
Abstract
Background
Empirical investigations on health care professionals’ (HCPs) perception of dignity have already spotted common themes in preserving dignity in end-of-life care. However, heterogenic assessment results of varying HCP groups exist. This pilot study wants to provide further evidence on HCPs’ rating of dignity-impairing aspects based on a patient-centered concept, especially regarding different underlying job profiles and other professional characteristics.
Methods
In a quantitative study design, the rating of dignity-impairing factors in end-of-life care via an adapted version of the Patient Dignity Inventory (aPDI) was assessed. Participants of the relevant professional groups were recruited via convenience sampling from a region of Germany.
Results
From the final sample of participants, 229 questionnaires were analyzed. The overall importance of each dignity-impairing aspect in end-of-life care was considered to be very high by all different HCP groups. Nonetheless, ratings differed between professions: nursing staff had the highest ratings of importance compared to both physicians and individuals with multiple occupations. Participants with previous knowledge in bioethics also rated some aspects as more important compared to those without this feature.
Conclusion
With the findings of this investigation, an insight of how professionals rate impairments of dignity at the end of life based on a patient-centered concept is given. Thus, a link between empirical research and medical ethics is added. Potential normative implications for HCPs in practice of a dignified care can be derived, consisting of actively addressing social topics as well as further stressing ethics as a fundamental subject in the training and continuing education.
Keywords
Introduction
Based on the 25th article of the Universal Declaration of Human Rights, 1 the subsequent corresponding General Comment of the United Nations Economic and Social Council includes “attention and care for chronically and terminally ill persons, sparing them avoidable pain and enabling them to die with dignity.” 2 (p9) As a consequence, a right to dignified dying and thus a normative claim not only for those who are confronted with a life-limiting disease but also those who offer health care services can be derived.
Health care professionals’ (HCPs) opinion or understanding of human dignity can correspond to the one that patients have.3,4 A questionnaire called Patient Dignity Inventory (PDI) is based on one empirically established concept of human dignity and addresses a broad range of dignity-related issues in terminally ill patients: Firstly, factors associated with or caused by the underlying disease; secondly, psychological and spiritual needs; and thirdly, external factors mediated mainly from the social environment. 5 These are factors that negatively influence human dignity as perceived by patients if deficits in the respective category occur.
Whereas it is easily comprehensible that affected patients themselves report aspects of their human dignity (in that case indeed a subjective concept), it remains a debatable question whether personal dignity can be assessed by others at all. 6 Nevertheless, by keeping in mind that it is the group of HCPs who deal with the variety of patients and their individual concept of human dignity, dignity assessment from a professional perspective can be set in relation to existing empirical evidence. Furthermore, dignified care is undoubtedly observable from the outside and its quantitative assessment by HCPs is existent.7-9 Thus, it seems to be a reasonable intention to gain insight and to compare the conception of human dignity by affected professionals.
Based on these reflections and the patient-centered concept of human dignity described above, the current study investigated how HCPs perceive potential impairments of human dignity of patients at the end of life. In addition, influences of the underlying job profile as well as other professional characteristics were explored. Thus, a contribution to the field of empirical research at the interface of end-of-life care and medical ethics wants to be delivered, resulting in potential normative and practical implications for those profesionally concerned with the subject.
Methods
Study Design
Sociodemographic and Professional Data of the Survey’s Participants. N = Number of Participants.
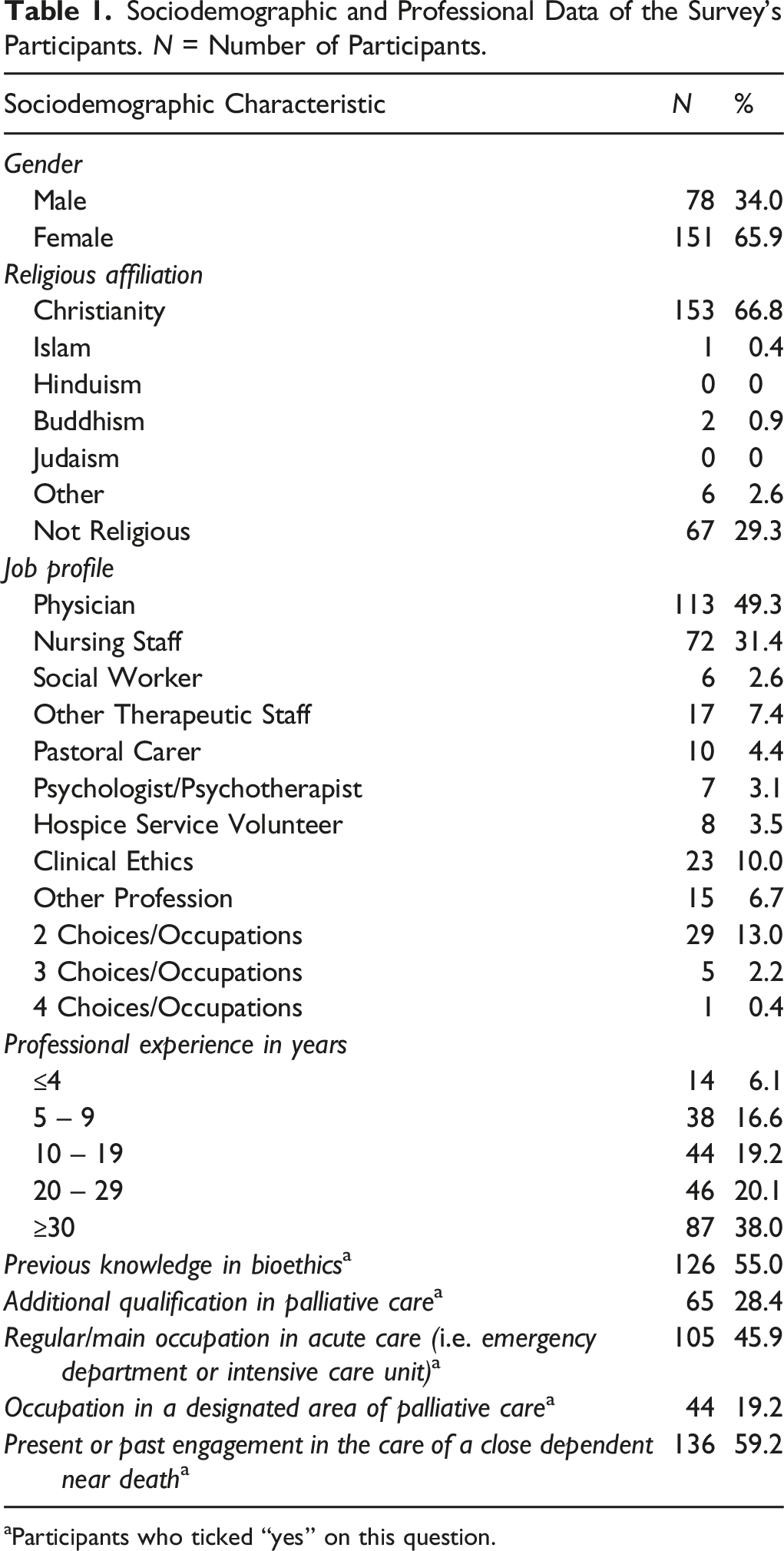
aParticipants who ticked “yes” on this question.
Setting and Subjects
Participation in the survey was voluntary and anonymous after the recipients received an invitational email either directly or via their respective head of the department/institution including information material. HCPs were recruited from the Heidelberg University Hospital as well as related institutions from the local area such as palliative care units of other hospitals or a specialist palliative home care team. The participating HCPs specified their respective job profile to the following (see also Table 1): physicians, nursing staff, psychologists/psychotherapists, other therapeutic staff (such as physiotherapists). Other non-therapeutic professions that play an essential role in the care of terminally ill patients were also included: social workers, pastoral carers, hospice service volunteers, and non-specified (“other profession”). There was no restriction to the underlying specialty so that HCPs from every discipline, also those who are not primarily working with patients near death but nevertheless share a certain point of commonality to the addressed topic, could participate in the study. Through the variety of included HCP groups, different perceptions of dignity at the end of life according to the respective professional background could be compared.
Data Collection
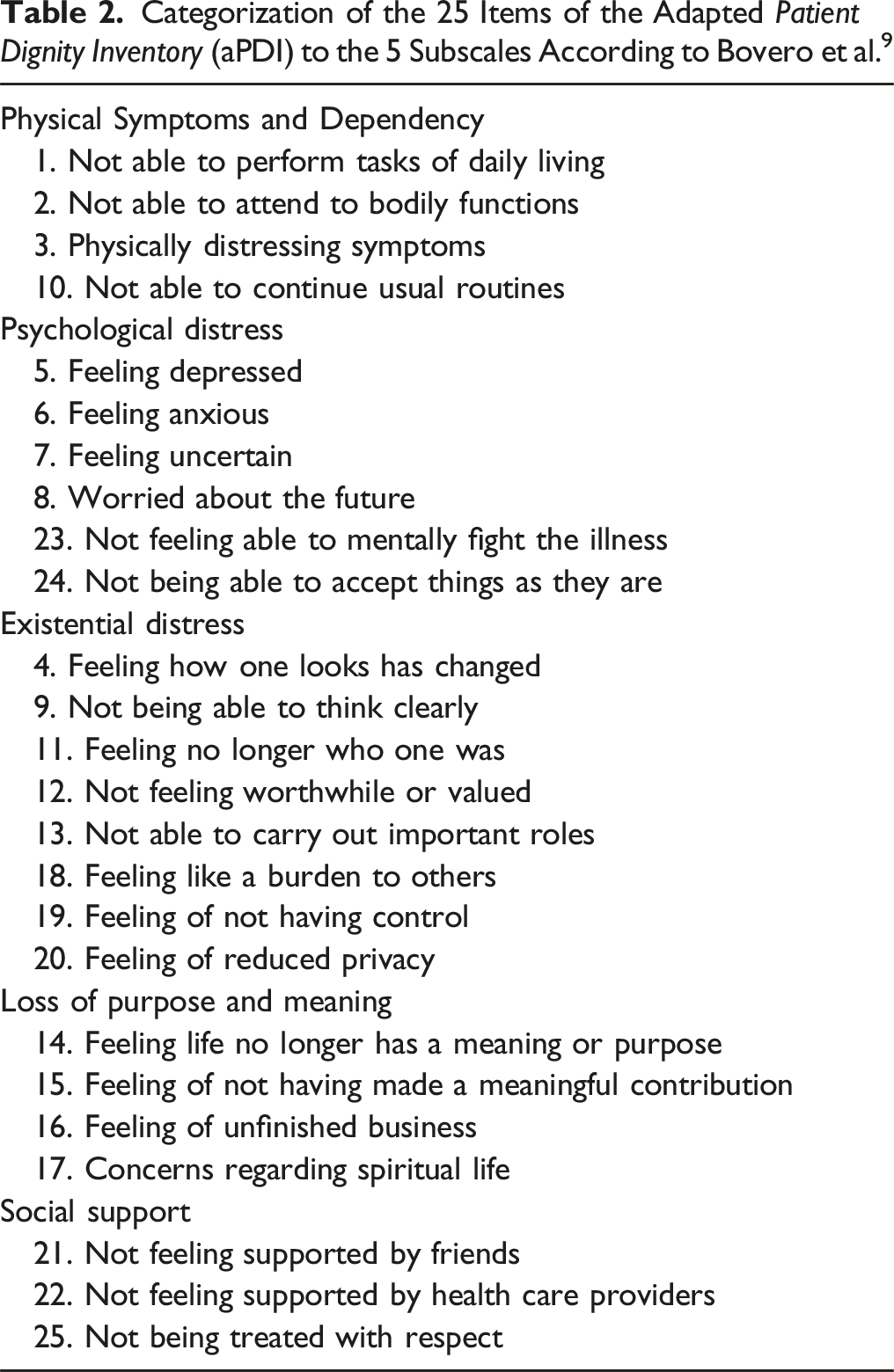
In order to investigate HCPs’ perception of impairments of human dignity at the end of life, an adapted version of the PDI was used. The PDI is a validated, reliable, quantitative self-questionnaire that addresses a broad range of dignity-related distress factors in terminally ill patients. 11 Participants completed the adapted PDI translated to German for the HCPs (instead of patients). The guiding question for the completion of the adapted PDI (aPDI) was: “How would you assess impairments of a patient’s human dignity at the end of life from your professional perspective?”. The aPDI is attached in Appendix 1.
Categorization of the 25 Items of the Adapted Patient Dignity Inventory (aPDI) to the 5 Subscales According to Bovero et al. 9
Data Analysis
Statistical analyses were executed using the software SPSS Statistics Version 27. There were no missing data across all variables. Data were screened for violations of the assumption of normality as well as univariate and multivariate outliers. Univariate outliers were defined as any value one and a half times the interquartile range (1.5 x IQR) below the first quartile (Q1) or above the third quartile (Q3) in any of the aPDI subscales. Mahalanobis distance was used to identify multivariate outliers. However, data of the participants were only excluded from the analysis if there were multiple outliers in the aPDI subscales of one data set or if there were multivariate outliers.
For the statistical analyses, participants were divided into different groups according to their stated job profile with participants indicating multiple job profiles being assigned to a separate group called “multiple occupations”. The underrepresented job profiles were pooled into one group named “other profession” (see Table 1). The aPDI subscales were compared between groups using a mixed analysis of variance (ANOVA) with the professional group (physicians, nursing staff, “other profession”, “multiple occupations”) as a between-subject factor and the aPDI subscales (“Physical Symptoms and Dependency”, “Psychological Distress”, “Existential Distress”, “Loss of Meaning and Purpose”, and “Social Support”) as a within-subject factor.
Multiple analyses of variance (MANOVA) were used to assess the influence of the following factors on the aPDI subscales: religiousness, the statements of having previous knowledge in medical ethics, additional qualification in palliative care, regular/main occupation in acute care (e.g., emergency department or critical care), occupation in a designated area of palliative care, and present or past engagement in the care of a close dependent near death. Due to the small or partially absent samples of non-Christians, any kind of stated religious affiliation was pooled in the group “religious”; the comparison group contained the participants with the statement of not being religious. In case of significant results, follow-up ANOVAs were applied for analyzing the association between each of the aPDI subscales and these factors. All the tests were two-sided, p values less than .05 were considered statistically significant. All assumptions of the statistical procedures were checked.
Results
Preliminary Analyses
Of the 297 total questionnaires received, 233 were fully completed, resulting in a sample of 233 participants (M age = 47.8, SD = 13.0, range: 22 – 81 years). A detailed response ratio can not be presented as the study’s design consisted of a convenience sampling (see above). For the statistical analysis, the data of 4 participants had to be excluded due to being statistical outliers (2 physicians, 1 “multiple occupations”, 1 “other profession”; see Data Analysis for details). Therefore, the final data set included 91 physicians (M age = 46.2, SD = 12.5, range: 28 – 70 years), 62 nurses (M age = 46.0, SD = 12.5, range: 22 – 63 years), 41 participants with other job profiles (“other profession”; M age = 49.7, SD = 12.9, range: 25 – 70 years) and 35 participants with multiple job profiles (“multiple occupations”; M age = 52.7, SD = 13.7, range: 28 – 81 years). Further details can be seen in Table 1. The number of participants in the group of physicians and nursing staff in Table 1 differs from what is presented here as n = 22/113 physicians as well as n = 10/72 nurses had the feature of multiple job profiles, thus excluding them from their respective job group and pooling them in the group “multiple occupations”.
Main Analyses
How important do HCPs assess impairments of human dignity at the end of life and its composed aspects? The overall importance of each of the dignity-impairing aspects at the end of life – displayed through the aPDI subscales – were considered to be very important, as can be seen in the mean scores of at least 3.3 up to 4.2 of each subscale (see Figure 1). The mixed ANOVA revealed a significant main effect of the job profile on the aPDI subcales (F (3, 225) = 4.31, p = .006, η
p
2
= .05). Tukey post-hoc analysis revealed that nursing staff rated all of the aPDI subscales as more important compared to both physicians (p = .012) and the group of “multiple occupations” (p = .013), whereas there were no significant differences in the aPDI subscales between nursing staff and “other profession” (p = .222). In addition, there were no significant differences among physicians, “multiple occupations”, and “other profession” (physicians vs “other profession”: p = .919; physicians vs “multiple occupations”: p = .893; “other profession” vs “multiple occupations”: p = .667). Results (means and standard deviations of the 5 subscales of the adapted Patient Dignity Inventory (aPDI) of each of the 4 groups: physicians, nursing staff, “other profession”, “multiple occupations”.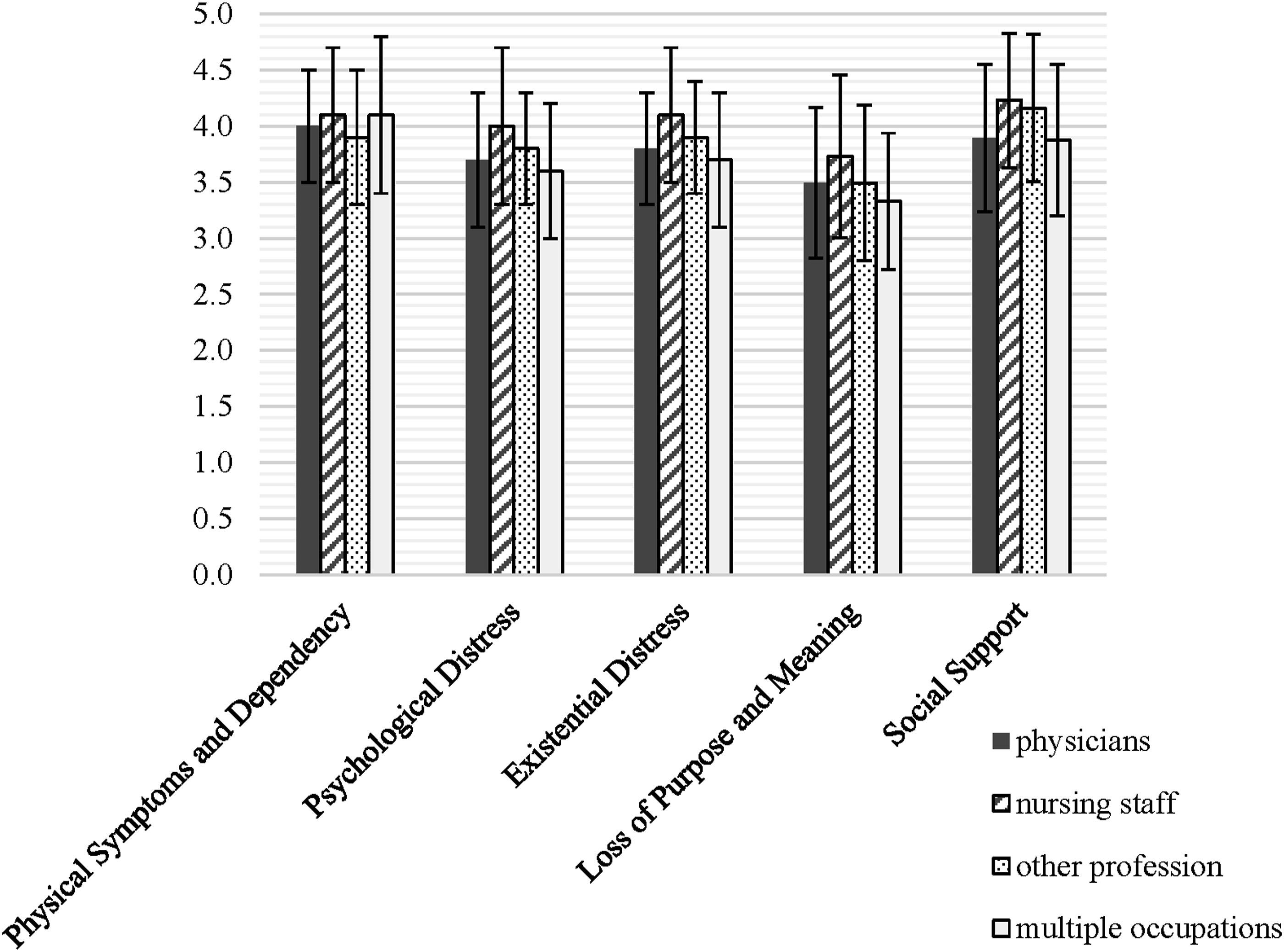
Additionally, the mixed ANOVA revealed a significant main effect of the aPDI subcales (F (3.37, 758.25) = 45.87, p < .001, η p 2 = .17, degrees of freedom corrected with Greenhouse-Geisser estimates of sphericity). Over all the participants, the aPDI subscales of “Social Support” (M total = 4.03, SD = .67) and “Physical Symptoms and Dependency” (M total = 4.02, SD = .56) were rated as most important, followed by “Existential Distress” (M total = 3.87, SD = .57), “Psychological Distress” (M total = 3.79, SD = .60), and finally “Loss of Purpose and Meaning” (M total = 3.53, SD = .69).
There was a significant interaction effect between the job profile groups and the aPDI subscales (F (10.11, 758.25) = 2.01, p = .029, η p 2 = .03, degrees of freedom corrected with Greenhouse-Geisser estimates of sphericity). The groups of physicians and “multiple occupations” rated the aPDI subscale “Physical Symptoms and Dependency” as more important compared to the aPDI subscale “Social Support”, whereas the groups of nursing staff and “other profession” rated the aPDI subscale “Social Support” as more important compared to the aPDI subscale “Physical Symptoms and Dependency”.
Are there different emphases on the perceived impairments of human dignity in end-of-life situations according to professional characteristics? The MANOVA revealed that the statement of having previous knowledge in bioethics had a significant effect on the aPDI subscales (Hotelling’s T = 0.64, F (5,223) = 2.87, p = .016, η p 2 = .06;). Follow-up ANOVAs revealed that having previous knowledge in bioethics led to a higher assessment of importance of the aPDI subscale “Psychological Distress” (F (1,227) = 4.57, p = .034, η p 2 = .02) compared to those who did not possess previous knowledge in bioethics. For the remaining aPDI subscales no significant effects were found (“Physical Symptoms and Dependency”: F (1,227) = 1.91, p = .168, η p 2 < .01; “Existential Distress”: F (1,227) = 2.59, p = .109, η p 2 = .01; “Loss of Purpose and Meaning”: F (1,227) = 0.001, p = .981, η p 2 < .01; “Social Support” (F (1,227) = 0.95, p = .331, η p 2 < .01).
The MANOVA revealed no significant effect of each of the following statements (“yes” vs “no”) on the aPDI subscales: possession of additional qualification in palliative care (Hotelling’s T = 0.26, F (5,223) = 1.16, p = .329, η p 2 = .03), regular/main occupation in acute care (Hotelling’s T = 0.47, F (5,223) = 2.10, p = .067, η p 2 = .05), occupation in a designated area of palliative care (Hotelling’s T = 0.17, F (5,223) = .76, p = .568, η p 2 = .02), present or past engagement in the care of a close dependent near death (Hotelling’s T = 0.02, F (5,223) = .73, p = .601, η p 2 = .02), being religious vs non-religious (Hotelling’s T = 0.18, F (5,223) = .79, p = .557, η p 2 = .02).
Discussion
In this quantitative survey, impairments of human dignity at the end of life based on a patient-centered concept were estimated as important or very important across all participating HCPs. This finding can be regarded as encouraging because the impression of undignified treatment of patients in our health care system sometimes arises.12-14
Nursing staff had the highest ratings of importance on the overall assessment of dignity-impairing aspects at the end of life compared to the other professional groups. Across all professions, support from the social environment as well as physical symptom control and self-reliance were assessed as more important than other dignity-related aspects. Between these two aspects, the rank of importance varied only according to the respective profession, with nursing staff and the non-classifiable job profile-group attributing top priority to social support, whereas physicians and the ones with multiple professions rated physical symptoms and dependency as most important. What has already been discovered by other empirical investigations concerning human dignity in end-of-life care is that physical symptom relief is of utmost importance to HCPs.5,9 In line with our study, nursing staff tends to rate psychological, existential, spiritual, and social issues as more important than the other HCPs, whereas in the literature psychologists appeared to be more sensitive to the existential concerns compared with physicians. 9 In terms of social and/or relational factors it has been found that this dimension seems to be underestimated by HCPs in contrast to patients and their significant others.6,9,15
One possible explanation for the high means on all scores of the nursing staff is the circumstance that this HCP group is the one that spends the most time close to the patient. Independent of whether the interaction with the patient takes place in an acute care setting, on a palliative care ward, or in an outpatient environment, nursing staff apparently gets to know all the various facets of dignity relevant for the patient at first hand. Furthermore, even though ethical standards for most of the various groups of HCPs exist, the fundamental nursing responsibilities according to the ICN (International Council of Nurses) Code of Ethics for Nurses includes “to alleviate suffering and promote a dignified death.” 16 (p2) This marks another possible explanation why the link between the general and the nurse-specific claim of respecting human dignity at the end of life seems so prominent. In addition to discipline-specific codes of ethics, professional degree programs emphasizing different influences on life domain categories (i.e., physical, mental, social, spiritual) or topics about care focus such as person-centred care (PCC) could be further implemented for each practice type. 17
Based on the results of the present investigation, previous knowledge in bioethics seems to influence the assessment of human dignity in end-of-life situations. Whereas the individual concept on human dignity probably derives from personal experiences and deliberations for most of the HCPs, those with a special bioethical background might have a more general approach based on theoretical considerations of normative principles. Therefore, it would be interesting to perform detailed studies on which specific reflections influenced the participants’ choices with a background of knowledge in bioethics. Another emerging question would be whether the implementation of ethics as a subject in the training of HCPs should be further stressed.18,19 Additionally, in terms of future study recommendations especially concerning the professional group of physicians, it would be interesting to know how the specialty background of all those represented in terminal care (internists, family physicians, anesthesiologist, etc.) might impact the ranked perceptions of end-of-life issues.
However varying the importance of different aspects of human dignity at the end of life might be assessed by different HCPs, it seems important to conclude that there is no homogenous concept on this topic for a single HCP group as there are highly individual perceptions of dignity. This fact can only be considered by a process of shared discussion with the patients and their significant others. An appreciative acknowledgement of the patient’s values, ideas and preferences is therefore inevitable. The challenge in our health care system’s everyday life is to provide the space and environment to encounter the need of acknowledging this variety of “dignity at the end of life” on the patient’s as well as on the HCPs’ side.
The following limitations must be considered: 1. No standardized quantitative instrument regarding human dignity and its impairments at the end of life from the perspective of HCPs could be found. The instrument used in this survey is not designed for dignity assessment by others than patients and therefore not validated for the application of this study’s purpose/audience. Furthermore, the PDI was not translated by a professional translator, thus not meeting the recommended specific standard. 20 Thus, the questionnaire’s validity and other psychometric variables are violated considerably. However, with the insights of this investigation and other comparable studies, evidence for the need to perform a validation study in this setting is growing. 9 For future studies, a reliable and validated instrument which directly assesses the perception of HCPs on impairments of human dignity should be developed. 2. Participants emerged from a geographically small area in the southwest of Germany. A more diverse setting concerning geographical or cultural circumstances in the surveyed sample could have led to different results as the cultural background is likely to influence some aspects of dignity. 21 Furthermore, a demographic criteria such as “years living in Germany” was not included in the completed exploratory study. This has to be kept in mind as on the one hand, self-identified religious affiliation is not necessarily tethered to particular ethnicity, and on the other hand, palliative care across several European countries may vary according to different cultural norms that influence care at the end of life. 22 Further studies addressing cultural influence on human dignity are needed to explore the relation between culture and perceptions of dignity. 3.1. Asking individual institutions to recruit participants for the survey may have introduced a selection bias. Nevertheless, this study was designed as a kind of proof of concept-study and not intended to present an unselected sample. 3.2. Analogous pertains to the limiting dynamics regarding the use of convenience sampling, thus resulting in a limitation of population-generalizability for example. 23 3.3. In order to provide a sufficient sample size for the statistical analyses and comparison of the results, differing job profiles with a low number of participants had to be pooled. The resulting two groups represent very heterogeneous groups due to the variety of jobs included in these groups. Future studies should recruit homogeneous groups with sufficient sample sizes for each group to allow more precise statistical analyses.
Conclusions
Empirical science can help to better understand the idea of human dignity at the end of life in a real-world application, here for HCPs. The analysis of the present investigation showed differences in the assessment between various medical professions. The job profile and the feature of having previous knowledge in bioethics could be extracted as significantly influencing factors on the assessment of impairments of a patient-centered concept of human dignity at the end of life.
With the insights from the gained results of this study, implications on the ethical level for HCPs involved in the care of people near their life’s end can be drawn with cautiousness concerning the methodological and cultural limitations. The first two implications listed here are of normative value, the two others seem of practical relevance: 1. To ascribe a higher priority to the social dimension of dignity in end-of-life care, thus involving significant others and addressing topics of social participation should be minded especially. 2. The HCPs’ high assessment scores underline the respect for dignity of their entrusted people, thus implying that the status quo for a dignified end-of-life care in practice is encouraging. 3. As a third potential implication, to conserve the professional ethos for HCPs as well as to keep a high standard of care in the end-of-life setting, regular reflections and interprofessional exchange about the concept of human dignity seem indicated. 4. Also, the relevance of ethics as a fundamental subject in the training of HCPs can be regarded as a potential further implication gained from the survey’s findings.
Supplemental Material
Supplemental Material - Impairments of Human Dignity at the end of Life Quantitatively Assessed by Health Care Professionals: A Pilot Study From Germany
Supplemental Material for Impairments of Human Dignity at the end of Life Quantitatively Assessed by Health Care Professionals: A Pilot Study From Germany by Florian Derler, and Emilia L. Mielke in American Journal of Hospice and Palliative Medicine®
Footnotes
Acknowledgments
Special thanks belong to Stefan Ladinig for proofreading an earlier version of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.