outcomes. 1 Studies show that only 10% of patients who have out-of-hospital cardiac arrests with initial asystole survive to reach the hospital. Less than 5% survive to discharge from the hospital with good neurologic function. Individuals with PEA have similarly poor outcomes. 2 The risk of SCA and out-of-hospital cardiac arrest increases with age. Patients who experience cardiac arrest while in the hospital have survival-to-hospital discharge rates varying from 6-19%. Younger patients with normal baseline neurological function and few medical issues have better outcomes after SCA. 3
Given the data that exists for certain patients undergoing CPR after SCA, the question arises: what are the impacts on the healthcare personnel responding to “codes” after sudden cardiac arrest who provide aggressive interventions that involve CPR? 4
The primary objective of this study was to provide qualitative and quantitative data related to healthcare workers participating in codes that involve CPR of patients. Our study specifically looked at the emotional and ethical impacts of these events on healthcare workers when they felt that the patient involved had a small chance of survival due to multiple comorbid conditions and advanced age.
Lastly, we wanted to gauge the interest of these healthcare workers in participating in hospital-system sanctioned debriefs after codes. There might be some debate on the implementation of “sanctioned” debriefs but the literature does illustrate some effective strategies that might mitigate the effects of moral injury related to participation in aggressive end of life procedures. Certainly, interventions such as debriefing could facilitate unintended consequences to an individual. Uniquely, our study included written responses and a subsequent qualitative analysis alongside the quantitative descriptive statistics. 5
Study Design and Methods
The study design was a cross-sectional, mixed-methods anonymous online survey. The survey was sent to existing email lists of healthcare personnel that worked within the Community Health System hospital system that consisted of hospitalists, nurses on the medical/surgical and intensive care units, and faculty and trainees. The survey comprised demographics such as age, gender identity, and position within the medical system. The participants answered 6 yes/no questions about their emotional experiences and ethical perspectives related to performing CPR. Participants were provided with the opportunity to expand on their answers to all of the yes/no questions through free-text response options after each question. They were also given the opportunity to add comments at the end.
The survey was distributed online using Qualtrics, a web-based survey software platform. The software created an anonymous link to the survey that was included in an email requesting their participation. The recipient was able to click on the link in order to participate in the survey (opt-in). A reminder email to complete the survey was sent 14 days later. Institutional Review Board (IRB) approval was obtained through our teaching hospital.
Statistical Analysis
Quantitative
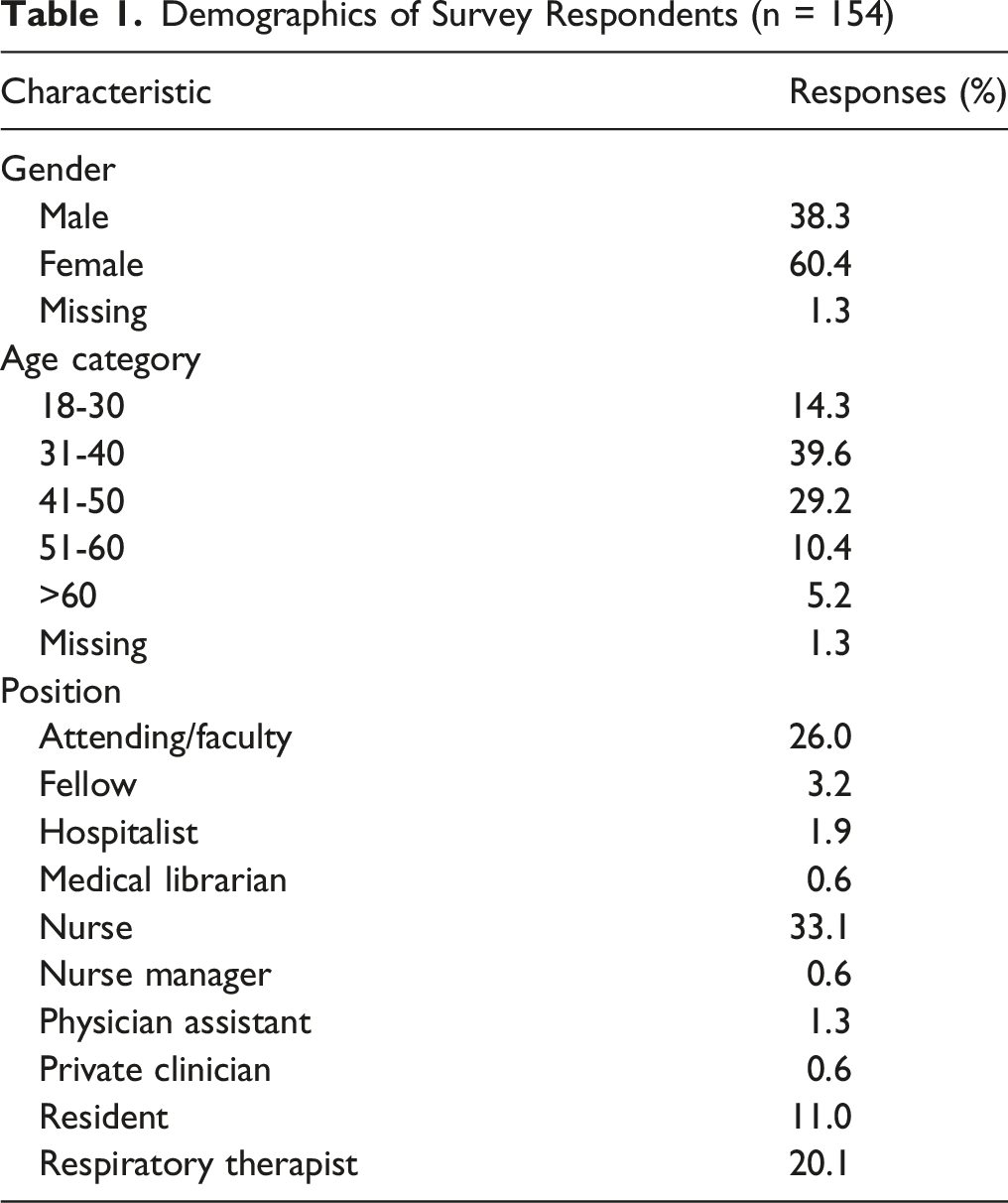
Percentages of respondents by age group, gender identity, and position within the hospital system were calculated. Percentages of responses of personnel with hospital code experience were also calculated.
Qualitative
All participants who provided at least one free-text response were included in the thematic analysis. Author I.P. applied an inductive, reflexive thematic analysis using NVivo 14 software, consistent with the established approaches described by Virginia Braun and Victoria Clarke. 6 Reflexive coding emphasizes the researcher’s active role in interpreting data and acknowledges coding can be either an individual or collaborative process, as subjectivity is the primary tool and resource for interpreting data. 6
Initially, I.P. familiarized themself with the data by thoroughly reading and re-reading the responses, noting preliminary ideas and patterns. Codes were generated inductively to capture the key features of the participants’ experiences. Throughout the process, reflexivity was used to critically examine how interpretations developed, with codes iteratively reviewed and refined to ensure consistency and coherence. Codes were subsequently organized into broader themes and subthemes that reflected patterns of shared meaning across providers’ experiences with CPR. Themes were reviewed and refined to ensure they accurately represented the dataset, and each was defined and clearly named.
Given study resources, the qualitative analysis was conducted by a single reflexive coder (I.P.), who has 9 years of experience in graduate medical education research, including both quantitative and qualitative surveying and interview methods and data interpretation. A single coder could introduce subjectivity and limit the opportunity for external validation. Multiple coders enhance credibility, but reflexive thematic analysis does not require inter-coder agreement as a marker of accuracy or objectivity. Future work may incorporate multiple coders to further enhance understanding of the data.
Results
Quantitative
Demographics of Survey Respondents (n = 154)
Survey Questions and Responses of Personnel With Hospital Code Experience (n = 145)
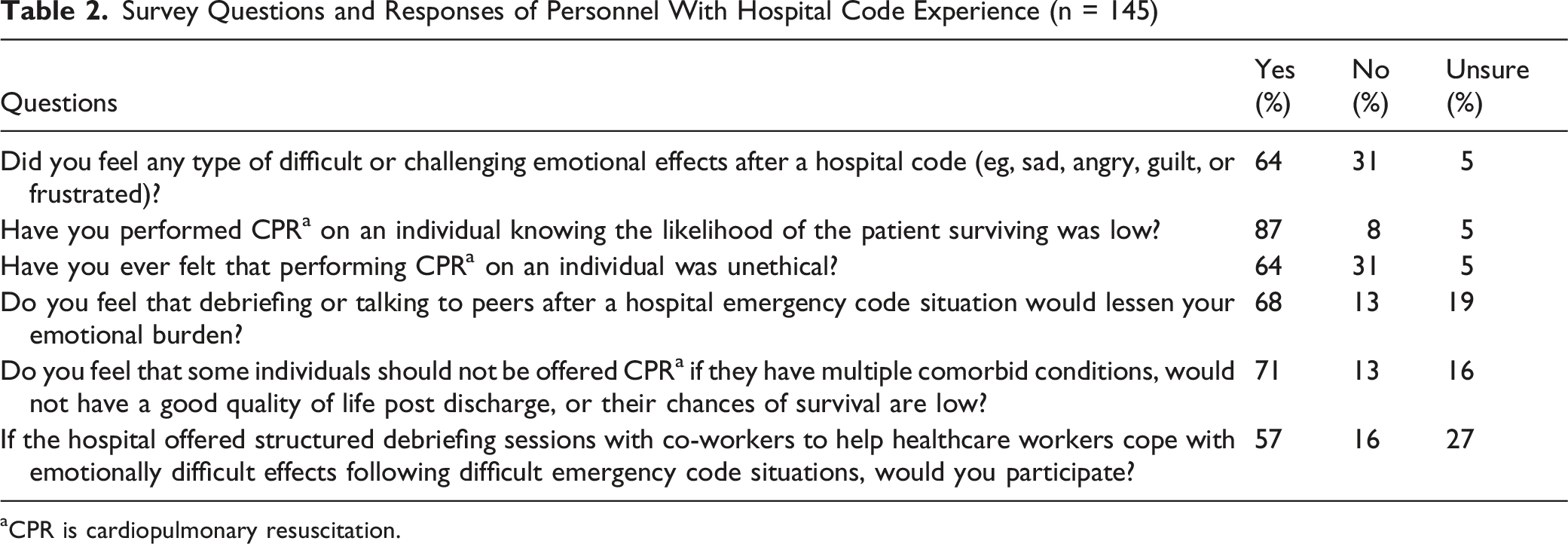
aCPR is cardiopulmonary resuscitation.
Qualitative
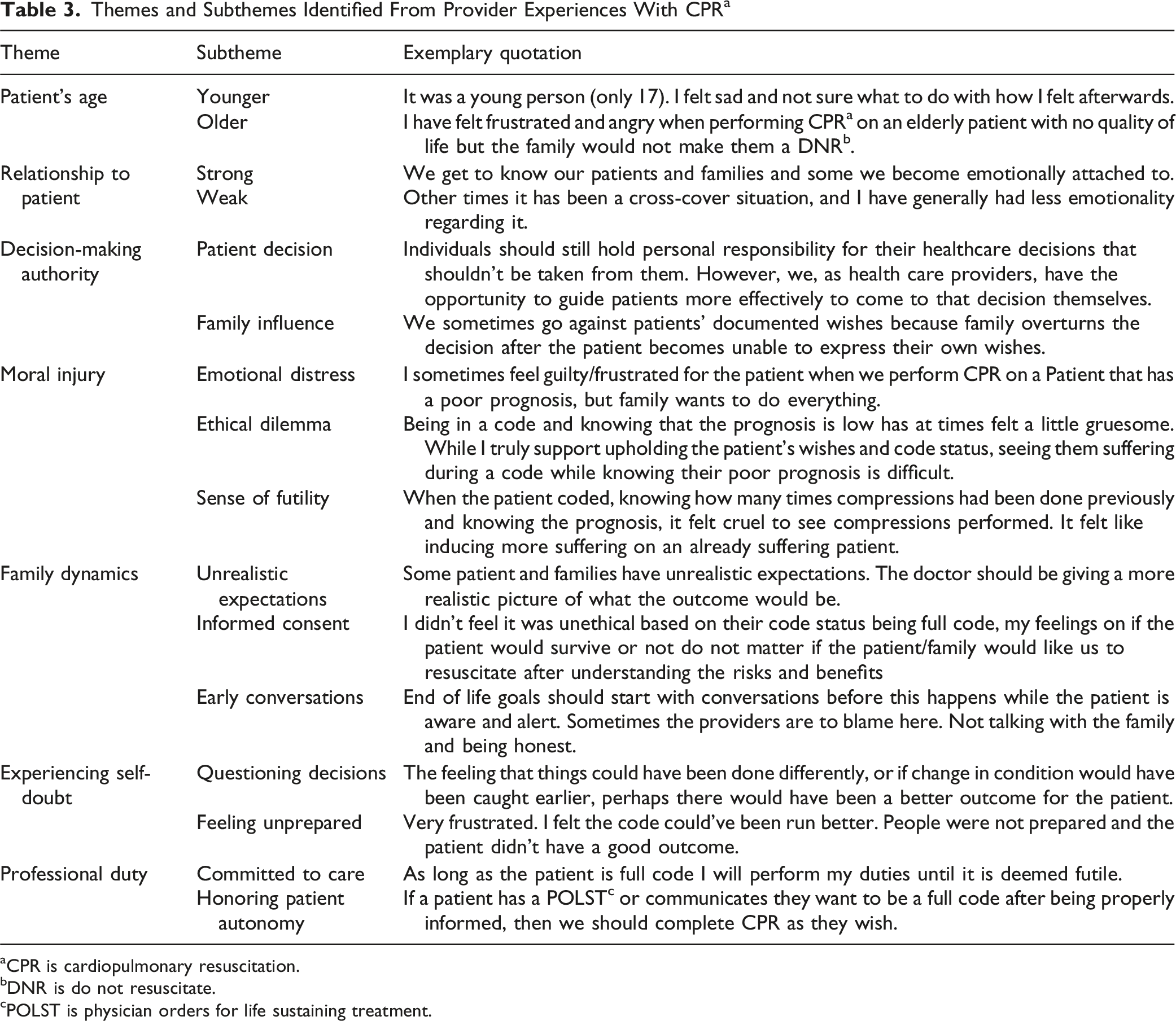
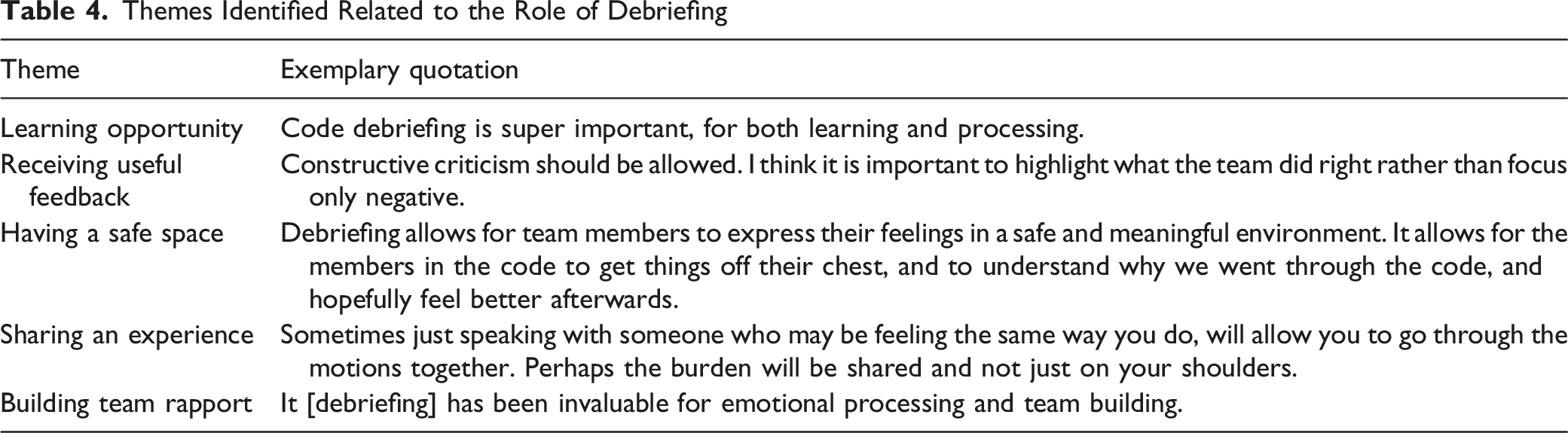
The analysis included 82 of the 154 respondents who provided at least one free-text response. Participants primarily had challenging emotions associated with taking part in CPR. Figure 1 is a word cloud of the emotions they reported experiencing during a hospital code experience. Table 3 presents 7 themes with subthemes identified and an exemplary quotation for each. Debriefing was a significant theme among the participants’ responses and thus is presented in Table 4, along with exemplary quotations related to debriefing. Word cloud of emotions reported by participants Themes and Subthemes Identified From Provider Experiences With CPR
a
aCPR is cardiopulmonary resuscitation. bDNR is do not resuscitate. cPOLST is physician orders for life sustaining treatment. Themes Identified Related to the Role of Debriefing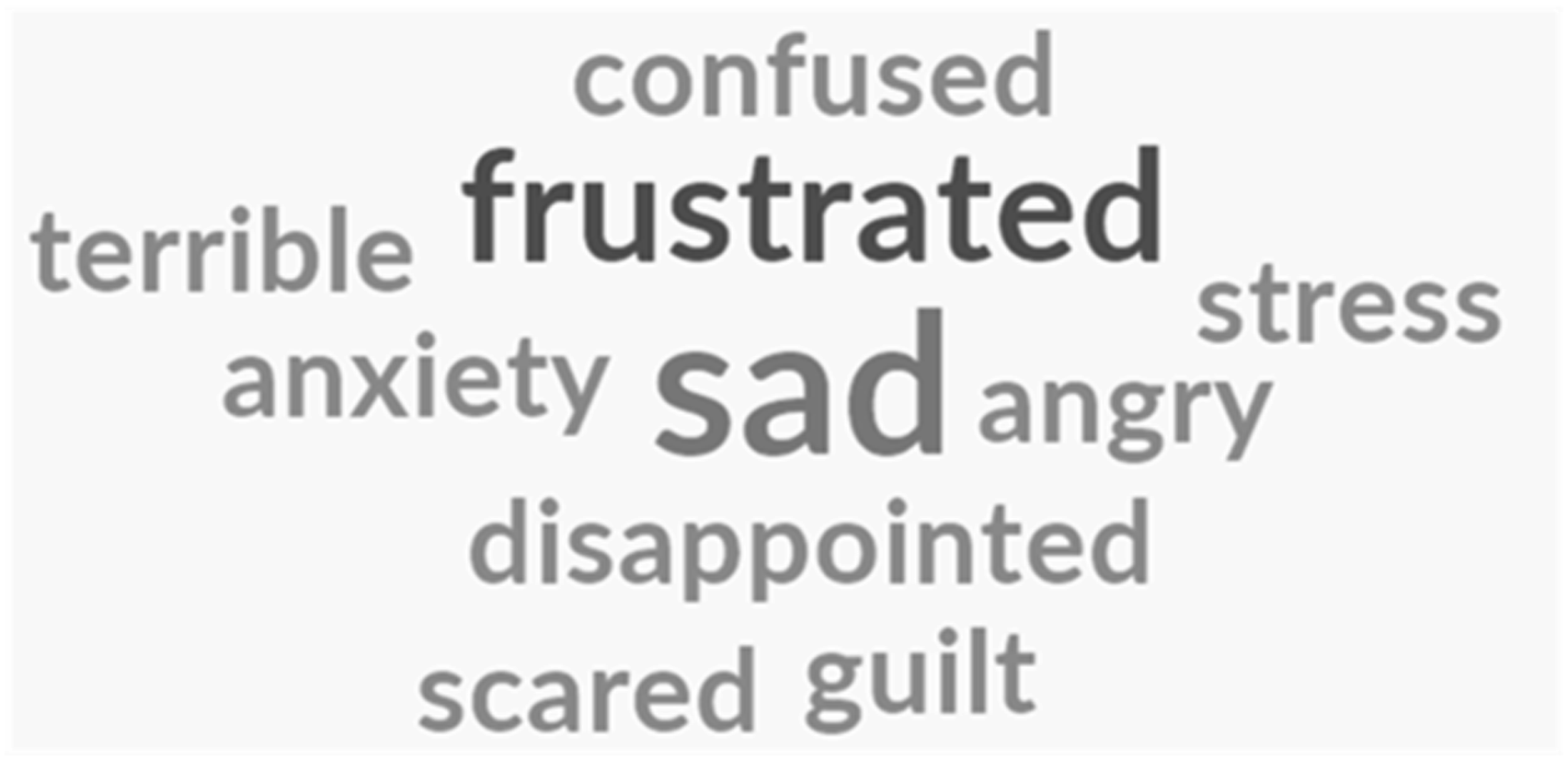
Themes
The qualitative analysis revealed the following themes related to performing CPR. Participants often used the term ‘code’ to denote CPR in their responses. Therefore, quotations may include ‘code’ and this distinction is made to prevent confusion with the coding process used in thematic analysis.
Patients Age
The age of the patient was found to be an important factor in how affected a provider would be during a CPR experience. CPR involving younger patients was described as more traumatic and difficult to process. One participant wrote, “Pediatric codes are worse since I have children. Sometimes you want to cry but you have to keep on working.” Performing CPR on older patients was also challenging, but it affected providers differently, as they felt such cases were more expected. However, they still felt like some patients were subjected to unnecessary CPR, with 1 participant stating older patients were being “subjected to futile pain and invasive procedures at the end of their life.”
Relationship to the Patient
The emotional distance between a provider and patient impacted the strength of their emotions after participating in CPR. If they were more familiar with the patient and had developed an emotional attachment, they felt stronger emotions related to performing CPR. One participant captured this theme by responding, “[I] have been involved in many dozens of codes during residency so far, and some provoked those feelings, others not, [it’s] highly dependent on the situation.” This indicates that emotional responses to CPR will differ and be guided by multiple factors that include emotional distance.
Decision-Making Authority
Participants commented that the decision-making authority of the patient and family plays a role in their feelings after CPR. Participants felt that the patient’s decision was the most important factor and expressed that tensions rise when the family’s decisions differ from the patient’s preferences regarding CPR. One participant noted, “Individuals should still hold personal responsibility for their healthcare decisions; that shouldn't be taken from them. However, we, as health care providers have the opportunity to guide patients more effectively to come to that decision themselves.”
Moral Injury
Moral injury is the psychological, social, and spiritual impact an individual experiences if they feel that there was a betrayal or violation of their moral values. The impact of moral injury was identified in the responses, but also appeared throughout all the themes. Phrases, for example, “unethical,” “contrary to oath,” “seems like torture,” and “needless suffering” were observed, among other comments that showed providers are strongly affected by performing CPR when they feel their moral values have been violated. They reported feeling guilty and conflicted when they performed CPR on a patient who had a poorer prognosis in terms of survival. Those feelings led to a sense of futility and an ethical dilemma where they wanted to uphold the patient’s and family’s wishes but felt that a particular patient should not receive CPR.
Family Dynamics
The impact of family dynamics on their emotions was a major theme among the participants. Many felt the families had unrealistic expectations and went against the patient’s wishes. Participants responded that it seems like sometimes, “family members don’t know how to let go” and “when a patient is known to be imminently or actively dying (and CPR is of no benefit), but the family insists on us performing CPR, I feel angry and sad.” Some participants expressed that if the patient and/or family were properly consented, providers should honor the patient’s and/or family’s wishes, even if they disagree with performing CPR. There was a significant consensus that conversations surrounding end-of-life care and code status need to be happening earlier, and that it is the provider’s role to educate and guide patients and their families in making decisions that best align with their values.
Experiencing Self-Doubt
Participants described second-guessing their decisions made during CPR. Some experienced doubt long after performing CPR, and they grappled with the uncertainty. One participant reflected on a specific experience involving a patient being moved from the ICU expressing uncertainty about the decision: “questioning whether they should have come out of the ICU that morning although [the] code would have just happened there [outside of the ICU] instead.” Part of the doubt for some participants was from feeling unprepared. Participants described some code experiences as being frustrating because supplies were not available or roles were not well defined, which added to the chaotic environment of the hospital code experience.
Professional Duty
Participants emphasized that regardless of their personal opinions, they are obligated to perform CPR according to the POLST or the patient’s and family’s preferences and should continue to do so until the patient is confirmed to have expired. A participant commented that performing CPR is “part of my job and goes with the territory of working in a hospital.” They felt it was important to be fully committed to the patient’s care, and as providers, “we have to give it 100%.” They also expressed that providing the highest quality of care honors the patient’s autonomy, emphasizing their responsibility to act decisively in critical moments: “All emotions are present because you are the person taking care of this patient, and your role is to do everything to save their life.”
Debriefing
Debriefing was an important theme in the participants’ responses. They felt it was an important learning opportunity and should be done regularly. They saw debriefing as valuable when the feedback was useful and not overly critical. Multiple participants used the words “safe space”, indicating that safety needs to be established for debriefing to be effective. Having a shared experience also was important because it provided emotional relief and helped them process the hospital code experience. A participant responded, “I believe keeping emotions to myself or ignoring them is not healthy. [It] not only helps my mental health to debrief, but also helps the people that I am sharing with.” Others expressed similar ideas that debriefing is healthy, and colleagues should not sit alone with their emotions.
Discussion
This study presents data that suggests that there is an association between moral distress and performing CPR on individuals who are elderly with multiple comorbid medical conditions. Specifically, most of our respondents felt they performed CPR on individuals when expectation of survival was low. More than sixty percent of our respondents were challenged emotionally during these types of code situations, and a similar number of healthcare workers felt the code could be considered unethical. Limitations of the study include the relatively low number of respondents, and that data was collected from only one hospital system.
Prior research helps us understand some factors that contribute to CPR being performed on frail and elderly patients. A 2015 study showed that nearly 3 quarters of all “codes” on television were successful. 7 Despite the numerous studies validating poor outcomes in elderly and chronically sick patients receiving CPR in the setting of sudden cardiac arrest, many still pursue that option in hospital settings.
The emotional and ethical challenges faced by healthcare providers during CPR and end-of-life care are multifaceted and deeply impactful. Our qualitative analysis revealed several key themes that have an emotional impact on the healthcare provider including decision-making authority, moral injury, and the importance of debriefing. We were particularly interested in the emotional responses of the survey participants and the moral distress that appears evident when participating in medically non-beneficial rapid response or code scenarios. This study’s results align with 2 studies that noted that providers experience an emotional toll after participating in intensive treatments when they perceived CPR was futile. 8 Moral injury emerged as a significant theme, with providers expressing feelings of betrayal when performing CPR that they deemed unnecessary. This also aligns with the ethical dilemmas described in those same papers, where providers felt conflicted about avoiding patient suffering while respecting patient’s and family’s wishes. At our hospital, we have a respecting life choices program designed to value the decisions our patients make regarding end-of-life care. Additionally, we have a policy at our hospital for medically non-beneficial treatment or futility of care. How can we strike a balance between both? How do we value the workforce in our healthcare system and the patients we serve in the arena of end-of-life care?
Our respondents indicated that end-of-life care is particularly burdensome when involving younger patients or those with multiple comorbidities, emphasizing the heightened emotional strain in these scenarios. The relationship with the patient also influenced emotional responses, consistent with the findings that close relationships can intensify the emotional burden of end-of-life care decisions. 9 It also affects the ability to be objective when having end-of life discussions or prognosticating.
We think the addition of a qualitative analysis to a subject such as this allows a more personal look behind the statistics. More studies need to be conducted in hopes that a larger discussion can address the statement, “just because we can do it, doesn’t mean we should.” Medical personnel are a precious commodity, and the question remains: why do we subject our medical staff to emotionally injurious situations that could be avoided? Are there ways the hospital or healthcare systems can better address goals of care discussions to avoid aggressive interventions at the end-of-life that would be considered non-beneficial to the patient? Certainly, the increase in palliative care services helps with guiding families and patients through goals of care discussions. Ethics committees can also help support the medical team, but a shift in how we approach end-of-life decisions and care must lead the way.
More than half of respondents in our study were receptive to a debrief following a code situation. The aforementioned study found that “Interprofessional collaboration, teamwork, and regular interdisciplinary debriefing were associated with a lower risk of intention to leave the job.” 9 In addition to debriefs, other approaches to stress management and continued wellness may be recommended. Our fellowship program developed a wellness curriculum that involves contemplative practice to assist our trainees to address compassion fatigue and burnout. Other individualized ways of stress reduction include meditation, yoga or other wellness practices that focus on individual preferences since group exercises can be intimidating. 10 , 11 Stress inoculation training can also be implemented. This cognitive behavioral intervention, originally developed by Donald Meichenbaum, instructs individuals on how to manage anxiety. It has been effective in establishing resilience strategies in the healthcare field. 12 Finally, psychological first aid, which was used during the COVID-19 pandemic, can also be a model for the healthcare industry to combat burnout. Making different stress management approaches, such as debriefing, optional may decrease the anxiety associated with a group setting but could also decrease the possibility of the positive effects when individuals choose to “opt out” or participating.
Lastly, how does the medical or healthcare system empower physicians or other providers to make clinical decisions based on science and not the emotions of family members or patients? How do we blend compassion with effective language about prognosis and survival when having these discussions?
Conclusions
A large majority of healthcare workers surveyed in a single hospital system reported performing CPR on patients knowing there was a low likelihood of survival. Many respondents reported emotional effects. A majority felt it was unethical to perform CPR on patients under certain conditions. More than half of respondents believed participating in debriefs could be helpful, and a majority felt that not offering CPR in certain cases was appropriate.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.