
Abstract
Keywords
Introduction
Intensive care unit (ICU) admissions can be turbulent times for patient’s family members. Psychological problems such as anxiety, depression, and post-ICU stress are commonly noted in them during ICU and post-ICU periods.1-3 Family members have an enhanced responsibility as health promoters through compassion towards critically ill dear ones and as fair decision-makers as patients advance from a breakpoint between life and death to a breakthrough towards life. 4 Bystander surrogate decision-making for patients is dependent on various factors such as educational status, sociocultural makeup, i.e., family structure, cultural belief, distress coping mechanisms, and economic concerns like financial assistance for healthcare expenditure.5-7 These factors vary substantially in the Indian ICU scenarios as compared to Western countries. 5 There is limited information in the Indian ICU settings evaluating different aspects of shared decision-making and its impact on family ICU satisfaction.8,9 Understanding the seriousness of a patient’s disease and shared decision-making by the treating physician will help in greater satisfaction and sensible presumptions about the patient’s outcomes.10,11 The family-centered approach has been regarded as one of the key performance indicators across Indian and Western ICU setups. 12 The primary objective of the survey was to explore different variables of decision making in FS-ICU 24R questionnaire enabling shared decision making and family satisfaction. The study aimed to ascertain the most critical components of the shared decision-making process affecting the family members’ satisfaction with intensive care services in our setting.
Materials and Methods
Study Design and Setting
We conducted the questionnaire-based prospective observational study in a multidisciplinary ICU of a tertiary care medical college hospital spanning 13 months (May 2022 to June 2023). The hospital is located in a town with an urban infrastructure catering to healthcare needs of people from three to four neighboring districts.
After obtaining written informed consent, 336 ICU patients’ families (one family bystander of each patient) were interviewed using the Family Satisfaction in the Intensive Care Unit 24 Revised (FS-ICU 24R) questionnaire. Study investigators had received ethical clearance from the institution (IEC 27/2022), and the study was registered with the Clinical Trial Registry - India (CTRI/2022/09/045571). This study was the analysis of the decision-making subscale obtained from FS-ICU 24R-based prospective observational study for families of ICU patients. 10
Participants
We recruited family bystanders of patients admitted to the ICU for more than 72 hours. A family member aged less than 18 years was considered an exclusion criterion. We used convenience sampling for data collection.
Tool
The FS-ICU 24R questionnaire 13 is a widely used patient-reported tool that significantly correlates with family satisfaction with ICU care. Study investigators had procured permission from FS – ICU 24R tool developers to use it in the study. The FS- ICU 24 R (revised version) questionnaire had 24 questions about families’ satisfaction with patient care and decision-making involvement subscales. It was available in English and the local vernacular language spoken at the study center. The questionnaire had ratings from one to five (one – very dissatisfied to five – completely satisfied) based on views best reflected by family bystanders. The questionnaire was valid and reliable to be used in the present study.
Study investigators surveyed the patients’ families on the day of their discharge from the intensive care unit to have a reasonable statement of the families' perspective of patient’s care in ICU and Involvement in shared decision-making. We surveyed the patient’s immediate kin whose near one had died in ICU due to ailment/palliation, with the same questionnaire via telephone after two months of death. The conceptual design of the study is depicted in Figure 1 for understanding of study methodology. Conceptual design for understanding the research methodology.
FS-ICU 24R questionnaire has been included in the Supplemental Material section.
Procedure
The study site had 30 beds receiving critically ill patients from medical and surgical broad/super specialties. ICU was managed on a semi-closed operative basis, with every decision on patient management being done during multidisciplinary rounds in the morning. The ICU team comprised qualified intensivists with more than five years of clinical experience and certified degrees from the National Medical Commission/ Diplomate in National Board. Intensivists were trained in core concepts of ethics and communication, which helped in goals of care discussion in day-to-day practice.
Structured care plans for ICU patients were followed with multidisciplinary counseling (Admitting unit and intensivists, including post-graduates/registrars) with the immediate kin of patients. Counseling was done in an isolated dedicated counseling room in the ICU complex. The counseling room was a spacious, well-ventilated space with adequate lighting and sitting arrangements and had 24 hour closed-camera audiovisual recordings of the counseling activities. The criticality of patients, available treatment options, and anticipated course of illness were discussed with the patient’s kin and recorded in the patient’s case files countersigned by both stakeholders. Counseling was not a one-time activity and continued during family visitation hours twice daily and on a per-need basis. Treatment decision-making also required multiple counseling sittings between the stakeholders where the treating unit assessed the family’s understanding of the patient’s disease. Perception assessment helped treating physicians provide the knowledge and treatment information in the family’s understandable language and in an empathetic manner. The study center had a dedicated end-of-life care unit under palliative and supportive care department with qualified palliative care physicians, allied healthcare professionals such as palliative care nursing staff, physiotherapists and nutritionists. The end- of-life care unit in the intensive care complex consisted of isolated rooms with provisions for immediate kin of the critically ill patients to be there by their side in the times of ordeal. The treating multidisciplinary team would consult palliative care team for difficult advanced goals of care discussion, end-of-life affairs, and grief addressal. Feedbacks were sourced from a) Suggestions during multidisciplinary family counseling regarding shortcomings in healthcare delivery in the intensive care unit as perceived by the family. b) Suggestions from feedback form provided to the family at the time of ICU discharge. The study site had the provision of suggestion boxes near the vicinity of ICU complex for the purpose of depositing the feedback forms. The feedback forms were then accessed by the concerned health-care professions for improvement in quality.
Statistical Data Analysis
The data analysis was done using Statistical Software for the Social Sciences (SPSS) version 29.0 (IBM SPSS Statistics for Windows version 6.0 Armonk, NY: IBM). The demographic factors were expressed as frequencies and percentages. The continuous variables were analyzed using mean +_ standard deviation (SD) or median and interquartile range (IQR) based on parametric/ non-parametric distribution, respectively. The Independent Student t-test was used to compare the means between the two groups for the variables with a parametric distribution, and the Mann-Whitney U test was used to compare the medians between the two groups with the variables with a non-parametric distribution. The Chi-square test was used to determine the association between categorical variables. A P-value ≤0.05 was considered significant.
The univariate analysis of each variable to predict satisfaction among family members was performed to determine the independent predictors of family satisfaction. In the univariate analysis, the variables with P-value <0.2 were selected to ensure as many variables to be taken for the multivariable regression analysis. After the multivariable logistic regression, adjusted Odd’s ratio and 95% confidence interval (95%CI) were calculated, and a P-value ≤0.05 was considered significant. Bootstrap multivariable logistic regression analysis was performed using the bias-corrected accelerated method for 5000 samples, and a P-value <0.05 was considered significant.
Results
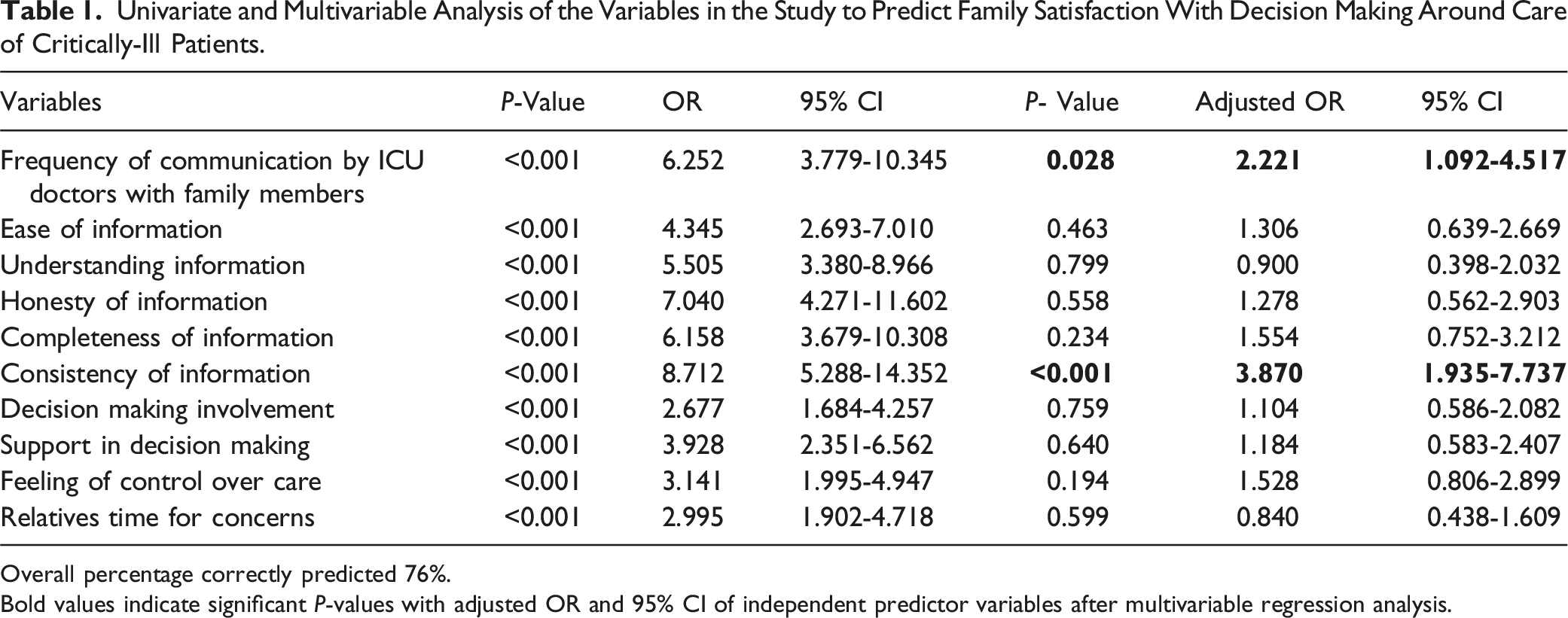
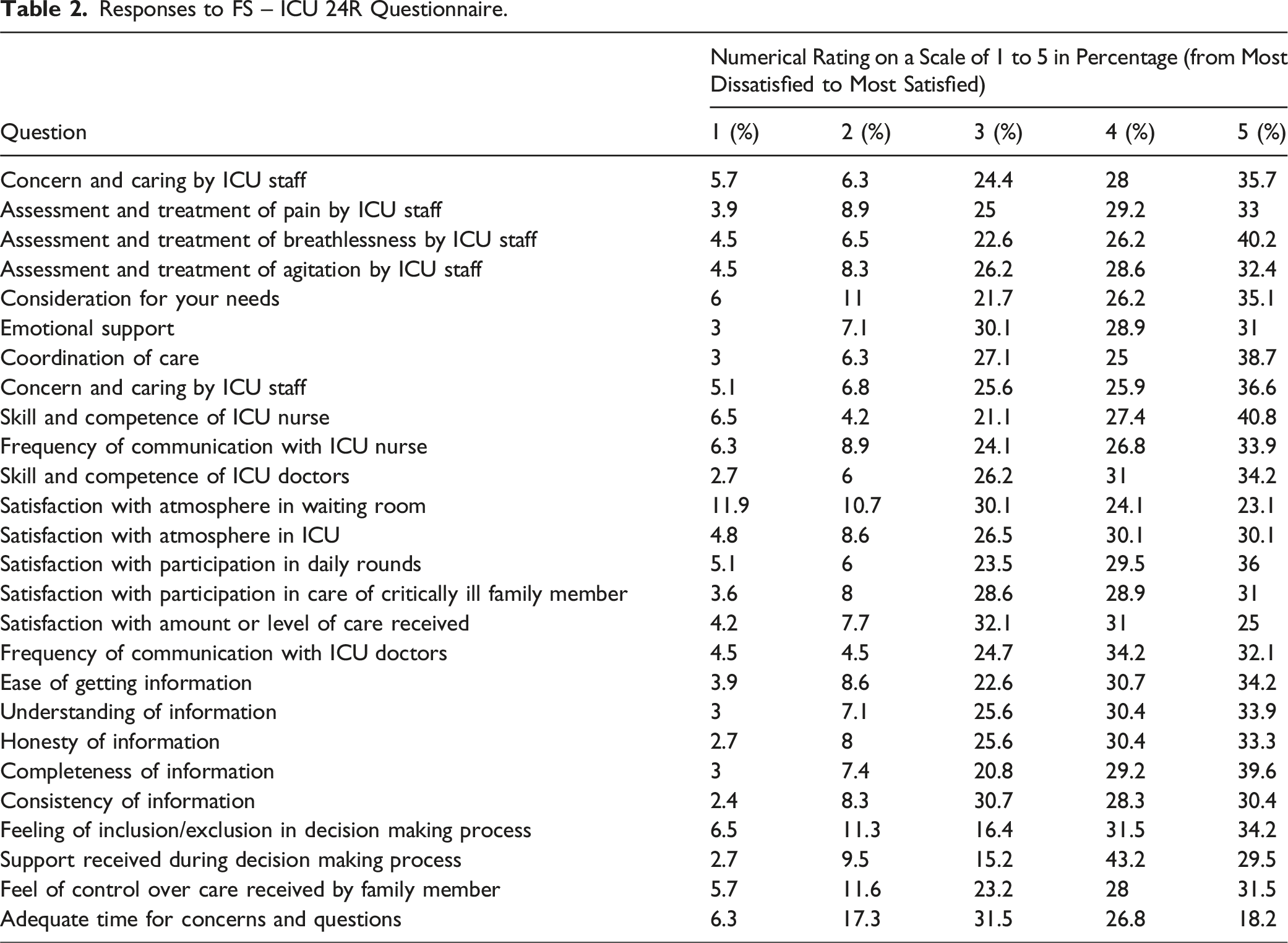
There were 2138 admissions to intensive care units at the survey sites during the study period. Out of these, 336 family bystanders were surveyed on a convenient sampling basis. Other details of the study methodology and patient recruitment are depicted in Figure 2. This study evaluated ten factors of the FS-ICU 24 R questionnaire predicting family satisfaction with decision-making around the care of critically ill patients (Table 1). Responses to 10 decision-making subscale variables of the questionnaire were analyzed (Table 2). (Figure 3). Depicting methodology and patient recruitment for the study. Univariate and Multivariable Analysis of the Variables in the Study to Predict Family Satisfaction With Decision Making Around Care of Critically-Ill Patients. Overall percentage correctly predicted 76%. Bold values indicate significant P-values with adjusted OR and 95% CI of independent predictor variables after multivariable regression analysis. Responses to FS – ICU 24R Questionnaire. Implications of study.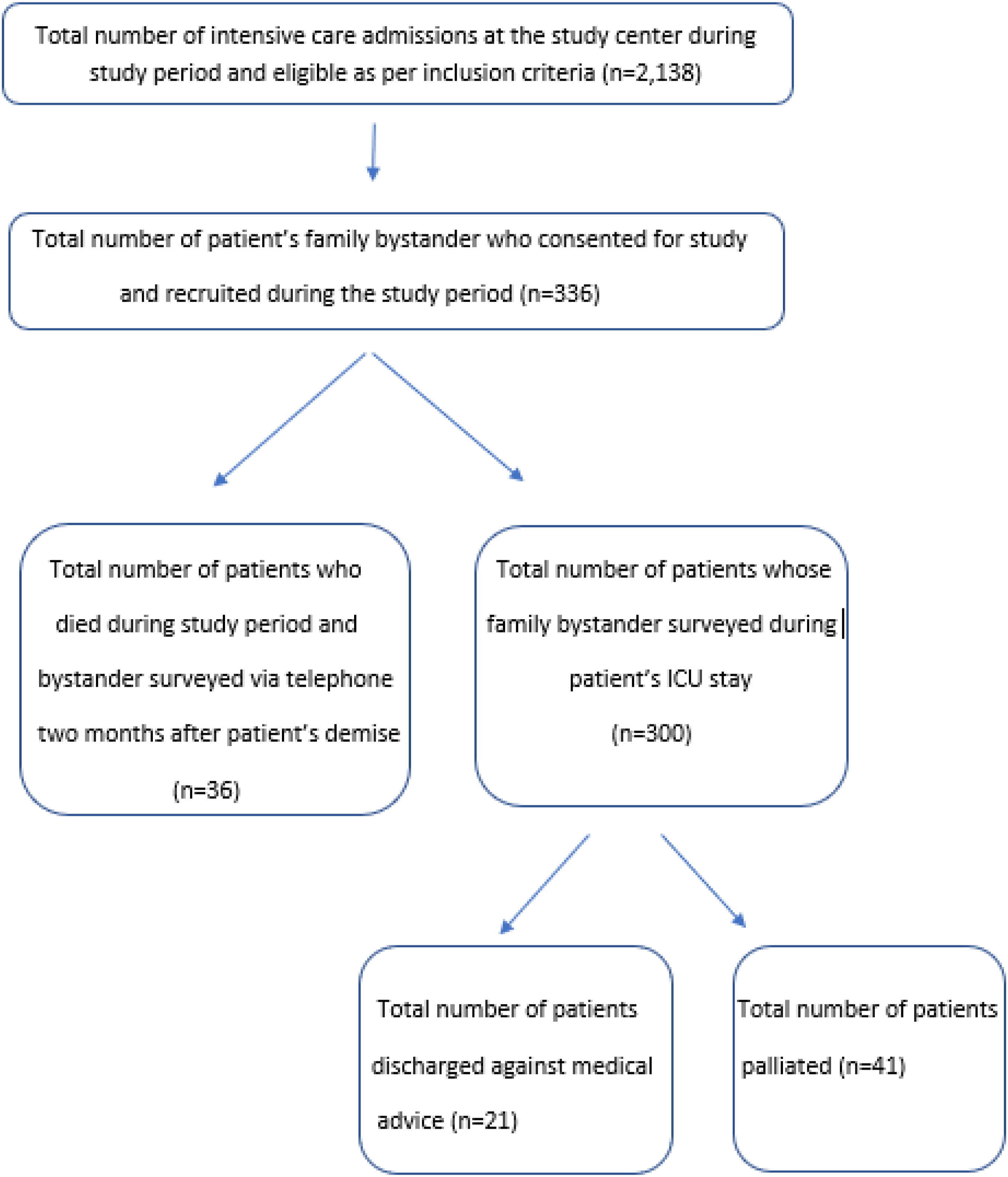
Sample Characteristics
Out of 336 family bystanders surveyed, 215 (64%) were males, and 121 (36%) were females. 72.3% of respondents were the patient’s immediate kin (parents, spouse, children).70.8% of respondents were staying with the patient. 51.9% of bystanders had studied till pre-university. The mean age of patients was 56.5 (SD 16.2) years, the median (IQR) of the SOFA score was 8 (6-11), the Charlson comorbidity index score was 2 (1- 4.75), the length of ICU stay was 6 (4-10) days, and length of hospital stay was 16 (11-26) days. The basic demographics of the study participants are detailed in Table 1 (Supplementary Appendix).
For setting standards of care in the ICU, the relatives who had opted only as either very satisfied or completely satisfied were categorized as finally satisfied with care. Relatives who had opted for either very dissatisfied, slightly dissatisfied, or mostly satisfied were categorized as not completely satisfied with the care provided. The Chi-square tests for the ten categorical variables showed that each variable was significant in predicting relatives’ satisfaction with care.
Group Differences and Associations
Frequency of Communication With ICU Doctors and Amount of Satisfaction to Care.
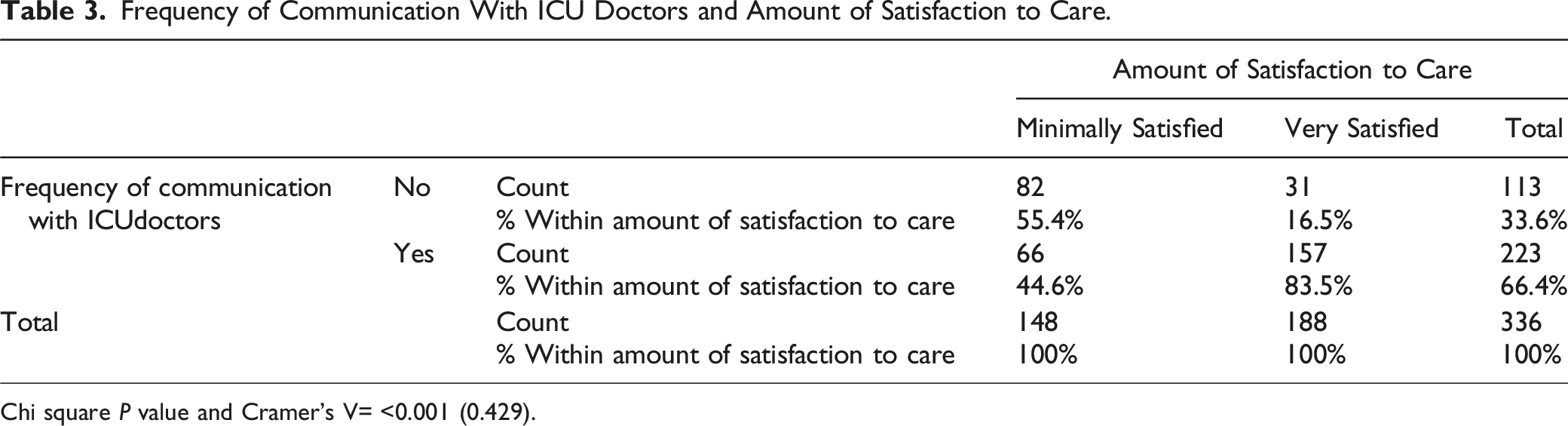
Chi square P value and Cramer’s V= <0.001 (0.429).
Consistency of Information and Amount of Satisfaction to Care.
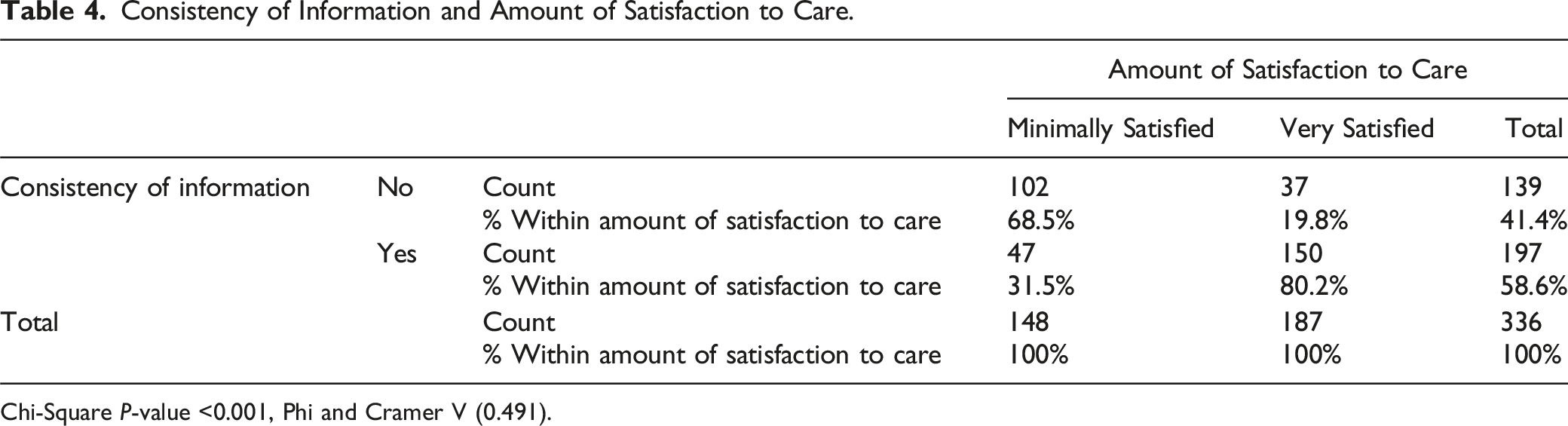
Chi-Square P-value <0.001, Phi and Cramer V (0.491).
Likewise, when the time for concern was adequately met, 56.9% of relatives expressed satisfaction, compared to 43.1% if there was inadequate time for concern (Chi-Square P-value <0.001). Similarly, the feeling of control over decision-making (Chi-Square P-value <0.001), support in decision-making (Chi-Square P-value <0.001), Involvement in decision-making (Chi-Square P-value <0.001), and completeness of information (Chi-Square P-value <0.001) were all associated with relatives’ satisfaction of care (Supplementary appendix Tables S5 -S9).
The univariate analysis showed that all ten variables in the FS-ICU 24R questionnaire significantly predicted patient relative satisfaction (P < 0.001). The multivariable regression analysis showed that the independent variables, which were predictors of the patient’s relative satisfaction with decision-making around care, were the consistency of information provided to the family (P-value <0.001, adjusted OR 3.856, 95% CI [1.944-7.648] and frequency of communication with doctors (P-value 0.028, adjusted OR 2.221, 95% CI [1.092 – 4.517] (Table 1). The multivariable regression model could correctly predict up to 74% of cases, and the model was a good fit (Hosmer and Lemeshow P-value 0.804, Nagelkerke R Square 0.350).
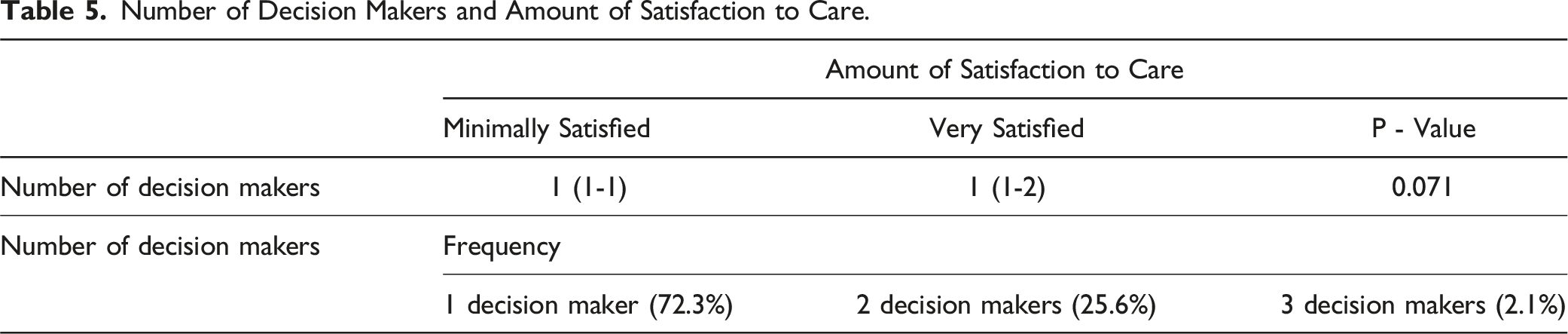
Number of Decision Makers and Amount of Satisfaction to Care.
Relative’s Previous ICU Experience and Amount of Satisfaction to Care.
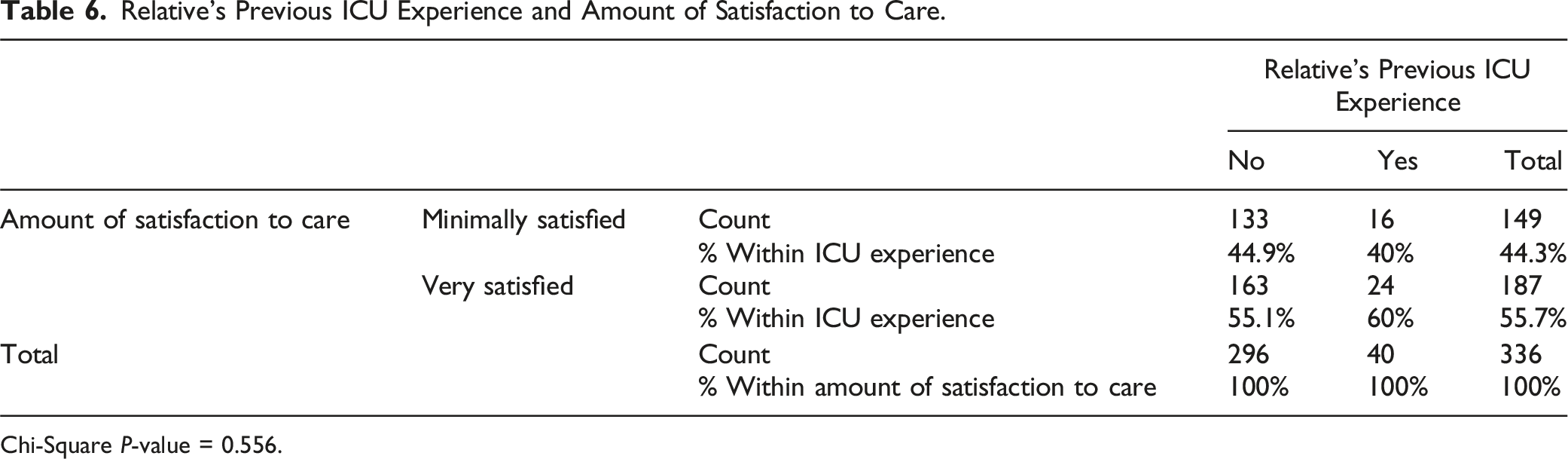
Chi-Square P-value = 0.556.
Discussion
This study found that an intensivist’s clarity on a patient’s clinical outcomes and hand-holding of the patient’s family in the decision-making process is critical to ensuring family satisfaction. This can be guaranteed by (a) meaningful communication with frequent counseling, (b) encouraging shared decision-making, (c) supporting family in difficult decision-making scenarios, and (d) catering to a safe ICU environment and flexible visitation policies as needed. Through the study findings, we could demonstrate that all the ten FS-ICU 24R decision-making subscale variables can be associated with family satisfaction. Univariate logistic regression model of variables demonstrated that components of information divulgement such as honesty, understanding, ease, completeness, consistency, and frequency of information scored a higher odds of family satisfaction as compared to time for relative’s concerns, feeling of control over patient care and family’s Involvement in decision making (Figure 3).
Developing a physician-bystander rapport, reassurance about patient care, and attending to bystander’s information needs are essential for ensuring the family’s ICU satisfaction and the patient’s better outcomes.14-16 These three factors can be established by frequent counseling with family. However, that might only sometimes be possible, especially in the acute phase of a patient’s illness. Firstly, the initial ICU phase is when patients need the physician’s undistracted attention and differential diagnoses being worked out. Less time for family’s needs and inconsistent information regarding diagnosis during the initial ICU phase might lead to mistrust and feelings of not being supported. 17 Complete and consistent information delivered to the family in an understandable language with honesty is required to cater to their needs.
Interestingly, family satisfaction was not associated with the number of bystanders involved in decision-making or their prior ICU experience. Families in India have a greater mean household size than Western countries (4.8 vs 2.6)5. Having relatives as bystanders in a hospital can positively influence decision-making and coping with distress. It can also be counterproductive if their suggestions are unhelpful and upsetting. Multiple studies in the past have demonstrated the negative impact of prior ICU exposure of a patient or bystander on family satisfaction.18,19 Contrasting observations in our study were surprising. The authors could offer some explanation. Irrespective of the family’s prior ICU experience, families had: 1. Easy access to patient information. 2. Decision-making assistance. 3. Surrogate decision-making as required on the part of physicians.
These three factors would have led to better family satisfaction, irrespective of family’s previous ICU experience and the number of family members in the immediate kith/kin to make decisions regarding goals of care.
A few observations from the study were surprising. Though statistically significant, the family’s involvement in decision-making, the physician’s time for relative’s concerns, and the family’s feeling of control over care had low odds of association with satisfaction. A reasonable interpretation of these findings can be as follows. Almost 3/5th (59.2%) of participants were from rural settings, and only 51.9% had completed education till pre-university (equivalent to senior secondary school in the American educational system). The burden of surrogate decision-making could have been entrusted to physicians to make the right decisions for the patient’s betterment. There could have been less physician-bystander interaction in the acute phase of the patient’s illness as the physician devoted more time in evaluating the patient’s bedside.
Almost 38% of patients in the study had more than seven days of ICU stay. Shared decision-making was not just a two-sided concern involving the patient’s immediate kin and treating physicians. The treatment decisions of those patients with more than seven days in the ICU came under the scrutiny of the hospital’s critical care review board. The Critical Care Review Board (CCRB) comprised of qualified physicians from intensive care, patient’s admitting broad and super specialty, palliative care medicine and other aligned specialties involved in patient’s management. The board met weekly to review the patient’s medical aspects, such as clinical trajectory during ICU stay, alternative treatment options, expected time to recovery, and non-medical concerns like familial support for emotional and decision-making needs, financial support for ICU expenses, and other assistance. After ratification of ongoing treatment decisions of the ICU patients, the review board would either suggest (a) appropriate to continue treatment, (b) time targeted trial for 48 hours or (c) need for multidisciplinary goals of care discussion with family considering rationale of ICU treatment. This review drill helped the treating team bring consistent, honest, and complete information to the family for better understanding.
In the present survey, we also tried to explore the impact of decision-making factors on family satisfaction in difficult decision-making scenarios. There were 6.25% of patients discharged against medical advice, 12.2% opting end of life care and 30.4% of patients expired during the study period. With advanced directives regarding treatment yet to gain a foothold in India, surrogate decision-making continues to be a routine practice. The concept of end-of-life care is slowly gaining visibility with clear position statements from Indian Intensive care and palliative care societies.20-22 It was surprising to note that the level of family satisfaction was not associated with patient outcomes like death (P = 0.331), palliation (P = 0.304), or discharge against medical advice (P = 0.570). Though the results cannot be extrapolated due to fewer patients, this can rightly stress the importance of attending to families’ needs, positively impacting despite adverse outcomes. Study investigators would like to mention many strengths of the study. The study was conducted on a large sample size on last day of a patient’s ICU stay. Study investigators felt a survey on the last day of ICU stay would rightly elicit a family’s perspective on ICU care and the magnitude of satisfaction/dissatisfaction towards it—Bootstrap multivariable analysis with 5000 samples of statistically significant independent variables of decision-making. Bootstrapping added value to internal validity for satisfaction prediction and the study’s generalizability. In contrast to previous studies, this survey also noted family satisfaction in palliative care, discharge against medical advice, and difficult decision-making scenarios. Satisfaction scores were analyzed against patients' disease severity scores, ICU survivors and non-survivors, medical conditions from the past, ICU/hospital length of stay, and other deciding factors like family’s monetary concerns and educational status. A critical care review board for difficult decision-making is something that was previously unheard of but is worth emulating.
This survey had its share of drawbacks as well. Investigators used convenience sampling for the survey. This could have led to selection bias and skewed representation of the samples. During the study period, the investigators would do family bystander survey at a specific time of the day. However, there were instances where surveys were missed due to unavailability of family bystanders in the ICU complex, unwillingness of the bystanders to participate in the survey or due to a shorter ICU stay because of mortality or discharge against medical advice. A better sampling methodology would ensure the external validity of the research. The tool had open-ended questions like suggestions to improve the care provided in the ICU? Comments on things we did well? Suggestions to improve the ICU experience for the family? Analysis of these responses will help in further improvisation. The percentage of patients seeking discharge against medical advice (6.25%) and end of life care services (12.2%) was negligible. The study was conducted in a single multidisciplinary ICU setup. India has got diverse socioeconomic, cultural and spiritual background. The study population for survey were reflective of diverse population with different socioeconomic settings. a) About 59.2% of patient bystanders were from rural background (Village, Taluk) as compared to 40.8% from urban background (Town, District) b) Around 48.1% of patient bystanders were well educated with undergraduate and postgraduate degrees as compared to 51.9% who had studied until pre-university degree. c) About 32.4% of patient’s bystander had out of pocket expenditure (OOPE) to meet healthcare costs, another 32.4% had prior health insurance from private health insurance providers while 35.1% relied on government health schemes to meet healthcare expenditure.
Despite this, the study results are not generalizable as this was a single center study. The decision-making variables and its impact on family satisfaction can be different if done in a metropolitan population with varied educational, socioeconomic and cultural status. Further research to analyze decision-making difficulties and family satisfaction in these subsets of patients is worth doing.
Conclusion
In conclusion, this study suggests that consistency of information regarding a patient’s clinical condition provided to families is the most critical component of the shared decision-making process, which drives family satisfaction with ICU services. Physicians should devote adequate time to convey an honest and complete picture of the patient’s clinical condition to families. This will ease their understanding of the patient’s condition, ensuring family satisfaction.
Supplemental Material
Supplemental Material - Impact of Shared Decision-Making on Family Satisfaction With Intensive Care Services: ‘Share With Care’ has a New Meaning in ICU
Supplemental Material for Impact of Shared Decision-Making on Family Satisfaction With Intensive Care Services: ‘Share With Care’ has a New Meaning in ICU by Margiben Tusharbhai Bhatt, Souvik Chaudhuri, Sunil Ravindranath, Viha Atri, Sagar Maddani Shanmukhappa, Vishwas P, and Roshan Fernandes in American Journal of Hospice and Palliative Medicine®.
Footnotes
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.