
Abstract
Background
As cancer patients approach the end of life, their needs become more complex, increasing the demand for palliative care. Advanced-stage cancer patients encounter increasing unmet psychological, physical, autonomy, and communication needs, reflecting the difference between patients’ perceived requirements and the support from health care professionals. The objective of this study was to synthesize qualitative evidence on unmet needs in palliative cancer care among inpatient and outpatient adults.
Methods
We conducted a meta-ethnographic review according to Noblit and Hare’s framework and the operationalized guidelines developed by Sattar. The eMERGe Reporting Guidance was followed. A literature search was conducted in Cinahl, Embase, Medline, Scopus, Web of Science, PsycINFO and Google Scholar for gray literature. For all the studies, direct quotes from the participants and authors’ results were identified, coded and analyzed in NVivo 1.7.1 and extracted as I and II order constructs from which higher third-order themes originated.
Results
Eight studies were included. Four new themes emerged, representing areas where palliative cancer care patients expressed a need for help: the need for comprehensive, patient-centered care, the need for maintaining a sense of autonomy and dignity, the need for attentive support to patients’ soul and the need for accessible and timely care.
Conclusions
Palliative care patients require a secure, suffering-free end-of-life journey with informed decision-making and team support. Ensuring continuity of care, validating their suffering, and allocating sufficient time are crucial aspects of care. This involves maintaining a consistent care plan, respecting patients’ emotions and experiences, and providing services tailored to individual needs.
Background
Globally, demographic, epidemiological and social dynamics are constantly changing, with an increase in chronic diseases leading to an escalation in the demand for palliative care.1-3
Palliative care has become an ingrained component of patient care in oncology with the aim of enhancing the quality of life of patients and families by alleviating symptoms, addressing spiritual and psychological needs, and supporting patients throughout their illness, even from the time of diagnosis.4,5
A shift in health status within the palliative care population can be discerned by improvements or deteriorations in specific symptoms, 6 which depend on the site and stage of cancer.7,8 As cancer patients near the end of life, they experience heightened complexity in their conditions, leading to more intricate needs. 9 The holistic conception of palliative care means addressing care needs in all areas and ensuring that patients can spend the remainder of their lives in peace.10,11 However, many patients do not readily voice their concerns to physicians or nurses. Some believe that suffering is inevitable with cancer or think that effective treatments are unavailable; this often causes these unaddressed needs to be overlooked, know as unmet needs.12,13
They reflect the discrepancy between an individual’s perceived essential need and the actual support given at every stage of the disease.8,14 When needs go unmet in palliative care, they can lead to profound distress and compromise patients’ quality of life. 15
Patients’unmet needs can easily lead to suggestions for improving patient care and outcomes.8,12 For example, cancer patients often rank functional loss as a top unmet care need due to the disease, its treatments, and related symptoms. This leads to decreased independence in daily routines as well as challenges in household tasks, social activities, and self-care. 16
In 2018, a systematic review by Wang T. et al found that advanced-stage cancer patients often face changing unmet needs due to swift disease progression, including psychological, physical, autonomy, communication, and nutrition needs that are influenced by cultural contexts, health care systems, and economic conditions. 17 In addition, the 2022 scoping review by Hart N.H. et al highlighted other significant unmet needs, such as financial needs and better dialogue with physicians, especially among patients with hematologic cancers. 18 Qualitative methods are suitable approaches that offer more profound insight into unmet needs than quantitative methods because the former consider participants’ deep experiences and subjective emotions that quantitative methods cannot measure. 17
In this study, we interrogate the literature for qualitative data on the experiences of adult patients in palliative oncological care to understand their views on the needs they perceive as unmet.
Aim
The purpose of this study was to synthesize qualitative evidence on unmet needs in palliative cancer care among inpatients and outpatients adults.
Method
The method chosen was a meta-ethnographic review which is a qualitative synthesis of evidence that seeks to provide new interpretations beyond individual study results rather than aggregate findings. 19 It is an interpretative approach synthesizing qualitative evidence to develop theories from existing research, ideal for generating new explanations and understandings of phenomena. 20 A meta-ethnographic review may offer new insights into unmet needs in palliative care to revise assistance for these patients by going beyond a simple summary of primary findings while maintaining the richness of primary studies.21,22 To undertake this review, we followed Noblit and Hare’s seven steps of meta-ethnography and the operationalized guidelines on this method developed by Sattar et al.23,24 To ensure comprehensive and transparent reporting of meta-ethnographic research, the eMERGe Reporting Guidance was followed. 19
The study was previously registered on the Open Science Framework (OSF), available at https://osf.io/gdy4x/.
Eligibility Criteria
Qualitative primary literature studies considering adult patients (aged >18 years) who were receiving oncological palliative care were included. The studies investigated the unmet needs of patients in this context using different methodologies (e.g., focus groups, interviews). No limits were placed on the year of publication, language or country of origin. Studies that met our inclusion criteria but lacked sufficient data for synthesis were excluded. The decision to evaluate cancer patients exclusively was driven by the need for a clinically consistent and homogeneous population. 7
Search Strategy
The research strategy was guided by the patient, interest, context (PICo) mnemonic, 25 which was developed in collaboration with the author FR, an expert database librarian. The databases consulted were Cinahl, Embase, Medline, Scopus, Web of Science, PsycINFO and Google Scholar for gray literature. The Supplementary Material includes an example of the search strategy used in the Embase database.
Study Selection
All the records extracted were first transferred to Mendeley software 26 for the removal of duplicates and subsequently to Rayyan Q software for study selection management and duplicate removal. 27 The titles and abstracts of all the records were screened first by title and abstract and then by full text by two reviewers (AL and DR). A third member was involved in resolving any disagreements (LC). Studies that did not meet the inclusion criteria were excluded for documented reasons. In cases of disagreement between reviewers, eligibility was resolved through discussion among all team members. Cohen’s kappa statistic was used to measure the interrater reliability of the study selection. 28 The entire process of study selection is presented in the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) diagram. 29
Quality Appraisal
To assess methodological rigor, we used the Critical Appraisal Skills Program (CASP) tool for qualitative research.30,31 The CASP tool comprises ten questions that target various methodological aspects of qualitative studies. This has prompted researchers to evaluate the appropriateness of research methods and the clarity and significance of findings. This user-friendly tool, which was approved by Cochrane and the World Health Organization, was designed for health-related research and suitable for our review context. 31 All the full texts were read and appraised for quality independently by two authors (IB and LC). Any disagreements were resolved by discussions with a third member (ML).
Data Extraction, Analysis, and Synthesis of Findings
Data from the included studies, including authors, publication year, origin, methodology, sample description, care context, and main results, were extracted.32,33
The chosen methodology identifies three data levels: first-order (participant quotes), second-order (authors’ findings), and third-order (meta-ethnographer interpretation).32,33 NVivo 1.7.1 software aided in data extraction and narrative analysis. 34 Two authors (IB and LC) conducted line-by-line coding of all study findings; our process involved revisiting first- and second-order constructs to forge common or divergent points among all the studies which were highlighted until a comprehensive synthesis of all studies was obtained, leading to third-order construct of the phenomenon. 35
These third-order themes moved beyond data summary and employed a line of argument approach to synthesize the data into a higher-level interpretation, enriching our conceptual understanding and contributing fresh insights to the literature. Finally, according to Noblit and Hare, a line of argument synthesis was developed33,36 with the results obtained previously collected in a mind map to maximize their impact.32,33 The whole process was iterative, revised through discussions within the review team and by consulting the original studies.
Results
Identification and Selection of Studies
We identified though the databases 11644 papers and 1000 papers from gray literature. A total of 6712 duplicates were removed. At the first level of screening, 5932 articles were included; at the next level of screening, 5844 articles were excluded, resulting in 88 articles for which the full text was read. The selection resulted in the inclusion of eight studies with agreement between the reviewers evaluated through Cohen’s k statistic, which was .66. Figure 1 shows the PRISMA flowchart of the entire study selection process. PRISMA flow diagram, 2020.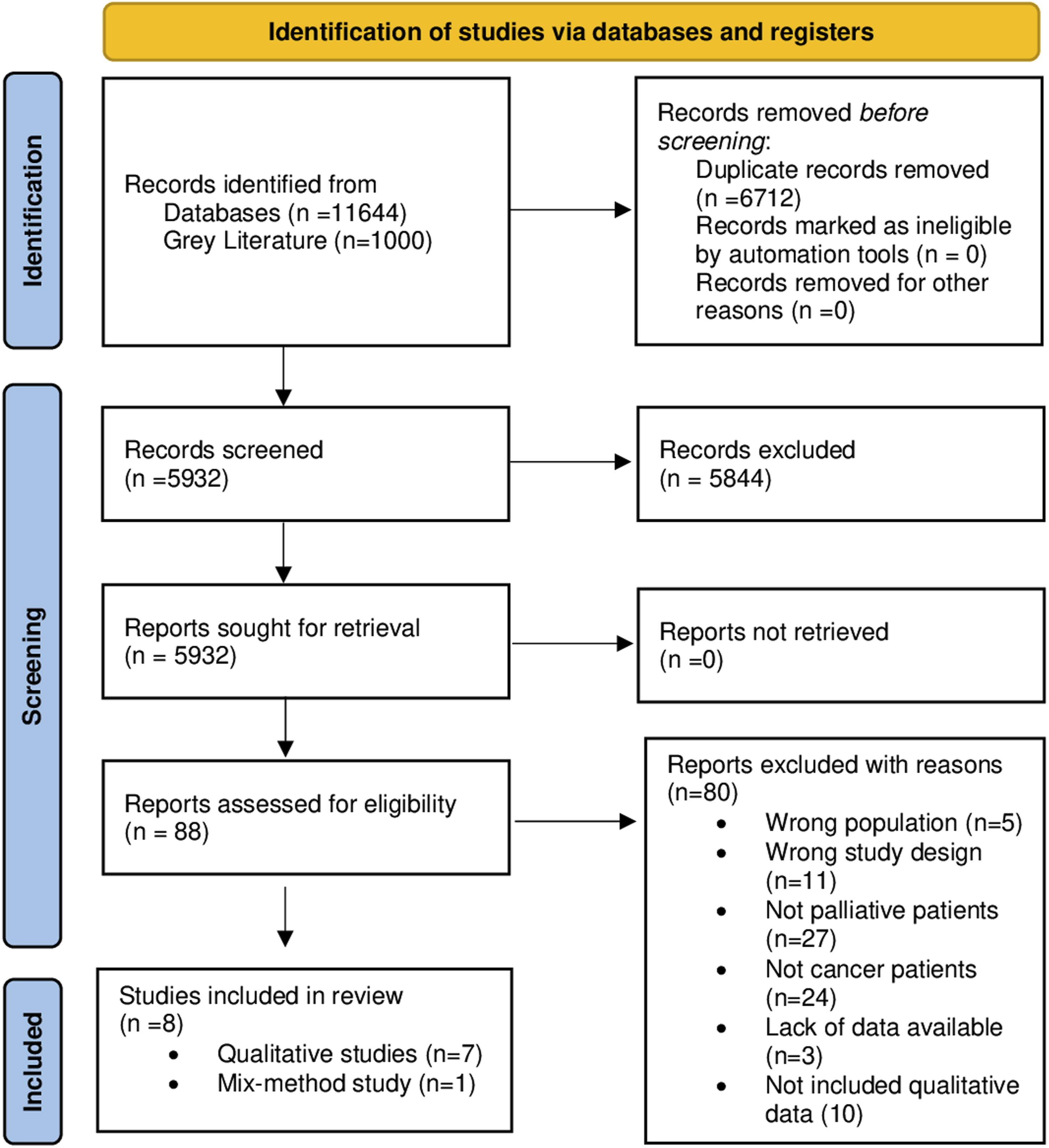
Characteristics of the Included Studies
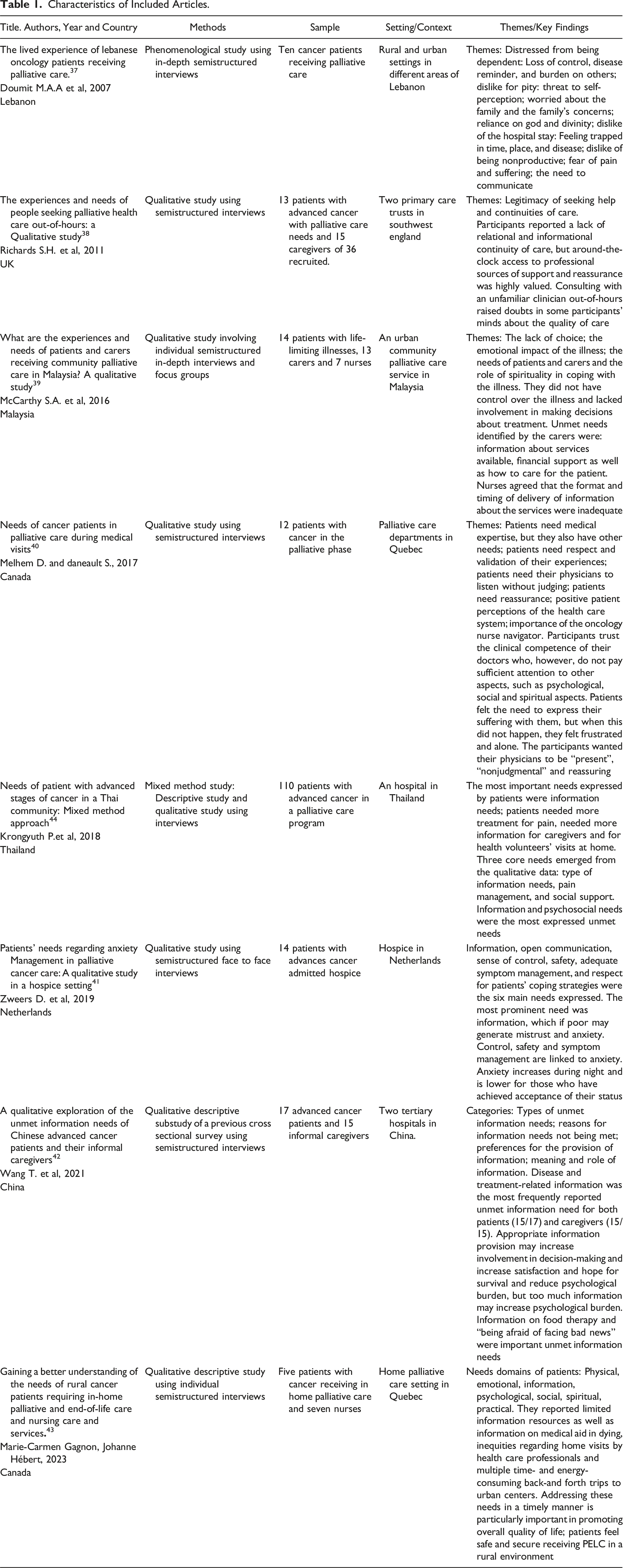
Characteristics of Included Articles.
Quality Appraisal of Included Studies Using CASP Checklist.
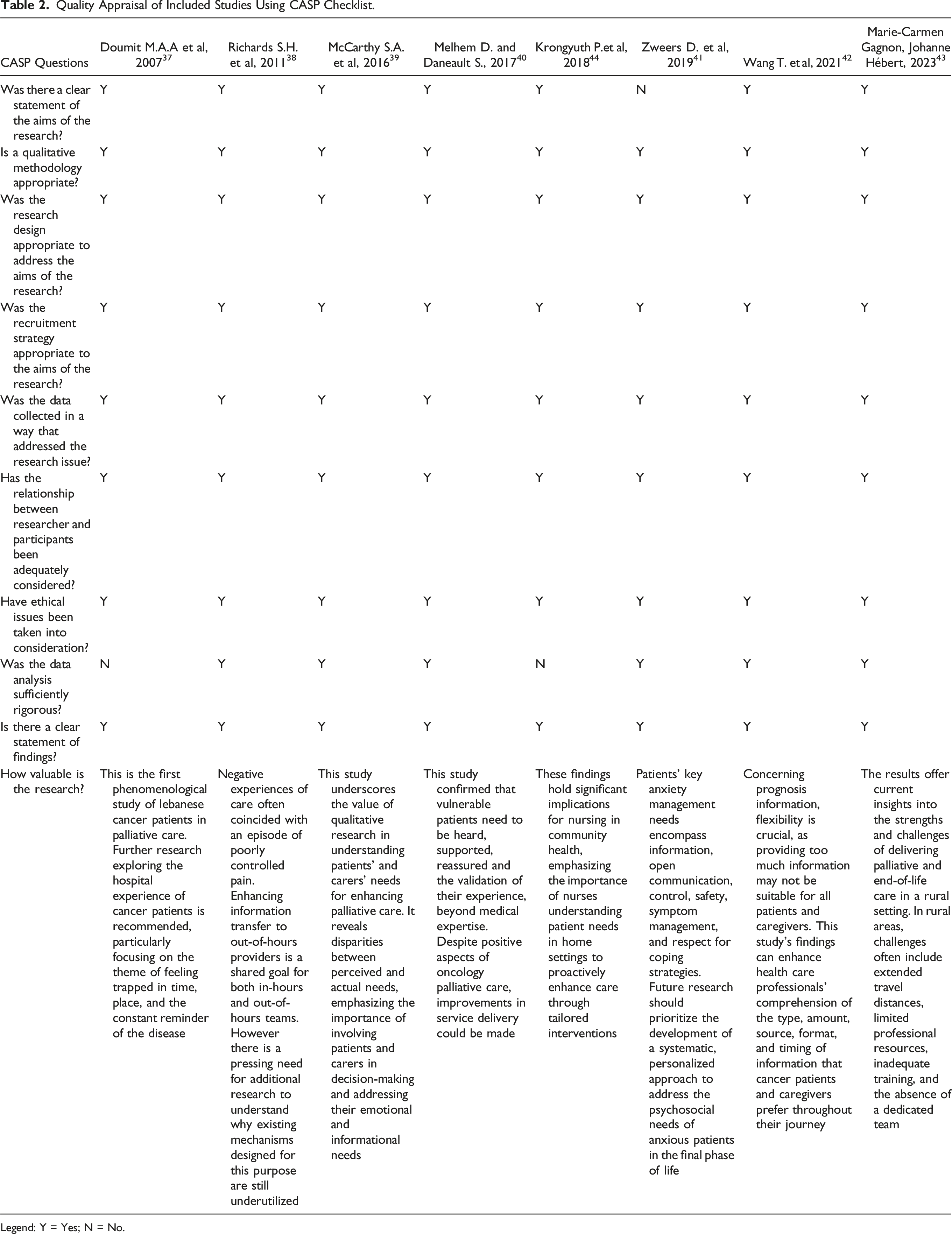
Legend: Y = Yes; N = No.
Qualitative Synthesis
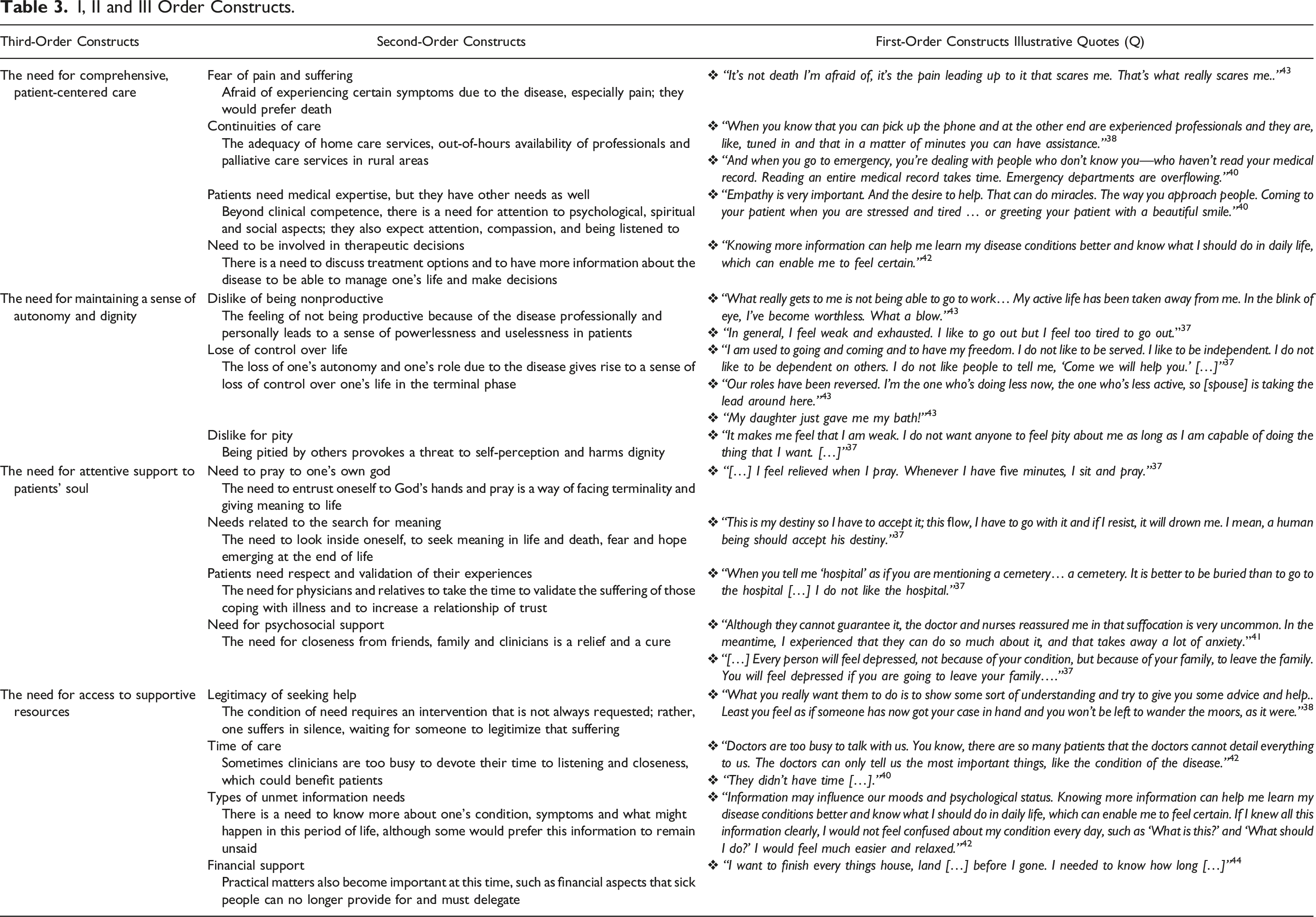
Line-by-line coding identified 129 first-order codes and 232 second-order codes. Furthermore, 15 subthemes and four themes were identified. The mind map in Figure 2 reports the connections between the two orders of constructs and the new third-order constructs resulting from the authors’ reinterpretation and reorganization of the results of the included studies. Mind map of order I, II and III constructs.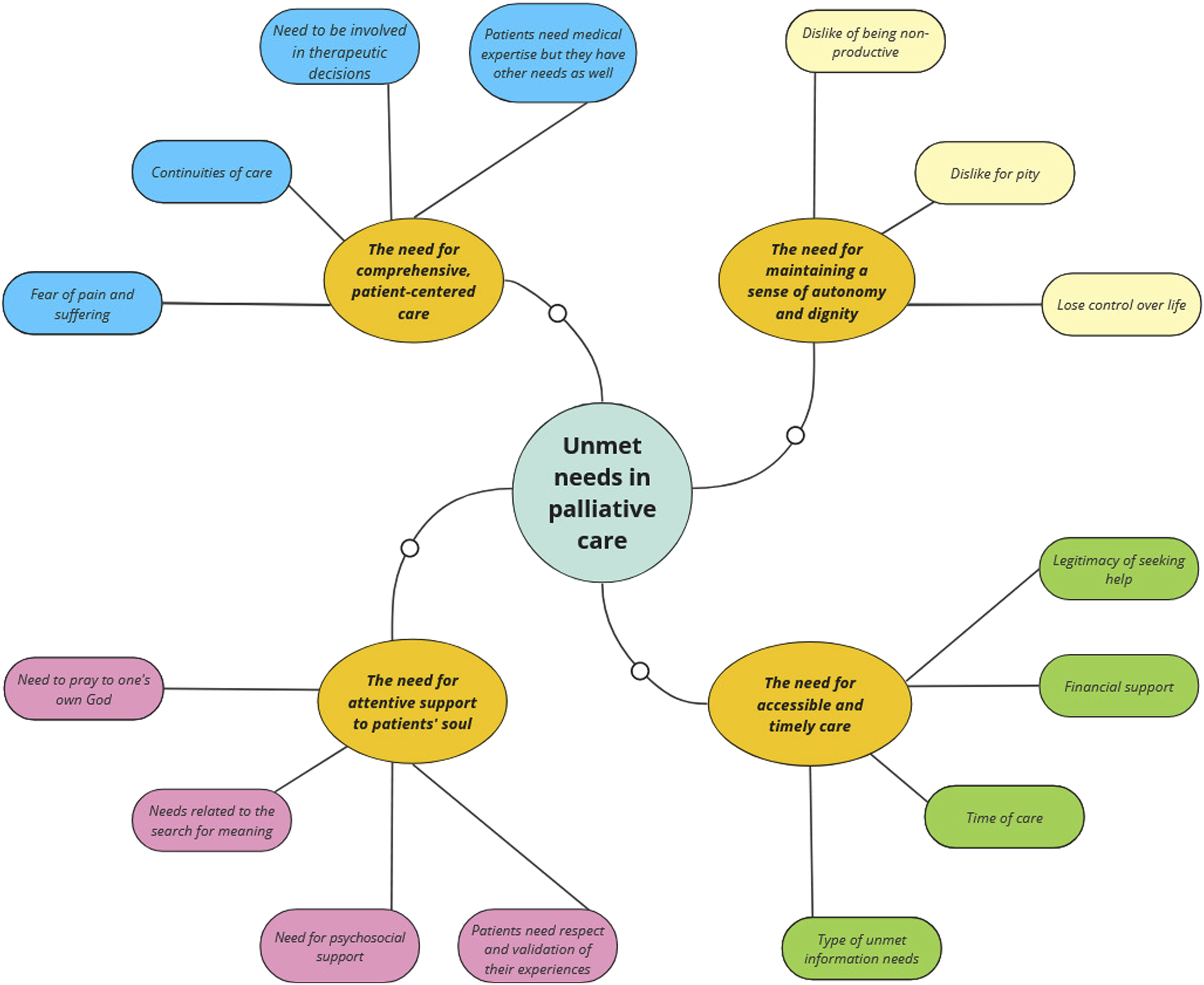
The four new themes that emerged and represented the areas in which palliative cancer care patients expressed the greatest need for help were as follows: the need for comprehensive, patient-centered care; the need for maintaining a sense of autonomy and dignity; the need for attentive support to patients’ soul; and the need for accessible and timely care.
I, II and III Order Constructs.
Unmet Needs in Palliative Care
The Need for Comprehensive, Patient-Centered Care
The theme “the need for comprehensive, patient-centered care” emerged in all eight included studies.37-44 It concerns the need for patients’ active participation in decisions about their care, which is essential for ensuring that their preferences and needs are respected, thereby guaranteeing truly personalized and humane care. This theme included four subthemes: fear of pain and suffering, patients need medical expertise but have other needs as well, continuities of care, the need to be involved in therapeutic decisions.
Fear of Pain and Suffering
The greatest fear expressed by patients was suffering caused by all the symptoms that the disease brings, especially pain, a disabling, stressful and influential symptom in people’s lives.37,42-44 This fear is so intense that it often overshadows the fear of death itself. Although patients try to modify their daily routines in response to symptoms, there is still a pervasive apprehension about a possible inability to control physical suffering, which may dominate their experiences and perspectives on illness.37,43 “The pain disturbed me and also made sleepless night. [...] The pain scared me. I have no fear for dying when I still suffered with the same pain. I thought that if I die soon, it better.”
44
Continuities of Care
One concern of patients related to symptom management is a lack of continuity of care, which generates bewilderment and a sense of abandonment. Indeed, a significant concern raised by the study participants was the limited availability of palliative care teams in rural areas, along with challenges accessing these services at night and on holidays.38,40,43,44 In studies by Melhem D. and Daneault S. and Richards S.H. et al, patients expressed concern about the intervention of professionals who were not familiar with their medical history during out-of-hour care or emergency department use.38,40 “I was kind of dreading it and I did think to myself, oh no, I am ringing on a Sunday, I don’t know what’s going to happen, am I going to have to wait around for hours? […]”
37
Patients Need Medical Expertise but Have other Needs as Well
Patients also prioritized the need for a health care team that not only excels in symptom management but also demonstrates other essential qualities, such as empathetic listening and the ability to forge a strong, personal connection with the patient.
40
“The approach with the patient—for sure it’s important. It’s maybe even a priority.”
40
The Need to be Involved in Therapeutic Decisions
Although palliative care is based on patient-centered care, some patients perceived little involvement in their treatment choices and complained that they did not receive sufficient information about their illness and actual condition.37,39,41,42 “The physician does not say everything. [...] I prefer the truth from the beginning of the road. It is much better.”
37
The Need for Maintaining a Sense of Autonomy and Dignity
The theme “the need for maintaining a sense of autonomy and dignity” was addressed by five out of eight studies,37,39,40,43,44 This theme highlights the crucial importance of supporting a sense of autonomy and dignity in palliative care. Preserving dignity at the end of life is fundamental due to the profound changes that illness imposes. This means supporting their aspiration to maintain a quality of life in line with their personal values and beliefs, rather than treating them with pity.
It included three subthemes: dislike of being nonproductive, lose control over life, and dislike for pity.
Dislike of Being Nonproductive
Patients perceive that the decline in performance, worsening of symptoms, and fatigue often limit their physical activity and ability to carry out daily tasks, thus requiring support from a family member. This need for help can lead to a sense of loss of their role within the family and a feeling of helplessness, both from a work perspective and a personal one.37,43 “[...] My life centres around this now. I’m like a little baby: I sleep, I eat and I go to the bathroom...”
42
Lose of Control Over Life
No longer having a position within society, being dependent on others, and being overwhelmed by the disease and the rhythms it dictates trigger a sense of loss of control over life, which is experienced as bewilderment and fear of how this path may evolve and how it will be managed.37,39–41,43 “Our roles have been reversed. I’m the one who’s doing less now, the one who’s less active, so [spouse] is taking the lead around here. […]”
42
Dislike for Pity
Loved ones try to be helpful in every way, but the caregiver’s closeness is often perceived as an attitude of pity that is not psychologically beneficial to the person who wants to feel like a normal, non-sick person.
37
“You feel people feel sorry for you. They pity you, ‘‘Poor lady’’, as if you have leprosy or something similar. I mean this is something that I have to face. I do not feel sorry about myself. When they pity me, and when they say ‘‘You look much better,’’ I feel that I am not normal—that I am different. They make me feel that I am handicapped.”
36
The Need for Attentive Support to patients’ Soul
This theme recurred throughout all the studies in this review.37–44 It concerns the importance of nurturing the inner, non-tangible aspects of a patient, providing comfort, peace, and a sense of wholeness even as they face life-limiting illnesses. This theme is identified in the following subthemes: need to pray to one’s own God, needs related to the search for meaning, patients need respect and validation of their experiences, and need of psychosocial support.
Need to Pray to One’s Own God
Spirituality can have a positive impact on coping with illness, particularly when patients try to accept their terminal situation. Some participants’ reliance and dependence on God helped them achieve a deeper and more positive perspective on life, giving it new meaning.37,39,43,44 “How long I can live, I don’t know. Everyday I pray […] I pray to Jesus, I pray to Buddha […] This is the only thing I can do. Other than that, what I can do? Just live day-to-day.”
38
Needs Related to the Search for Meaning
However, among the participants, there was a pervasive need to ascribe meaning to both life and death that transcended any specific religious belief. It highlights the intrinsic human inclination to find coherence and significance in the journey of life and the inevitability of death, regardless of one’s religious affiliations or lack thereof.39,43 “Sometimes I can’t believe what’s happening! Why me? There are so many questions that will never be answered. You can try to find them, but all this — life, death — it’s all so personal [...].”
42
Patients Need Respect and Validation of Their Experiences
Participants in the studies also voiced a strong need for health care professionals and caregivers to recognize and validate their experiences of suffering. This need reflects a desire for a compassionate approach, where patients’ feelings and struggles are acknowledged as legitimate and significant aspects of their care “But I wasn’t alone. I had my partner with me. I didn’t necessarily need to talk. Sometimes, there’s nothing to say.”
40
Need for Psychosocial Support
Patients expressed a deep need for reassurance and opportunities to openly discuss their emotions, not only with family members and caregivers, but also with others who were going through similar experiences. The opportunity to share and voice their feelings in a supportive environment is invaluable in creating a network of support, helping patients navigate their emotional landscape, understanding their feelings, and reducing the sense of isolation and fear associated with their condition.37,38,40,41,43,44 “Talking extensively about anxiety helps, but it cannot take all the anxiety away.”
40
The Need for Accessible and Timely Care
This theme was addressed by six out of eight studies,38,39,41–44 It highlights how this approach to palliative care is grounded in creating a supportive, informed and timely care pathway for patients and their loved ones and includes four subthemes: legitimacy of seeking help, time of care, type of unmet information needs, and financial support.
Legitimacy of Seeking Help
As shown in the study by Richards SH. et al patients often grapple with feelings of uncertainty about the legitimacy of seeking help, especially because they may doubt the meaning or validity of their needs. Such uncertainty can lead to a reluctance to express their real needs for fear that they may be perceived as minor or irrelevant.
38
“…night times it’s ten times worse, you know. (…) you are very vulnerable. You don’t want to phone the doctor just to chat, that’s for sure.”
38
Time of Care
Wang et al.’s study revealed that participants occasionally expressed dissatisfaction with the amount of time health professionals allocate to their care. They often perceive these professionals as overly occupied or feel that the professionals do not regard their concerns as significant enough to warrant more time and attention.
42
“Doctors are too busy to talk with us. You know, there are so many patients that the doctors cannot detail everything to us. The doctors can only tell us the most important things, like the condition of the disease.”
42
Types of Unmet Information Needs
Several studies have highlighted a gap in meeting patients’ information needs. Often, patients find themselves lacking essential information about various critical aspects of their condition and care. Key areas where patients frequently feel uninformed include the nature and progression of their disease, the prognosis, life expectancy, the expected trajectory toward the end of life, and details about available treatments and their implications.41-44 “I really need to know what is going to happen, not that you can always count on it because things are changing, but information takes away a lot of uncertainty and as a consequence I am feeling less anxious.”
40
Financial Support
During this critical phase, financial concerns become increasingly significant. The substantial burden of medical bills, medication costs, and potential loss of income adds complexity to a challenging period. Patients often struggle with the inability to manage their finances due to their illness, making the shift from financial independence to reliance on others particularly difficult.39,44 “I can’t afford this kind of money […].”
39
Discussion
In this review, we performed a meta-ethnographic synthesis of the literature to explore unmet needs in the context of palliative cancer care among the adult population. This methodology has allowed us to generate a broader explanation and understanding of the phenomenon. 20 Our main findings illustrate several needs that health professionals should pay attention to from the perspective of patients experiencing the disease. These needs are affected by cultural contexts, health systems and economic conditions, as stated by Wang et al. 17
Four third-order themes emerged from an in-depth analysis and reinterpretation of the eight studies included in this review: the need for comprehensive, patient-centered care, the need for maintaining a sense of autonomy and dignity, the need for attentive support to patients’ soul and the need for accessible and timely care.
The need for comprehensive, patient-centered care is closely linked to the primary goals of end-of-life care, which include symptom management and improving quality of life.4,5 The aim is to provide people with terminal illnesses the best possible remaining life and to help them accept coexistence with an unwelcome guest, hopefully making it as unobtrusive as possible. Indeed, the fear of experiencing increasing pain as the illness progresses and death approaches remain a tangible concern despite the numerous available symptomatic therapies. This concern sometimes exceeds the concern about death itself, or patients may ask for a quick end to their life to avoid additional suffering.37,42–44
This heightened sense of vulnerability at the end of life, as highlighted by Melhem D. and Daneault S., leads to hesitations and uncertainties, creating a demand for enhanced security. This security involves not only ensuring a journey free from suffering but also having a health care team that recognizes and respects patients as individuals with unique needs, beyond just professional medical care. 40 The participants in the studies expressed a clear desire for professionals to be close to them as individuals, not solely as experts, as they seek deeper answers and greater reassurance beyond the realms of medicine and science. 40
However, challenges arise especially when patients seek these compassionate services outside regular hours. Studies have shown that they often face challenges in receiving adequate responses, particularly when they encounter professionals who are unfamiliar with their cases.38,40,43,44 This issue is prevalent in emergency departments where professionals may not have the time to dedicate to thorough assessments of their needs. 40 This lack of personalized attention can hinder the provision of effective patient-centered care.
While patient involvement in decision-making is a fundamental goal of palliative care, findings from the included studies reveal that this objective often remains unfulfilled. Patients frequently feel sidelined from making therapeutic choices and report a lack of adequate information about their medical conditions, indicating a gap between the ideals of palliative care and the actual experiences of patients. 42
The need to maintain a sense of autonomy and dignity is deeply intertwined with how individuals perceive and experience dignity, especially in the face of illness. Indeed, dignity is a personal and fluid concept, shaped uniquely by each person’s experiences. Being forced to ask for help, sometimes even without speaking because the body, with its fatigue and suffering, speaks for itself, is costly for those who are used to being autonomous and free from dependency on others, as stated by Wang T. et al and previous studies.16,18,42 The eyes of the beholder, while communicating love and sorrow, are seen as the mirror of one’s condition, terminality and end. Feeling pitied because of the physical limitations produced by illness is what patients want least; they want to continue to be seen as they have always been. The struggle to balance the desire for normalcy with the realities of their condition reflects the deep need for stability and continuity amidst life’s uncertainties.
Attentive support to patients’ soul therefore becomes crucial, especially when studies reveal that patients often feel that their souls are threatened by the upheaval of an end-of-life diagnosis and the fear of venturing into unknown territory. This situation underscores the necessity of nurturing the well-being of individuals’ souls, who face the daunting challenge of losing their sense of identity amidst their illness.37-44 When life requires new perspectives, sometimes very brief, or readjusted to a new truth, everything is transformed. This gives rise to the need to attribute meaning to one’s life and to the death that is to come even though there is no rational explanation for suffering.39,43 Sometimes, a prayer addressed to a deity above them, who has mapped out a precise path for their journey on Earth gives meaning to patients’ lives, as reported in several studies.37,39,43,44 For those who cannot find an explanation, all that remains is to resign themselves to an unstoppable descent. Interacting with people who are going through a similar process can sometimes help patients face their anxieties and fears by finding support in closeness and communication with fellow patients and their families and helping them to not feel alone.37,41,44 This sense of community and mutual understanding reinforce the importance of acknowledging and validating each patient’s unique experiences and preferences, particularly concerning their end-of-life journey.38,41
However, the need to share suffering is often underestimated by patients because of the uncertainty of the relevance of their needs. From this, the need emerges to legitimize their suffering and seeking help, giving it space through confrontation and approval by loved ones and health professionals. 38 According to the literature, many patients hesitate to share their concerns with health care providers because they often believe that suffering is inevitable with cancer or that effective treatments are unavailable, leading to the neglect the importance of their unmet needs. 12
Additionally, time constraints are perceived as an unmet need even during scheduled visits as the moments of care allocated are restricted to addressing immediate concerns only, leaving aside aspects such as personalized information on the disease, prognosis, life expectancy and trajectory to death.41,42 End-of-life care requires more time to consider the submerged aspects of terminality and to ensure that patients feel fully supported and understood. Even some professionals who participated in the study of McCarthy SA et al, highlighted that the limited time allocated to these patients hinders the identification of psychosocial and emotional needs. 39
Limitations
The heterogeneity of the studies, especially in terms of their geographical origin and qualitative nature, limits the ability to generalize findings. This limitation is further exacerbated by the absence of studies published in major countries, including the USA, suggesting a gap in the research landscape. In addition, there is a large discrepancy in the years of publication (from 2007 to 2023), which is also a limitation because palliative care has evolved over time in terms of policy geared toward improving infrastructure and service delivery. Furthermore, the qualitative assessment of the methodology of the included studies revealed that the data analysis was not rigorous in all the studies.
Conclusion
Unmet needs in many areas of palliative care have a direct impact on the quality of care people receive and thus on their quality of life. The guarantee of a safe end-of-life pathway that is free of suffering and accompanied by decision-making awareness and team understanding appears to be an essential need for patients. The needs for continuity of care, the validation of one’s suffering, and appropriate care time require prioritized and responsible attention from health care providers within the context of palliative care. This entails ensuring a consistent care plan over time, recognizing and respecting patients’ experiences and emotions, and dedicating the necessary time to provide comprehensive and personalized care that accounts for each patient’s individual needs. The included studies represent the realities of different countries worldwide, where the health services and experiences of palliative care teams are certainly different. For this reason, more studies should investigate these needs in greater depth in each country.
Supplemental Material
Supplemental Material - The Perspective of Cancer Patients in Palliative Care on Unmet Needs: A Qualitative Synthesis Using Meta-Ethnography
Supplemental Material for The Perspective of Cancer Patients in Palliative Care on Unmet Needs: A Qualitative Synthesis Using Meta-Ethnography by Ilaria Basile, Letteria Consolo, Daniele Rusconi, Laura Arba, Flavia Rampichini, Augusto Caraceni, and Maura Lusignani in American Journal of Hospice and Palliative Medicine®.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.