
Abstract
Purpose
To identify disparities in access, utilization, and quality of end-of-life (EOL) and palliative care services for American Indians and Alaska Natives (AIAN) with cancer in the US.
Methods
Systematic searches were conducted in PubMed/MEDLINE, Embase, and Scopus. English-language original research studies reporting any quantitative estimates of measures of care quality or utilization for EOL and palliative care for AIAN individuals with cancer compared to other races were included (2014-2025). Screening and data extraction were conducted by two independent reviewers and discrepancies were resolved through consensus. Findings were synthesized through iterative team discussions.
Results
Of 1693 unique records, 153 underwent full-text review, and 22 met inclusion criteria. Considerable heterogeneities were observed in EOL care outcomes and covariates included in multivariable regression models assessing disparities: Compared to White individuals, AIAN individuals with cancer had significantly lower in-home or hospice and higher medical facility deaths (9/11 studies); higher acute care use (3/4 studies); lower hospice use (2/4 studies); lower anxiolytic medication use (1/1 study); and higher receipt of any palliative treatment (3/6 studies); but no differences in late hospice initiation (0/3 studies); or aggressive treatment near the EOL period (0/6 studies).
Conclusions
AIAN individuals with cancer appear more likely to experience a medicalized death. Mechanisms underlying these disparities remain poorly understood. Future studies should provide greater clarity in analytical methods to improve interpretability of disparities measures, use more consistent measures of EOL care quality, explore within-AIAN variation such as regional, tribal, and rural–urban differences, as well as cultural implications for the delivery of appropriate EOL care.
Keywords
Introduction
Throughout history, care for the dying has often involved ceremonies, music, storytelling, and rituals, aimed at helping the person and their loved ones feel more comfortable making a natural life transition. 1 End-of-life (EOL) care, defined as the medical care and support received at the time surrounding death, 2 is a unique experience for each individual, where the goal is providing compassionate, person-centered, and family-oriented care to reduce suffering, provide comfort, and maintain or improve quality of life. 3 For individuals with serious illness such as cancer, appropriate EOL care, including hospice care and other palliative care services, improves quality of life for the patient and caregivers,4-6 and reduces the costs associated with excessive medicalization, prolonged hospitalization, and receipt of futile aggressive treatments.7,8 Despite these benefits, many individuals with cancer in the US continue to experience suboptimal and often value-discordant EOL care, 9 characterized by excessive medicalization, receipt of aggressive treatments, and underuse of symptom management, palliative care, and hospice services, leading to a higher likelihood of dying in medical facilities. These patterns are especially pronounced among minoritized racial and ethnic groups.10-18
From the 2020 Census, about 9.7 million people (∼3% of the US population) identified as American Indian and Alaska Native (AIAN). 19 AIAN people are highly diverse in culture, history, and geography, representing 574 tribes and people groups recognized by the US federal government and more than 200 not recognized by the US government that may be recognized by the state in which their tribal homelands are located. Persistent health disparities, i.e. unjustified and preventable differences in health outcomes, 20 have been widely documented for AIAN populations. 21 These disparities do not merely reflect individual preferences but are rooted in longstanding structural inequities in socioeconomic status, healthcare access, cultural communication barriers, historical trauma, and medical mistrust.22-25 For instance, compared with about 10% of non-Hispanic Whites in the US, about 22% of AIANs experience poverty with rates exceeding 60% in some tribal areas and reservations. 26 AIAN individuals are also more likely to be uninsured (approximately 20%) and reside in rural areas. 26 Parallel to the socioeconomic differences, AIAN individuals with cancer often experience greater symptom burden across the illness trajectory and higher mortality rates. 27 Limited EOL care offered by tribal organizations may contribute to these patterns by leaving patients and families to seek such care outside, where culturally sensitive EOL care is less available. 28 This lack of proper EOL care can lead to more pain, financial hardship, and caregiver burden for AIAN individuals and their loved ones during an especially vulnerable period.
Healthcare disparities are not immutable. In addition to efforts addressing disparities in disease prevention, treatment, and life expectancy, policy makers and clinicians share a responsibility to work towards eliminating disparities in the quality of care that individuals receive near their end of life, as ensuring a “good death” for all is a fundamental goal of the healthcare systems. 28 We aimed to review the existing evidence on disparities in EOL care access and quality for AIAN populations with cancer in the US. To better understand and address EOL care in this vulnerable population, we provide policy, practice, and research recommendations based on the results of our review.
Methods
The protocol for this scoping review was developed according to Arksey and O’Malley’s framework. 29 We decided to conduct a scoping review to characterize the range of existing evidence, clarify key concepts, examine emerging research areas from various study designs and outcomes, map key findings, and identify knowledge gaps to guide future research. 30 This paper follows the Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for scoping reviews. (PRISMA-ScR). 31
Databases and Search Strategies
PubMed/MEDLINE, Embase, and Scopus were systematically searched for any peer-reviewed studies published through February 2025, with no restrictions on the earliest year of publication. A health sciences librarian helped develop and refine the search strategies (available in Supplementary Materials). All retrieved records were uploaded to Covidence (Veritas Health Innovation, Melbourne, Australia) for screening.
Study Selection and Inclusion Criteria
After removing duplicates in Covidence, records were reviewed through a two-step process: (i) screening titles and abstracts for relevance, followed by (ii) full-text review of the selected records to evaluate eligibility based on predetermined criteria. In both steps, two authors independently reviewed and voted for inclusion of the record. Discrepancies were resolved through regular consensus meetings.
Studies were included if they met the following criteria: (i) focused on AIAN individuals with cancer; (ii) studied outcomes relevant to access, utilization, or quality of EOL care or palliative care near EOL; (iii) provided quantitative results for AIAN individuals (i.e., not aggregated with other racial/ethnic groups) compared to other races; and (iv) published as full-text original research in English, with no restrictions on publication year (the earliest included study was published in 2014). Original qualitative research studies are reported in a separate paper to allow for more in-depth analysis. Conference abstracts, reviews, commentaries, book chapters, protocols, and editorials were excluded.
Data Extraction
Data abstraction was conducted as per a pre-established form by two independent investigators and discrepancies were resolved by a third reviewer. Quality appraisal of the included studies is not recommended in the context of scoping reviews and was not conducted. 29
Conceptual Framework and Evidence Synthesis
Consistent with a socioecological view, access to, utilization, and quality of healthcare services are influenced by an array of complex and interconnected factors at multiple levels (i.e. individual, interpersonal, organizational, community, and policy levels). 32 Understanding the influence of these multilevel factors is essential for developing targeted interventions to reduce disparities. Ecological frameworks have been frequently used in conceptualizing and reviewing evidence on health-related disparities.33-36 Moreover, in 2019, the National Institute on Minority Health and Health Disparities (NIMHD) proposed a comprehensive framework presenting the etiological factors as well as intervention targets to reduce health disparities for populations with health disparities including minoritized racial and ethnic groups. 37 Data extracted from the included studies were synthesized through iterative consensus team meetings. The team used the socioecological and NIMHD framework concepts to synthesize the empirical evidence on disparities in access to, utilization, and quality of EOL and palliative care. These concepts also identified gaps in the evidence and priorities for future research, practice, and policy interventions to address the disparities and improve the EOL care quality for AIAN populations with cancer.
Results
Study Characteristics
Figure 1 shows the PRISMA diagram for study inclusion. After removing duplicates, 1693 unique records were identified. Of these, 153 articles were selected for full-text review, and 22 met the inclusion criteria for final analysis.38-59 The included studies were published from 2014 to 2025, with the vast majority (20/22) published since 2021. Reported AIAN sample sizes varied substantially from 4
38
to 14,359.
54
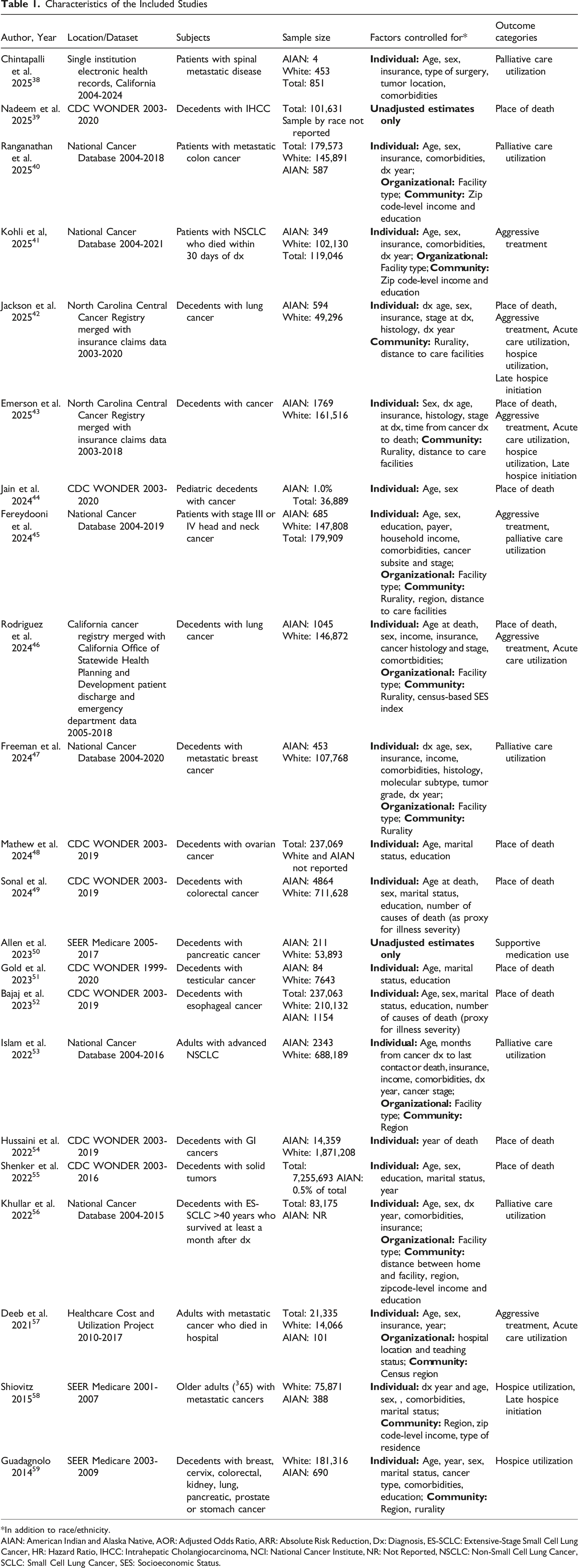
Only two studies focused specifically on disparities in AIAN populations,42,43 whereas the remaining studies reported AIAN estimates alongside those for other racial groups. Table 1 lists the studies included and their characteristics. Study identification and inclusion diagram Characteristics of the Included Studies *In addition to race/ethnicity. AIAN: American Indian and Alaska Native, AOR: Adjusted Odds Ratio, ARR: Absolute Risk Reduction, Dx: Diagnosis, ES-SCLC: Extensive-Stage Small Cell Lung Cancer, HR: Hazard Ratio, IHCC: Intrahepatic Cholangiocarcinoma, NCI: National Cancer Institute, NR: Not Reported, NSCLC: Non-Small Cell Lung Cancer, SCLC: Small Cell Lung Cancer, SES: Socioeconomic Status.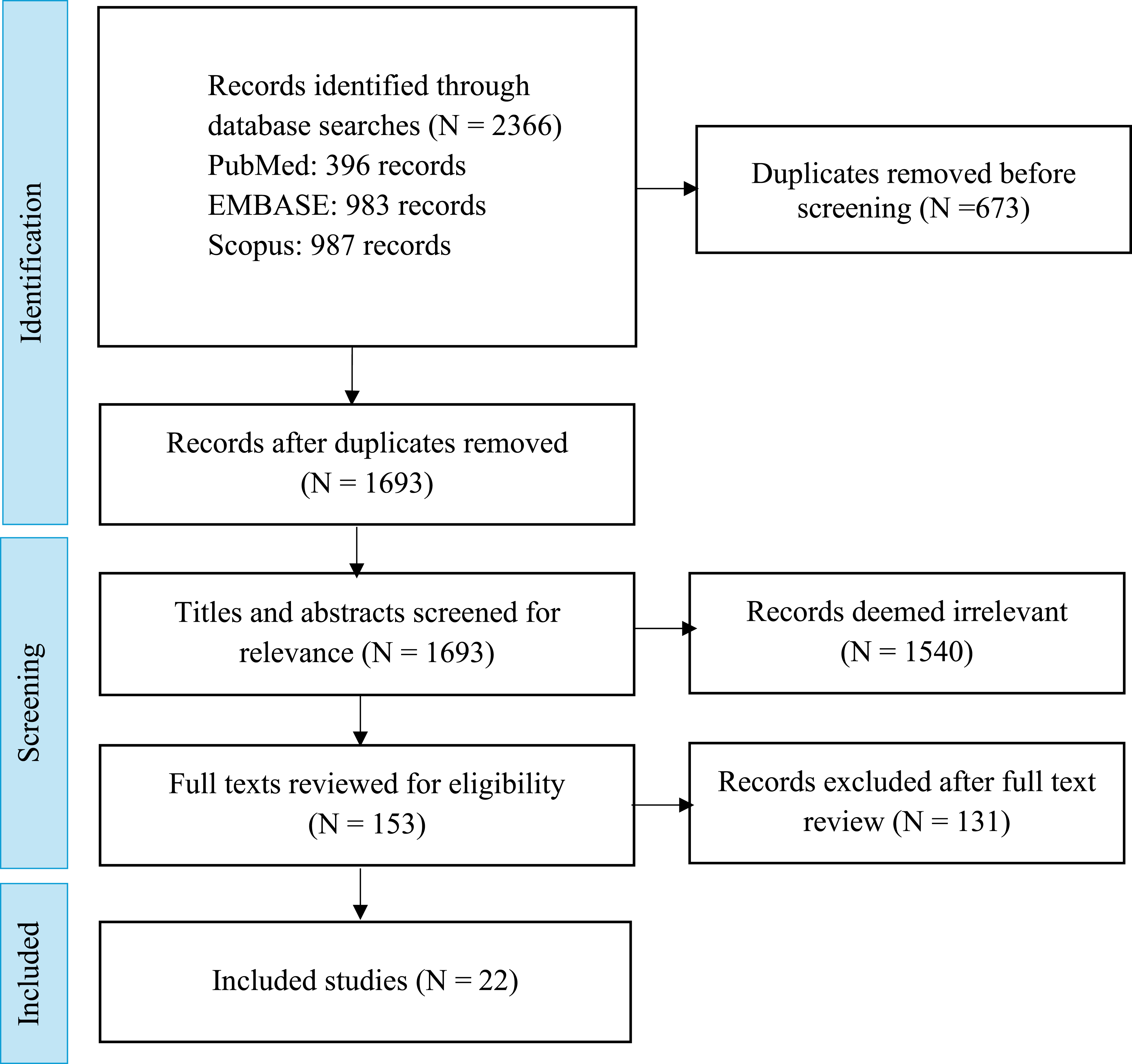
Summary of Evidence on AIAN/White Disparities Across End-Of-Life Care Outcome Categories
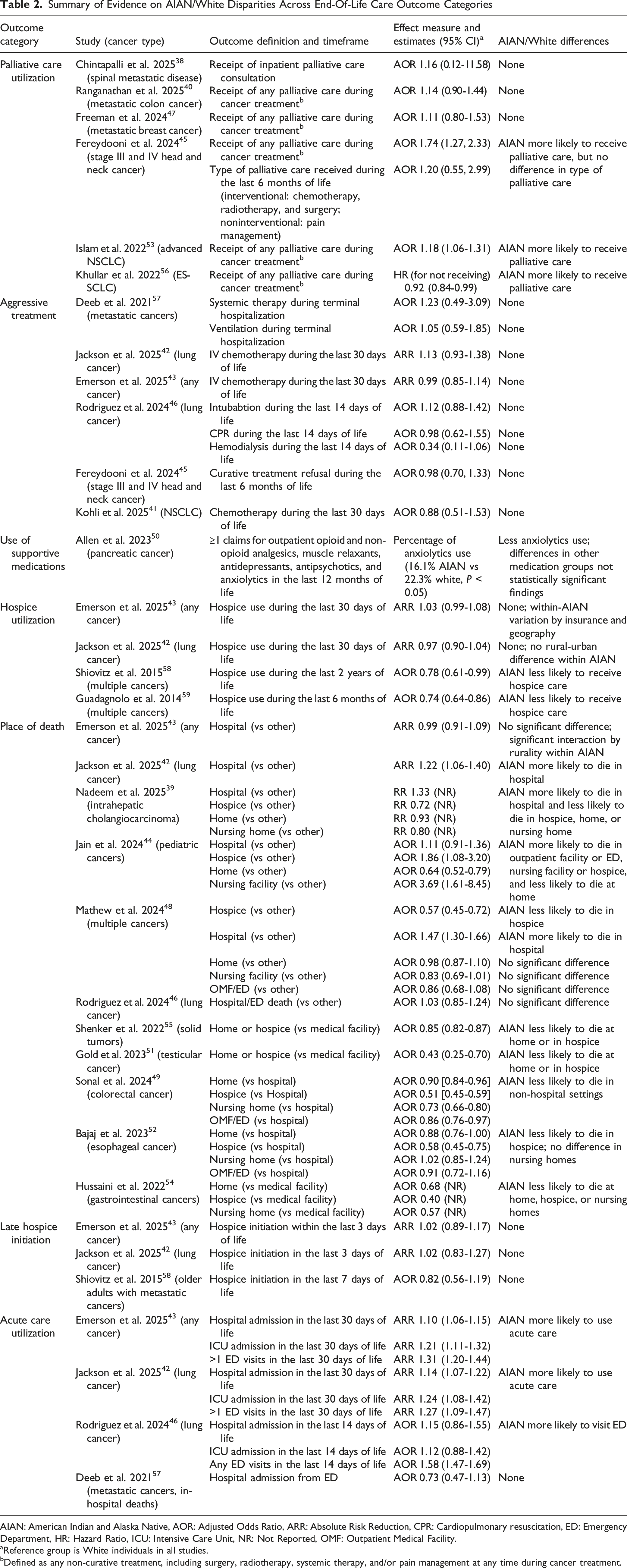
AIAN: American Indian and Alaska Native, AOR: Adjusted Odds Ratio, ARR: Absolute Risk Reduction, CPR: Cardiopulmonary resuscitation, ED: Emergency Department, HR: Hazard Ratio, ICU: Intensive Care Unit, NR: Not Reported, OMF: Outpatient Medical Facility.
aReference group is White individuals in all studies.
bDefined as any non-curative treatment, including surgery, radiotherapy, systemic therapy, and/or pain management at any time during cancer treatment.
Disparities in EOL Care Outcomes
As summarized in Table 1 and Figure 2, the most frequently examined outcomes were place of death (n = 11),39,42-44,46,48,49,51,52,54,55 followed by palliative care utilization (n = 6),38,40,45,47,53,56 aggressive treatment near the end of life (n = 6),41-43,45,46,57 hospice utilization (n = 4),42,43,58,59 acute care utilization including emergency department (ED), inpatient or intensive care unit (ICU) admissions (n = 4),42,43,46,57 late hospice initiation (n = 3),42,43,58 and supportive medication use (n = 1).
50
Distribution of studies by outcome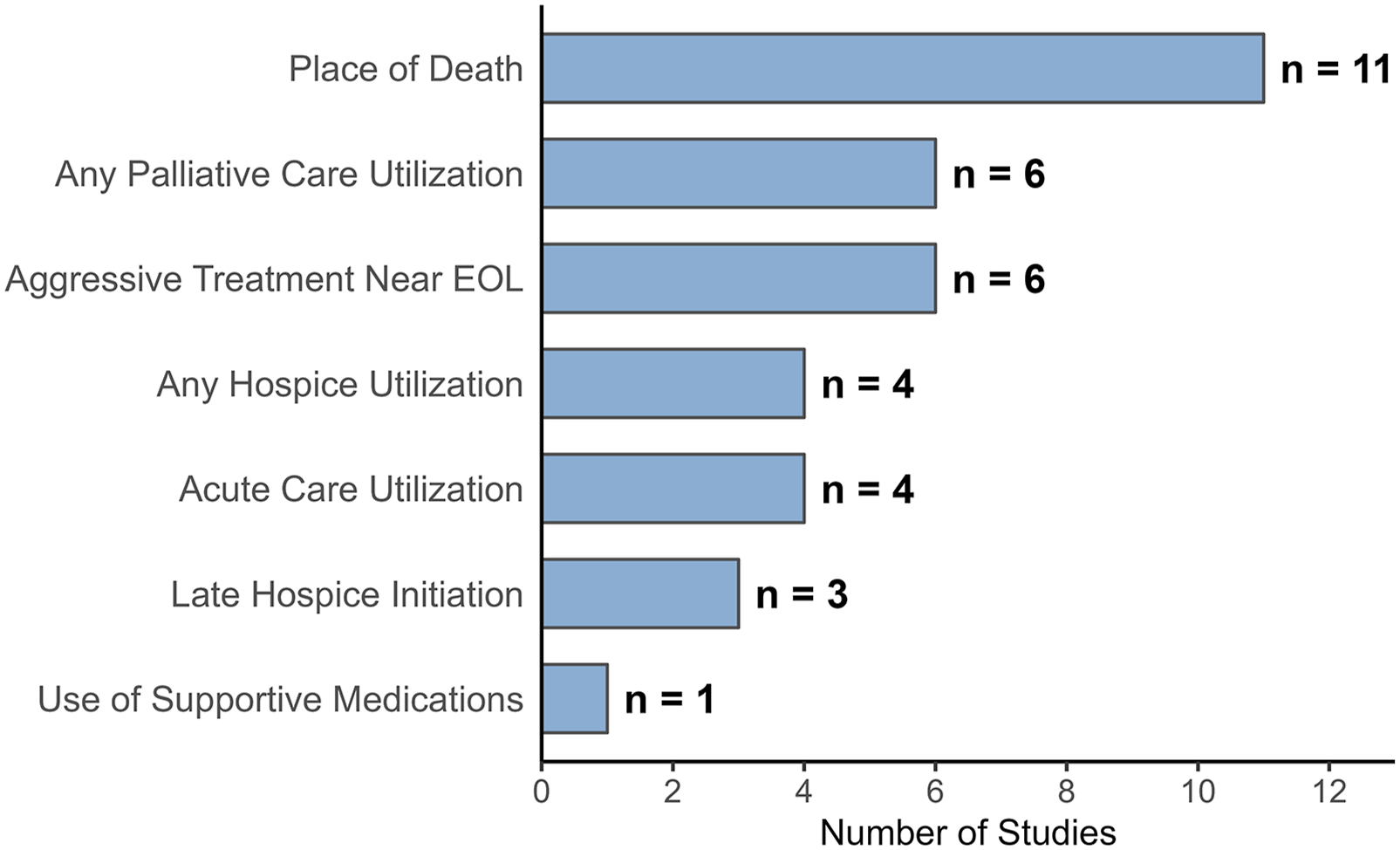
Place of Death
Most studies (9 out of 11) examining place of death among AIAN decedents with cancer reported statistically significant disparities compared to White counterparts. While operational definitions of the outcomes varied (as listed in Table 2), their findings consistently indicated lower likelihood of AIAN individuals with cancer dying in home or hospice facilities, and higher likelihood of hospital or other medical facility deaths. It remains unclear whether home deaths occurred with in-home care, likely reflecting patient preferences and comfort, or represented unmet palliative care needs in settings where such services are less available.
Despite being a key determinant of access to healthcare for the AIAN peoples, only two studies examined the intersection of rurality with AIAN race and their effect on place of death: (i) Emerson et al (2025) 43 found no significant difference in the likelihood of in-hospital death between AIAN and White decedents with cancers in North Carolina. However, this null finding masked heterogeneities by rurality. Specifically, rural AIAN decedents had a lower likelihood of in-hospital death compared with rural White decedents, whereas urban AIAN decedents had a higher likelihood of in-hospital death relative to their urban White counterparts. (ii) Jackson et al (2025) 42 examined in-hospital deaths among decedents with lung cancer and identified significant disparities between rural AIAN and their rural White counterparts, whereas no significant difference was observed in the urban populations.
Palliative Care Utilization
Six studies evaluated disparities in palliative care utilization, defined as the receipt of any non-curative treatment for cancer. As summarized in Table 2, three45,53,56 reported a higher likelihood of receiving palliative care among AIAN individuals compared to their White counterparts. Fereyodooni et al (2024) 45 attributed this finding to cultural acceptance of death as a natural life transition among AIAN communities. Additionally, the definition of any palliative care includes symptom management and supportive care, as well as non-curative surgery, radiotherapy, or systemic chemotherapy. This is an important distinction, especially in the context of advanced cancer where treatment intent is non-curative. Palliative care utilization defined as any non-curative treatment may not properly reflect early access to comprehensive and culturally-responsive palliative care services. Fereyodooni et al (2024) 45 were the only study that further disaggregated palliative care utilization into interventional (surgery, radiotherapy, systemic therapy) vs non-interventional (symptom management) within 6 months of death, and observed no differences between AIAN and White counterparts.
Hospice Utilization
Four studies assessed hospice use outcomes and reported mixed findings. Two recent studies from North Carolina, Emerson et al (2025) 43 and Jackson et al (2025) 42 reported no statistically significant difference in hospice use during the last 6 months of life between AIAN and White decedents. In contrast, two earlier studies using national SEER-Medicare data, Shiovitz et al (2015) 58 – looking at the last 2 years of life – and Guadagnolo et al (2014) 59 – looking at the last 6 months of life – found significantly less hospice use in AIAN decedents with cancer compared to their White counterparts.
Exploring potential heterogeneities within the AIAN population in North Carolina, Jackson et al (2025) 42 reported no significant difference between urban and rural AIAN decedents with lung cancer, while the larger study by Emerson et al (2025) 43 found substantial heterogeneity within the AIAN decedents with all cancers, namely higher hospice use among Medicare beneficiaries and those residing farther from major medical centers.
Aggressive Treatment Near the End of Life
Six studies evaluated disparities in the use of intensive medical interventions during the final stages of life, and none found significant disparities between AIAN individuals with cancers and their White counterparts. As shown in Table 2, how aggressive care is operationalized and the timeframes examined varied widely across studies. Although receipt of aggressive care near EOL is often associated with poorer patient and caregiver outcomes,60-63 population-based studies using large databases are unable to determine whether patients opted for such intensive care. 64 Moreover, some forms of treatment commonly classified within aggressive care definitions, such as chemotherapy, could have been delivered with palliative intent. Future studies should examine how best to define and measure inappropriate and value-discordant aggressive care near the EOL period that more accurately reflect unmet supportive or palliative care needs, and assess whether, for the AIAN individuals, early integration of culturally-responsive palliative care services may reduce such care.
Acute Care Utilization
Three of four studies evaluating acute care utilization near the EOL period reported significantly higher use in AIAN individuals with cancer compared to their White counterparts. Emerson et al (2025) 43 and Jackson et al (2025) 42 reported higher risks of hospitalization, intensive care unit (ICU) admission, and >1 emergency department (ED) visits in the last 30 days of life, and Rodriguez et al (2024) 46 identified more ED visits during the last 14 days of life among AIAN individuals with cancer compared to their White counterparts. Deeb et al (2021) 57 found no statistically significant difference in the likelihood of being admitted to the hospital from the ED among terminally hospitalized individuals with metastatic cancers.
Late Hospice Initiation
Three studies examined disparities in late hospice initiation. Whether defined as initiation within the last 342,43 or 7 58 days of life, no significant disparities were found for AIAN individuals with cancer compared to their White counterparts.
Use of Supportive Medications
Allen et al (2023) 50 reported fewer anxiolytic medications use in AIAN vs White individuals with pancreatic cancer. There were no significant differences for other supportive medications (opioid and non-opioid analgesics, muscle relaxants, antidepressants, and antipsychotics). In addition to the small AIAN sample size (N = 211 vs 53 893 White), these findings were based on unadjusted analyses without controlling for confounders.
Key Evidence Gaps
Despite growing number of studies in the recent years, our review revealed several important gaps in the existing evidence base on EOL care outcomes for AIAN populations: 1. 2. 3. 4. 5. 6.
Discussion
This scoping review aimed to synthesize the literature on disparities in EOL care for AIAN individuals with cancer, as well as gaps in evidence, research priorities, and actionable practice and policy recommendations. We identified 22 studies examining EOL care disparities affecting AIAN individuals with cancer. Studies reported disparities in places of death (9/11 studies) – with AIANs less likely to die in home or hospice and more likely to die in medical facilities compared to their White counterparts. Disparities were also reported in hospice use (2 of 4 studies reporting lower utilization among AIANs), acute care services including hospitalizations, ICU care, or frequent ED visits (3 of 4 studies reporting higher acute care use among AIANs), and supportive medication use (1 of 1 studies reporting lower use among AIANs). Significant differences were reported after accounting for clinical and sociodemographic factors, healthcare setting, community-level socioeconomic status, and rurality, highlighting inequitable EOL care experiences for AIAN individuals with cancer and their families.
AIAN peoples are remarkably diverse, with hundreds of federal, state, and unrecognized tribes, each with distinct cultural identities, geographic contexts, healthcare access, and lived experiences. Over the past centuries, AIAN communities have often experienced greater suffering from modern society’s afflictions, whether it was COVID, smallpox, tuberculosis, or alcoholism. 65 Persistent disparities exist today across the cancer care continuum, reflecting the compounded impact of historical marginalization, structural racism, socioeconomic disadvantages, and geographic isolation. These structural forces continue to shape access to timely and patient-centered care for AIAN individuals with cancer, including access to high-quality EOL care. Access to hospice and palliative care services at Indian Health Service (IHS) or Urban Indian Health Programs (UIHP) remains limited and most such care is accessed outside through Purchased/Referred Care (PRC). 28 Strengthening capacity for providing EOL and palliative care by IHS and UIHP facilities should be a priority. Strategies such as provider training programs, collaborating with local hospice agencies, leveraging telehealth services to better support rural residents, as well as enhancing PRC coverage and navigation for hospice and palliative care should be explored. Tribal health organizations should be supported in developing and sustaining palliative care and hospice programs that are tailored to local Indigenous cultures and practices. Examples of such programs have been successfully operating for the past decades. 66 Moreover, AIAN individuals from tribes without federal recognition must often rely on external health systems. Partnering with indigenous communities and integrating their voices and knowledge systems into the design and evaluation of EOL and palliative care programs not only ensure that these services align with their values but also shapes our knowledge base on cultural safety of such services for diverse populations.
In addition to access disparities, issues about culturally responsive EOL care for AIAN communities have been raised repeatedly in the past decades. 66 Patient-clinician cultural communication barriers may contribute to EOL outcome disparities. For example, the literature often notes a common assumption among healthcare providers that AIAN cultures universally view discussions about death as taboo, 67 which can hinder proper EOL care planning. This taboo exists for only a few tribal nations. Notably, none of the studies in our review examined disparities in goals of care conversations or advance directive completion. Addressing cultural barriers in communication is an essential, intervenable target for improving EOL care experiences and reducing outcomes disparities for minoritized groups, including AIAN patients. Strategies may include increasing AIAN representation within the palliative care workforce to foster trust and cultural alignment in care delivery.68,69 Strengthening patient navigation services through the integration of community health workers who are more accessible as well as familiar with local values and traditions may help bridge the gap in access to culturally responsive care. 70 More broadly, in the face of diversity, practicing compassionate presence and cultural humility by clinicians can enhance patient-clinician communication regardless of race or other characteristics.71,72 Efforts at promoting approaches rooted in cultural humility frameworks for palliative care are critical not only for AIAN communities but for ensuring person-centered care for all individuals facing serious illness.72,73
It is important to recognize that current EOL-related outcomes have limitations in their ability to capture what matters most to the dying person and their loved ones. 74 For instance, it is uncertain to what extent evidence of aggressive care near the EOL, as captured from administrative data, reflects the circumstances in which care was delivered and whether it was concordant with the values of patients and their families. Future studies may consider pairing these measures with evidence of early hospice enrollment or advance care planning to assess whether discussions around EOL care decisions occurred. Moreover, despite home being regarded as the preferred place of death for the majority of Americans, 75 it is hard to generalize this to all AIANs given the geographical and cultural diversity and concerns for forgoing care in the context of historical mistrusts. In addition, the universality of preference for in-home death has been questioned for patients with burdensome EOL needs. 64 This issue is more pronounced for specific cancer populations. For instance, severe pain in patients with bone cancers and agitated delirium in patients with brain cancer are not unlikely during the days or weeks before death. In such cases, intermittent home hospice visits may not be ideal for symptom management, and inpatient hospice or skilled nursing facilities may be able to offer more comfort to the patient and their families. Recent efforts at developing more standardized, person-centered core outcome sets for EOL care have emphasized recognition and discussion about dying, continued access to care, and addressing symptoms such as pain and anxiety, among outcomes that matter the most to patients and families. 76 Such studies with a focus on or contribution from AIAN communities are needed.
To address the existing gaps in evidence, future studies on EOL care disparities should prioritize transparency in model specification and reporting, as the interpretation of race coefficients in multivariable models depends on covariates included, 77 and adjusting for mediator variables in addition to confounders can lead to overadjustment and obscuring disparities. 78 Examining mediating pathways between AIAN race and EOL outcomes would be helpful to move the field from documenting disparities toward identifying targeted interventions. Potential pathways include socioeconomic factors, geographic location, health literacy, cultural and religious values, communication barriers, and trust in the healthcare systems. For instance, many AIANs live in rural areas, and rural residents, regardless of race, have more limited access to EOL services. 79 Future research may clarify whether there is an interaction between rurality and AIAN race, for instance due to stronger cultural practices in rural areas. To better unmask within-AIAN heterogeneities, community-specific research is essential and data collection strategies such as oversampling in nationwide surveys are critical to ensure adequate representation to enable research and monitoring progress on eliminating disparities for this vulnerable population. 80
Truly comprehensive cancer care must address the complex physical, emotional, spiritual, and social needs of individuals, including the universal human need for compassion, connection, and care during difficult life transitions. As such, supporting patients and their loved ones during the EOL period is a core tenet of high-quality cancer care. 81 Behind the statistics on EOL care disparities are persons with cancer and their loved ones who face avoidable pain and suffering, financial distress, and heavy caregiving demands. 28 Providing high quality EOL care – one that prioritizes comfort and quality of life, is patient- and family-centered, and eliminates the observed disparities – requires multilevel action across policy, health system, and community levels. 82
Limitations
Findings must be interpreted considering several limitations: The terms palliative care, EOL care, and hospice were used interchangeably up until about a decade ago. Although our search strategy included all three terms, some studies may have been missed due to the inconsistent usage of these terms in the literature. AIAN is frequently lumped with the “other” race category due to small sample sizes. Even a systematic review of hospice use in minoritized populations excluded AIAN findings. 83 Lastly, disparities research is inherently population based, and we cannot say if population-based outcomes represent the patient and family preferences for all individuals.
Conclusion
This scoping review highlights persistent disparities in EOL and palliative care among AIAN individuals with cancer in the US. AIAN populations remain underrepresented in research including research evaluating health disparities. Across included studies, our findings point to a more medicalized EOL experience for AIAN individuals with cancer compared to their White counterparts, indicated by higher rates of acute care use and death occurring in medical facilities such as hospital or emergency departments rather than in home or hospice facilities. Expanding access to hospice and palliative care services and promoting culturally safe, community-driven research and practice in EOL and palliative care is essential to move beyond documenting disparities to targeting their underlying mechanisms for AIAN communities.
Supplemental Material
Supplemental Material - End-of-Life and Palliative Care Disparities Among American Indians and Alaska Natives with Cancer: A Scoping Review
Supplemental Material for End-of-Life and Palliative Care Disparities Among American Indians and Alaska Natives with Cancer: A Scoping Review by Soroush Fariman, Joel Begay, Linda Burhansstipanov, Marc A. Emerson, Stephanie B. Wheeler, Jennifer Elston Lafata, Ronny A. Bell in American Journal of Hospice and Palliative Medicine®
Footnotes
Acknowledgments
The authors wish to thank Rebecca B Carlson, Health Sciences Librarian at the University of North Carolina at Chapel Hill, for her guidance on the methodology. We also thank Katie E Johnson and Ana I Salas with the Community Outreach and Engagement Program at the Lineberger Comprehensive Cancer Center for their assistance with research coordination. This work was presented in part as a poster at the American Society for Preventive Oncology (ASPO) 49th Annual Meeting, Philadelphia, Pennsylvania, April 6 –8, 2025.
Ethical Considerations
This study did not involve human participants and therefore did not require ethical approval or informed consent. All data were obtained from published sources.
Author Contributions
Conceptualization: SF, RAB; Data Curation: SF, JB, RAB; Formal Analysis: SF, JB, LB, MAE, JEL, SBW, RAB; Methodology: SF, JB, RAB; Project Administration: SF; Supervision: MAE, SBW, RAB; Writing – Original Draft Preparation: SF; Writing – Review & Editing: SF, JB, LB, MAE, JEL, SBW, RAB; All authors reviewed and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Southeastern American Indian Cancer Equity Partnership (SAICEP), the V Foundation for Cancer Research, the University Cancer Research Fund, and the National Cancer Institute (NCI) Center Core Support Grant (5-P30-CA016086) to support the UNC Lineberger Comprehensive Cancer Center.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.