
Abstract
Background
Caregivers of cancer patients are at increased risk of depression and other health challenges. There is limited understanding of the role of the caregiver’s own family members in promoting or discouraging mental wellbeing. Family functioning conceptualizes how family members interact to promote a positive family environment and has the potential to impact caregiver mental health. The purpose of this study is to assess the association between family interactions and depressive symptoms among family caregivers of cancer patients.
Methods
Secondary analysis of baseline data from an NIH-funded randomized control trial of family caregivers of cancer patients recruited from academic palliative care clinics at three sites (2 Midwest, 1 East). We tested for an association between caregiver responses to the Family Quality of Life in Dementia-Family Interactions Subscale and Patient-Reported Outcomes Measurement Information System Depression Short Form 8A using a block-wise approach to linear modeling.
Results
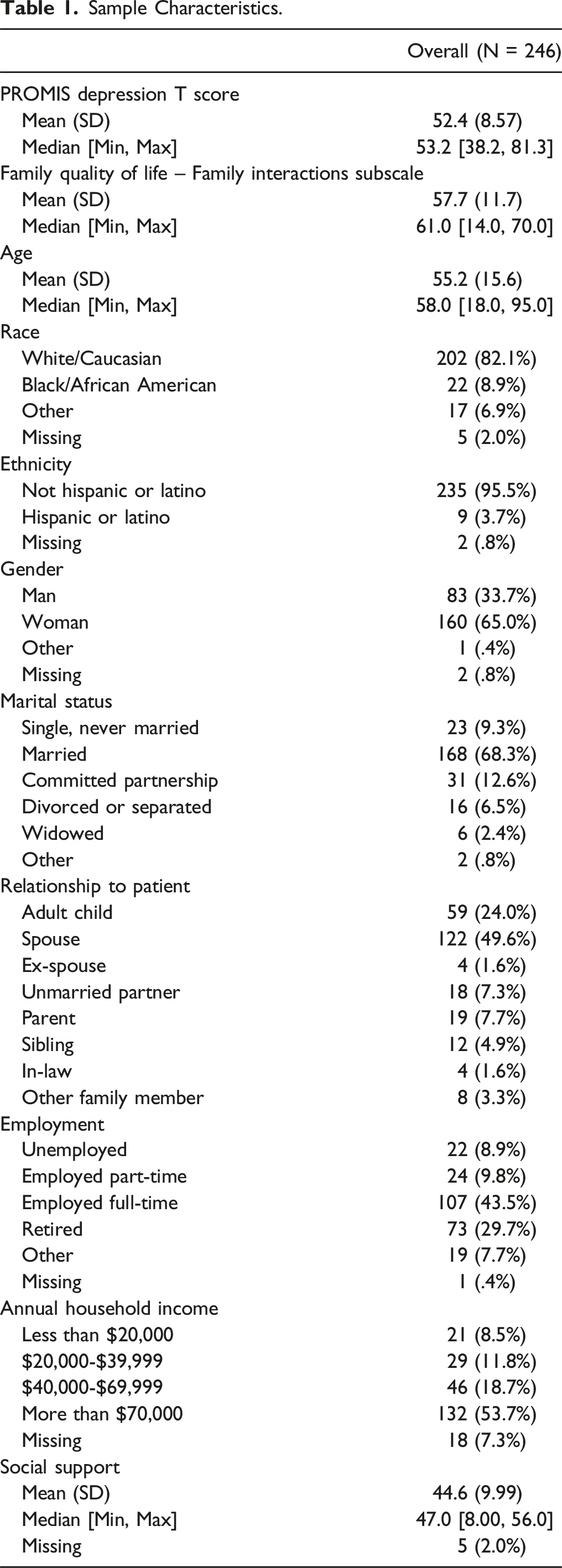
A total of 246 caregivers were included in analysis; caregivers were mostly White (82%), not Hispanic or Latina/o (96%), and female (65%), with an average age of 55 years. Overall, participants had high family interactions (mean 57.7, sd 11.7) and an average depressive symptom burden (t-score 52.4, SD 8.57). Family interactions was significantly negatively associated with depressive symptoms (b = −.163, se = .057) when accounting for relevant covariates.
Conclusion
Family caregivers with more positive family interactions are likely to have fewer depressive symptoms, suggesting family functioning may play a key role in bolstering family caregiver mental health and wellbeing.
Introduction
Caregivers of cancer patients provide tremendous support to family or friends experiencing cancer—often at significant burden to themselves.1,2 The provision of cancer care is increasingly shifting towards outpatient and home-based care, and family caregivers are playing an increasingly vital role in supporting patients throughout their cancer journey. 3 Caregiving tasks may include accompanying and participating in medical appointments, giving medications regularly, assisting with toileting and bathing, preparing meals and/or feeding, and providing emotional support for the cancer patient. While caregiving can be a rewarding experience,4,5 the literature highlights the tremendous burdens of caregiving.1,6–11 A 2015 report by the National Alliance for Caregiving reported that 62% of caregivers experience high burden situations. 3
The toll of caregiving can have serious implications for the health of caregivers, including worse physical and mental health outcomes.12–16 Depression is a serious illness that can impact mood, feelings, and behaviors. 17 Depressive symptoms persisting for prolonged periods of time may progress to a major depressive disorder which can have serious implications including increased risk for suicide, which is higher among older adults and women. 18 In addition to biological factors, the literature has firmly established the role of environmental factors contributing to the risk of depression, such as stress and exposure to adverse life events.19,20 Caregivers of cancer patients have particularly high rates of depression, with a recent meta-analysis of more than twenty thousand caregivers demonstrating that almost half met criteria for depression. 19 Several factors have been implicated in worse caregiver mental health outcomes, including the demands of being a caregiver, competing roles in the caregiver’s personal life, and lack of social support.21–23 Given the tremendous mental health impacts of cancer caregiving, it is imperative to understand the factors that can help strengthen caregiver mental health.
One important factor in cancer caregiving mental health that is inadequately addressed in the literature is the role of the caregiver’s family in promoting (or discouraging) wellbeing. Family functioning is a broad concept representing how or to what degree family members’ interactions and ways of relating to one another promote an environment conducive to clear communication, role performance, cohesion, and good affect regulation. 24 In the context of illness, how well family members cope with and adjust to family stress is an important indicator of family functioning. 25 A well-functioning family unit can positively impact physical and mental health 26 ; conversely, individuals with depressive symptoms may have poor family interactions or respond negatively to family members expressing optimism and reassurance, resulting in excessive interpersonal conflict.27,28 Although robust family functioning has been demonstrated to improve cancer patient outcomes,29,30 there have been few studies assessing the impact of family functioning on outcomes for caregiver physical or mental health. Additionally, much of the literature has focused on subconcepts, such as family cohesion25,29,30 and fulfilment of family roles, 25 with less attention given to family interactions. Family interactions describes the pattern of how family members interact with each other and the factors impacting these interactions. 31 This gap in knowledge has been noted in calls to include family systems based work within palliative oncology research. 32 In other populations, researchers have shown that better family functioning is associated with improved mental health among dementia caregivers,33,34 heart failure caregivers, 35 and military spouse caregivers of veterans with post-traumatic stress disorder following war— 36 all of whom experience stressful and burdensome care similar to caregivers of cancer patients. The few available studies in palliative oncology demonstrate that cancer patients and their caregivers have different perspectives on family functioning. Despite traversing the illness experience together, caregivers of cancer patients are more likely to report that family functioning worsens over the course of the illness,37,38 which further highlights the need for dedicated caregiver-focused assessment.
Given the extraordinary mental and emotional toll of caregiving for cancer patients and the potential for deleterious subsequent effects, it is critical to understand which factors are associated with caregivers’ psychological wellbeing. Cohen and Willis proposed the Stress Buffering Hypothesis as a framework to understand how social support may intervene in the relationship between stress and deleterious mental health outcomes, 39 and prior studies have demonstrated that having a robust social support network is associated with better mental health outcomes among caregivers of cancer patients facing substantial stressors.19,40–42 This study builds on existing research by focusing on families as social support networks and potential sources of social support. More specifically, the purpose of this study is to assess the association between family interactions and depressive symptoms among family caregivers of cancer patients. Based on the current evidence, we hypothesize that there will be a negative association between the perceived quality of caregivers’ family interactions and depressive symptoms while adjusting for relevant covariates.
Methods
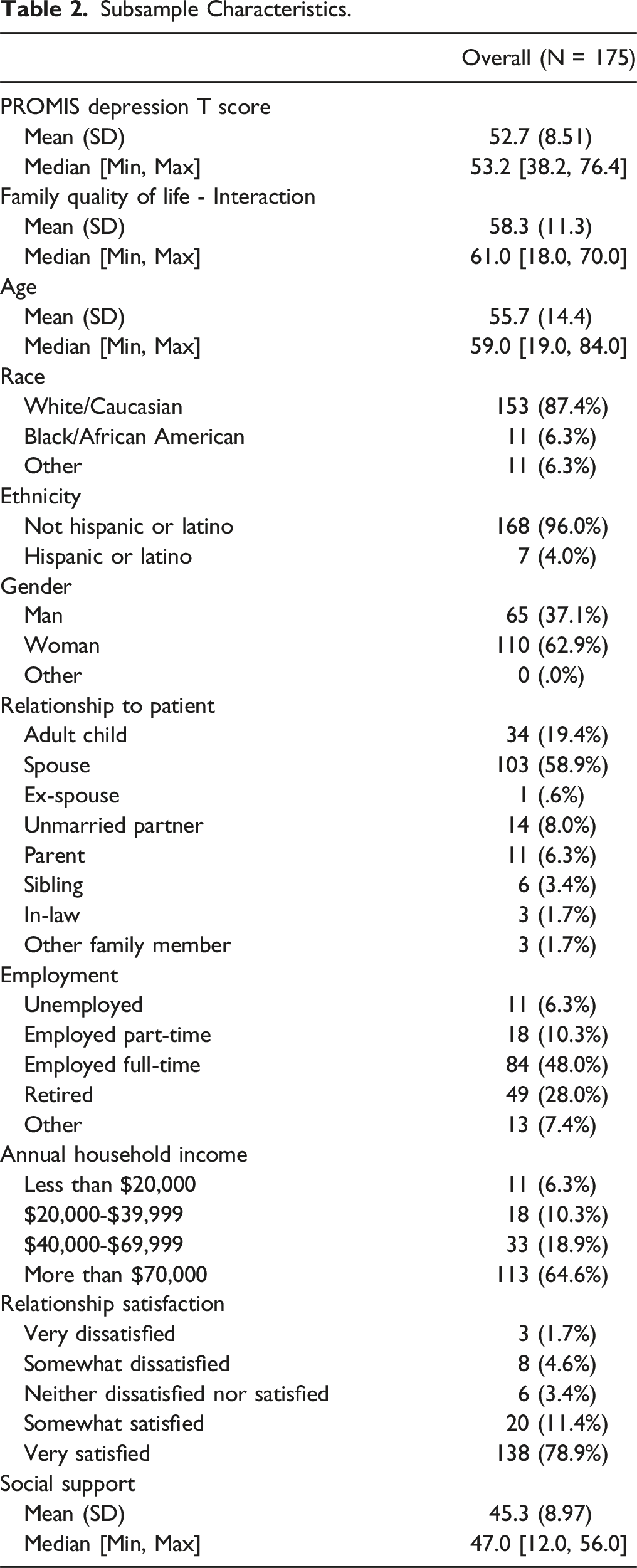
We conducted a secondary analysis using baseline data obtained from “Problem-solving Therapy for Cancer Caregivers”, an ongoing multi-site, randomized clinical trial that funded by the NIH NCI (R01CA258311). Participants were family caregivers enrolled from academic palliative care clinics in the USA (two Midwest and one East). Participants were required to be at least 18 years old and actively serving as the unpaid family caregiver of a patient with cancer who is receiving outpatient palliative care. The definition of “family caregiver” in this trial pertains to individuals who play a significant role in the patient’s care, without requirement of a legal or biological relationship. For the present study, 246 participants were included in our analysis. Given the potentially unique relationship between family interactions and depressive symptoms among caregivers of different marital/relationship statuses, we also conducted a subset analysis on 188 participants who reported being married or partnered; this subset analysis, similarly, analyzed the association between family interactions and depressive symptoms. The study protocol was approved by the Institutional Review Board at Washington University in Saint Louis.
Explanatory and Outcome Variables
Family Quality of Life in Dementia-Family Interactions Subscale
The primary factor we focused on in our models was family interactions, which we measured with the Family Interactions subscale of the Family Quality of Life in Dementia scale (FQOL-FI). The development and validation of the complete scale are extensively described in the literature. 43 This measure’s score is calculated by summing the responses of 14 items, which are rated on a 1-5 Likert-type scale with agreement anchors. The Family Interactions subscale does not include items or prompts related to dementia; statements pertain to various aspects of family interactions, such as open communication, addressing challenging topics, and displaying love and care among family members. Examples of these statements include: “My family is able to handle life’s ups and downs,” and “my family members support each other to accomplish goals”. 43 The total scores can range from 14 to 70, with higher scores indicating a better perceived quality of family interactions. 43 FQOL-FI demonstrated high internal consistency reliability in our sample (Cronbach’s alpha = .94).
Patient-Reported Outcomes Measurement Information System (PROMIS) Short Form v1.0 – Depression 8a
In our models, the primary outcome was depressive symptoms, which was assessed using the PROMIS Short Form v1.0 - Depressive symptoms 8a. The PROMIS initiative, developed by the National Institutes of Health is dedicated to creating thoroughly tested patient-reported outcome measures. This measure has undergone validation in diverse populations44–48 and is extensively described elsewhere.49–51 The raw score for the PROMIS Short Form v1.0- Depression 8a is derived by summing the responses to 8 items. These items utilize a Likert-type scale ranging from 1 to 5, with frequency anchors, to assess symptoms of depression over the past 7 days. The raw scores for the PROMIS – Depression measure in our sample indicated high internal consistency reliability (Cronbach’s alpha = .92). Standardized T-scores are obtained by converting the raw scores have a mean of 50 and a standard deviation of 10. 49 Higher values on the T-score indicate more depressive symptoms.
Covariates
Demographics
During baseline assessments, participants provided self-reported information on several demographic variables. These variables included age, race, ethnicity, sex, marital/relationship status, relationship to the patient, employment status, and household income.
Multidimensional Scale of Perceived Social Support
We included social support, measured with the Multidimensional Scale of Perceived Social Support (MSPSS), as a covariate to account for the variance it might potentially explain in caregiver depressive symptoms in our models. The MSPSS is a validated instrument that consists of 12 items which evaluate an individual’s perceptions of support from family, friends, and significant others. 52 Given overlap in family-related questions in the Family Interactions subscale of the FQOL-FI, the trial excluded the FQOL-FI items measuring perceptions of social support from family members. Thus, the items utilized in our analysis focused solely on perceived social support from friends and significant others. These items consisted of 8 prompts, which participants rated their agreement or disagreement with using a Likert-type scale ranging from 1 (very strongly disagree) to 7 (very strongly agree). Example prompts include “I can talk about my problems with my friends,” “I can count on my friends when things go wrong,” and “there is a special person who is around when I am in need.” The sum of the responses to these items constitutes the measure’s score, which can range from 8-56; higher scores correspond to more positive perception of social support. The MSPSS had high internal consistency reliability in our sample (Cronbach’s alpha = .95).
Relationship Satisfaction
To assess relationship satisfaction, married or partnered respondents were asked a question generated by the researchers: “In general, how satisfied are you in your marriage/current partnership?” Participants provided their responses on a 5-point Likert-type scale, where higher scores indicated a higher level of relationship satisfaction.
Statistical Analysis
Statistical analyses were conducted using R Statistical Software version 4.2.1 (R Core Team 2021). Before testing the hypotheses regarding the relationships between family interactions and depressive symptoms, descriptive statistics were examined for all variables in the model. For continuous variables, descriptive statistics included mean, standard deviation, median, and range, while frequencies were examined for categorical variables. A block-wise approach was employed to estimate the linear models. The first model consisted of only the outcome variable and family interactions. In the second model, all covariates were added. In a third model, a subsample of respondents who were married or partnered was examined with the addition of relationship satisfaction as a predictor. The final model included demographic and contextual covariates as well. We report estimates and significance for individual variables, as well as the overall fit of the model. A significance level of P < .05 was used to determine statistical evidence of relationships between the explanatory variable and covariates and the outcomes. In addition to results for the main research objective, findings with practical significance were also reported. Model assumptions and diagnostics were examined using scatterplots for residuals and fitted values, a normal quantile-quantile (q-q) plot, and a scale-location plot. Missing data were managed using list-wise deletion.
Results
Sample Characteristics.
Subsample Characteristics.
Regression Results for Family Interactions and Depression.
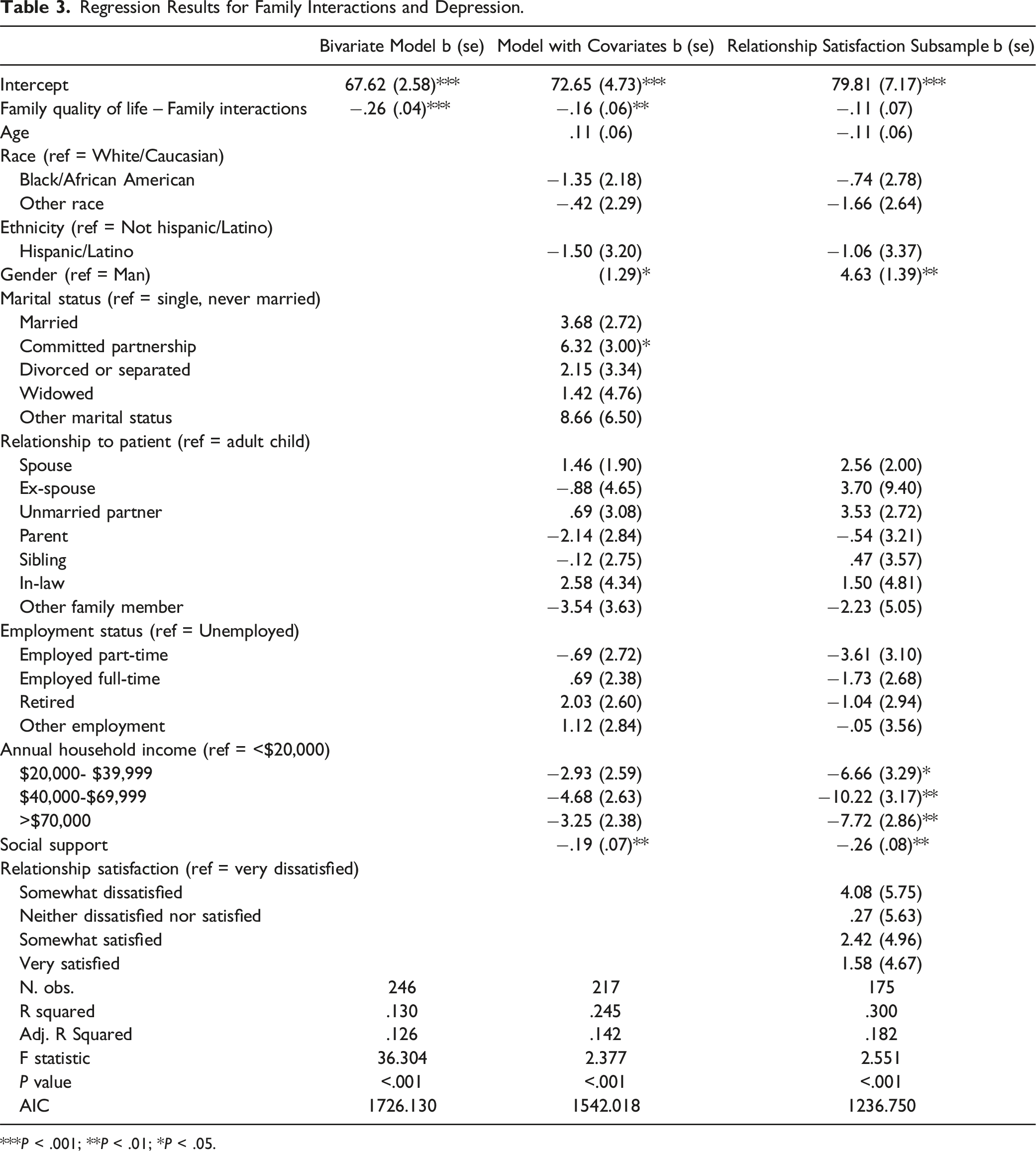
***P < .001; **P < .01; *P < .05.
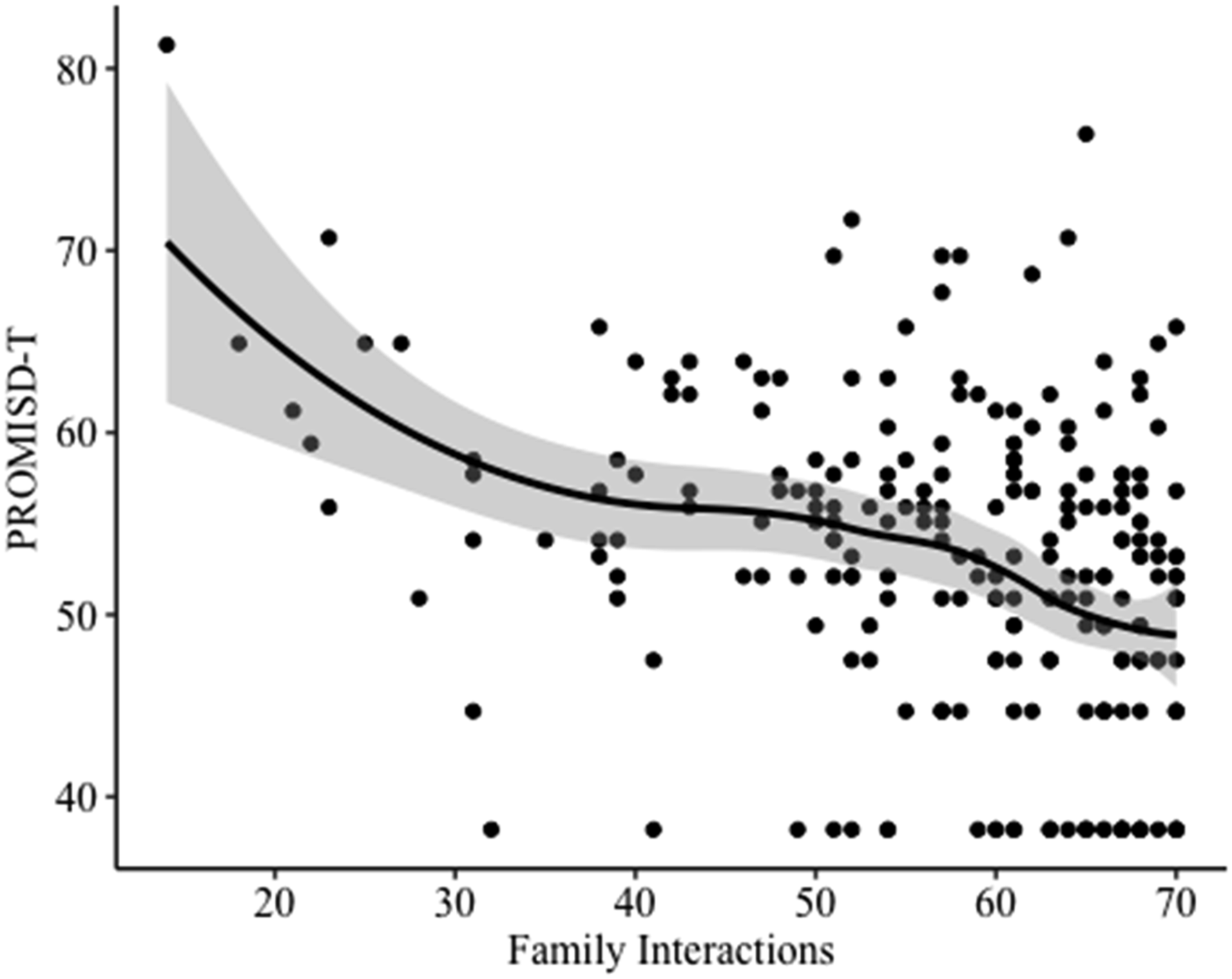
Scatterplot for bivariate relationship between Perceived Quality of Family Interactions and Depression.
Model results for our married or partnered subsample did not indicate a relationship between family interactions and depressive symptoms. This model did, however, indicate associations between gender, household income, and social support and depressive symptoms. Similar to the full sample, being a woman was associated with greater depressive symptoms on average. Having household incomes of $20,000 to $40,000 per year, $40,000 to $70,000 per year, or $70,000 per year or more was associated with lower depressive symptoms on average. Also similar to the full sample, every 10-point increase in social support was associated with a 2.6-point decrease in depressive symptoms (b = −.259, se = .083). The results did not indicate a significant association between relationship satisfaction and depressive symptoms. This subsample model demonstrated a good fit to the data (F = 2.551, P < .001) and explained 30% of the variation in depressive symptoms (R2 = .300). The statistically significant variables explained about 18% of the variation in depressive symptoms (adj. R2 = .182).
Discussion
This study explored the link between depressive symptoms and family interactions for caregivers of cancer patients. Findings supported our hypothesis of a negative relationship between depressive symptoms and family interactions. Our work extends existing literature on cancer caregiving and family interactions. It is well established in the literature that caring for someone with cancer affects family interactions. Ginter and Radina, 53 for example, provided qualitative narratives of the impact of caregiving on the family interactions of adult women providing care for their biological mothers with breast cancer, identifying pronounced alterations within the family system. Our work quantitatively examines caregivers’ perceptions of the quality of interactions within these potentially changed family systems and investigations the association between these perceptions and caregivers’ experiences of depressive symptoms. Additional studies examining a broader range of family types are needed to further elucidate the relationship between family interactions and caregiver mental wellbeing. Ultimately, understanding the association between family interactions and caregiver mental health may be useful to integrate into intervention-based support programs for families and family caregivers. There are several caregiver psychoeducational interventions which can improve caregiver depressive symptoms, although the impacts of these interventions diminish over time.54,55 Many caregiver-focused psychoeducational interventions focus extensively on (1) healthcare professionals’ screening and identification of caregiver needs, (2) education on assessment of the care recipient’s cancer-related symptoms and psychosocial needs, and (3) education on coping resources such as stress management and problem solving. 54 Few studies focus on interventions at the family-level, despite the notable impacts of family interactions on quality of life. 56
Notably, we also find that social support remains a key predictor of depressive symptoms across our models. Our findings are consistent with previously reported literature demonstrating the importance of social support to optimal mental health and wellbeing.39,54,57 The literature is clear that received and perceived social support can have different impacts 58 ; here we assess perceived social support. Whether or not caregivers receive social support from their network is likely paramount to whether they can reap the full benefits on their mental health. Finally, there are many types of social support that may be provided—instrumental, informational, and emotional support. 59 Future studies should examine the role of specific types of social support in bolstering family interactions, as these findings is likely to provide fertile soil for effective family interventions to improve caregiver mental health.
While this study has several strengths including a diverse population and more robust sampling of male participants than typically reflected in the caregiving literature, there are several limitations that should be acknowledged and considered by readers. First, our sample is well-resourced with more than half of the sample being married, employed, and with a household income >$70,000 per year which is well above the poverty level of $27,750 for a family of four in 2022 when data collection began. Bradley et al 60 longitudinally assessed cancer caregiving financial impacts and demonstrated that families with household income less than the median ($75,000) shoulder significantly more of the adverse financial impacts such as decreased income, increased debt, and having to stop working. It is likely that families from even more socioeconomically disadvantaged communities have additional stressors and fewer resources when taking on the caregiver role; future studies should strategically recruit from lower income communities. Additionally, our study population had limited recruitment of Hispanic families; given the significant increase in the Hispanic population over the last several decades 61 and the influence of cultural factors on the caregiving experience, 62 clinicians and researchers should seek to better understand the cultural nuances of the caregiving experience to work toward equitable, culturally-sensitive outcomes. Finally, we emphasize that our study focused on associations between variables; thus, we are unable to draw conclusions regarding causation or the direction of the relationship. We have framed much of our discussion within the context of family interactions as it relates to caregiver depressive symptoms; it is similarly possible that caregivers with depressive symptoms may have different interactions with their family members, creating worse family functioning. These nuances are captured in theoretical works on interpersonal models of depression 27 and in scholarly works.28,56 While this study adds to the existing literature in examining the understudied relationship between family interactions and depressive symptoms among caregivers of cancer patients, additional research is needed to understand the likely complex relationship more fully between these consequential variables.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Cancer Institute (R01CA258311; ![]() NCT04867122). The article’s contents are solely the responsibility of its authors and may not reflect the position of the study’s funder.
NCT04867122). The article’s contents are solely the responsibility of its authors and may not reflect the position of the study’s funder.