
Abstract
Keywords
Poor communication between clinicians, patients, and their families has serious consequences for physical and psychosocial health. 1 Many studies have found that families report experiencing deeply flawed communication with clinicians in the intensive care unit (ICU), with up to 50% of families experiencing anxiety, depression, and post-traumatic stress disorders (PTSD).2–4 Family members of ICU patients often report feeling unprepared for surrogate decision-making. 5 Previous research suggests that interventions that empower families to think deeply about their existing values, beliefs, and responses in advance of a family meeting may help them be more prepared for Shared Decision Making (SDM) and improve communication quality.6,7
SDM has been endorsed by many professional societies as an evidence-based communication strategy for improving clinical communication by encouraging healthcare providers to partner with family members during the decision-making process. 7 However, complex interventions aimed at facilitating SDM have met limited success in improving psychological outcomes in the ICU.8-10 New approaches are needed.
Multiple Goals Theory (MGT) is a useful model for defining “high-quality” communication in a way that is useful for ICU clinicians.11,12 The theory describes 3 types of communication goals: (1) Task goals (eg, disclosing a prognosis, eliciting information, making a decision); (2) relational goals (eg, maintaining trust, strengthening the therapeutic alliance, demonstrating empathy); and (3) identity goals (eg, treating the whole person, affirming personal traits, respecting autonomy).13-15 Each of these goals are pursued during clinical conversations, and when clinicians are able to meaningfully “juggle” task, relational, and identity goals by attending to them within a conversation, high-quality communication is achieved; when 1 or more goals are ignored or inadequately addressed, lower quality communication occurs. 12
The objective of this study was to use MGT to develop a family-centered communication tool (Let’s Talk workbook) to help prepare families for ICU family meetings and to assess the feasibility of using a method called “Communication Quality Analysis” (CQA)11,16 to measure communication quality in ICU family meetings. Specifically, the Let’s Talk workbook was created by generating content to address task, relational, and identity goals, and CQA was developed as a rigorous assessment in which raters score individuals’ communication based on their attention to task, relational, and identity goals. 16
Method
Overview of Study Design
This mixed methods study was conducted at a single, academic tertiary care center in [redacted] from March 2019 to 2020. The study was conducted in 3 parts, all of which fall within Phase 1 of the NIH Stage Model for behavioral intervention development and refinement. Phase 1a involved conceptual design of the tool; Phase 1b involved qualitative acceptability testing and refinement of the tool’s format and language with stakeholders; and Phase 1c involved testing the feasibility of using CQA to measure family members’ and providers’ communication quality during ICU family meetings. Although the pilot study for Phase 1c was designed and conducted as a small, randomized controlled feasibility trial, it was stopped early in late 2020 because of low enrollment and logistical challenges due to the COVID-19 pandemic. Thus, intervention-type comparisons were not pursued due to lack of power. Findings are reported as an observational study focused on tool development and assessment. This manuscript follows STROBE guidelines.
Phase 1a: Conceptual Design and Development
Alignment of Shared Decision-Making Framework With Multiple Goals Theory of Communication to Generate Let’s Talk.
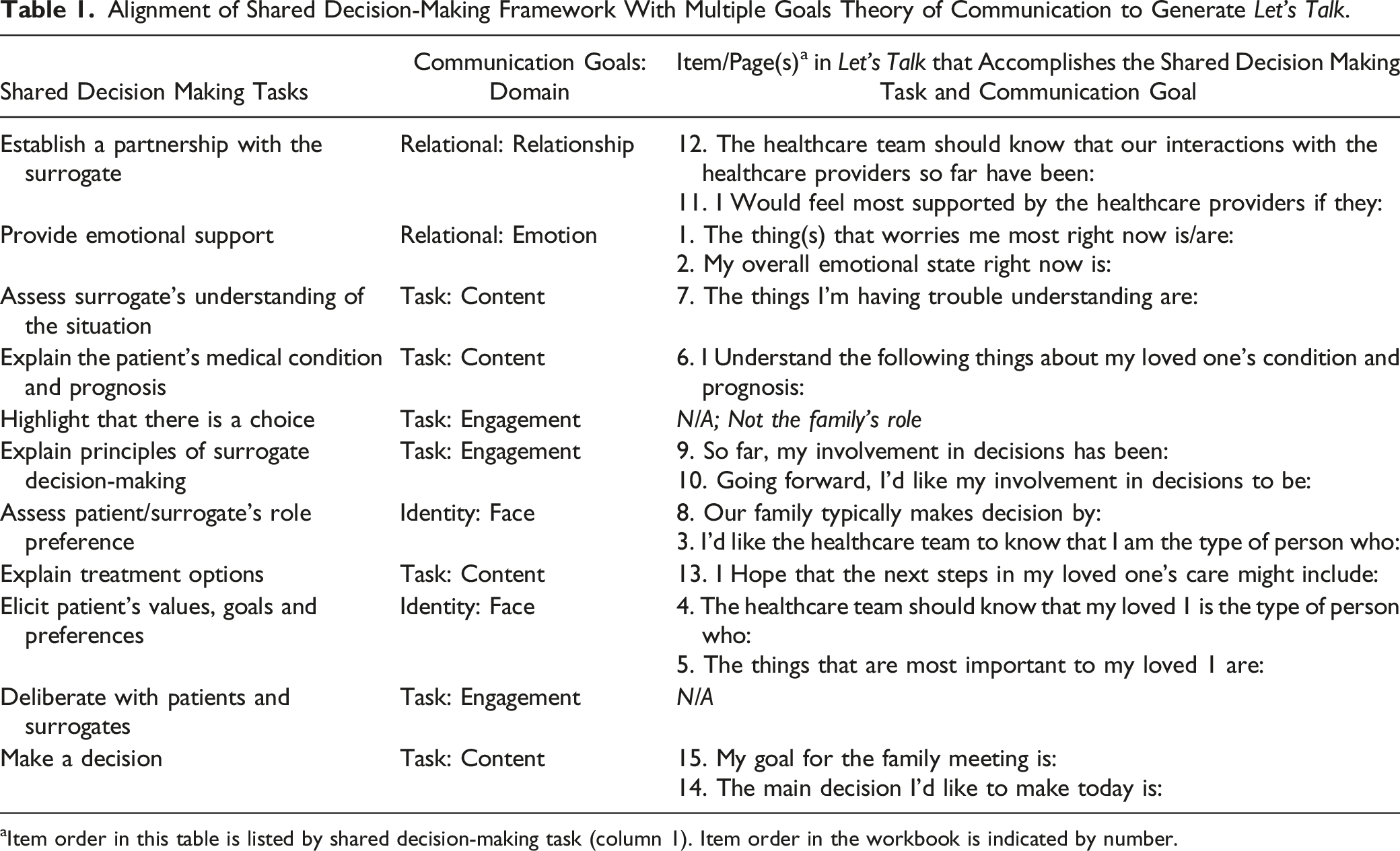
aItem order in this table is listed by shared decision-making task (column 1). Item order in the workbook is indicated by number.
The workbook was developed with input from multiple stakeholders (n = 11), including ICU physicians, nurses, social workers, communication scientists, a chaplain, psychologist, and family members of critically ill patients. Each independently reviewed the tool and provided verbal feedback while research assistants took field notes. Some found the format of the workbook to be “elegantly clean and simple”, yet others thought the tool could be more tailored to maximize engagement. Based on extant literature showing that the medium of comics is accessible, immersive, and disarming and that it attends to readers’ informational and emotional needs,
18
we created a second version of Let’s Talk using a comic form. The comic-based workbook used a welcoming visual style to engage readers affectively while ensuring the content matched the original version so it still aligned with the 2 conceptual models. The result was a 25-page workbook designed to be completed before engaging in a family meeting (Figure 1; eFigure 1). Excerpted pages from Let’s Talk. (A) represents the Face domain (Identity goal); (B) represents the Emotion domain (Relational goal); (C) represents the Relationship domain (relational goal); and (D) represents the Engagement domain (Task goal). Reproduced with permission from Taylor and Francis Ltd, (www.tandfonline.com).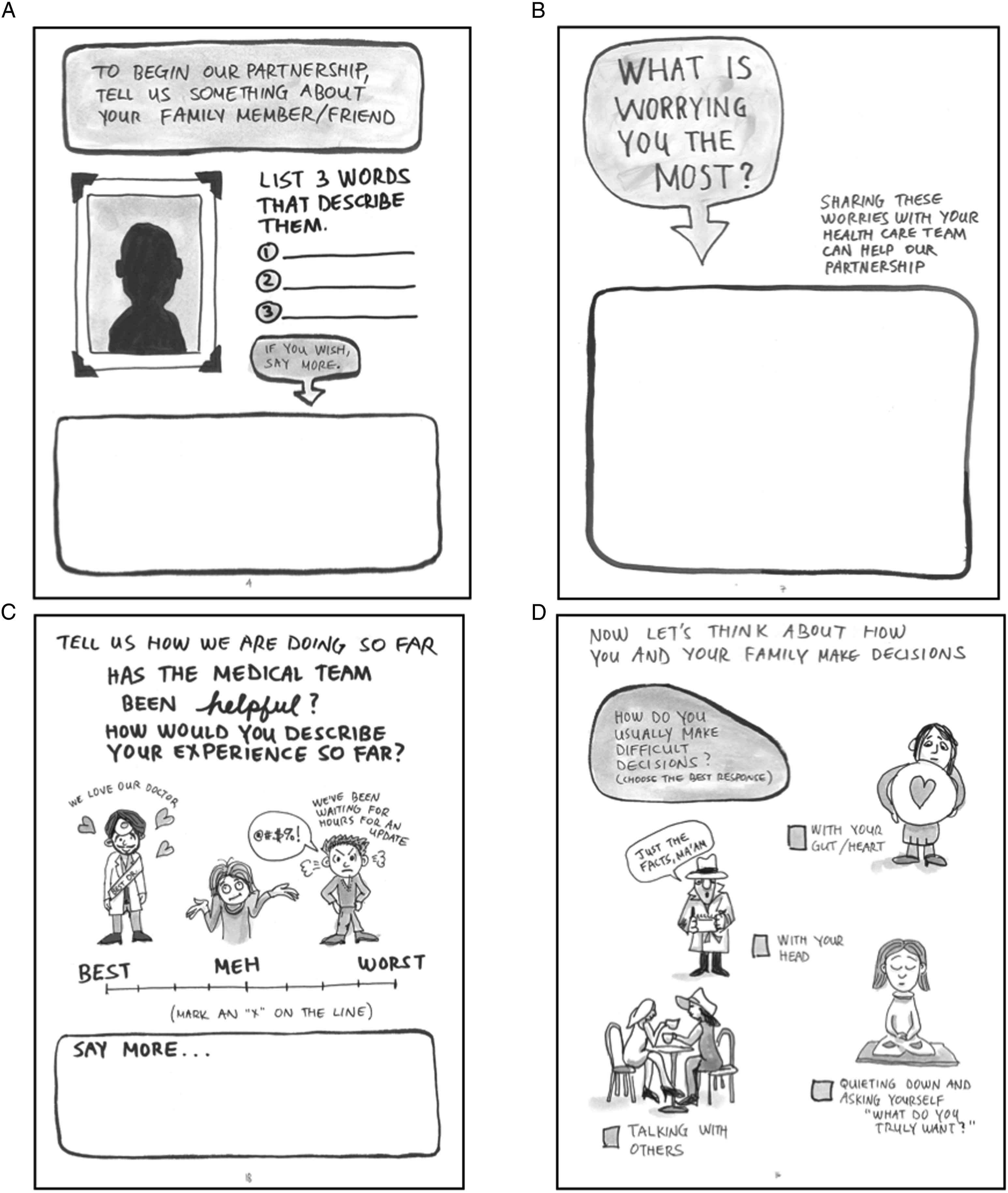
Completing the workbook before a family meeting enables families to reflect on their emotional and relational needs privately, giving them a sense of control and ownership in the family meeting. It also allows them to identify and draw upon their pre-existing knowledge and experience rather than focus on learning new information, which can be challenging during stressful times. Additionally, by empowering families to think deeply about their existing values and beliefs before a family meeting, we anticipated they would be better prepared to share their responses in the meeting during the SDM process. Since it is recommended that clinicians ask open-ended questions during SDM in family meetings, 19 we heavily utilized an open-ended question format.
Phase 1b: Qualitative Acceptability Testing
Participants were family members of ICU patients for whom surrogate decision-making was likely to occur. Inclusion criteria were: 1. Adults (≥18 yrs old) able to provide informed consent; 2. A family member of an ICU patient, defined as the individual identified by the healthcare team as the person responsible for surrogate medical decisions; and 3. A need for a family meeting to engage in SDM about a major medical decision as identified by the care team.
Family members were excluded from Phase 1b if they were unable to read and speak English. After informed consent, participants completed a brief demographic questionnaire. Next, they were presented with the original and comic form of the workbook and invited to select 1 to review in detail; written responses were encouraged yet optional. Most families reviewed the tool ∼1 hour prior to the family meeting and reviewed the tool for ∼20-30 minutes; no families had difficulty completing the tool. After the family meeting, a research assistant conducted a 20-minute structured qualitative interview (Appendix 1) that solicited family thoughts about the workbook, reviewing it 1 page at a time. Interviews were audio-recorded and transcribed verbatim.
Phase 1c: Feasibility Testing of CQA
Family members in Phase 1c met the same eligibility criteria as those in Phase 1b. The purpose of this phase was to assess the feasibility of using the CQA coding method to assess clinical communication quality. Clinicians who attended the family meetings of consented participants provided verbal informed consent for audio recordings. If any individual did not consent, the meeting was not recorded. To minimize observation bias, research assistants did not attend meetings. Charts were reviewed retrospectively to abstract diagnoses, SOFA scores, and hospitalization characteristics (ie, length of stay).
CQA, which has been validated across multiple contexts.11,16,20 involves having 3 coders independently review audio recordings and verbatim transcripts. For each 5-minute interval of the recorded conversation, coders rate how well each participant attended to task, relational, and identity goals on 7-point Likert scales (1 = lowest quality and 7 = highest quality). Each goal includes 2 domains (eFigure 2). For all 6 domains, coders increase or decrease scores as warranted by the conversation. At the end of each 5-minute segment, the score represents the overall quality of the full 5-minute increment for each participant. CQA accounts for how and for what purpose something is said,11,12 rather than simply coding for whether communicative behaviors occur, such as by using frequency counts of certain behaviors.
An overview of the coding process is shown in Figure 2 and Appendix 2. Coders were trained using video modules and a 25-page CQA manual detailing all coding procedures, definitions, and examples. Frequent reliability checks were performed to ensure that interrater reliability (measured by the intraclass r coefficient) remained high.
21
Score calculations are described below. Rating process for CQA domains. A domain score is calculated for each of the 6 communication quality domains. Using the emotion domain as an example, the neutral score is assigned as a “1,” and as participants express emotion (as per the definition above and further detailed in the CQA codebook) the score increases. A domain score is assigned every 5 minutes for each of the 6 domains. All domains are scored 1-7 with “7” being the highest quality score. Reproduced with permission from Taylor and Francis Ltd, (www.tandfonline.com).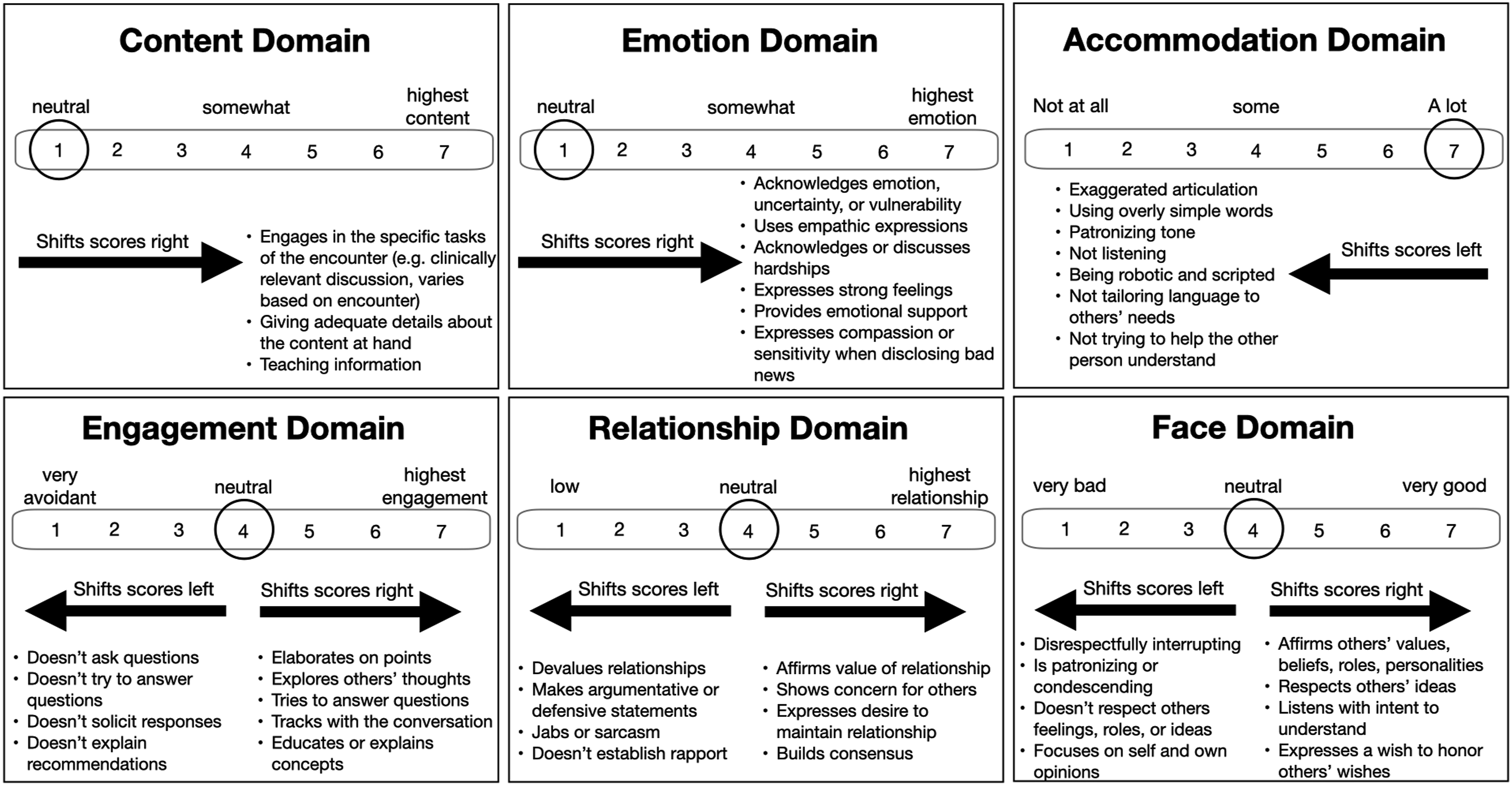
Analysis
Sample size for Phase 1b was determined using an estimated point of data saturation (n = 10). The sample size calculation for the originally designed two-site pilot, feasibility RCT was n = 30 family meetings. However, recruitment was stopped at n = 18 family meetings (total recordings n = 17 due to unuseable audio). The first 5 Phase 1b interview transcripts were reviewed by an experienced qualitative researcher (LJV) to assess saturation; 4 additional interviews were conducted, saturation confirmed, and recruitment ceased after 9 interviews. Since Phase 1b aimed to identify areas of concern or refinement regarding Let’s Talk, summary coding was utilized. Two analysts (LJV, JH) reviewed transcripts independently and inductively created codes to summarize the data. Codes were organized into a codebook and data was analyzed using MAXQDA 2020. 22 The coding report was reviewed with the team. Only minor adjustments to the tool were necessary.
Scores for each
Results
Phase 1a and 1b
Participant Demographics From Phase 1b and Phase 1c.
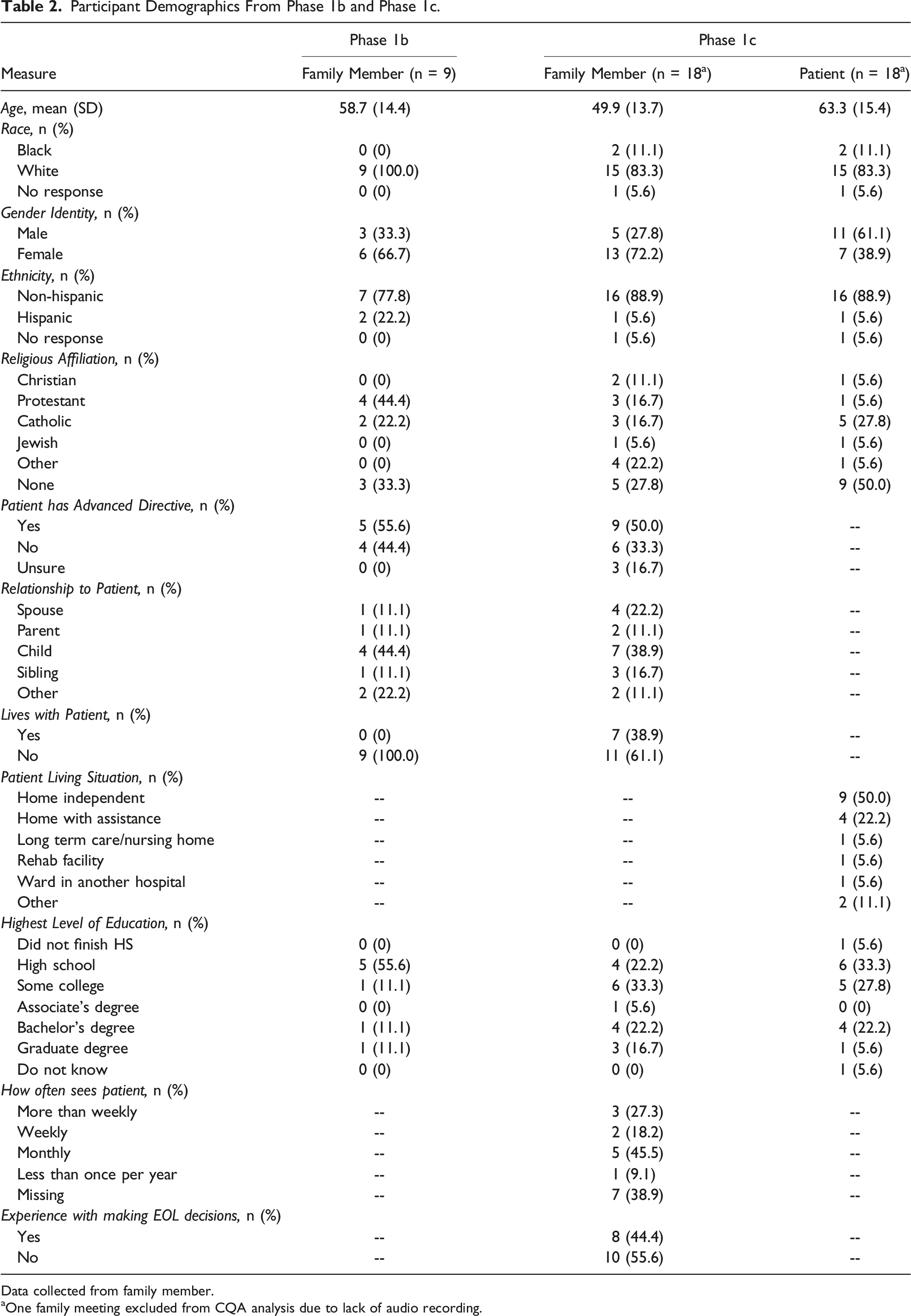
Data collected from family member.
aOne family meeting excluded from CQA analysis due to lack of audio recording.
Themes and Exemplar Quotes From Phase 1b Qualitative Interviews.
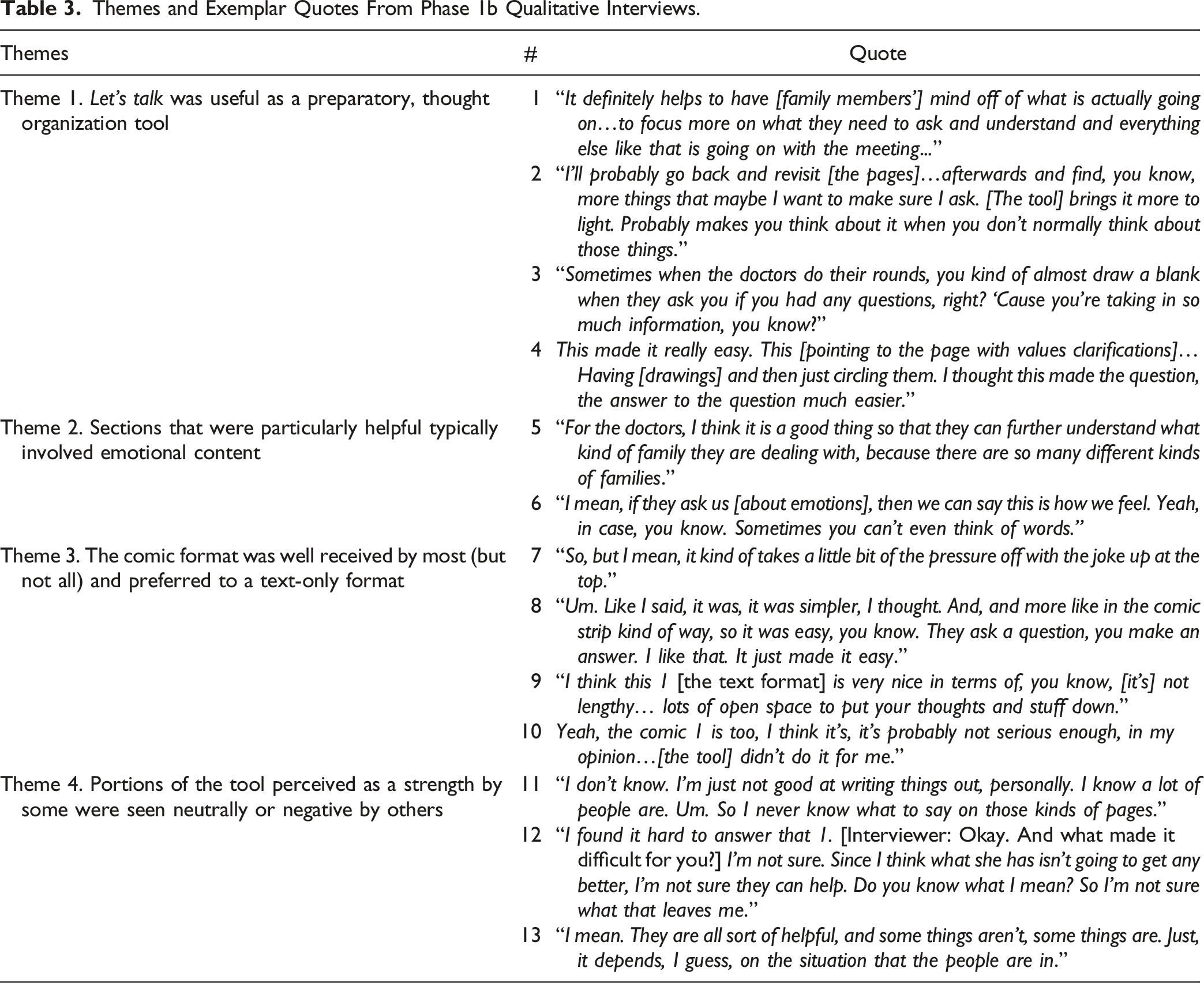
Let’s Talk was useful as a preparatory, thought organization tool
After participating in family meetings, participants reported that Let’s Talk provided a helpful framework for preparing for the meeting (Quote 1) and helped prompt thoughts and questions that may have been overlooked but were important (Quote 2). Participants described how the workbook helped them prevent “drawing a blank” during the meeting (Quote 3) and noted that the tool’s simplicity made difficult topics easier to address (Quote 4).
Sections that were particularly helpful typically involved emotional content
Some participants shared that the recommended breathing exercises were helpful for managing overwhelming emotional states and also that the workbook was a way for providers to get to know more about the family and how they handle emotions (Quote 5). Some participants noted that Let’s Talk depicted illustrated feelings, which made it easier to convey to the medical team how they were feeling (Quote 6).
The comic format was well received by most (but not all) and preferred to a text-only format
Participants were given a choice between the comic and workbook formats of Let’s Talk, and most (67%) chose the comic format. Participants appreciated the lightheartedness of the comic format (Quote 7) and its simplicity (Quote 8). Some participants preferred the text-based version, including the “white space” provided for writing responses (Quote 9). A minority of participants who chose the comic format did not like the comic approach (Quote 10).
Portions of Let’s Talk that were perceived as a strength by some were viewed neutrally or negatively by others
These instances primarily centered around expressing feelings, individual circumstances of the patient’s condition, and the comic format. One participant felt that expressing their emotions in writing was difficult (Quote 11). Others found it challenging to articulate responses to some questions (Quote 12). Several participants acknowledged that the usefulness would depend on each family’s unique circumstances (Quote 13). The refined, full version of Let’s Talk is presented in eFigure 1.
Phase 1c
For Phase 1c, 34 family members were approached for enrollment, and 17 individuals (50%) consented (eFigure 3). Participants were primarily White (83%) females (72%) with a mean age of 49.9 (SD = 13.7) years (Table 2). The mean patient SOFA score was 7.5 (range 3-14). CQA was performed on all (n = 17) recorded family meetings. Intraclass coefficients (r) for each domain were high: content = .92, engagement = .91, emotion = .95, relationship = .80, face = .86, and accommodation = .78. Figure 3 compares domain scores and MGS of the clinicians and family members. For most domains, both groups had similar CQA scores. However, in the content (P = .008) and engagement (P = .026) domains, providers scored significantly higher than family members, and family members scored significantly higher than providers in the emotion domain (P = .015; Figure 3(A)). MGS were similar between the 2 groups (Figure 3(B)). CQA Scores for family members and clinicians during ICU family meetings. (A). Domain scores range from 1 to 7; to account for differences in the neutral ‘starting point’ for coding for the varied domains, data are presented as distance from the neutral point for each domain. Neutral is 1 for content; family members had significantly lower communication quality in the content domain than clinicians as assessed by their distance from the neutral score for that domain. The raw scores on the content domain are thus 4.5 and 5.3, respectively (data not shown) because the neutral point for content domain is 1. For the engagement domain, the neutral point is 4. There was no significant difference between communication quality scores in the distance from neutral for the engagement between family members and clinicians (1.7 vs 2). The raw scores for engagement were 5.7 and 6.0, respectively. By reporting distance from neutral (rather than the raw scores) allow comparison across domains as it standardizes by distance from the neutral point of each domain. Note that for the accommodation domain, the neutral starting point is ‘7’, and therefore lower scores signify lower quality communication. (B). Raw multiple goals scores are reported.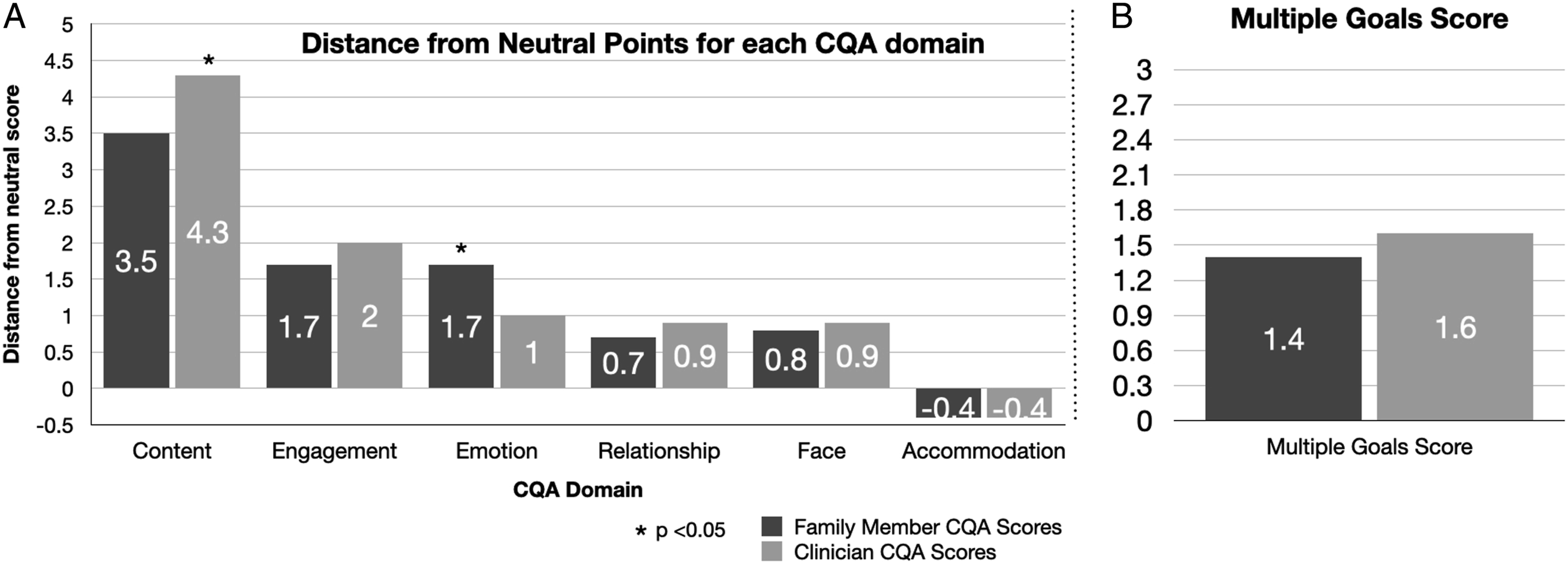
Discussion
Finding new ways to improve and assess communication quality is key to reducing stress for family members of ICU patients and improving health outcomes for patients. Our results demonstrate that Let’s Talk was positively appraised as a useful preparatory tool for family meetings and that CQA can be feasibly and reliably applied to ICU family meetings.
Let’s Talk is a family-centered workbook tool grounded in communication theory. Few interventions prepare families for the stresses associated with decision-making, despite the fact that families involved in decision-making without emotional support are more likely to experience PTSD. 4 Our qualitative evaluation revealed that Let’s Talk prepared families for their family meeting by helping them anticipate some topics and identify their emotional state. However, not all family members appreciated the emotionally laden content of the workbook and were less engaged by that aspect of the tool. Our qualitative analysis informed minor modifications of some workbook pages (eg, we eliminated a drawing exercise based on user feedback).
That 6 of 9 family members chose the comic over text form of the workbook is not surprising given the way the comic-based workbook engaged readers with non-threatening imagery and interactive exercises that attended to a broad range of family members’ experiences. The use of comics in medicine has grown recently and has helped launch a new field of “Graphic Medicine” that explores how the medium of comics intersects the discourse of medicine. 23 By showing through words and images how people experience various life challenges, comics-based workbooks promote empathy and can reduce the sense of isolation so commonplace in the ICU environment.
The result of this pilot work is a theory-driven and easy-to-use workbook to facilitate ICU family meetings. Next steps in tool development include efficacy testing on a larger sample to examine preferential differences between formats and whether Let’s Talk stimulates high-quality communication and improves psychological outcomes for families who use it compared to families who do not.
To conduct this work, a robust and valid measure of communication quality is necessary. The third part of this project helped establish that CQA can be feasibly and reliably applied to ICU family meetings, as evidenced by the high interrater reliability for each communication quality domain. Previous work shows that CQA is feasible, reliable, and valid in other settings when distinguishing between high-quality and low-quality conversations based on communication goals,11,12,16,20 but this was the first study to use CQA in a clinical context. The present CQA data provide a descriptive account of how specific communication goals are achieved by family members and clinicians. This is important, because the communication quality of a conversation is influenced by the contributions of each participant, not simply the clinicians’ communication (which has been the focus of prior studies). When applying CQA to this small dataset, we found that clinician CQA scores were highest for the content and engagement scores, the 2 domains of the task goal, whereas scores for the emotion domain were higher for family members. This is unsurprising given that previous work has shown that clinicians tend to do the talking, disclose information, and facilitate decision-making in family meetings, 24 and meetings are typically more taxing emotionally for family members than for clinicians.
In short, our CQA data points to a need for greater attention to relational and identity goals during family meetings. Interventions emphasizing therapeutic partnerships and promoting respect for identity may help improve communication quality; Let’s Talk is an example of a tool that specifically targets these domains. Furthermore, CQA allows researchers to test the impact of interventions on specific domains of communication to identify areas that are most lacking in quality.
The current investigation had several limitations. First, the small sample size and study design limits generalizability of the findings. While our results demonstrate the feasibility of Let’s Talk and CQA assessment, more work is needed to evaluate their relationships with outcomes. Second, there is potential for selection bias (as those more open to end-of-life conversations are more likely to participate) and social desirability bias in qualitative responses. Furthermore, the study was not designed for quantitative comparisons between the text-only version and the comic version of the Let’s Talk workbook. Finally, we do not report clinician perceptions of the tool in this report.
Strengths of this study include the theory-driven design of Let’s Talk and the assessment of the tool, which allows us to explore what specific aspects of communication constitute high-quality communication and explains why certain aspects of communication quality matter (ie, goal attention). Our use of comics is unique in the ICU setting and sets the stage for additional studies utilizing this intervention form. Finally, by demonstrating feasibility and reliability of CQA in the ICU context, CQA is poised for use in future studies assessing communication interventions.
Conclusions
Let’s Talk is grounded in principles of communication science and has potential for helping family members better prepare for ICU family meetings. CQA provides a theory-driven and feasible approach to assessing communication quality. Ongoing research will evaluate clinician perspectives on how best to incorporate Let’s Talk in practice, wether CQA scores are associated with health outcomes, and the extent to which Let’s Talk improves communication quality.
Supplemental Material
Supplemental Material - Feasibility and Acceptability of a Novel Intensive Care Unit Communication Intervention (“Let’s Talk”) and Initial Assessment Using the Multiple Goals Theory of Communication
Supplemental Material for Feasibility and Acceptability of a Novel Intensive Care Unit Communication Intervention (“Let’s Talk”) and Initial Assessment Using the Multiple Goals Theory of Communication by Lauren J. Van Scoy, MD, Allison M. Scott, PhD, Jacob Higgins, RN, PhD, Emily Wasserman, MSc, Daren Heyland, MD, Vernon Chinchilli, PhD, and Michael J. Green, MD, MS in American Journal of Hospice and Palliative Medicine®
Footnotes
Acknowledgments
The authors would like to acknowledge [redacted] for aiding with the design and content of the comic form of Let’s Talk. We also thank research assistants [redacted] for their assistance with data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Society for Critical Care Medicine Discovery Research Grant award.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.