
Abstract
Introduction
The place of death is an important quality aspect of end-of-life care. 1 The needs of terminally ill patients differ, and therefore the preferred place of death of patients and the reasons behind these preferences may vary. Previous studies, as well as a systematic review of the subject, 2 have shown that most cancer patients prefer to die at home rather than at a hospital to spend their last time in a familiar environment.3-5 There are also indications that dying at home is associated with a better death for most patients. 6 In 1 study comparing places of death in different countries, there was a median of 54% of hospital deaths and 18% of deaths in residential aged care facilities. 7 Also, the proportion of hospital deaths varied considerably between different countries which may be due to cultural reasons as well as differences in health care systems in different countries.7,8 Death certificate data from all deaths in 2002 in Sweden showed that 85% of all cancer deaths occurred in a hospital. 9 In a more recent population-based study based on death certificate data from all deceased patients in Sweden in 2012, 42% of all deaths occurred in hospitals, 18% occurred at home and 38% in nursing home facilities, suggesting a trend over time in Sweden of decreasing likelihood of hospital death. 10 However, the opposite trend has also been observed in other countries. 11 There are patients who prefer to die at a hospital or a nursing home because of hope of receiving treatment or to reduce the burden of care of their family. 12 Also, limitations regarding level of care and complex symptom control makes end-of-life care at home unsuitable for some patients. Therefore, it may be inappropriate to assume that all end-of-life care should be organized in a home setting and the preferences and needs of the patient should always be considered. However little research has been conducted regarding preferred vs actual place of death in cancer patients and the factors that influence these variables. In 1 retrospective study investigating patients admitted to advanced medical home care in Stockholm, Sweden, it was shown that of the patients who expressed a preferred place of death, 75% wanted to die at home and 80% had their wishes fulfilled. 13 In this study, the wish to die at home was the only factor significantly influencing the place of death. Other studies, from different countries and time periods, have shown a congruence between preferred and actual place of death of 31%–73%,14-21 suggesting significant variations between different populations. In these studies, various other factors that the patient’s preferences have been significantly associated with the actual place of death. To improve the quality of end-of-life care, it is important that patients are able to die in their preferred locations and that health care workers help patients to achieve this. The aim of this prospective trial was to investigate the preferred and the actual place of death of palliative cancer patients and to assess the impact of various socio-demographic factors on these variables.
Methods
Setting
Palliative home-care teams in Sweden are organized in different ways in different parts of the country depending on regional preconditions. They have in common that they offer hospital-like care at home, including visits of nurses, palliative care physicians and paramedics with the aim to provide good palliative care to patients in their own home, to avoid hospital admissions and to make it possible for the patient to live at home for as long as possible during the end of life. Usually, only patients with symptoms that require specialized palliative care are enrolled in a palliative home-care team but the practice varies between different regions. Patients who need health care services or nursing care at home but who do not need specialized palliative care can receive help from municipal home care (Sw: hemsjukvård). Furthermore, municipal domestic service (Sw: hemtjänst), offering non-medical care, is accessible to all elderly and disabled in Sweden for a subsidized fee.
This study was conducted in the Swedish municipalities of Gävle, Bollnäs and Avesta. Together they have a population of 153,000 inhabitants which makes up about 1.5% of the total population in Sweden. Each of the municipalities has a central city with the same name as the municipality in which a majority of the population lives. However, there is also a sizable rural population in each municipality. Each of these 3 municipalities has its own palliative home care team which resides in the central city.
Data collection
Patients aged 18 years or above diagnosed with cancer in a palliative setting who were enrolled in a palliative home-care team in the Swedish municipalities of Gävle, Bollnäs and Avesta between 2019 and 2022 were asked to participate in the study.
Exclusion criteria were cognitive impairment, or any co-morbidity or communication issue that obstructed the ability to fill in a questionnaire according to a medical assessment by the study staff.
Patients who gave their written consent to participate were given a questionnaire (Supplemental Table 1) which consisted of 5 multiple choice questions regarding preferred place of death and whether this decision was made by the patient alone or together with relatives, marital status, need of domestic service or health care at home and need of assistance from relatives. The questionnaire was completed either by the patient or by health care personnel together with the patient. Also, demographic data regarding age and sex and type of cancer were collected for all patients at the time of inclusion. The place of death was recorded for all the patients in the study who died before the last follow up date of 5-May-2023. Ethical approval was received on 8-Nov-2017 from The Swedish Ethical Review Authority (Dnr 2017/271).
Statistical analysis
Patients’ characteristics were presented with descriptive statistics where categorical variables were presented as absolute numbers and percentages. In a next step, preferred place of death, and actual place of death was described by patient characteristics and statistically tested using the Chi-square test (and fisher’s exact test if the expected numbers were less than 5). In a subsequent step, the comparison of preferred and actual place of death was testing using the Chi-Square test (or Fishers exact test). All tests were 2-sided and statistical significance was considered with a P-value less than 5%. The statistical analyses were performed using R version 4.2.2. (R basis for statistical calculation, Vienna University of Economics and Business, Vienna, Austria).
Results
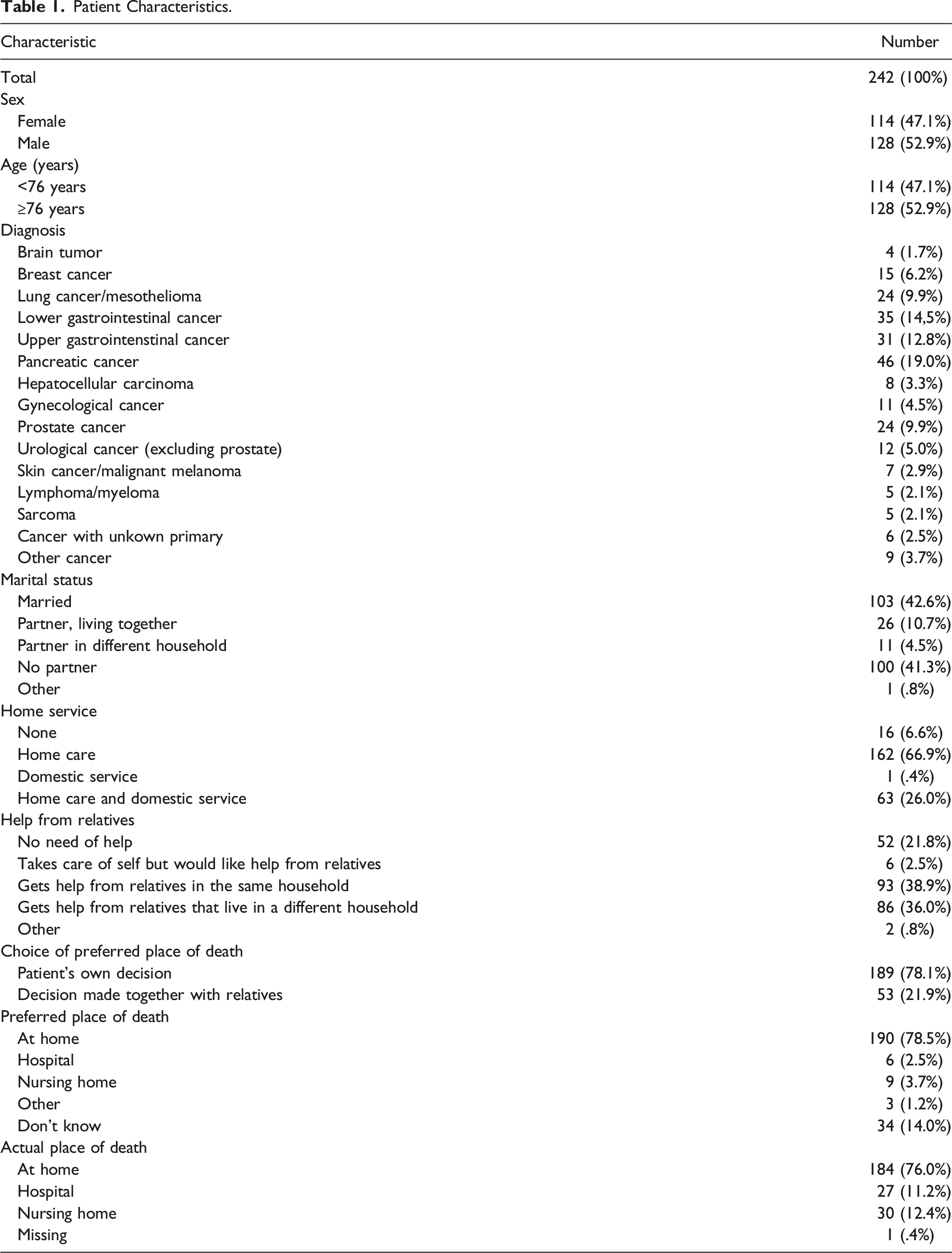
Patient Characteristics.
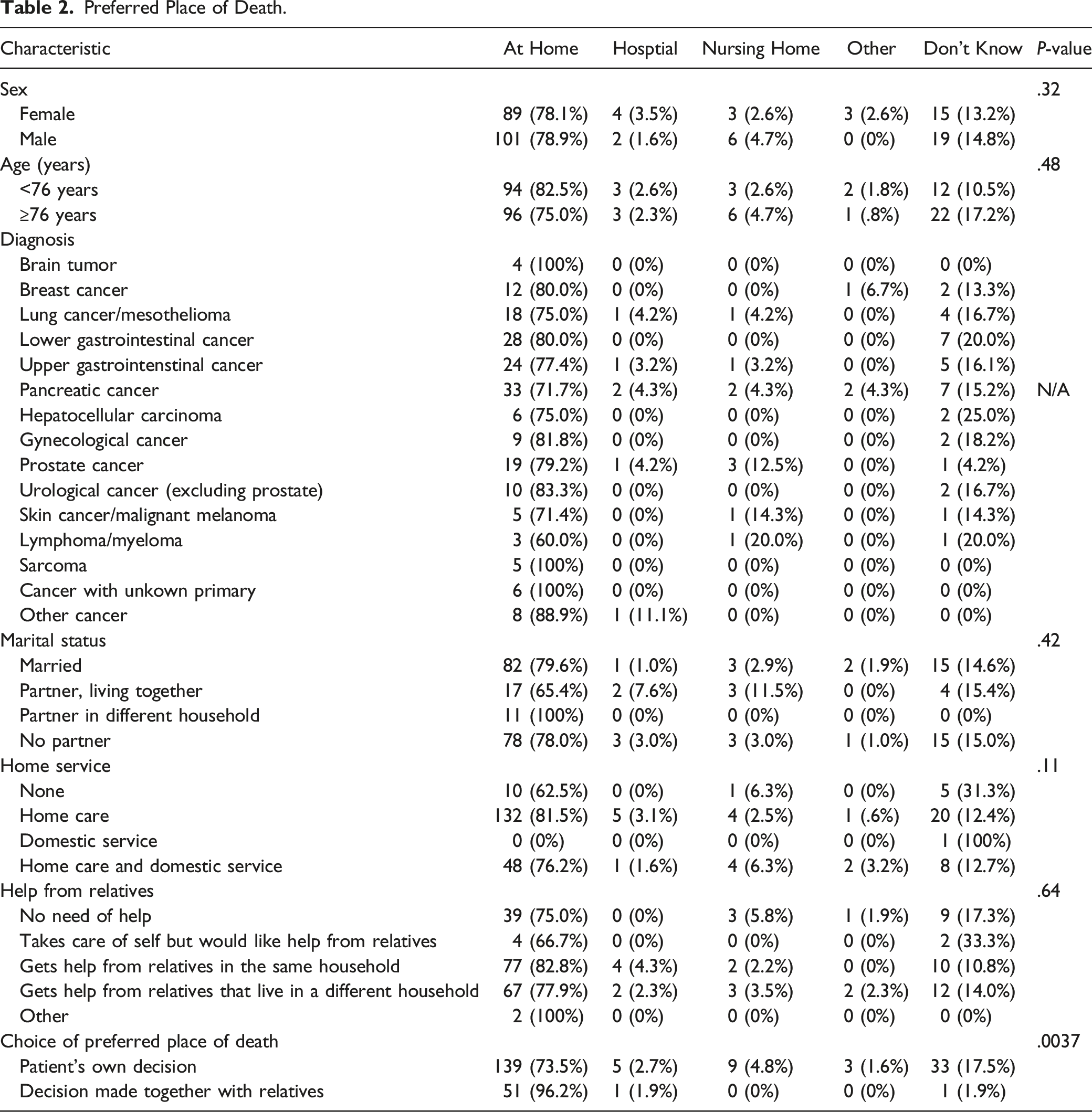
Preferred Place of Death.
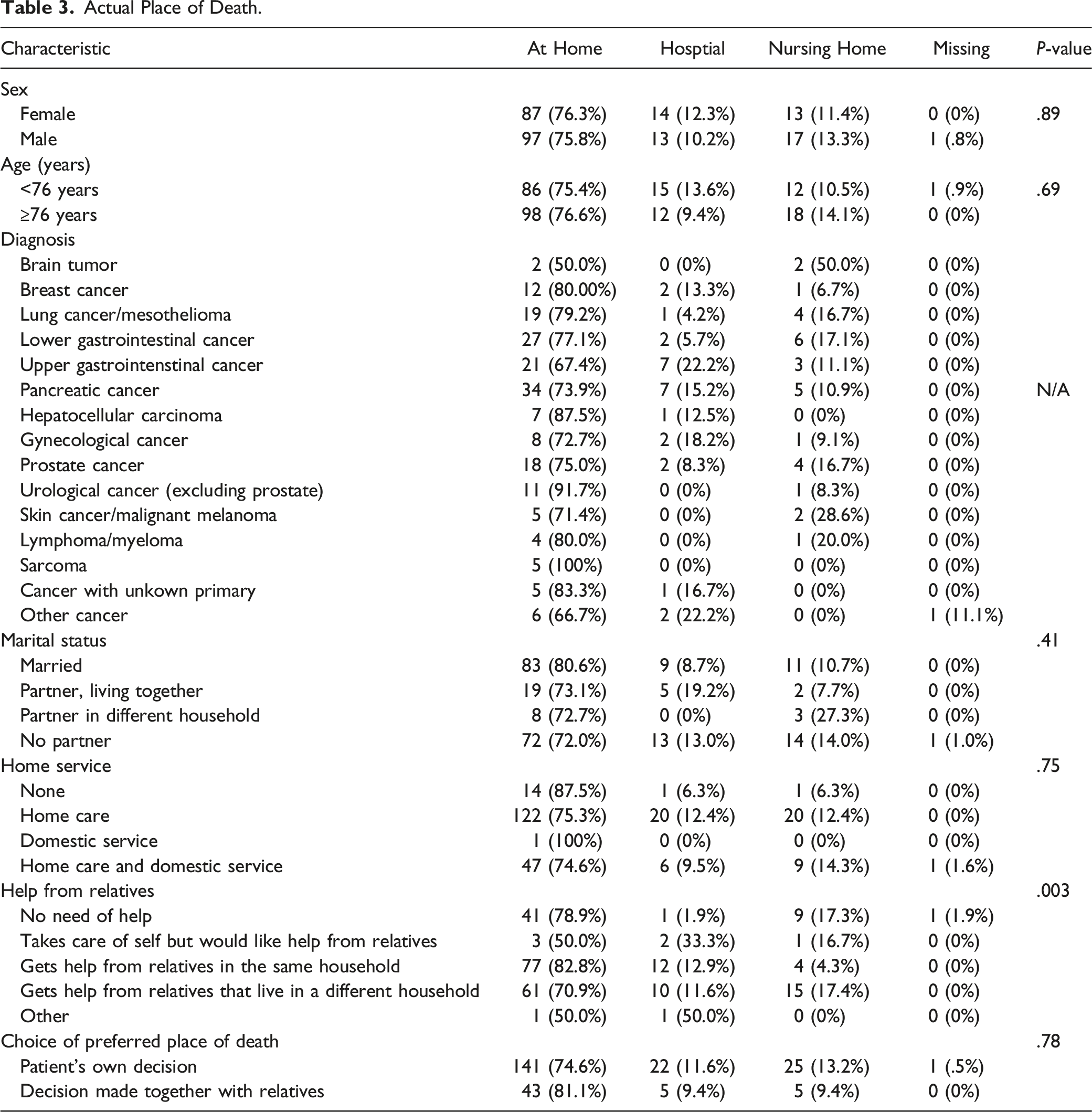
Actual Place of Death.
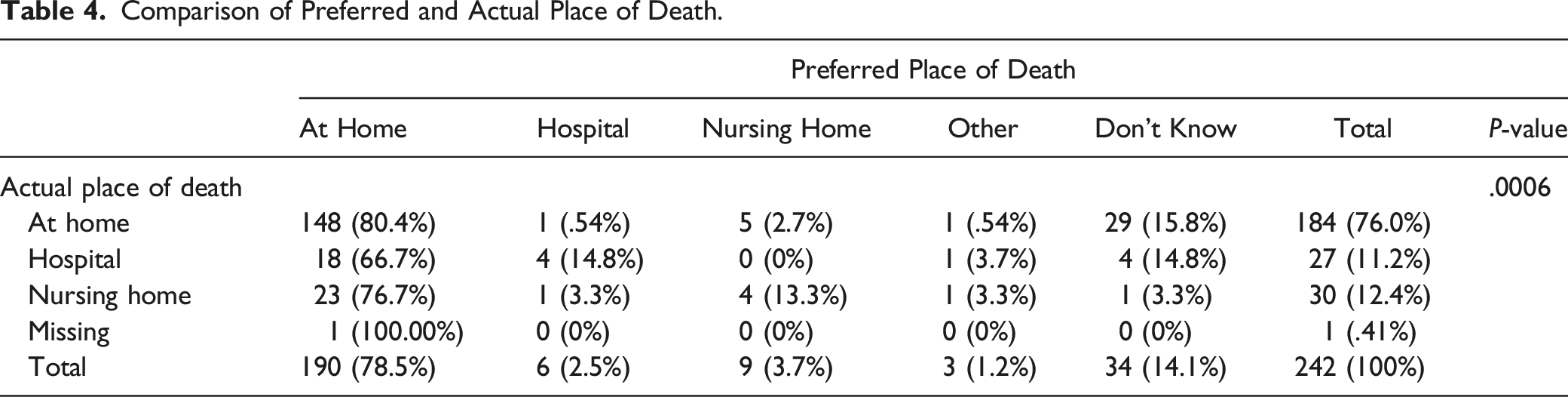
Comparison of Preferred and Actual Place of Death.
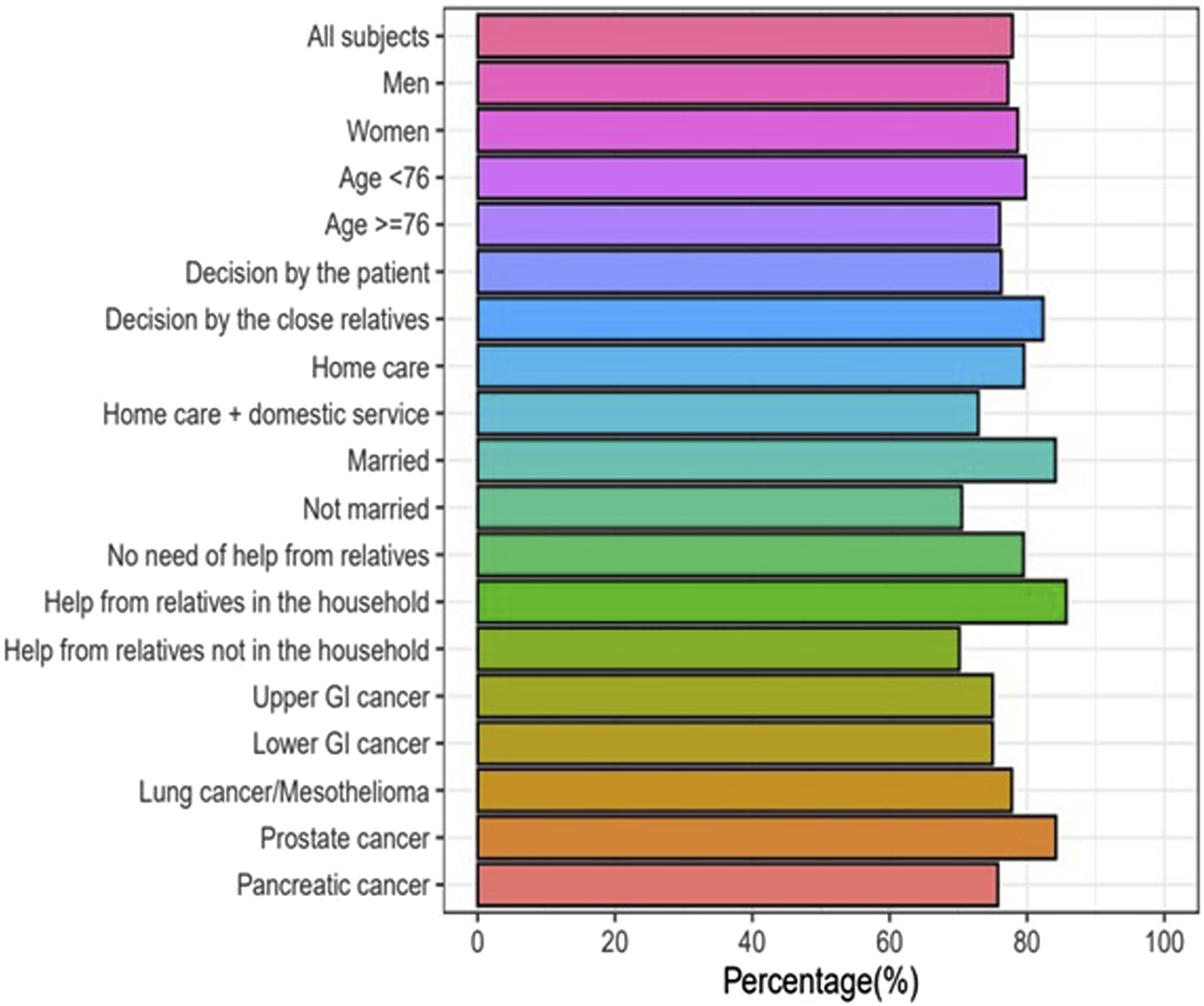
Percentage of home deaths of patients wanting to die at home in different subgroups.
Discussion
In this prospective study of palliative cancer patients enrolled in a palliative home-care team setting in the Swedish municipalities of Gävle, Bollnäs and Avesta, we have shown that most of the patients (79%) wanted to die at home. Furthermore, most patients actually died at home (76%) whereas the percentage of patients who died at a hospital or a nursing home was much lower (23%).
Of the patients who wanted to die at home, 80% actually died at home. Very few patients in our study wanted to die at a hospital or a nursing home and in the end only about 1 10th of the patients actually died at a hospital or a nursing home. However, due to the low number of patients in these groups it is hard to draw any certain conclusions from these data. A minority of the patients (14%) did not know where they wanted to die and of these patients most (85%) died at home.
The proportion of patients who wanted to die at home was similar across different subgroups, however when the decision was made together with relatives, the proportion of patients who wanted to die at home was significantly higher (96%) as compared to when the decision was made by the patient alone (75%). The reason for this is unclear but could be due to that the patients who make their decision regarding place of death together with relatives have a higher confidence that they will get the support necessary to be able to spend their last days at home. However, when looking at the actual place of death, there was no significant difference in the frequency of home death between patients who made their decision together with relatives as compared to when the decision was made by the patient alone. Neither did the other investigated factors (sex, age, marital status, type of tumor, assistance from relatives or health care at home) affect the likelihood of home death. Of note in our study was that all brain tumor patients wished to die at home, however the wish was only realized in 2 out of 4 patients. However, the small number of patients makes this finding hard to interpret. Results from previous studies suggest that several factors influence the place of death in cancer patients. In a systematic review from 2006 including 58 studies with over 1.5 million cancer patients from 13 different countries it was found that 6 factors were strongly associated with home death; low functional status, patient preferences, home care, the intensity of home care, living with relatives and extended family support. 22 Other factors associated with place of death has been proposed in recently published studies including marital status, the primary caregiver’s relationship with the patient and pain score.19,20
This study provides unique insights as it is to our knowledge the first study of Swedish cancer patients that has examined the preferences and actual death place of patients in a prospective manner. The percentage of patients who died at home is, by international comparison, high and an indicator of high quality of end-of-life care. In a multi-national comparison of places of death including 21 countries, there was a median of 54% of hospital deaths and 18% of deaths in residential aged care facilities. 7 Also, there were large variations between different countries with 78% hospital deaths in a Japanese population as compared with 11% in an Albanian population. In another multi-national study, the percentage of cancer deaths occurring at home in several Western European countries during the years 2002-2003 ranged from 12.8% in Norway to 45.4% in the Netherlands. 8 Generally, higher proportions of home deaths can be seen in more recently published studies; however the numbers vary cosiderably.13,18-20
Regarding the congruence between preferred and actual death place, previous studies have shown that between 31%–80% of patients achieved their preference for place of death.13-21 In previous studies using a prospective interview or questionnaire-based method similar to the present study, the congruence between preferred and actual death place was 48%–72%.16-18,21 The high level of congruence (80%) between preferred and actual death place in the present study is encouraging and similar to what was reported from a retrospective study of patients admitted to an advanced medical home care unit in Stockholm, Sweden. 13 The differences observed between this study and previous studies may be due to cultural reasons 12 as well as due to differences in access to palliative care specialists, nursing support, and equipment such as hospital beds. 23
A considerable strength of the present study is the relatively large number of palliative cancer patients that have been included in a prospective manner. However, there are also limitations with the study that needs mentioning. One limitation is the relatively limited geographical area that has been subjected to the study and the results may be different in other areas of the country. Also, almost 2 thirds of the patients who were evaluated for the study had to be excluded, mainly due to cognitive impairment, which could possibly lead to selection bias. Another limitation of the study is the relatively few patients who wanted to die at other places than at home which makes it hard to draw conclusions regarding factors that influence the decisions of these patients. Another noteworthy aspect of the present study is that it was in large parts conducted during the COVID-19 pandemic. In theory, this may have affected the participants’ preferred place of death since being at home could be perceived as safer due to less risk of contagion, compared to being at a hospital or a nursing home.
Conclusion
In conclusion, the findings of this study show that 79% of the Swedish palliative cancer patients included in this study wanted to die at home and 80% of these patients actually died at home, which are encouraging findings. We also found that patients who make their decision together with relatives are more likely to want to die at home whereas the actual place of death does not differ between these groups. Other factors such as sex, age, marital status, type of tumor, assistance from relatives or health care at home does not seem to impact the preference or likelihood of home death. These findings give valuable insights into the area of end-of-life care and the place of death preferences in palliative cancer patients in a Swedish context.
Supplemental Material
Supplemental Material - Prospective Study of Preferred Versus Actual Place of Death Among Swedish Palliative Cancer Patients
Supplemental Material for Prospective Study of Preferred Versus Actual Place of Death Among Swedish Palliative Cancer Patients by Jonas Nilsson, Stefan Bergström, Hampus Hållberg, Anders Berglund, Michael Bergqvist, and Georg Holgersson in American Journal of Hospice and Palliative Medicine
Footnotes
Acknowledgments
We thank all the patients and their families for their participation in this study. We would like to thank the palliative care team and the oncology clinic in Gävle for their contributions to the study; in particular we want to thank palliative care nurse Malin Holmgren. We would also like to give special thanks to the palliative care team in Bollnäs and Irinia Ruchkina at the specialized palliative care clinic in Avesta, Dalarna County, for help with collection of patient data.
Author Contribution
GH drafted the original manuscript. SB and JN participated in the acquisition of data. HH and AB performed the statistical analyses of the data. All authors participated in the interpretation of data and the revision of the manuscript and have participated sufficiently in the work to take public responsibility for appropriate portions of the content. All authors approve of the current version of the manuscript to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from Stiftelsen Gävle Cancerfond. No grant number is available.
Ethical Statement
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.