
Abstract
Objectives:
Achievement of patients’ preferred place of death is recognized as a component of a good death. This study aimed to investigate the symptom burden in advanced cancer patients, achievement of their place of death preferences and factors associated with home death.
Methods:
In this retrospective review of 287 patient deaths, we examined patients’ symptom prevalence, preferred and actual place of death and achievement of their place of death preferences using descriptive statistics. Associations between patient factors, home death preference and actual home death were further analyzed using multivariate logistic regression.
Results:
The most prevalent symptoms were weakness, pain and poor appetite, with a mean of 5.77(SD: 2.37) symptoms per patient. The median interval from palliative care referral to death was 21 (IQR: 74) days. Of the 253 patients with documented place of death preference, 132 (52.1%) preferred home death, 111(43.9%) preferred hospital death, 1 (0.4%) preferred to die at a temple and 9(3.6%) expressed no preference. Overall, 221 of 241(91.7%) patients with known actual place of death achieved their preference. Older patients were more likely to prefer home death (OR 1.021; 95% CI 1.004-1.039, p = 0.018) and die at home (OR 1.023; 95% CI 1.005-1.041, p = 0.014). Gender, marital status, cancer diagnosis and symptoms were not associated with preference for or actual home death.
Conclusion:
Despite a high symptom burden, most patients preferred and achieved a home death. Late palliative care referral and difficult symptom management contributed to failure to fulfill home death preference. Preference for home death should be considered when managing terminally ill geriatric patients.
Introduction
The fulfilment of end-of-life preferences, including the preferred place of death, is an important component of a good death.1,2 The achievement of a good death experience can positively impact the bereaved by reducing the incidence of negative psychological symptoms and shortening the duration of grief. 3 Most patients prefer to die at home, regardless of cultural differences or nationality.4-11 The preference for a home death is associated with patients’ desire to be close to their loved ones, older age and the availability of home palliative care services.4,8,9 Furthermore, dying at home may have positive effects, including a more peaceful experience for both the patient and caregivers, a better grief experience for the bereaved and a reduced impact on caregiver work commitments. 12 Conversely, the factors that are associated with a preference for a hospital death include a sense of security associated with the hospital setting, poor patient performance status, lack of palliative care team involvement and perception of better symptom control.10,13
Prevalent symptoms among advanced cancer patients include pain, nausea, lethargy, insomnia, depression and anorexia.14-16 The suboptimal control of symptoms such as pain may be further associated with additional factors including a limited access to medications, 17 the underestimation of symptoms by physicians compounded by a hesitancy in prescribing opioids, 18 and the fear of medication side effects and dependence among patients.16,19,20 Additionally, poorly controlled symptoms can lead to hospital admissions at the end-of-life, precluding the achievement of patient’s preference for a home death.
Barriers to achieving patient’s preference for a home death include socioeconomic constraints, being single, a lack of social support, inadequate community nursing support and a lack of discussion regarding end-of-life preferences with treating clinicians.5,13,21-23 In addition, lack of training in advanced communication skills among healthcare professionals may contribute to hesitancy in initiating discussions about end-of-life preferences and concerns about causing psychological distress to the patients, 20 which may further lead to delay in referral to palliative care services and inadequate end-of-life care planning.
The reported rate of achievement of preferred place of death ranged from 49%-88% in western countries in Europe,4,11 United Kingdom5,13,21,24,25 and Canada, 26 and 66% in South Africa. 9 Although studies in Asian countries including China, Japan and India found that most patients preferred a home death,7,8,27 to our knowledge, place of death preference and achievement have not been reported in the Malaysian context.
This study aimed to gain a deeper understanding of the symptom burden among advanced cancer patients and the factors that affected the achievement of their end-of-life preferences by examining the (1) symptom prevalence in advanced cancer patients; (2) preferred place of death; (3) factors associated with incongruence between the preferred and actual place of death; and (4) the factors associated with home death.
Methods
This is a retrospective review of the deaths of patients with advanced cancer (Stage 3 and 4) (n = 287), who died while under the care of the specialist palliative care service in Sunway Medical Centre, a private tertiary hospital in Malaysia, from September 2017 to December 2019.
Data Collection
Relevant data was extracted by reviewing patients’ medical records and palliative care plan documents, which had been created as part of standard patient care. Full ethics approval was obtained from the institutional research and ethics review board (037/2020/IND/ER). Patients’ demographic data (gender, age and marital status), cancer diagnosis, interval between time of palliative care referral and death, indications for referral (based on physician’s documented referral request) and symptom prevalence were reviewed. Data on symptom prevalence was extracted from the staff-proxy reported Integrated Palliative care Outcome Scale (IPOS) (English version), a validated and reliable tool, with good internal consistency (α = 0.77) and test–retest reliability (60% of items kw > 0.60), 28 which had been used to document the presence of symptoms observed by palliative care clinicians during the first palliative care consultation. These symptoms included pain, constipation, weakness or lack of energy, poor appetite, poor mobility, dyspnea, sore or dry mouth, nausea, vomiting and drowsiness. In addition, data concerning patients’ preference for place of death (expressed by the patients themselves or by their next-of-kin), achievement of preferred place of death, and reasons for not achieving the preferred place of death was also collected.
Data Analysis
The extracted data was tabulated, organized and analyzed using IBM SPSS® software. In the univariate analysis, associations between patient variables and the patients’ preferred and actual place of death were examined using descriptive statistics, paired chi-square test (gender, marital status, cancer diagnosis and symptoms) and independent t-test (mean age). A p-value less than 0.05 was considered statistically significant. Patient variables which were identified as significantly associated with place of death (hospital or home) in the univariate analysis were further analyzed with multivariate logistic regression to adjust for potential confounding variables, with associations expressed as odds ratio (ORs) with 95% confidence intervals (CIs).
Results
Patient Demographics and Cancer Diagnoses
A total of 287 patient deaths were reviewed, including 136 (47%) women and 151 (53%) men. The mean age of the patients was 61.2 (Standard Deviation 15.4) years. 249 (87%) patients were married, 35 (12%) were single, and 3 (1%) were divorced. Among the 287 patients, one patient had 3 concurrent malignancies, and 3 patients had 2 concurrent malignancies. The most common cancer in our patient cohort was lung cancer (55 of 287 patients; 18.8%), followed by colorectal (35; 12%) and breast cancer (34; 11.6%) (Figure 1).
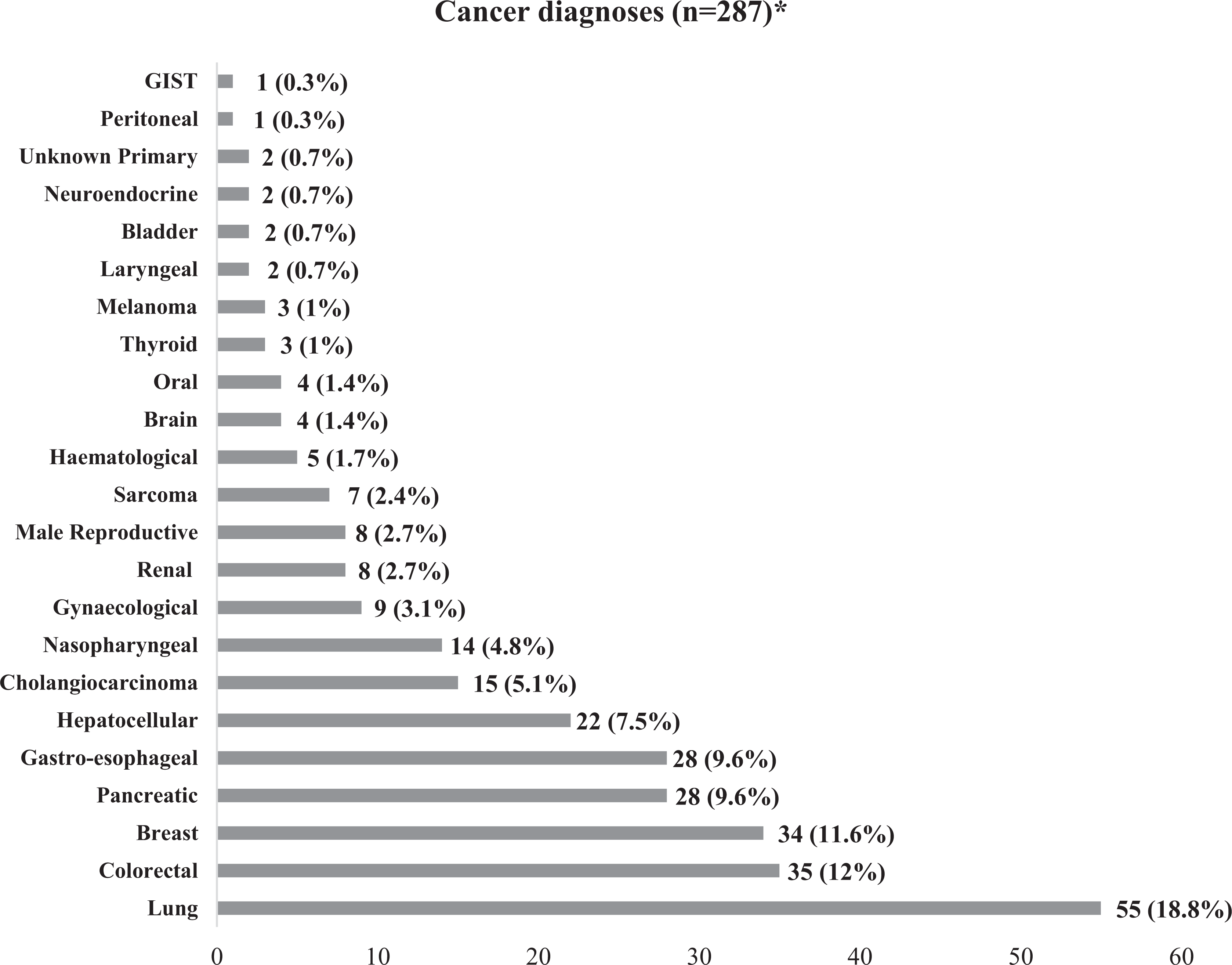
Distribution of cancer diagnoses in patients who passed away under the care of the palliative care unit (n = 287). *Three patients had 2 concurrent tumors, 1 had 3 concurrent malignancies. GIST indicates gastrointestinal stromal tumor.
Symptom Prevalence and Indications for Palliative Care Referral
Complete data on patients’ symptom prevalence as documented at the first palliative care consultation was available in 281 of 287 patients. Among these 281 patients, the most common indication for physician referral to palliative care was pain management (200 of 281; 71.2%), followed by gastrointestinal symptoms (108; 38.4%), psychosocial support (82; 29.2%), end-of-life care (81; 28.8%), liaison with community hospice (75; 26.7%), respiratory symptoms (73; 26%), discharge planning (52; 18.5%), complex wound management (13; 4.6%) and mood disturbance (5; 1.8%) (Figure 2).
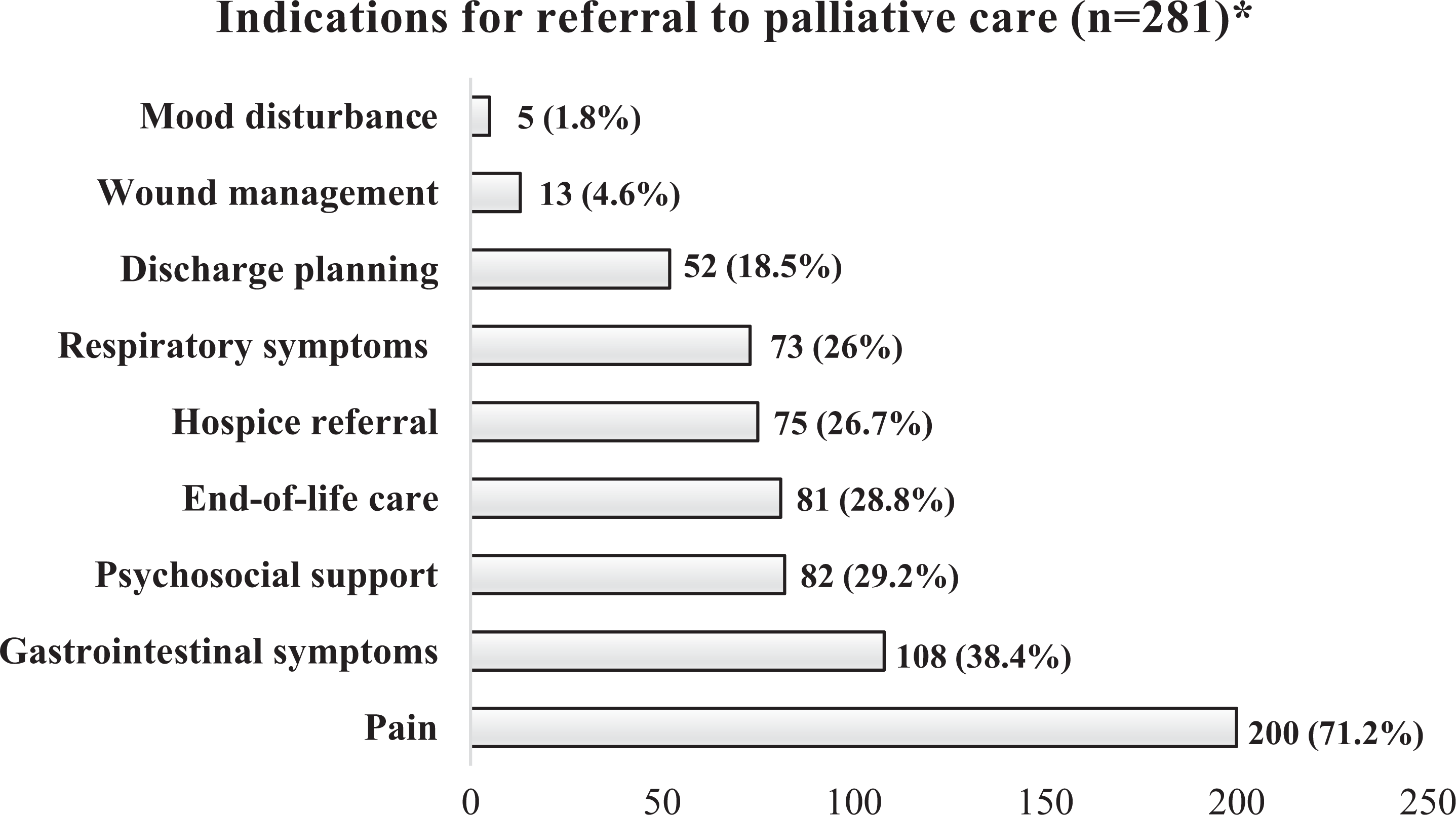
Indications for palliative care referral. *There was incomplete data for 6 patients, thus these patients were excluded from analysis.
Among these 281 patients, weakness was the most prevalent symptom (251 of 281 patients; 89.3%), followed by pain (218; 77.6%), poor appetite (214; 76.2%), poor mobility (209; 74.4%), constipation (183; 65.1%), dyspnea (139; 49.5%), sore or dry mouth (125; 44.5%), nausea (100; 35.6%), drowsiness (99; 35.2%) and vomiting (84; 29.9%) (Figure 3.) The mean number of symptoms was 5.77 (standard deviation 2.37) per patient, reflecting a high symptom burden.
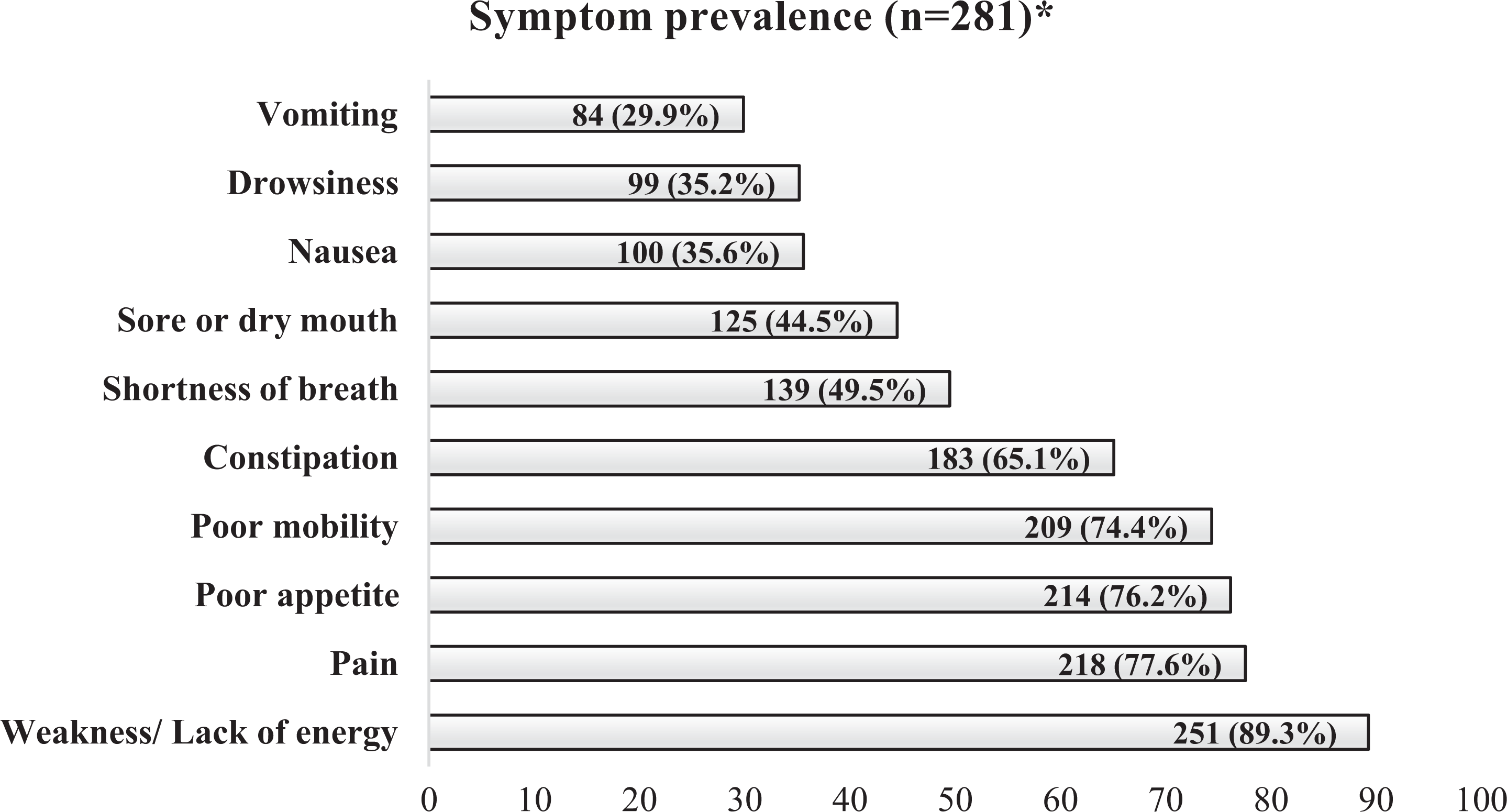
Symptom prevalence observed at first palliative care consultation. *Six patients were excluded due to incomplete data on symptom prevalence.
Among 271 of 287 patients (16 patients were excluded due to incomplete data regarding the date of death), the median time interval between palliative care referral and patient death was 21 (interquartile range 74) days. In addition, 155 (57.2%) patients were referred less than 1 month prior to death.
Place of Death Preferences
Discussions about preferred place of death was documented in 253 of 287 patients (88.2%); 9 of the remaining 34 patients were lost to follow-up, 13 were transferred to another center, and 12 deteriorated acutely before preferences regarding place of death could be established. 10 of these latter 12 patients (83.3%) were referred to the palliative care service less than 1 month prior to death. Of the 253 patients, 132 (52.1%) patients preferred a home death, 111 (43.9%) preferred a hospital death, 9 (3.6%) had no preference and one (0.4%) preferred to die at a Buddhist temple, as the patient was practicing as a nun at the temple (Figure 4). As most of the patients were referred less than 1 month prior to their death, patient’s preference for place of death was expressed by proxy by their next-of-kin in 174 of 253 (68.8%) patients, as they were too ill to express their preferences. The reason for a home death preference was not documented in most cases; the documented reasons for preference for a hospital death included difficulty coping at home, complex symptoms, and not wanting to burden their families.
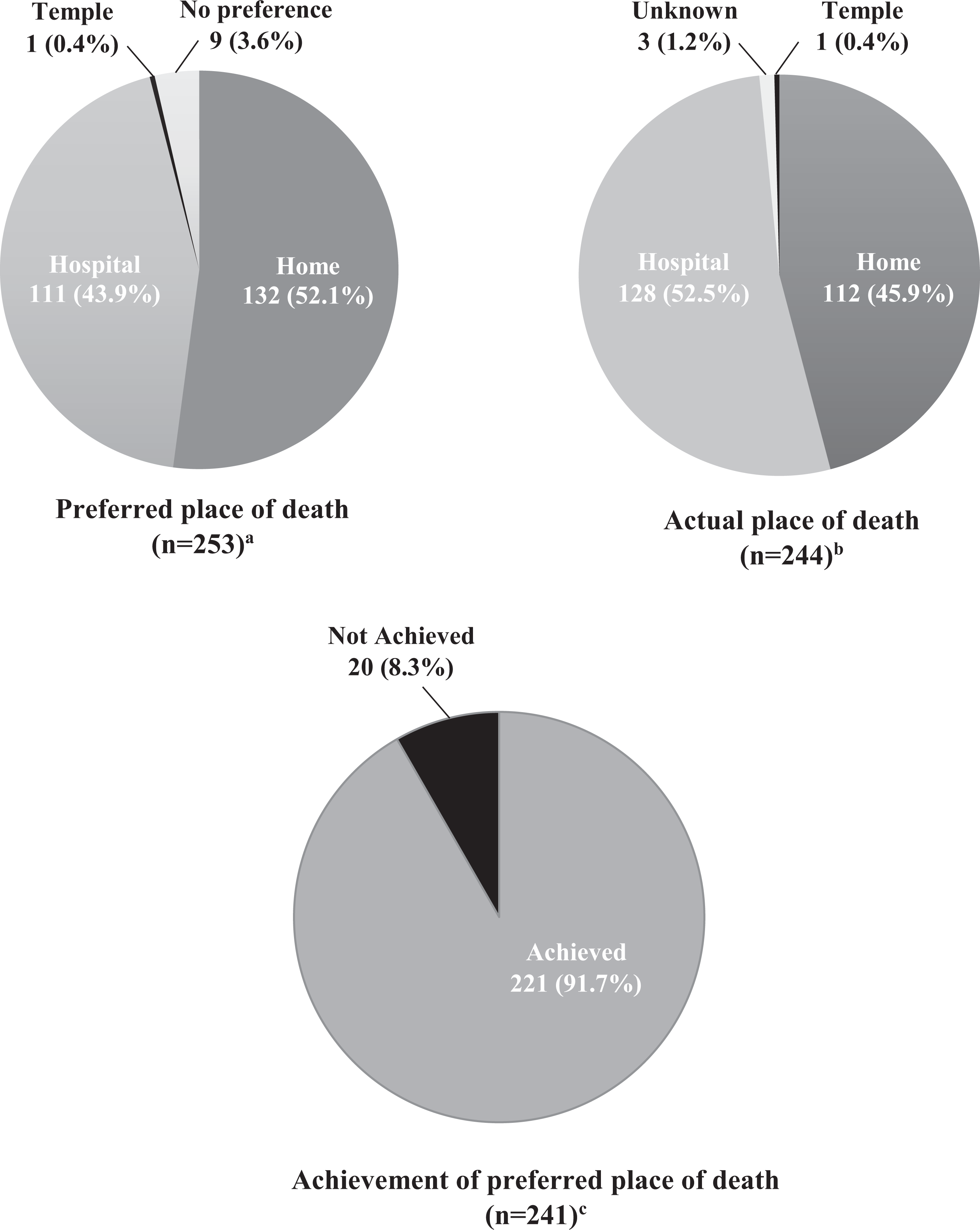
Comparison between preferred and actual place of death and achievement of preferred place of death. (a) 34 of 287 patients were excluded (9 patients were lost to follow-up, 13 were transferred to another center, and 12 deteriorated acutely before preferences regarding place of death could be established). (b) 9 of 253 patients who expressed no preference for place of death were excluded. (c) 12 of 253 patients were excluded (9 patients with no preference for place of death, and 3 who were lost to follow-up).
Achievement of Place of Death Preference
Figure 4 shows a comparison between the preferred and actual place of death and the achievement place of death preference. Among 244 patients who had a preferred place of death (excluding 9 patients with no preference), 128 of 244 (52.5%) patients died in hospital, 112 (45.9%) patients died at home and one (0.4%) patient died in a temple. The place of death was unknown in 3 (1.2%) patients due to loss to subsequent follow-up. Overall, 221 of 241 (91.7%) patients with a known actual place of death achieved their preference, compared with 20 (8.3%) patients who did not (all of whom preferred a home death but died in hospital). Among the patients who preferred a home death, 112 of 132 (84.8%) patients managed to achieve their preference and 20 (15.2%) did not. Reasons for failure to achieve the preference for home death were mainly due to an inability to cope at home because of difficult symptom management (10 of 20 patients), acute deterioration before their planned terminal discharge home (8 of 20) and insufficient time to arrange for terminal discharge home (2 of 20), with an average interval between referral and death of only 2 days in the latter 2 patients.
Associations Between Patient Variables and Preferred and Actual Place of Death
Preferences and patient variables for 237 of 253 patients who had expressed their preferred place of death (home or hospital) were further analyzed to identify the associations between patient variables (age, gender, marital status, cancer diagnosis and symptoms) and the preferred and actual place of death (hospital or home). Sixteen patients were excluded; 9 with no preference for place of death, one who preferred to die at the temple, and 6 with incomplete data on symptom prevalence.
Univariate analysis revealed a significant association between older age and the preference for a home death (p = 0.035). Preference for hospital death was significantly associated with symptoms of nausea (p = 0.028), vomiting (p = 0.035) and constipation (p = 0.034) (Table 1). Older age (p = 0.014) was further associated with actual home death, and nausea (p = 0.001), vomiting (p = 0.001) and constipation (p = 0.015) were associated with actual hospital death. Gender, marital status, cancer diagnosis and symptoms of pain, dyspnea, weakness, poor appetite, drowsiness and poor mobility were not significantly associated with the preferred or actual place of death (hospital or home).
Comparisons Between Patient Variables, Preferred Place of Death and Actual Place of Death (n=237)*
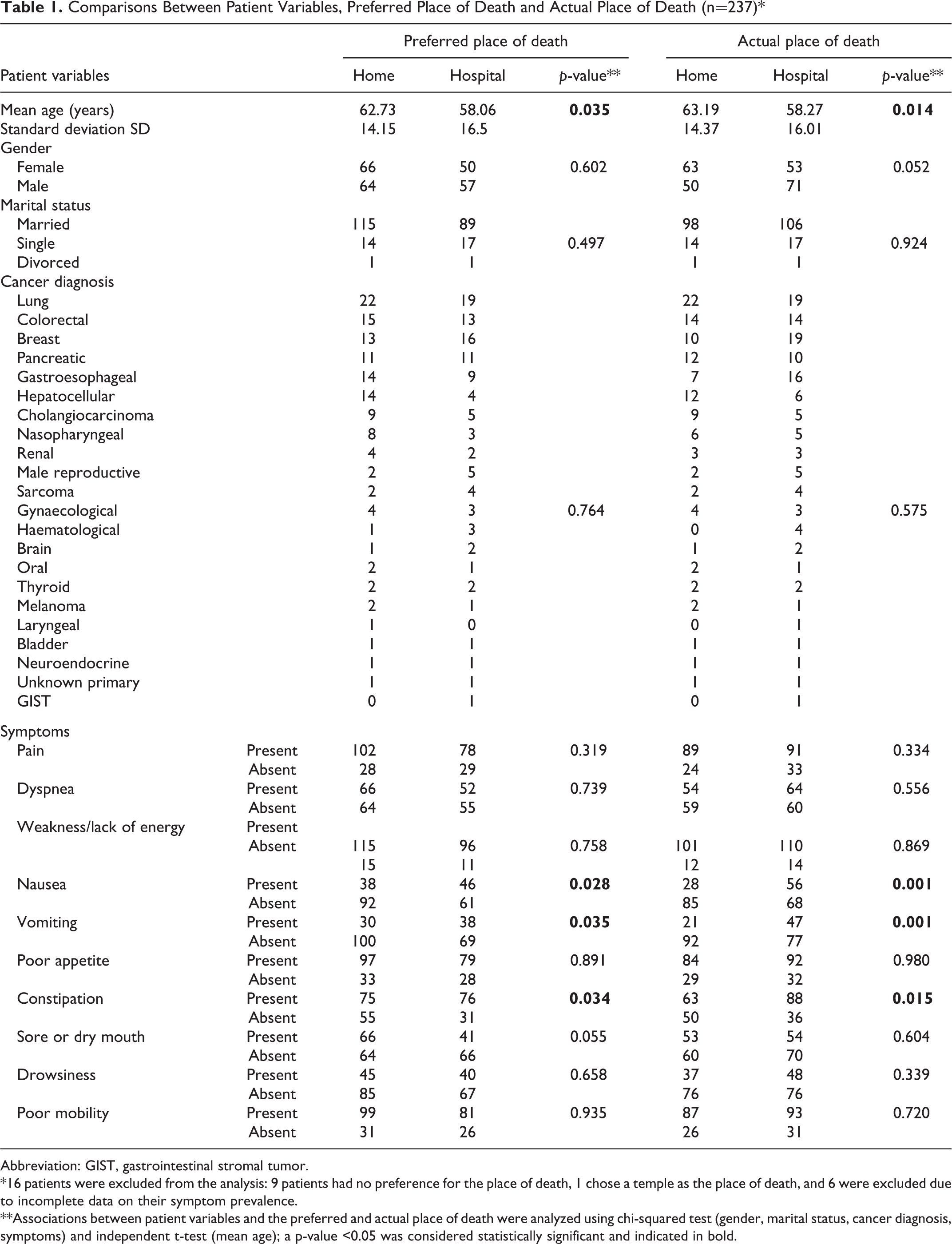
Abbreviation: GIST, gastrointestinal stromal tumor.
*16 patients were excluded from the analysis: 9 patients had no preference for the place of death, 1 chose a temple as the place of death, and 6 were excluded due to incomplete data on their symptom prevalence.
**Associations between patient variables and the preferred and actual place of death were analyzed using chi-squared test (gender, marital status, cancer diagnosis, symptoms) and independent t-test (mean age); a p-value <0.05 was considered statistically significant and indicated in bold.
Patient factors that were identified as significantly associated with home death (older age) and hospital death (nausea, vomiting and constipation) in the univariate analysis were further analyzed used multivariate logistic regression. Only older age remained significantly associated with the preference for a home death (OR 1.021, 95% CI: 1.004-1.039, p = 0.018) and an actual home death (OR 1.023, 95% CI: 1.005-1.041, p = 0.014) (Table 2) after considering confounding variables.
Multivariate Logistic Regression Analysis of Patient Variables With the Preferred and Actual Place of Death.
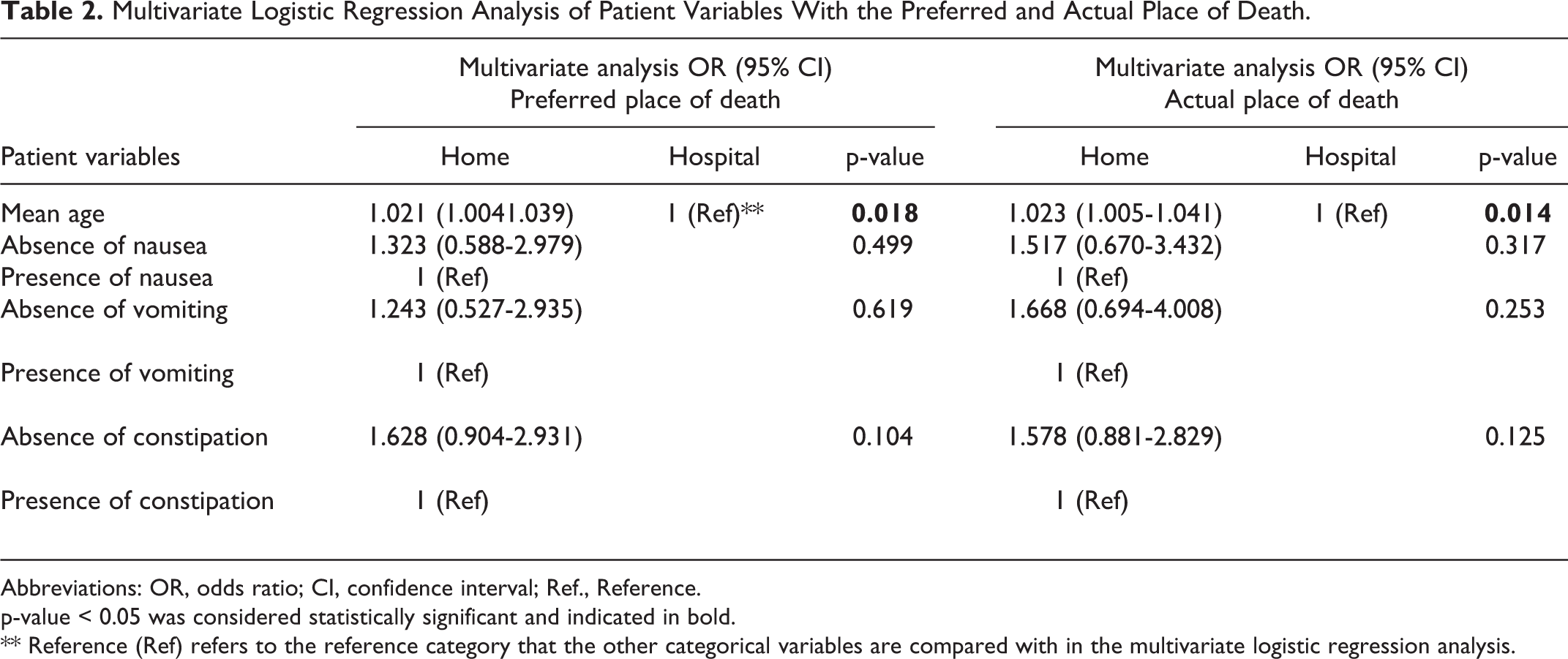
Abbreviations: OR, odds ratio; CI, confidence interval; Ref., Reference.
p-value < 0.05 was considered statistically significant and indicated in bold.
** Reference (Ref) refers to the reference category that the other categorical variables are compared with in the multivariate logistic regression analysis.
Discussion
The most common cancer diagnosis among the 287 patient deaths that were reviewed in this study was lung cancer (18.8%), followed by colorectal cancer (12%) and breast cancer (11.6%). Based on the World Health Organization 2018 global cancer statistics, cancer mortality was also reported to be highest for lung cancer (18.4%), followed by colorectal cancer (9.2%) and gastric cancer (8.2%). 29
Symptom Burden
Symptom burden was high among the patients, with a mean of 5.77 symptoms per patient at the time of the first palliative care consultation. The most prevalent symptoms were weakness and lack of energy (89.3%), pain (77.6%) and poor appetite (76.2%). Similar symptoms have been reported to affect more than 50% of patients with advanced cancer. 14 The most common reason identified for palliative care referral was for pain management (71.2%). Although dyspnea was observed in 49.5% of patients, it was only documented as a reason for referral in 26%, which might imply a lack of awareness and thorough symptom evaluation among referring physicians. Underestimation of symptoms can further lead to inadequate symptom control and poor quality of life in cancer patients.16,30,31
Preference for Home Death
Despite high symptom prevalence, most of the patients in the study preferred home death (52.1%) compared with hospital death (43.9%). In the Malaysian context, specialist palliative care services are only available in a minority of public and private hospitals, and inpatient hospices facilities are scarce. 32 Community palliative care services are provided mainly by non-governmental organizations, catering mostly to the urban population due to limited resources. In contrast, a study in Scotland reported a preference for hospice death in 60% of patients, home death in 37% and hospital death in only 0.7%. 6 Another study in Hong Kong reported a preference for home death in only 31% of patients. 33 The differences in place of death preference could be partially attributed to differences in socioeconomic circumstances7,9,23,34 and the availability of community palliative care services to ensure adequate support at home at the end-of-life.4,9,34
In this study, patients who preferred a hospital death cited inability to cope at home, presence of difficult symptoms, and fear of being a burden as primary reasons for their preference. This further highlights the importance of good symptom management and psychosocial support to facilitate a good death at home. Additionally, the valid preference for death in a hospital or hospice among patients who prefer to avoid burdening their families or creating negative associations between death and home should be acknowledged. 35
High Rate of Achievement of Place of Death Preference
Overall, 222 of 241 (91.7%) patients achieved their preference for place of death (hospital or home) (Figure 4) and 111 of 132 (84.8%) patients achieved their preference for a home death. This result is comparable to reports from palliative care units in the United Kingdom and Europe, where the achievement of the preferred place of death ranged from 63% to 88%.6,11,13,24,25 High rate of achievement of place of death preference in this study could be related to systematic documentation of end-of-life preferences and inclusion of preferred place of death as a standard component of goals of care discussion, which had also been observed in previous studies.11,24,25 In addition, the hospital where this study was conducted is situated in a large city in Malaysia, supported by a well-developed network of community-based palliative care organizations and private nursing services. Thus, most patients were able to fulfill their preference for a home death due to adequate medical, nursing, social and palliative care support in the community.
Barriers to Achievement of Home Death Preference
The median time interval between palliative care referral and death was only 21 days. Consequently, there was insufficient time to facilitate rapid terminal discharges in 2 cases and discussions regarding end-of-life preferences did not occur in some patients as they were actively dying or too ill to participate. The negative association between late referral to palliative care and home death had been demonstrated previously. 36 Further qualitative studies exploring the reasons for late palliative care referrals would provide a deeper understanding of the barriers to early palliative care involvement in the management of cancer patients.
In this study, patients with nausea, vomiting and constipation were more likely to prefer a hospital death and die in hospital. Severe gastrointestinal symptoms can affect patients’ ability to maintain basic nutrition and tolerate oral medications, leading to poor symptom control. Better clinician assessment and management, improved access to parenteral medications at home, and adequate knowledge on symptom management among patients and caregivers might enable patients to cope better at home. Conversely, symptoms of dyspnea and pain were not found to be associated with a hospital death. This could be related to prompt availability of oxygen concentrator machines for home rental, and availability of opioids for symptom in the healthcare setting of this study.
Patient Factors Associated With Home Death Preference
In addition, older age was found to be significantly associated with both a preference for and the achievement of a home death, which corresponded with the findings from previous South African 9 and Southeast Asian studies. 37 This might reflect an increased societal and cultural acceptance of death among older patients, resulting in reduced medicalization of dying. In this study, most patients were Malaysian Chinese. Culturally, elderly Chinese patients may prefer a home death as dying at home symbolized a connection to one’s ancestors and descendants. 38 Furthermore, the importance of filial piety in Asian culture39,40 might contribute to better family support at the end-of-life and thus better achievement of home death preference. Dying at home may also hold religious significance as the home environment can better facilitate the completion of cultural and religious rituals at the end-of-life, which is viewed as an integral part of a peaceful death in some Asian cultures.40,41
Other patient factors, including gender, marital status, cancer diagnosis, and symptom presentation, were not significantly associated with either a preference for or the achievement of either a home or hospital death. This result was in contrast with previous studies that reported that male gender8,37 was a predictive indicator for home death preference. Further studies investigating the factors that enable patients and caregivers to cope with end-of-life care at home, and the impact of culture, spirituality and religiosity on patient’s preference for place of death, would help to identify existing gaps in socioeconomic support and community palliative care delivery, leading to improvement in achievement of end-of-life preferences.
Limitations
The setting of this study was at a private tertiary hospital in a large city in Malaysia. Thus, the findings may not be representative of the rural population, areas with poorer socioeconomic status, or districts without the availability of inpatient and community specialist palliative care services. Most of the sample population was Malaysian Chinese and might not be representative of the end-of-life preferences of other ethnicities.
Conclusion
In conclusion, although a high symptom burden exists among advanced cancer patients, this might not translate to a higher preference for hospital death if the symptoms can be adequately controlled at home, with sufficient medical, nursing, social, and palliative care support in the community. Although most patients preferred to die at home, this was not achieved in some patients largely due to difficult symptom management at the end-of-life, resulting in the inability to cope at home. Late referrals further contributed to failure to establish end-of-life preferences before acute clinical deterioration and insufficient time to arrange for a smooth terminal discharge. This highlighted the importance of early palliative care referral to ensure better outcome at the end-of-life. The positive association between older age and home death further highlighted the importance of considering home death as an option when caring for elderly terminally ill patients.
Footnotes
Acknowledgments
The authors are grateful for the valuable input from Dr Caryn Khoo Shiao Yen in reviewing the manuscript, and from Dr Grace Low Sook Hoon for the administrative support. The authors are indebted to the management, clinical research, medical and nursing divisions of Sunway Medical Centre, Malaysia, for their continuous support in research and advocacy for palliative care.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was not funded, but publication of this article was sponsored by Sunway Medical Centre.