
Abstract
Introduction
Family caregivers play an essential role in the direct care and support of patients with cancer. 1 The importance of family caregivers is increasing with a shift to outpatient treatment and home-based care. 1 The guidelines for family support in palliative care highlight the importance of support as an indicator. 2 Studies have also focused on the burden of caregiving tasks. 1 Previous research has been conducted on the caregiver burden for various cancer types.3,4
Caregiver burden is a subjective appraisal among family caregivers and is defined as the caregiver’s perceived physical, emotional, social, and financial hardships as a result of caring for their relatives. 5 While considerable research has been conducted in the area of caregiving for older adults, in recent years, there has been an increase in research on caregiver burden among caregivers of patients terminally ill with cancer, including patients with cancer. 6 A study of caregivers of patients with pancreatic cancer noted that burden is an important predictor of mental illness. 4 Moreover, the higher caregiver burden in family caregivers of older adults with cancer calls for target interventions to reduce adverse health outcomes related to caregiver burden. 7 Research on caregiver burden among caregivers of patients with solid tumor cancer demonstrated inconsistent intervention effects. 8 While most studies focus on caregiver burden in family members of patients with cancer, few have focused on terminal cancer.
Educational interventions provided by nurses are called nursing interventions or nursing support. In providing nursing support to patients, nurses should use the current evidence in conjunction with clinical experience and patient values. 9 Therefore, providing families of patients with effective nursing support is a high priority. However, in the case of caregiver burden in family caregivers of patients with cancer, including terminal cancer, nursing support is frequently provided based on patient value and nurses’ clinical experience since sufficient evidence has not been accumulated. More effective palliation of caregiver burden in family caregivers of patients terminally ill with cancer requires evidence-based support in addition to nurses’ clinical experience. This need requires a broad, comprehensive review of research on nursing support for caregiver burden in family caregivers of patients with cancer. There is a gap between clinical practice and research evidence. To bridge this gap, this comprehensive scoping review summarizes relevant research regarding patients with cancer across all stages and a variety of research designs. 10
This scoping review comprehensively explores the nursing support provided to reduce caregiver burden among family caregivers of patients with cancer. The current results are expected to be used to understand the actual state of nursing support provided to family caregivers of patients terminally ill with cancer in the future, as well as to examine possible support that can be implemented.
Materials and Methods
Methods
We conducted a scoping review to comprehensively explore and map the nursing support provided to reduce caregiver burden in family caregivers of patients with cancer. We applied a standard framework proposed by Arksey and O’Malley11,12 and expanded by the Joanna Briggs Institute. 13 We followed reporting guidelines described in the Preferred Reporting Items for Systematic Reviews and Meta-analyses Statement (PRISMA) extension for PRISMA Scoping Reviews. 14 The scoping review protocol was published prospectively. 10 Nursing support was defined in the protocol paper, implying that we defined nursing support as support that nurses can implement. In addition, we determined through discussions among the researchers whether nurses could implement each support extracted. This review did not require ethical approval because it is a secondary analysis of pre-existing, published data.
Identifying the Research Question
The research question was “What types of nursing support are provided to reduce caregiver burden in family caregivers of patients with cancer?”
Identifying Relevant Studies
We searched PubMed, CINAHL, Cochrane Central Register of Controlled Trials in the Cochrane Library, and Ichushi-Web of the Japan Medical Abstract Society databases from each database’s inception to July 31, 2023. We also assessed the relevant studies from the article list and manually searched through key journals. Search formulas were first created in PubMed as an initial search. Subsequently, search formulas were created to match other databases (see the protocol paper 14 for details of the search formula). KK and KM completed this initial search in consultation with the librarian.
Eligibility criteria were determined by physicians and nurses specializing in caregiver burden in family caregivers of patients with cancer (details are described in the protocol paper 14 ). We identified studies using the Patient–Intervention–Comparison–Outcome model. The inclusion criteria were (1) caregivers of patients with cancer aged 18 years or older, (2) intervention studies for the relief of caregiver burden or outcomes similar to caregiver burden, (3) nursing support including multidisciplinary support, and (4) quantitative data showing an outcome. We excluded papers wherein more than 20% of the participants were patients without cancer, papers with secondary analyses, and papers in languages other than Japanese and English.
Study Selection Process
The first screening included an independent assessment of the title and abstracts of all studies by 2 reviewers (KK and MK), followed by second screening and full-text screening against eligibility criteria. Any discrepancies in study selection were resolved by discussion between the reviewers. The study selection process is summarized in Figure 1. Flow diagram of the scoping review process.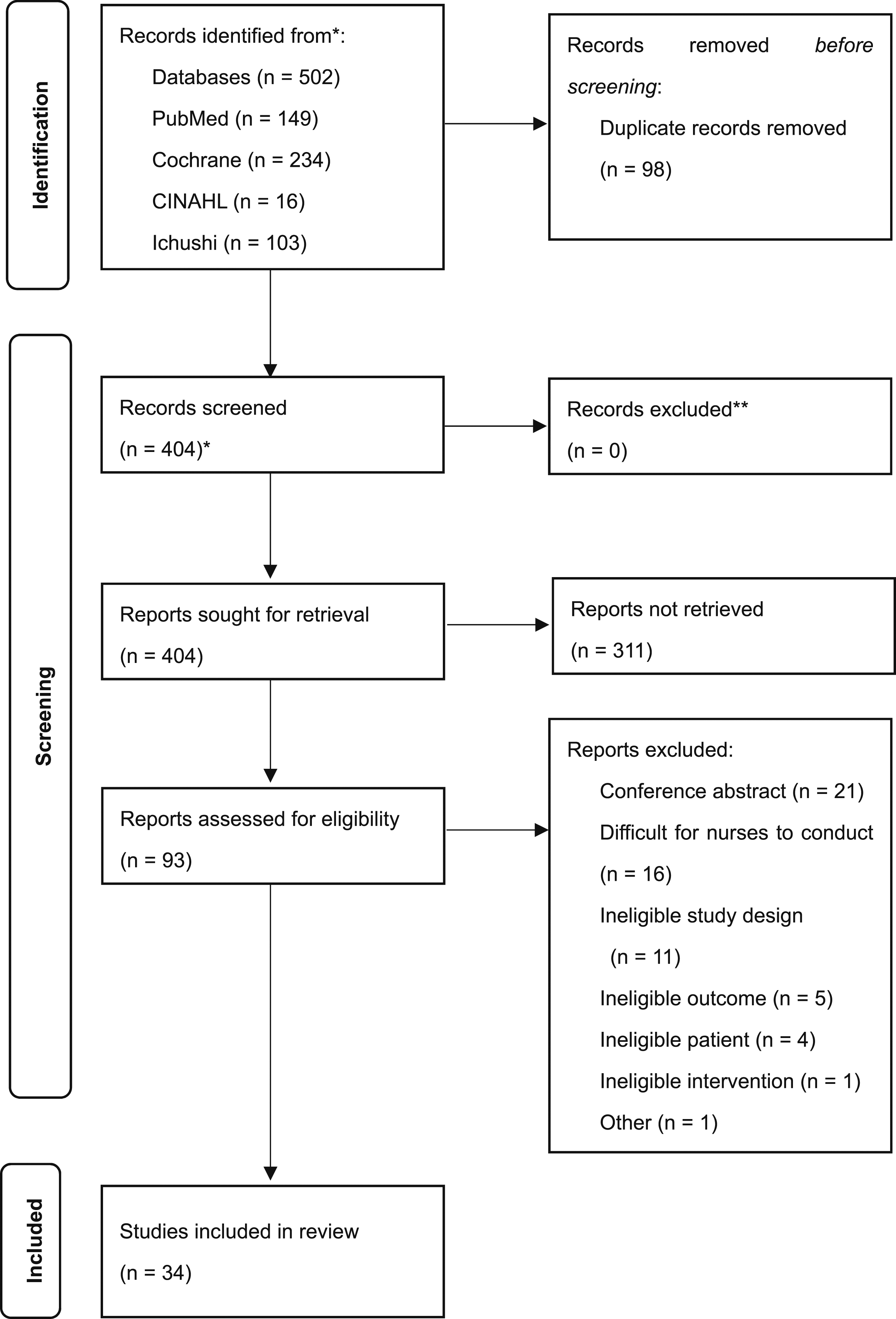
Charting the Data
A form was created to extract study characteristics, including first author, publication year, country of publication, study design, aims, sample size, type of nursing support, provider, and results of the interventions for caregiver burden. Data were extracted independently by the same 2 reviewers. Studies were excluded at this phase if they did not meet the eligibility criteria.
Collating, Summarizing, and Reporting the Results
The nursing support provided in the studies extracted from the literature review was categorized by care component using qualitative thematic analysis. In the analysis, the classification by 1 author (KK) was checked by another author (MK), followed by the study group to verify validity. We categorized the components of nursing support according to whether they were primarily nursing support or whether nurses were included in the support provided by multidisciplinary professionals.
Results
Figure 1 shows the literature screening process and results. We identified 502 studies based on eligibility criteria. After removing 98 duplicates, we screened the titles and abstracts of 404 studies and excluded 311 studies. In addition, we assessed 93 full-text studies for eligibility and excluded 55 for the following reasons: conference abstract (n = 21), difficult for nurses to conduct (n = 16), ineligible study design (n = 11), ineligible outcome (n = 5), ineligible patient (n = 4), ineligible intervention (n = 1), and others (n = 1).
Characteristics of the Included Studies (N = 34).
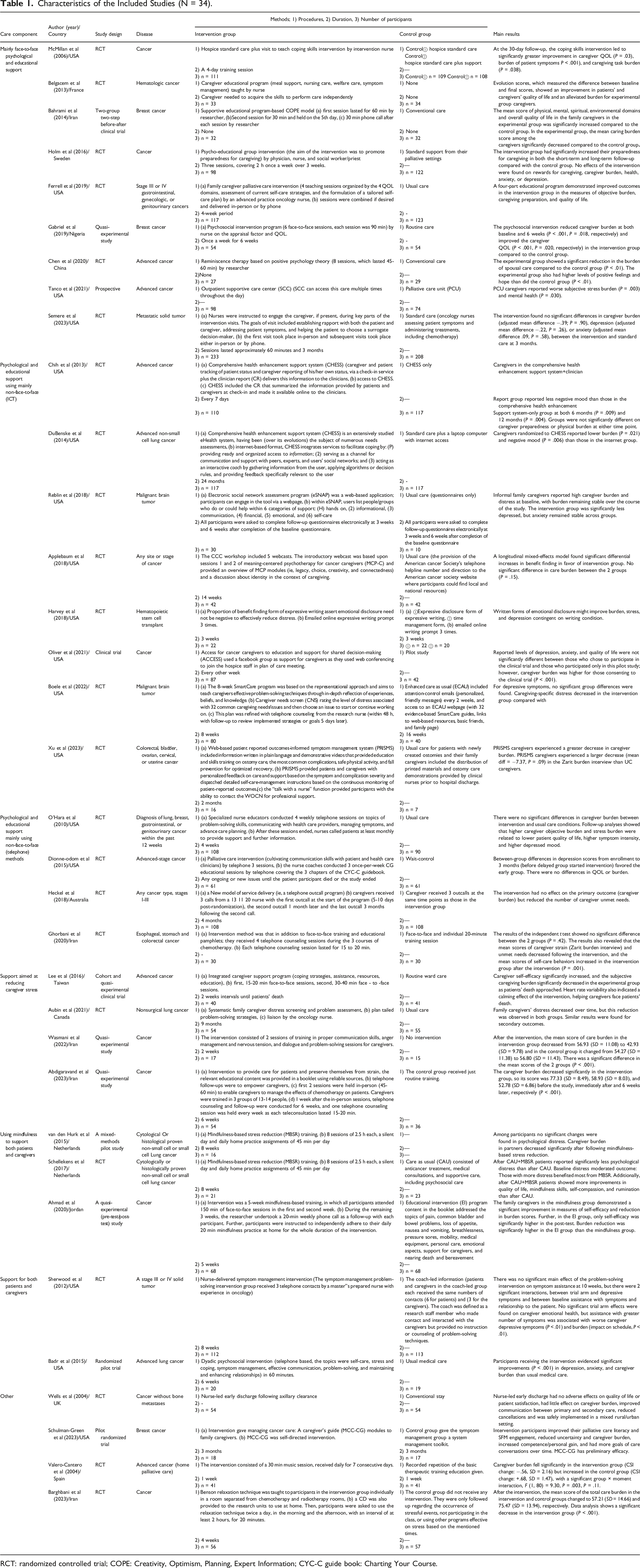
RCT: randomized controlled trial; COPE: Creativity, Optimism, Planning, Expert Information; CYC-C guide book: Charting Your Course.
Discussion
Our research question was to identify the nursing support provided to reduce caregiver burden in family caregivers of patients with cancer. While most previous studies focused on the burden of caregiving for a specific cancer type, this study shows the caregiver burden for cancer in general. We categorized the 34 included studies into 7 components of nursing support. The most commonly classified nursing support groups were educational programs, family caregiver palliative care interventions, and psychosocial intervention programs, and most of the components included family caregivers of terminally ill patients with cancer. Nearly 70% of the studies were RCTs. Educational psychological interventions showed variability in effectiveness. ICT-based psycho-educational interventions also showed positive results.
Nurses were the primary intervention support in 13 studies, which also included specialist oncology nurses.15,16,19,20,23,30,32-34,37,38,43,45 Multidisciplinary collaboration existed between nurses, physicians, social workers, health professionals, and supportive care teams. Interventions for caregiver burden included those that were implemented not only by nurses but also through multidisciplinary collaboration. In our results, nursing support for caregiver burden was mainly face-to-face psychological and educational support provided by a nurse, including teaching coping and caregiving skills, and establishing self-care plans. Similarly, we identified psychological and educational support mainly using telephone methods provided by nurses, including support using problem-solving skills and providing support information. A previous study reported the types of interventions based on intervention components. 49 The authors categorized similar interventions as educational programs, a web-based program, and a telephone support service outcall program, among others. 49 Other studies labeled the intervention as face-to-face or via telephone. 50 These components were similar to those of nursing supports identified in our study. Face-to-face and non-face-to-face implementation could differ in terms of their effects on the caregiver burden. Therefore, we categorized the intervention type accordingly.
Psychological and educational interventions using ICT were mainly conducted through multidisciplinary methods and included those conducted by caregivers themselves using the Internet. Psychological and educational interventions were characterized as including both nurse-led and multidisciplinary interventions. Psycho-educational interventions have been mainly face-to-face or telephone-based, but recently, ICT-based interventions have been increasingly used.24-31 ICT-based interventions are highly versatile as they can be used anywhere and at any time. In addition, many studies were RCTs, which varied in terms of their effects on caregiver burden. In a systematic review limited to Internet-based supportive interventions for caregivers of persons with dementia, all 17 applicable studies were RCTs, and 10 studies used outcomes related to caregiver burden. 51 However, most studies used multidisciplinary interventions. In addition, Internet-based support in dementia caregiving is effective in treating depressive symptoms, perceived stress, anxiety, and self-efficacy. 51 Therefore, we believe that family caregivers of patients with cancer are likely to be studied using Internet-based strategies in the future.
Face-to-face based interventions often included nurses as interveners, and the intervention periods varied. Telephone-based intervention were those that the nurses were implementing in addition to their usual care. Most interventions included counseling sessions. Although we believe that telephone-based assistance can be used as standard support, no effective trend was demonstrated in this study. Support aimed at reducing caregiver stress was mainly conducted by nurses, and the content was diverse, including approaches to caregiver screening assessments and problem-solving skills. Using mindfulness to support was a commonly employed mindfulness-based stress reduction (MBSR) methodology.
A previous study of informal caregivers for people living with cancer indicated that there were not any clearly identifiable patterns in the effects of interventions based on the delivery format. 52 It is necessary to examine not only whether an intervention works but also how it is implemented, its causal mechanisms, and how its effects vary by context.53,54 The frequency and duration of an intervention vary across studies, and whether frequency and duration lead to reduced caregiving burden needs to be clarified in future studies.
In 1 out of 7 components of nursing support, no research has been reported for patients terminally ill with cancer. Caregiver burden is not directly invasive to the patient because the target is a family caregiver; thus, there is no difference in intervention content depending on the stage of the cancer. As such, studies on nursing support for caregiver burden in caregivers of patients with advanced cancer could be applicable to family caregivers of patients terminally ill with cancer. Accumulation of evidence in nursing support for these caregivers is expected in the future.
This scoping review has some limitations. First, the search was limited to studies published in Japanese and English, and this review could have excluded relevant articles published in other languages. Second, this scoping review was not designed to assess methodological quality. Therefore, the conclusion is based on the extraction of nursing support being provided rather than on the effectiveness of nursing support for caregiver burden. Third, the search was limited to studies in which at least 80% of the participants were patients with cancer; thus, studies conducted primarily on caregiver burden in family caregivers of patients without cancer were not included. Further, because of the wide range of cancer stages included, it is impossible to determine the effects on disease characteristics, and so on. Fourth, caregiver burden was not operationally defined to distinguish between subjective and objective caregiver burden.
Conclusion
This scoping review categorized nursing support for caregiver burden in family caregivers of patients with cancer into 7 components. Future research should examine the feasibility of implementing these nursing support categories for caregiver burden in family caregivers of patients with cancer with a prognosis of months or weeks and should explore effective prognosis-based nursing support components.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the JSPS KAKENHI [grant number 21H03236]. This study received guidance from the National Center Consortium in Implementation Science for Health Equity (N-EQUITY) funded by the Japan Health Research Promotion Bureau (JH) Research Fund (2019-(1)-4) and JH Project fund (JHP2022-J-02).
Authorship Statement
All authors (Kohei Kajiwara, Masamitsu Kobayashi, Miharu Morikawa, Yusuke Kanno, Kimiko Nakano, Yoshinobu Matsuda, Yoichi Shimizu, Taichi Shimazu, Jun Kako) contributed to the preparation, drafting, and editing of this scoping review. Kohei Kajiwara and Masamitsu Kobayashi conceived the idea for this research, followed by discussions with the other authors (Miharu Morikawa, Yusuke Kanno, Kimiko Nakano, Yoshinobu Matsuda, Yoichi Shimizu, Taichi Shimazu, and Jun Kako), contributing to the finalizing of the research idea. Kohei Kajiwara and Masamitsu Kobayashi developed the data extraction tool and the systematic database search strategy in consultation with the specialist librarian at YCU. All authors contributed to the preparation and editing of the manuscript and read and approved the final version of this manuscript.