
Abstract
Key Message
This study demonstrates clinical characteristics of patients who received life-supporting measures via VV-ECMO at the intensive care unit due to acute respiratory distress syndrome but were later withdrawn from life-sustaining treatment. The results showed that palliative care consult is directly associated with an increased duration of treatment with VV-ECMO and longer duration of ICU stay.
Introduction
With the advancement of medical technology and increasing availability of state-of-the-art life-extending equipment such as extracorporeal membrane oxygenation (ECMO), the narrow window of making a conscious decision about the goal of care by critically ill patients’ advance directives has significantly widened.1-3 Among different ECMO modalities, the veno-venous ECMO (VV-ECMO) has been exclusively used for patients with acute respiratory distress syndrome (SARS).1,4-6 However, in critically ill patients with poor prognosis, extending the duration of receiving life supporting measures via treatment with EMCO, might not seem a very cost-effective way of utilizing the healthcare system resources 7 and has been even ethically debated.8,9
A medically unjustifiable continuation of care in these cases, also referred to as “a bridge to nowhere”, is burdensome, costly to the healthcare system and emotionally overwhelming to the patients' next of kin. Nevertheless, withdrawal of life-sustaining treatments (WOLST) such as that with VV-ECMO is not a straightforward decision to attain, not by the healthcare providers or by the patient’s advance directives. Palliative care consult (PCC) uses an inter-disciplinary patient/family-centered approach focusing on the improvement of patient’s and/or their family’s quality of life rather than only focusing on life-extending measures.10,11 Despite its proven benefits in improving the quality of life of patients, increasing the satisfaction of their families and healthcare providers, and decreasing the costs of care through more efficient comfort measures,12-15 PCC seems to be underutilized in the management of patients with critical illnesses.16-18 Additionally, few studies have demonstrated the potential benefits of PCC among patients receiving treatment with ECMO,19-21 and none among those on VV-ECMO. Hence, we conducted this study to demonstrate the clinical characteristics of critically ill patients receiving VV-ECMO and to compare factors associated with WOLST among those receiving PCC and those not receiving PCC.
Methods
Study Design
This was a retrospective observational study in a tertiary care hospital affiliated with the University of Texas Health Science Center at Houston, TX. The institutional review board of our hospital approved the study protocol and exempted the investigators from obtaining an informed consent due to the retrospective nature of this investigation and collection of the data in an unidentifiable manner.
Patients
Electronic medical records of adult patients (age ≥18 years old), who required VV-ECMO for any clinical indications between January 1, 2015, and October 31, 2021, were reviewed. Patients were included if they were on VV-ECMO for more than 48 hours and the WOLST with ECMO occurred during the same ICU stay. Those who received VV-ECMO for less than 48 hours were excluded, due to uncertain causes of death.
Palliative Care Consultation
At our center, PCC is provided through a joint effort between physicians, physician assistants, social workers, case managers, and chaplains. The main objective of PCC is to facilitate an interdisciplinary approach to planning the goal of care between the primacy team and other individuals involved in the care of the patient, managing the end-of-life symptoms, and providing psychological support to the patient and/or their families. Additionally, PCC was mainly engaged in sufficient pain management, addressing non-pain related symptoms, clarifying the goal of care to the advance directive, help with the selection of surrogate decision maker or treatment preference, psychosocial or spiritual support, and education about the patient’s critical condition and its pathological course leading to such poor prognosis.
Data Collection
Data was collected on demographics (age and gender), code status (full code, do not intubate, do not resuscitate, do not intubate or resuscitate), clinical characteristics (comorbidities, indication for VV-ECMO, life-supporting measures [vasopressors or inotropic agents, continuous renal replacement therapy, mechanical ventilation, or non-ECMO cardiac care]), the main reason(s) for WOLST (futility, extreme pain, poor quality of life, or decision maker’s wish), duration of ICU stay and supportive measure with VV-ECMO before and after PCC, and characteristics of PCC. In terms of PCC, we documented the number of visits and the communication modes between PCC team members and the patient’s family or advance directives, recorded the time interval between the initiation of VV-ECMO, PCC, and/or WOLST.
Outcome Measures
The primary endpoint of this study was to determine the difference in demographics, clinical characteristics, hospital timelines, and causes of WOLST between patients on VV-ECMO receiving PCC and those not receiving PCC. The secondary endpoint of this study was to demonstrate characteristics of PCC visits and its relationship with ECMO and ICU stay.
Statistical Analysis
Data were analyzed using STATA/IC 14.2 (StataCorp, College Station, TX). Comparison between PCC group and non-PCC group was done using Chi-squared test for categorical variables and Student’s t-tests for continuous variables. Data are presented as number (%) or mean ± standard deviation (SD) when appropriate. A P value was deemed statistically significant at < .05.
Results
Demographics, clinical characteristics, and primary in-hospital interventions among patients undergoing treatment with ECMO.
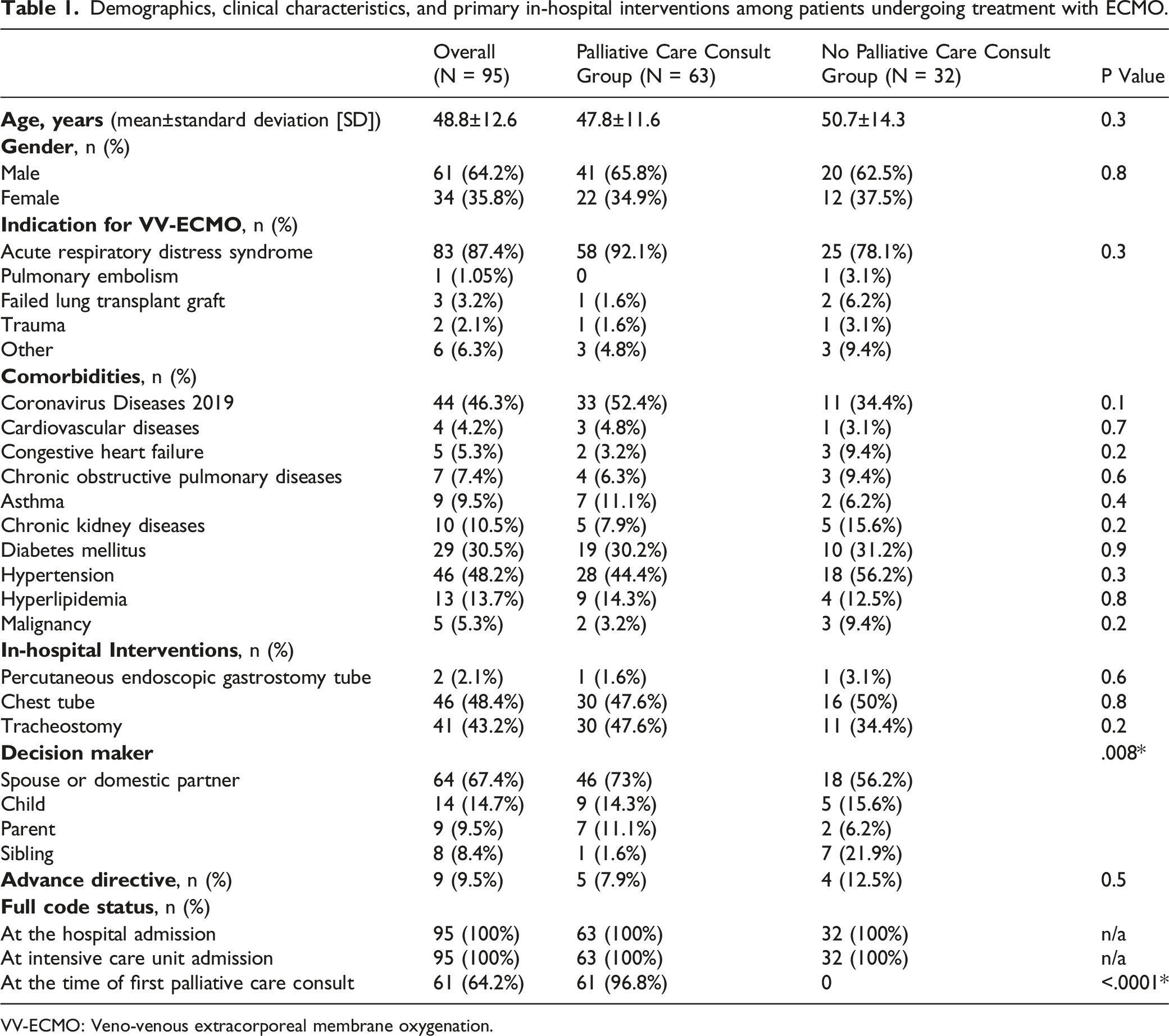
VV-ECMO: Veno-venous extracorporeal membrane oxygenation.
Characteristics of Patients at the Time of Receiving PCC
Code status and life supportive measures for patients at the time of palliative care consultation (PCC).
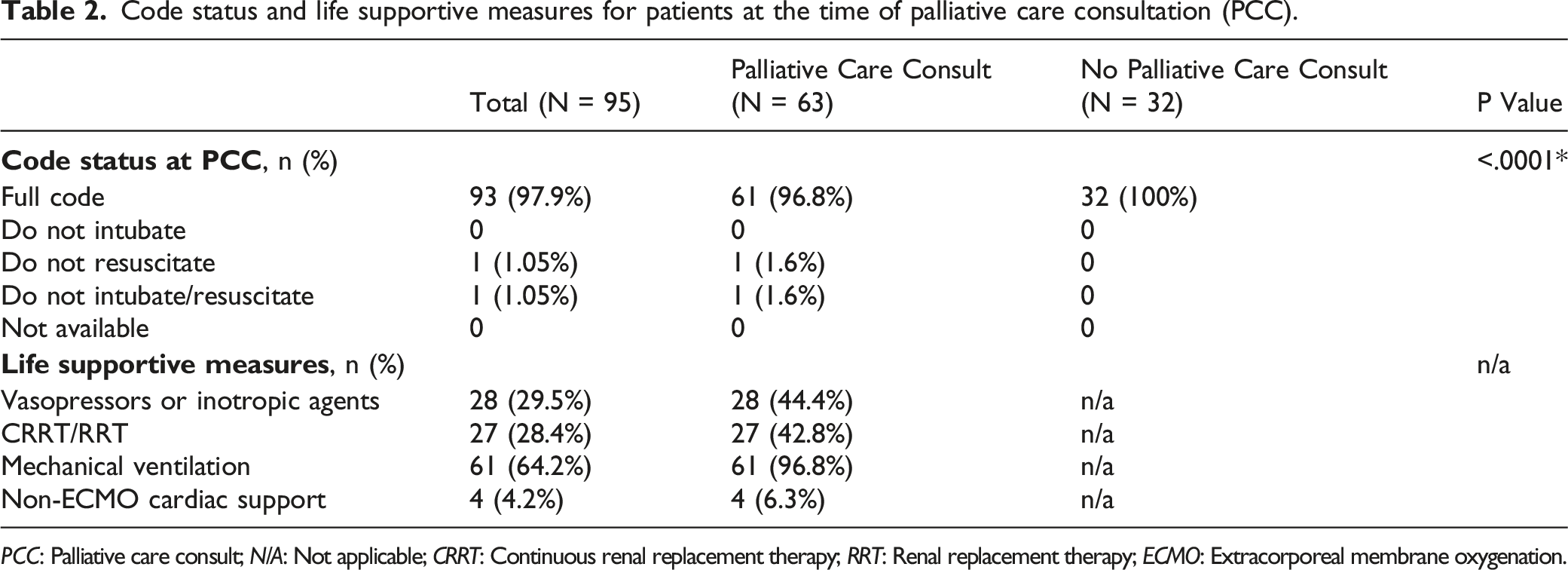
PCC: Palliative care consult; N/A: Not applicable; CRRT: Continuous renal replacement therapy; RRT: Renal replacement therapy; ECMO: Extracorporeal membrane oxygenation.
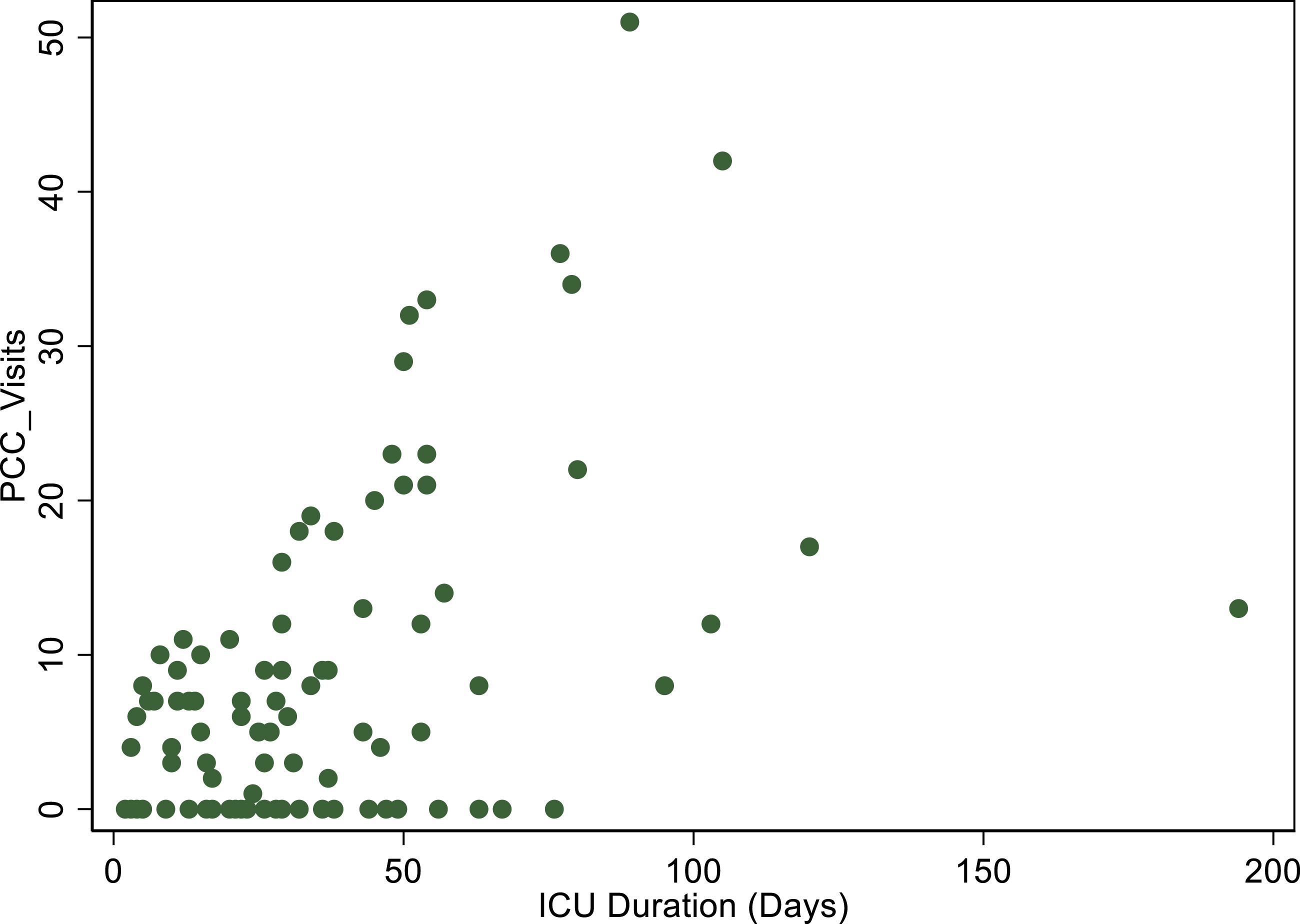
Relationship between length of ICU stay and the number of visits for palliative care consult.
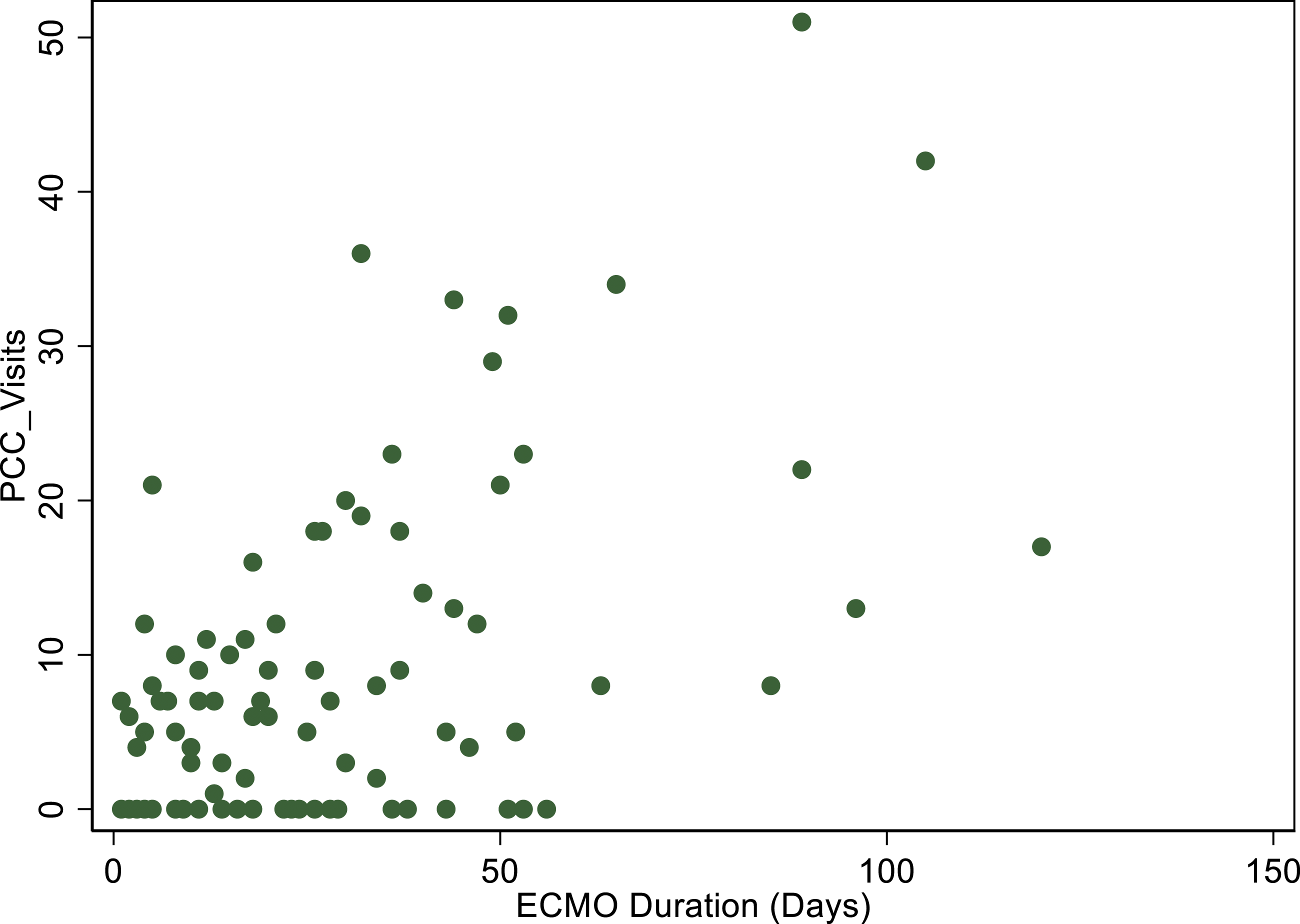
Relationship between duration of support with extracorporeal membrane oxygenation and the number of palliative care visits.
Comparison of Patients’ Characteristics at the Time of Withdrawal of Life-sustaining Treatment
Comparison of critical care measures and life-sustaining treatments between patients with and without PCC at the time of WOLST.
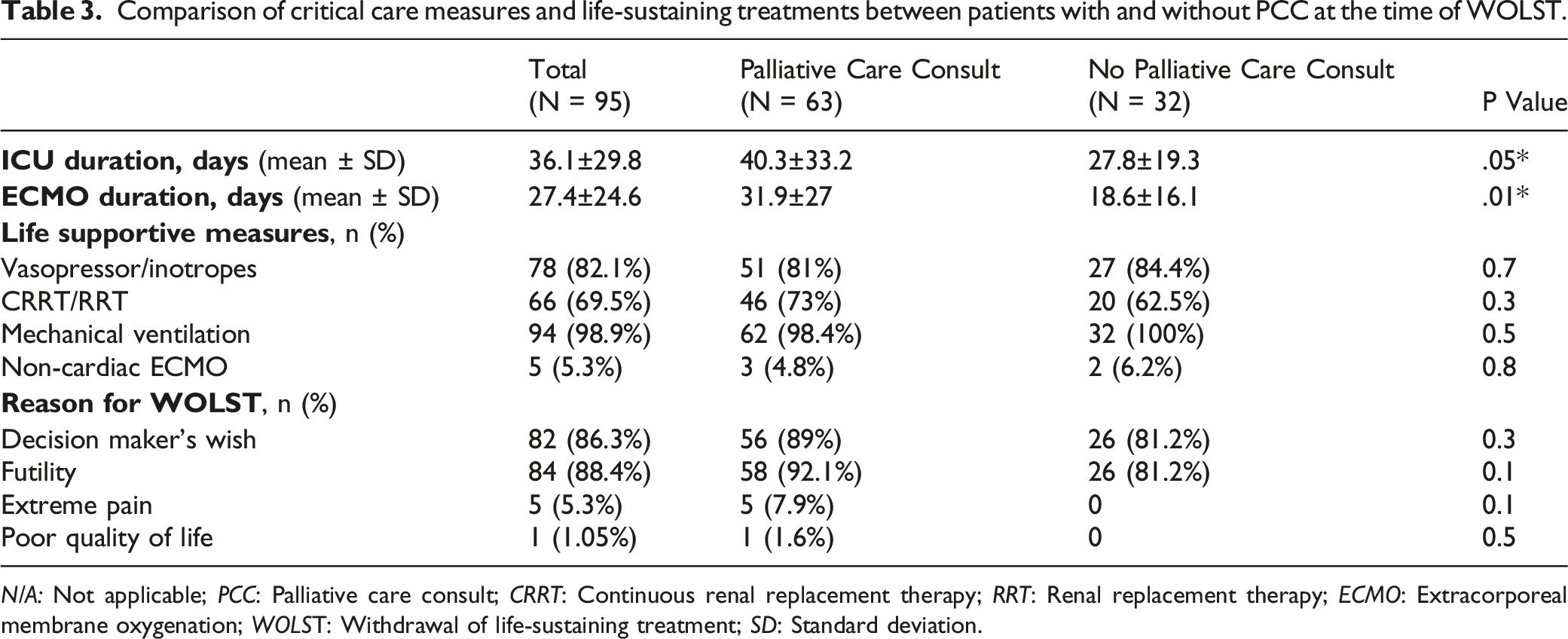
N/A: Not applicable; PCC: Palliative care consult; CRRT: Continuous renal replacement therapy; RRT: Renal replacement therapy; ECMO: Extracorporeal membrane oxygenation; WOLST: Withdrawal of life-sustaining treatment; SD: Standard deviation.
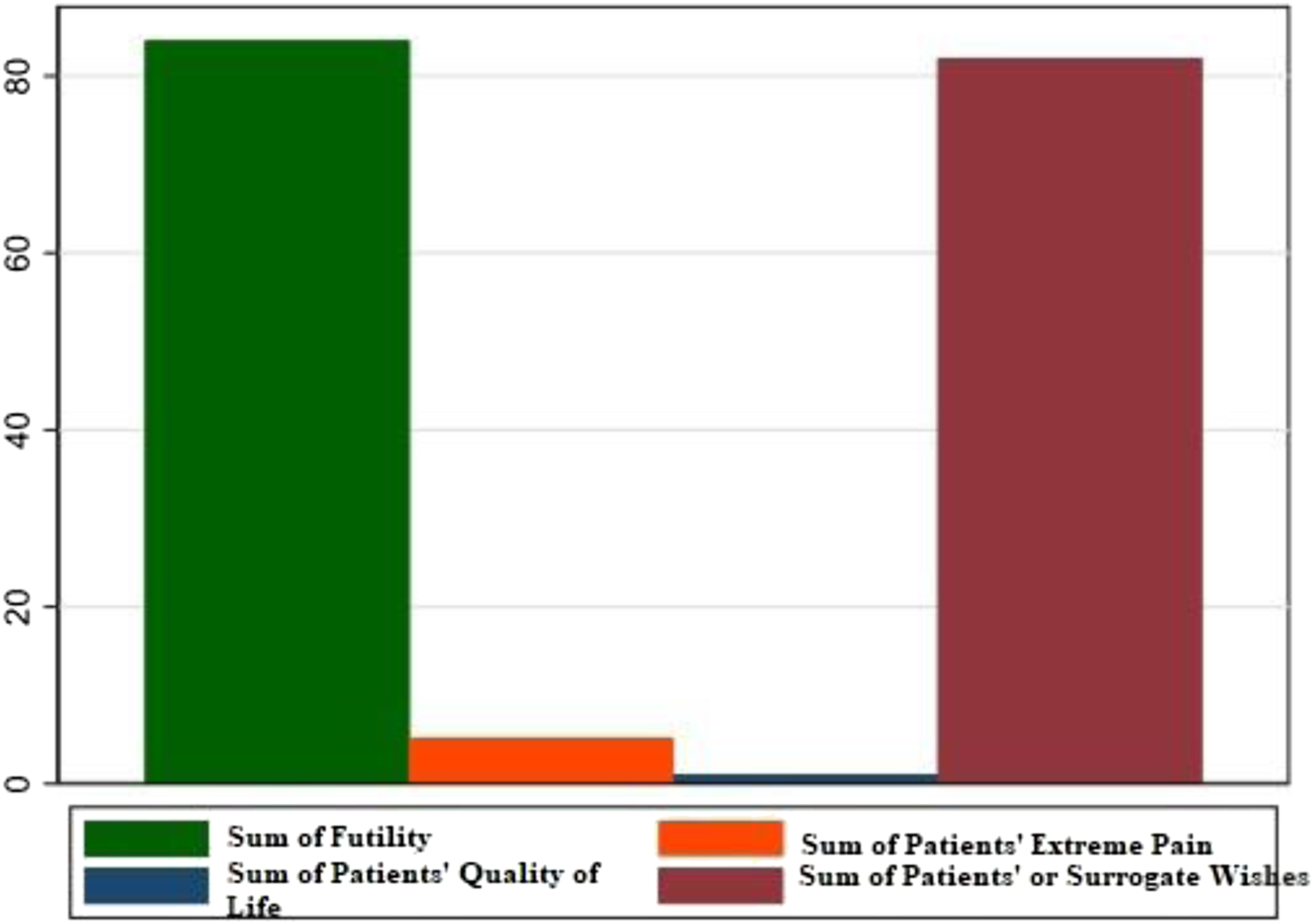
Underlying reasons for the withdrawal of life-sustaining treatment among patients with and without palliative care consult.
Characteristics of PCC
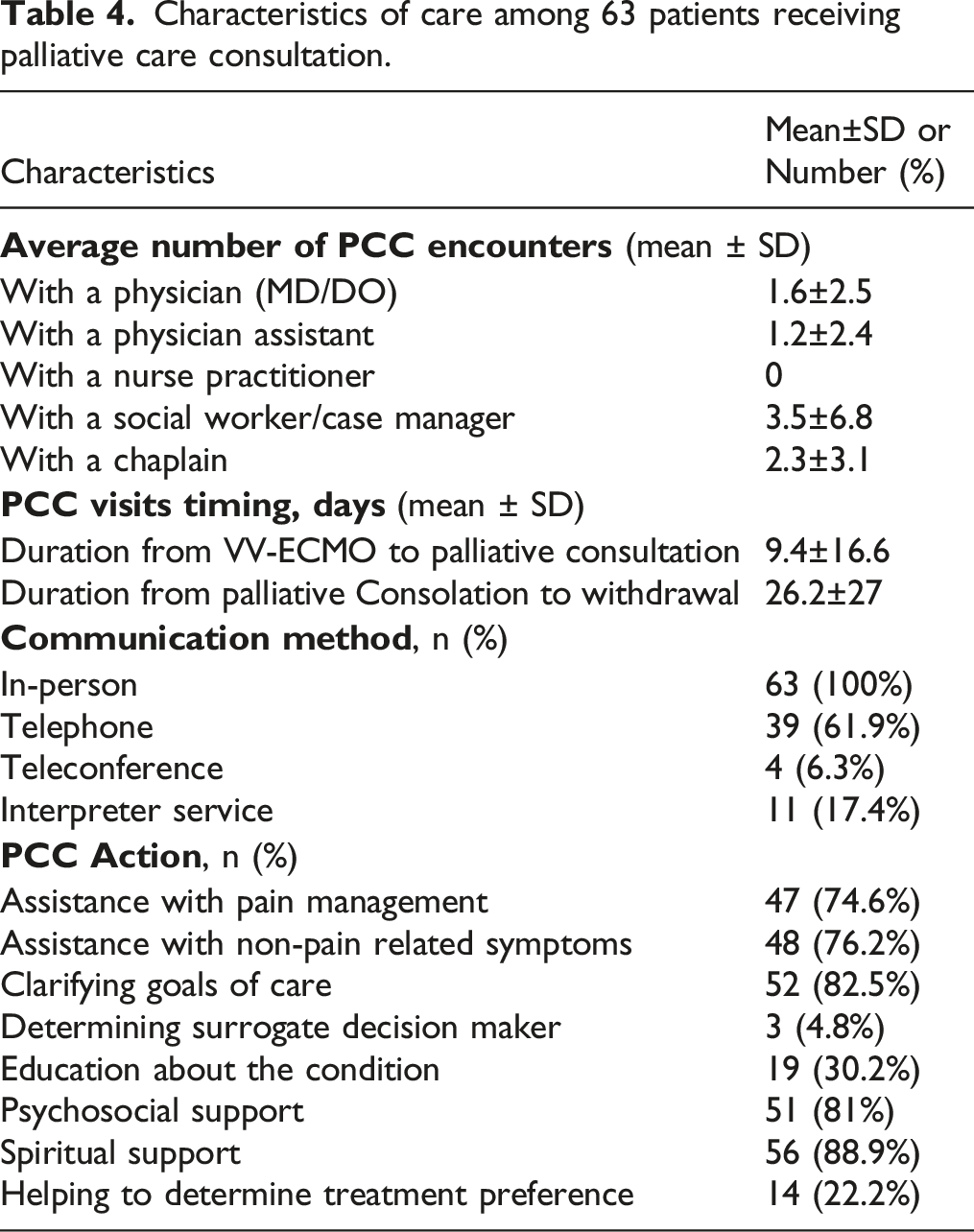
Characteristics of care among 63 patients receiving palliative care consultation.
Discussion
We described the characteristics of 95 patients who received supportive measures with VV-ECMO and for whom the decision to withdraw the treatment with ECMO was made by an advanced directive. Our study showed that the number of PCC visits was directly associated with the duration of ECMO support and the length of ICU stay. However, the underlying reasons for WOLST was not different between VV-ECMO patients, who received PCC and those who did not.
To the best of our knowledge, this is the first study comparing clinical parameters between patients on life-sustaining measures through VV-ECMO. A previous study on 91 deceased patients who had been withdrawn from support with VA- ECMO showed a median duration of 4.0 days (interquartile range 8.8 days) for ECMO support, which was significantly longer for patients who received PCC compared to those who did not (8.8 days vs 2.0 days). Additionally, patients receiving PCC who received early consultation (<3 days) had significantly shorter duration of support with VA-ECMO compared to those receiving consultation at a later time after initiation of ECMO support (>3 days) (7.6 days vs 13.5 days). 21 In our study, the average time interval from initiation of treatment with VV-ECMO to the first PCC encounter was 9.4 ± 16.6 days and the time interval from the first PCC encounter to the WOLST was 26.2 ± 27 days. Although PCC has been reported to be underutilized in patients requiring ECMO,22,23 its direct correlation with a longer duration of treatment seems to be in debate. On one hand, PCC has been shown to educate the surrogates on the goal of care, which is essentially beneficial for those making decisions about life-sustaining measures for patients with complex medical conditions. On the other hand, PCC engagement in the management of pain and non-pain related symptoms might inadvertently result in the prolongation of decision-making process by the patients or their advance directives on whether to continue or withdraw the life-sustaining measures. Hence, it is not surprising to see that PCC has a paradoxical impact on the duration of treatment with ECMO, and in turn, on the duration of ICU stay among patients with poor prognosis, especially those with ARDS or hemodynamic instability. Nonetheless, patients receiving treatment with ECMO constitute a population of patients for whom PCC provides an invaluable educational resource for decision-making as well as parallel psychosocial support.
In more than 80% of our cohort and specifically 90% in the PCC group, the decision to withdraw VV-ECMO was due to futility and extreme pain. Additionally, in majority of the cases, the role of PCC was clarification of the goal of care and symptom management, with non-pain related symptoms as important as pain management. More than 50% of the patients in the PCC group and about 30% in the non-PCC group had COVID-19 as the underlying causes of ICU admission. Previous studies have shown that engagement of PCC to address the goal of care in COVID-19 patients requiring ECMO is associated with a higher chance of changing the code status from full-code to the Do not resuscitate/DNR status.22,24 Similar to our study, offering PCC has been associated with a longer duration of ICU stay. Besides the fact that COVID-19 was an evolving condition with uncertain prognosis at the time of collecting the data for this study, utilization of ECMO and PCC was also in its infancy for COVID patients requiring ICU level of care. While clarifying the goal of care seems as important as a task as symptom management to the advance directives of the patients at the end of life, this might be one of the explanations for the increased length of ICU stay and the longer duration of life-sustaining treatment with ECMO.
Limitations
Our study has several limitations, which need to be considered when interpreting its results. As a retrospective study, it is not feasible to obtain data on all the parameters affecting the decision to withdraw support with VV-ECMO. Particularly, data is lacking on why PCC has been underutilized for patients with poor prognosis. Additionally, due to the conduction of this study in a single hospital, our study findings have limited generalizability to other inpatient settings. While our exclusive inclusion of patients on VV-ECMO makes study findings not applicable to those requiring VA-ECMO, it makes our results amenable for a population of ARDS patients on VV-ECMO which might benefit from PCC.
Conclusion
Our study demonstrated the clinical characteristics of patients who were withdrawn from life-sustaining treatment with VV-ECMO showing that the number of PCC visits was directly associated with a longer duration of ECMO support and length of stay. Pain and futility were the main indications for WOLST among most of the patients. However, it remains to be determined which VV-ECMO patients benefit the most from PCC and what the best timeline would be.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.