
Abstract
Key Message
Providing culturally sensitive end-of-life care for Muslim populations requires understanding the role of non-disclosure practices. Healthcare providers must actively address these challenges to deliver compassionate and culturally appropriate care.
Introduction
Non-disclosure is the deliberate withholding of information and refers to the practice of withholding information about a patient’s condition or prognosis from the patient themself. 1 This can happen at the patient’s request or due to cultural and religious beliefs that might influence how a family shields information from a patient. In end-of-life care, the practices of decision making and disclosure carry profound significance, especially within diverse cultural and religious contexts. Among Muslim patients, the approach to nondisclosure at end-of-life is deeply intertwined with religious teachings, ethical considerations, and familial dynamics.2,3
In this way, disclosure practices at the end-of-life in Muslim communities are significantly influenced by religious beliefs and cultural practices. This is even more important in palliative care, specifically for Muslim populations. Culture, encompassing such factors as ethnicity, race, religion, language, nationality, behavior, and tradition, plays a central role in understanding psychosocial needs and influencing healthcare interactions.4,5 While universal principles of end-of-life care apply across different cultural contexts, unique cultural incongruencies exist, including attitudes towards death, hope, patient abandonment, and religious interpretations surrounding end-of-life care.6,7 Religion in particular can have a profound influence on medical decision making and end-of-life care, emphasizing its significant association with an individual’s health outcomes. 2 Religious beliefs shape preferences regarding the disclosure of medical information, the inclination towards aggressive medical interventions, and a reduced willingness to opt for hospice care. Two systematic reviews further highlight the diversity in end-of-life-care approaches across populations, driven by individual, cultural, and religious beliefs.3,8 Healthcare providers (HCP) are urged to acknowledge this diversity within patient populations and recognize variations in preferences and values related to medical care. 9
Moreover, present efforts to provide culturally relevant care to Muslim patients in the palliative care setting are insufficient. The cultural norms, religious beliefs, and family dynamics that mold end-of-life preferences significantly affect the delivery of palliative care. 10 Studies underscore the prioritization of comfort over aggressive medical interventions, calling attention to the crucial role of family in the decision-making process.11,12 Consequently, this inclination towards non-disclosure often prolongs the dying process fueled by belief in “miracles” alongside other factors.13,14 In addition, prevalent cultural taboos surrounding death and dying contribute to non-disclosure practices in Muslim-majority countries, presenting challenges for healthcare providers in delivering appropriate palliative care interventions.12,15,16 Mendieta and Buckingham (2017) highlight the influence of Islamic culture and religion on end-of-life care, emphasizing the role of faith in fostering hope for a miracle and the challenge of managing the unrealistically high expectations of a patient’s family. 17
Although, global efforts are underway to provide culturally relevant care to Muslims, advocating for the development of culturally sensitive decision-making tools to facilitate discussions and enhance end-of-life care outcomes, the research is scarce. 18 Nayfeh (2024) explores various aspects, including advance care planning programs, interventions led by healthcare providers, decision aids, and communication strategies tailored for minority backgrounds. They conclude that further research is necessary to “co-design” and “co-pilot” instruments for setting goals of care, emphasizing collaboration with patients, their healthcare teams, and families. 19 With regards to understanding the influences on end-of-life care in Muslim communities, there is a lack of emphasis, thus far, on disclosure practices for Muslim patients and how nondisclosure around prognosis and diagnosis is influenced by cultural dynamics often resulting in withholding of medical information. As a result, nondisclosure in the Muslim population at end of life warrants further research. Gustafson and Lazenby (2019) suggest that healthcare education should prioritize patient-centered care. This approach acknowledges the significance of accommodating family dynamics, especially in cultural contexts like the Middle East, where decision making often extends to the entire family.20,21
Moreover, recognizing the gap between the Muslim patients’ understanding of their prognosis and diagnosis and disclosure will facilitate future research aimed at systematically addressing this issue in a way that is customized to the needs of the Muslim patient population, around their understanding of decision making at end of life and implementing a family-centered model for medical decision making. The focus of this review is to examine the disclosure practices in Muslim populations and its impact on palliative care delivery, particularly around resources and goals of care.
Methods
Search Strategy
The search strategy involved retrieving literature from 2009 to 2024 on April 11, 2024, from different databases, including CINHAL, PsychINFO, Scopus, and PubMed. The author collaborated with an informationist to best identify the Medical Subject Heading (MeSH)/Index headings in the selected database. The search was conducted using a combination of two separate searches with MeSH: Search 1 with keywords “Muslim” OR “Muslims” AND “end of life” OR “terminal care” AND “decision making” OR “patient care planning,” and Search 2 with keywords “end of life” OR “terminal care” AND “disclosure” OR “truth telling” AND “Muslim” OR “Muslims.” References from the articles were utilized to further identify relevant literature. The search strategy is outlined in Figure 1. The literature inclusion criteria focus was on studies documenting terminal diagnoses in Muslim patients aged 18 and above, covering the period from 2009 to 2024. Excluded from the review are articles reporting chronic but non-terminal diagnoses, studies involving patients under 18 years old, those conducted before 2009, abstract-only articles, commentaries, editorial reviews, and articles not in English (NEL). These criteria aim to ensure the relevance and quality of the selected literature for the review process (refer to Table 1). Flow diagram chart of identification & selection of articles. Inclusion and Exclusion Criteria.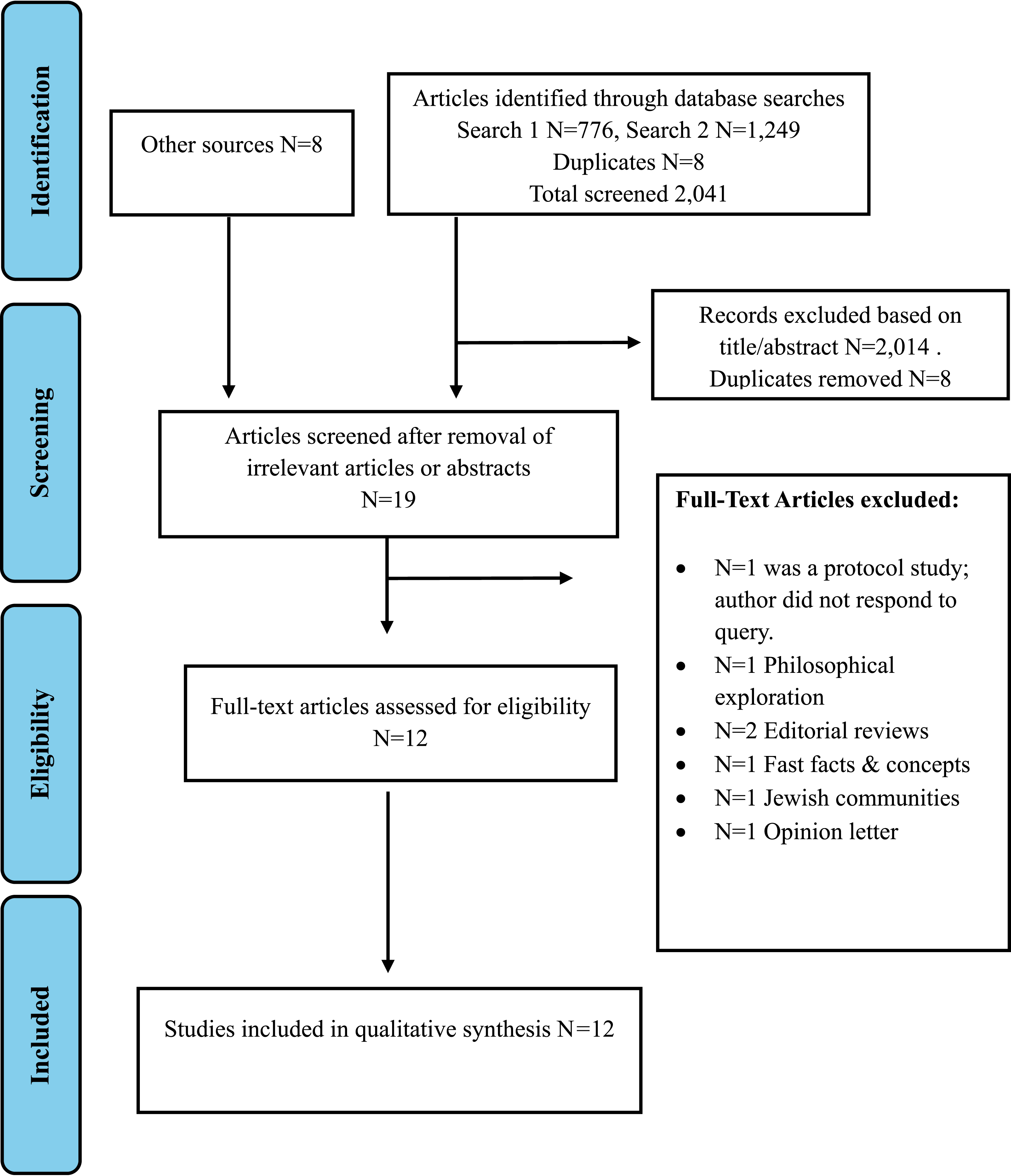
The SANRA guidelines, which stands for the Scale for the Assessment of Narrative Review Articles with a 6-item scale, was used. 22 The reviewer is a U.S.-trained palliative medicine physician with over 15 years of experience working in an academic setting in the United Arab Emirates (UAE).
The SPIDER framework, which stands for Sample, Phenomenon of Interest, Design, Evaluation, and Research type, was employed to guide the analysis of the chosen articles. Each article was analyzed based on these dimensions to ensure a comprehensive understanding of the research landscape.23-25
Results
The studies range in publication dates from 2009 to 2024. The initial search on April 11, 2024 yielded a total of 2041 articles. After the removal of 8 duplicate articles, the total number of articles was 2033. Once the searches were complete, the references underwent sorting and management. All abstracts were reviewed. Following the abstract review, studies meeting inclusion criteria were selected. Studies included were systematic reviews n = 2, literature reviews n = 2, mixed methods n = 3, qualitative n = 4, and quantitative n = 1.
The study selection process is outlined in flow chart format (Figure 1). After the initial screening using the search engines described and the title search in addition to abstract review, predefined inclusion and exclusion criteria was used to identify the relevance to the review objectives uncovering a total of 2025 articles. Of the 2025 articles included, eleven full-text articles met inclusion criteria. Hand-searching of the reference lists from the full text articles revealed a further 8 in-text references. This resulted in a total 19 full text articles for review. Of the final 19 full-text articles for review, 7 full-text articles were removed from the qualitative synthesis, given n = 1 protocol study and the author did not respond to query, n = 1 was a philosophical exploration, n = 2 were editorial reviews, n = 1 was fast facts, n = 1 was regarding Jewish communities and n = 1 was an opinion letter.
Themes and Subthemes
Articles Selected for Review.

Abbreviations: ACP, advance care planning; CASP, critical appraisal skills programme; CDD, cancer diagnosis disclosure; DD, diagnosis disclosure; FC, family caregivers; HCP = healthcare provider.
Theme 1: Reluctance Driven by Cultural, Religious, and Emotional Factors Leading to Non-Disclosure Requests
Theme 1 reflects a preference for nondisclosure linked to (a) the influence of the family unit, (b) hopes and beliefs in miracles, and (c) concerns about hastening death and its implications (Figure 2). Patients often resisted accepting their diagnosis, instead opting for aggressive treatments fueled by a hope for a “miracle.”
3
As a result, families of Muslim patients frequently requested non-disclosure and withheld medical information, concerned that disclosure could accelerate death. This inclination to protect patients’ optimism led family members to assume roles as “conveyors of hope,” choosing to withhold information, which in some cases prolonged the dying process.
3
Circular diagram representation of themes and subthemes across 12 studies.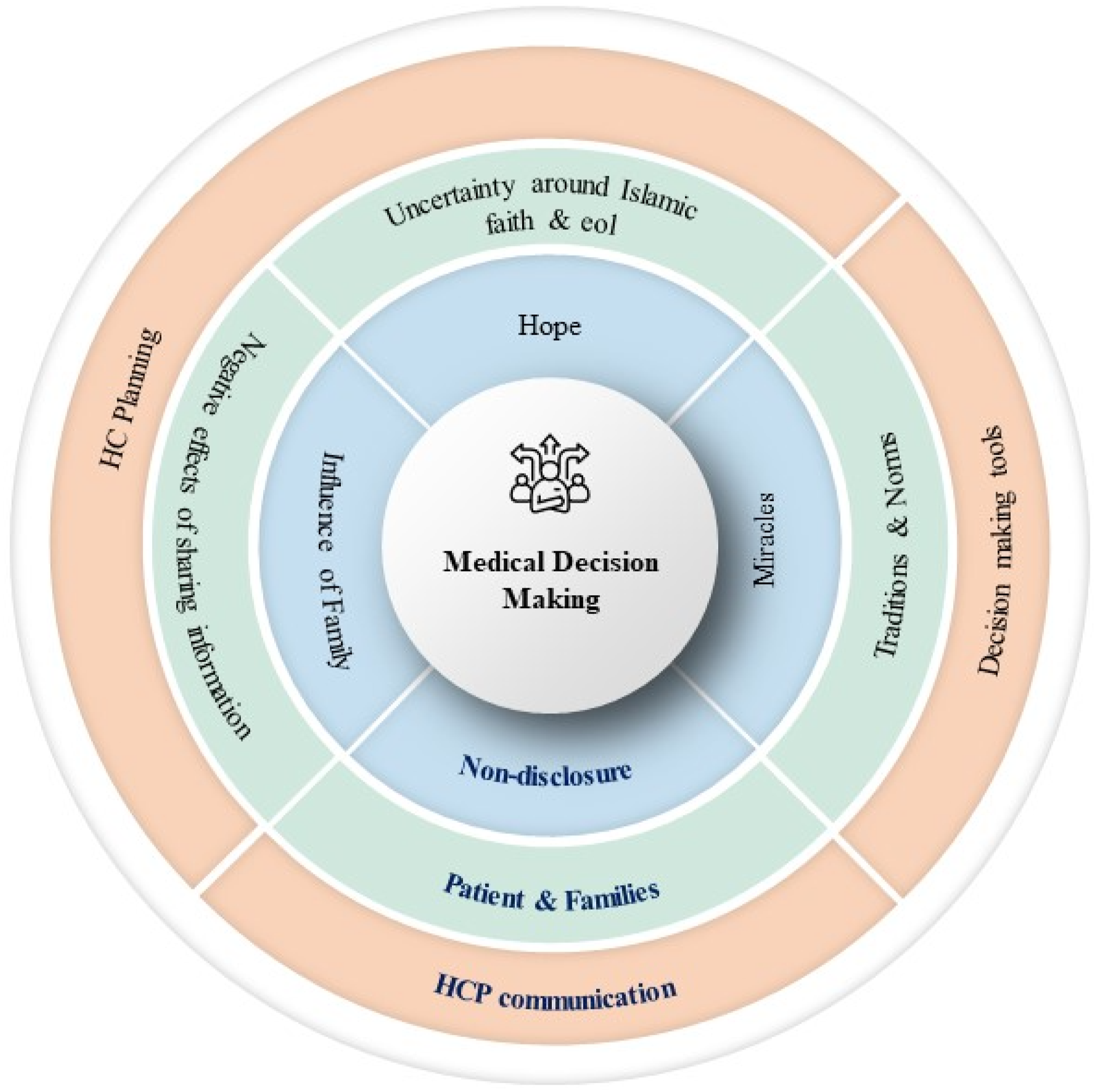
This non-disclosure practice created tension with healthcare providers, as multiple studies illustrated the impact of disclosure decisions on care goals in Muslim communities. 26 Abdullah et al (2020) documented conflicts around diagnosis disclosure and the hope for a “miracle,” echoing findings by Mendieta and Buckingham (2017), Piracha et al (2024), and Bahramnezhad et al (2018). Gustafson and Lazenby (2019) highlighted the role of the “whole family” as a decision-making entity contributing to nondisclosure, while Al-Amri (2009) emphasized the family’s central role in clinical decisions.
Theme 2: Centered Around the Patient and Family
Theme 2 centers around the family unit, their traditions and norms, uncertainty around Islamic faith and view on end-of-life care in addition to concerns around the negative effects of sharing medical information which could result in psychological distress and hastening death (Figure 2). Additionally, the studies highlighted the influence of cultural norms, traditions, and religious beliefs on decision-making processes within Muslim families, impacting the delivery of palliative and hospice care.3,8,28 Specifically, the literature emphasized the importance of recognizing the “whole family” as a decision-making unit, rather than solely focusing on the patient. 20 In many Muslim communities, decisions about end-of-life care are made collectively, with input from multiple family members. 29 This collective decision-making process can be influenced by cultural values, religious beliefs, and perceptions of illness and death.3,29-31
Theme 3: Healthcare Provider Communication and Its Impact on Disparities in Palliative Care Access
Theme 3 examines the critical role of healthcare providers (HCPs) in effectively communicating with patients and families and how this communication influences healthcare planning, decision-making, and ultimately, access to palliative care services (Figure 2). Studies indicate contrasting perspectives among patients regarding information disclosure. 32 For instance, Zafar et al (2016) found that nearly half of patients with advanced cancer preferred that HCPs withhold certain information if disclosure might diminish their hope. 33 However, despite this preference for limited disclosure, 90% of these patients still wanted to be presented with all therapeutic options, including palliative care. This preference led to complexities in treatment planning and extended decision-making processes, as patients sought comprehensive care without necessarily wanting full transparency.3,33
Conversely, Al-Amri (2009) reported that in a different patient population, 100% of individuals expressed a desire for HCPs to openly share diagnoses and treatment plans, underscoring a nuanced relationship between family involvement and information sharing. Here, rather than withholding information, HCPs were encouraged to communicate openly, with the understanding that family members play a significant role in interpreting, managing, and supporting clinical decisions. This finding highlights how cultural contexts shape communication preferences, where the family’s role is integral to aligning treatment choices with patient and family values.
Additionally, Nayfeh (2024) observed that end-of-life care quality tends to be lower for Muslim patients compared to non-Muslim patients, which points to disparities in healthcare delivery. These disparities are often exacerbated by cultural misunderstandings between HCPs and Muslim families. Some Muslim families, for instance, may hesitate to engage with palliative care services due to misconceptions about its objectives or doubts about the cultural sensitivity of the care provided.
This review emphasizes the importance of culturally competent, compassionate care in reducing these barriers. For HCPs, fostering trust and aligning communication with the cultural and religious expectations of Muslim families is essential for supporting patient and family-centered care goals. Addressing these factors can help mitigate disparities and improve palliative care experiences for Muslim patients and their families. Key themes in the literature reveal that disclosure practices within Muslim communities are deeply influenced by cultural, religious, and emotional factors, while effective healthcare provider communication is essential for navigating complex decision-making processes (Figure 2).
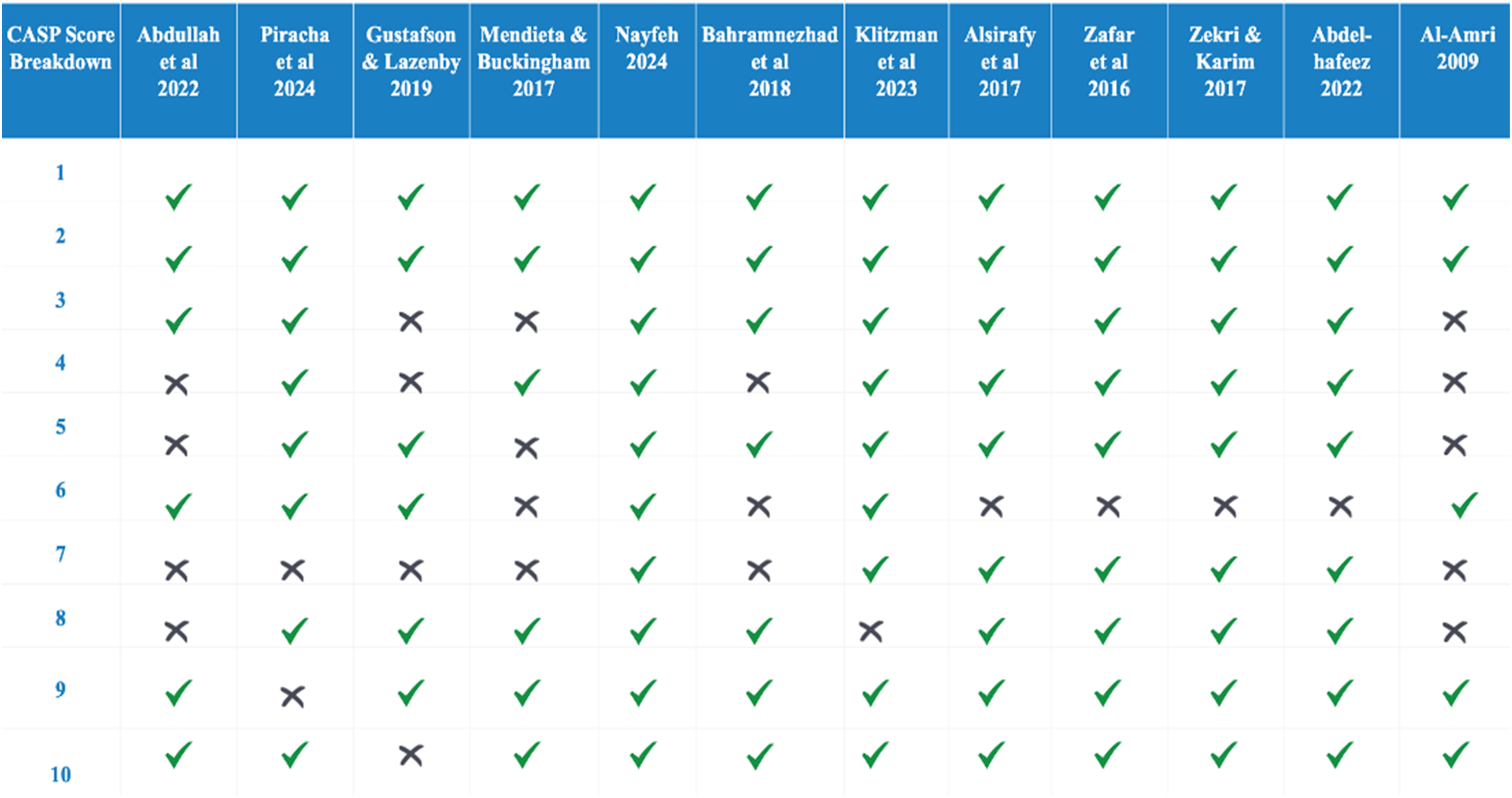
Critical Appraisal Skills Programme (CASP) Score
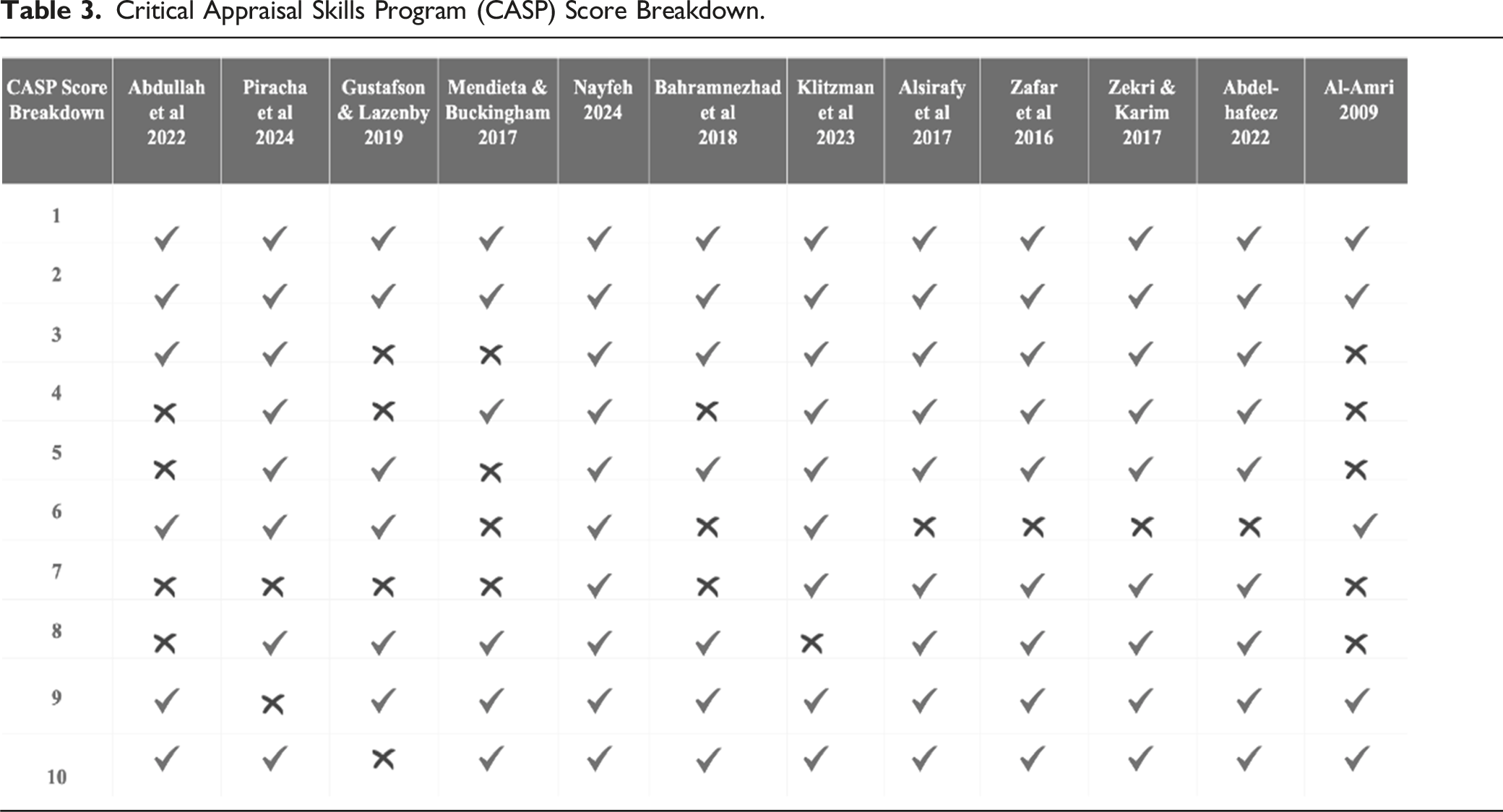
Critical Appraisal Skills Program (CASP) Score Breakdown.
Discussion
This narrative review shows the complex nature around medical decision-making in the Muslim population approaching end-of-life. It reveals the patients’ families are often the main communicator and request for non-disclosure or withholding of medical information in fear of loss of hope and psychological distress therefore resulting in conflict between HCP and the family. The review identified 12 papers that met the study criteria, shedding light on the intricacies of the decision-making processes and disclosure practices within Muslim populations. Three core themes emerged, which include the (1) requests for non-disclosure, (2) portrayal of the patient and family in Muslim population as the “whole family,” and (3) healthcare provider communications. These themes encompassed other subthemes from the articles surrounding (1) very high levels of hope; (2) belief in miracles; (3) the influence of the family unit on decision making; (4) tradition and norms; (5) uncertainty around the Islamic faith and end-of-life care; (6) the negative effects associated with the sharing of information around prognosis and diagnosis; (7) healthcare planning; (8) decision making tools; and (9) HCP communication (Figure 2).3,13,19,20,26,27,30,31,33-35,44 These subthemes call attention to the importance of understanding the attitudes and beliefs of Muslim populations, as they significantly influence the decision-making process regarding end-of-life care.
One notable finding across the literature under review is the desire among patients for information regarding their diagnosis and prognosis. This centers around the second theme of patient and families where the sharing of information would exert negative effects. 34 This finding challenges the prevailing stereotype of Muslim populations favoring non-disclosure in healthcare settings. It also suggests that when investigating attitudes towards palliative care issues within regions where Muslim communities are not marginalized, stereotypes commonly held in Western contexts may break down. Patients frequently express a need for clarity and understanding, emphasizing the critical role of effective communication between healthcare providers and patients from diverse cultural backgrounds.27,34 The identified themes in decision-making processes underscore the significant influence of cultural and religious beliefs on healthcare preferences within Muslim communities. By examining studies set in both Muslim-majority countries and regions where Muslims are not marginalized, this review aims to provide insights into how cultural and religious contexts shape these preferences and challenge stereotypes present in Western narratives.
The concept of hope and belief in miracles related to the theme of non-disclosure, emerges as a significant factor shaping decision making, reflecting the intertwining of faith and healthcare choices.3,35 Additionally, the influence of family dynamics on decision making cannot be overstated, as familial relationships and communal decision making often play pivotal roles in healthcare matters. 20 Tradition and norms within Muslim communities also impact healthcare decision-making processes. 3 These cultural frameworks may either support or hinder the acceptance of medical interventions and disclosure practices. This narrative review examines how decision making within Muslim communities are influenced by disclosure practices regarding the health status of a sick family member and their impact on palliative care delivery, prolongation of the dying process, and conflicts with the healthcare provider. Understanding these traditions is crucial for healthcare practitioners to navigate cultural sensitivities and provide patient-centered care. Furthermore, uncertainty surrounding the Islamic faith and its implications for end-of-life care pose unique challenges for both patients and healthcare providers. The intersection of religious beliefs, cultural practices, and modern medical ethics requires careful consideration to ensure respectful and dignified end-of-life care that aligns with a patient’s values and preferences.
Strengths and Limitations of the Review
The CASP score is an indicator of a stronger methodology and a lower risk of bias in several studies. It indicates that the results are consistent and validates the findings facilitating a conclusion which is accurate. Despite variations in methodological quality, all of these studies offer valuable insights into the intricate dynamics of family, cultural beliefs, and end-of-life care practices within Muslim communities. These findings necessitate further research and the development of culturally sensitive interventions aimed at improving care outcomes for Muslim patients and their families.
The studies included provided valuable insights into the complexities surrounding decision making and disclosure practices among Muslim patients, shedding light on the impact of these factors on palliative care delivery and end-of-life care. These studies employed various methodologies, including qualitative interviews, systematic reviews, and mixed-method approaches, allowing for a comprehensive exploration of the research problem from different angles. This diversity enriched the findings by providing multifaceted perspectives on decision making and disclosure practices within Muslim communities. Many of the included studies demonstrated a nuanced understanding of cultural and religious beliefs, effectively capturing the intricacies of the decision-making process within Muslim families. By acknowledging and respecting these cultural nuances, the studies offered valuable insights into the unique challenges faced by healthcare providers in delivering culturally competent care. It was discovered that several studies were conducted in Muslim-majority countries or regions with significant Muslim populations, ensuring the contextual relevance of the findings. This contextualization allowed for a deeper understanding of how cultural, religious, and social factors shaped decision-making and disclosure practices in specific cultural contexts. The studies reviewed provided CASP scores, offering transparency regarding the methodological rigor and quality of the research. This critical appraisal enhanced the credibility of the findings by allowing readers to assess the trustworthiness of the evidence presented.
Many of the studies exhibited sampling bias, with small sample sizes or convenience sampling methods that may not have adequately represented the diversity of Muslim populations. This limitation restricted the generalizability of the findings and may have overlooked the perspectives of underrepresented groups within Muslim communities. Moreover, while some studies received high CASP scores, others had methodological shortcomings, such as a lack of clear inclusion criteria, inadequate sample sizes, or limited data analysis techniques. These limitations may have compromised the validity and reliability of the findings, warranting cautious interpretation. Furthermore, the exclusion of non-English language articles and the focus on studies conducted in specific geographic regions may have introduced language and cultural biases into the review. This limitation hindered the inclusivity of perspectives from diverse Muslim populations worldwide, potentially overlooking valuable insights from non-Western contexts.
Implications and Recommendations
The reviewed literature highlights the complexities associated with sharing information about prognosis and diagnosis within Muslim populations. The reluctance to disclose diagnoses and prognosis within Muslim families, as discussed in several studies reflects deeply ingrained cultural and religious beliefs.14,36-40 The emphasis on protecting hope and the pursuit of miracles can prolong the dying process, impacting both patients and families.2,13,40 Moreover, cultural norms and religious beliefs shape preferences for aggressive medical interventions and influence attitudes towards hospice care.10,12 While transparency is valued in Western healthcare systems, cultural and religious factors may sometimes lead to reluctance in disclosing sensitive medical information. Understanding the potential negative effects of information sharing is crucial for striking a balance between respecting a patient’s autonomy and honoring cultural norms. Literature reviews such as this one can serve as a valuable resource for healthcare practitioners working in multicultural settings. Insights gleaned from these studies can provide practical guidance for fostering effective communication, navigating cultural differences, and delivering culturally competent care. By acknowledging and addressing the diverse needs and preferences of Muslim populations, healthcare providers can enhance patient trust and satisfaction while promoting positive health outcomes.
Moving forward, there will be a pressing need to further explore the role of the Muslim family in healthcare decision-making processes. Emphasizing the concept of “relational autonomy,” which acknowledges the interconnectedness of familial relationships and its impact on individual decision making, can deepen our understanding of cultural dynamics within healthcare settings.
29
The “whole family” approach to decision making, prevalent in Muslim communities, underscores the significance of family involvement in end-of-life care decisions.
41
Family members often serve as gatekeepers of information, contributing to the tension between healthcare providers and families.
20
Recognizing the collective decision-making process within families is crucial for providing patient-centered care that aligns with cultural values.
29
Future research should aim to elucidate the nuances of the decision-making processes within diverse Muslim communities, taking into account variations in cultural practices, religious interpretations, and social contexts. This review might suggest that the preference for non-disclosure of diagnosis and prognosis within Muslim populations such as those in the UAE may vary across subpopulations based on the above results, highlighting the need for further investigation. Taking this into account, the following are recommended: • Integrate “Relational Autonomy” into Healthcare Practices: Emphasizing the concept of “relational autonomy” can deepen our understanding of the decision-making processes within Muslim families.
29
Healthcare practitioners should recognize the interconnectedness of familial relationships and involve the entire family in end-of-life care decisions, respecting cultural values and preferences. Subsequently, a family-centered model for medical decision making is recommended. • Promote Research on Decision-Making and Disclosure Practices: Continued research is essential to further explore the complexities surrounding decision-making and disclosure practices within diverse Muslim communities similar to subpopulations within the UAE. Future studies should employ rigorous methodologies and ensure adequate representation of diverse Muslim populations to enhance the generalizability and applicability of the findings. • Develop Culturally Sensitive Decision-Making Tools: Given the influence of cultural and religious beliefs on healthcare preferences within Muslim communities, there is a critical need to develop decision-making tools that are culturally sensitive and tailored to the unique needs of Muslim patients and their families. These tools should consider the identified themes such as hope, belief in miracles, and the influence of family dynamics on decision making. • Enhance Communication and Education Efforts: Healthcare providers should prioritize effective communication with Muslim patients and their families, providing clear and culturally appropriate information about diagnosis, prognosis, and treatment options. Educational initiatives aimed at healthcare professionals should focus on increasing cultural competency and understanding of the Islamic beliefs and practices related to healthcare decision making. • Address Barriers to Palliative Care Access: Significant disparities exist in access to and utilization of palliative care services among Muslim populations. Efforts should be made to address cultural misunderstandings and misconceptions surrounding palliative care, ensuring equitable access to quality end-of-life care for all patients, regardless of cultural background.
Conclusion
End-of-life care is influenced by several factors in Muslim populations. While common subthemes include providing hope, wishing for a miracle, and the desire to protect their loved one from negative influences, the patients themselves have often stated that they would like to know their prognosis and diagnosis. This review has demonstrated a need for future studies to look into end-of-life care among different Muslim populations as well as the impact of non-disclosure on medical decision making. Non-disclosure can lead to conflict around the decision-making process and increase strain on the healthcare provider, ultimately leading to a prolongation of the dying process, which can further result in non-beneficial treatments.13,35 Significant disparities exist in access to and utilization of palliative care services among Muslim populations, exacerbated by cultural misunderstandings and misconceptions.8,28 Addressing these barriers will require culturally competent approaches that acknowledge and respect the beliefs and preferences of patients and families. 42 Developing tools to assess these factors will further help address the goals of care among Muslim populations and the intricate nature of hope within Muslim communities, emphasizing its importance in ultimately finding meaning and fostering a balance at the end of life.43,45 The literature review further illustrates the research problem concerning the discrepancy between a patient’s understanding and their family members’ knowledge of terminal diseases, as well as prevalent non-disclosure practices and the consequential loss of hope among families upon learning the prognosis. Emphasizing the critical importance of addressing these challenges, the review underscores the necessity of enhancing the quality of end-of-life care for Muslim patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
AI or AI-Assisted Technologies
The author did not use AI or AI-assisted technologies in the writing process.