
Abstract
Introduction
Following the historic Canadian legislation on medical assistance in dying (MAiD) in 2016, many implementation challenges and ethical quandaries have formed the focus of further scholarly investigation and policy revisions. Of these, conscientious objections held by some healthcare institutions have involved relatively less scrutiny, despite indicating possible hurdles to the universal availability of MAiD services in Canada.
Methods
In this paper, we contemplate potential accessibility concerns that pertain specifically to service access, with the hope to trigger further systematic research and policy analysis on this frequently overlooked aspect of MAiD implementation. We organize our discussion using two important health access frameworks: Levesque and colleagues’ Conceptual Framework for Access to Health and the Provisional Framework for MAiD System Information Needs (Canadian Institute for Health Information).
Results
Our discussion is organized along five framework dimensions through which institutional non-participation may generate or exacerbate inequities in MAiD utilization. Considerable overlaps are revealed across framework domains, indicating the complexity of the problem and the need for further investigation.
Conclusion
Conscientious dissensions on the part of healthcare institutions form a likely barrier to ethical, equitable, and patient-oriented MAiD service provision. Comprehensive, systematic evidence is urgently needed to understand the nature and scope of resulting impacts. We urge Canadian healthcare professionals, policymakers, ethicists, and legislators to attend to this crucial issue in future research and in policy discussions.
Keywords
Introduction
Achieving patient-centred goals in end-of-life care (EoLC) remains complex in light of health inequities, the medicalization of death, and competing ethical perspectives on diverse EoLC practices. Sociomedical attitudes of death-denialism1,2 continue to be pertinent to mainstream medicine, and importantly, to death-hastening practices.3,4 In June 2016, when the Supreme Court of Canada legalized medical assistance in dying (MAiD), 5 it created a new EoLC option for Canadians suffering from advanced and untreatable illnesses, and simultaneously, marked an important milestone in the country’s biomedical and social history. Since then, further legislative advances and amendments have been made to clarify and modify this controversial law as new challenges have emerged following its implementation. One of these unresolved problems, and the subject of this paper, is the variability of accessing MAID services, insofar as it relates to the volitional non-participation of certain healthcare institutions.
Thus far, discussions about patient autonomy, dignity, and involvement in medical decision-making have driven the events leading up to legalized assisted dying in all permissive jurisdictions across the world. 6 In Canada, these concepts and ideals have reinvigorated public discourse in EoLC ethics and policymaking following MAiD. 7 Moreover, for much of the last century, the management of death has been deeply entangled with its institutional setting and its reliance on medical techniques. 8 Most deaths across the world still occur in institutional locations; for example, with 56% of Canadians 9 and 48% of British people 10 dying in hospitals. Some have argued that widespread institutionalized dying has further fragmented access to high quality EoLC, 11 as seen from the inadequate utilization of palliative care services worldwide. 12 Others have investigated whether legal assisted dying services might, in turn, hinder palliative care utilization. 13 Yet others have studied if alternative clinical advancements (eg, terminal sedation) might serve as a middle ground to reconcile the ethical contentions that continue to perplex assisted dying practices.14,15 In general, contentions about the character and constitution of EoLC are far from settled, with new complexities coming to the fore as assisted dying in Canada, or elsewhere, achieves legalized status.
Following MAiD legislation, the subject of conscience rights—and the regulation of its diverse constituent moralities—has recaptured the attention of Canadian healthcare professionals, policymakers, ethicists, and the public. In Canada, healthcare is taxpayer funded and health service delivery is a provincial responsibility. This means that although MAiD is a federal legislation, its implementation as a healthcare service is structured and facilitated locally. While all eligible Canadians should have right of access to MAiD, a substantial proportion of inpatient palliative support and EoLC in Canada is delivered by religiously affiliated healthcare facilities, most of which decline participation in MAiD for reasons of faith. The rights of individual healthcare professionals to refuse aid in dying remain protected in most jurisdictions where assistance in death is legal; however, there is little consensus in the literature base on whether publicly funded healthcare institutions—as collective entities—should be able to decline service provision on moral grounds.16-18
In this paper, we depart from the normative arguments within which conscience-related biomedical discourse is usually situated. Instead, we attend to accessibility concerns emerging from Canada’s morally diverse society and consider the potential implications of institutional prohibitions on MAiD participation. It is important to note, however, that there is little systematically gathered evidence on this relatively narrow phenomenon, given the novelty of MAiD in Canada and the small population utilizing this service. As a result, the scope and impact of institutional non-participation in MAiD on service access remains unknown in the absence of scientific studies investigating this subject. Accordingly, we provide an exploratory view of the problem in order to forecast its potential effects on MAiD service access, and correspondingly, to make the case for further investigation and dialogue. In the forthcoming sections, we first describe our methodological approach, and subsequently, build our interpretations through the prisms of two important health access frameworks.
Methods
As part of a larger study on MAiD access, we conducted an extensive search of newspapers and grey literature to understand the public debate on institutional abstention from MAiD and associated views or perceptions about accessibility generated by and amongst various stakeholders. We searched Canadian Newsstream (Canadian database for print media) and CanLII (database of the Canadian Legal Information Institute), supplemented by a grey literature scan (using a University of Toronto library tool and an independent Google search). Our search terms, which varied slightly by database, included: “medical assistance in dying”, and related terms, “MAiD”, “euthanasia”, “physician-assisted death”, “physician-assisted suicide”, “voluntary assisted death” AND “conscientious objection”, and related terms, “moral objection”, “faith-based objection”, “religious objection”, “faith-based organization”. We limited the search to English language articles between 2016 and 2022, in accordance with the time elapsed since the passing of the Canadian legislation.
After redundant, duplicate, and unrelated items were discarded, 89 media articles and 22 legislative, institutional policy, or other relevant documents (eg, position statements) were found relevant for inclusion in our analysis. We report findings about the thematic content of stakeholder discourses elsewhere (manuscript in review). In this paper, we concentrate on the tensions emerging about MAiD service provision, thus forming an argument for MAiD access within and across the health system landscape. Our goal is to discuss access concerns in relation to non-participating institutions—as they are perceived and portrayed—rather than to make definitive claims about what these might, or should, be in practice. Furthermore, we do not profess that conscience rights—whether at the personal or the collective level—should be rescinded. Instead, we provide an exploratory, descriptive, and interpretive discussion of publicly available data on the subject, attempting to highlight its importance for further inquiry.
To do this, we employ Levesque et al’s Access to Healthcare Framework
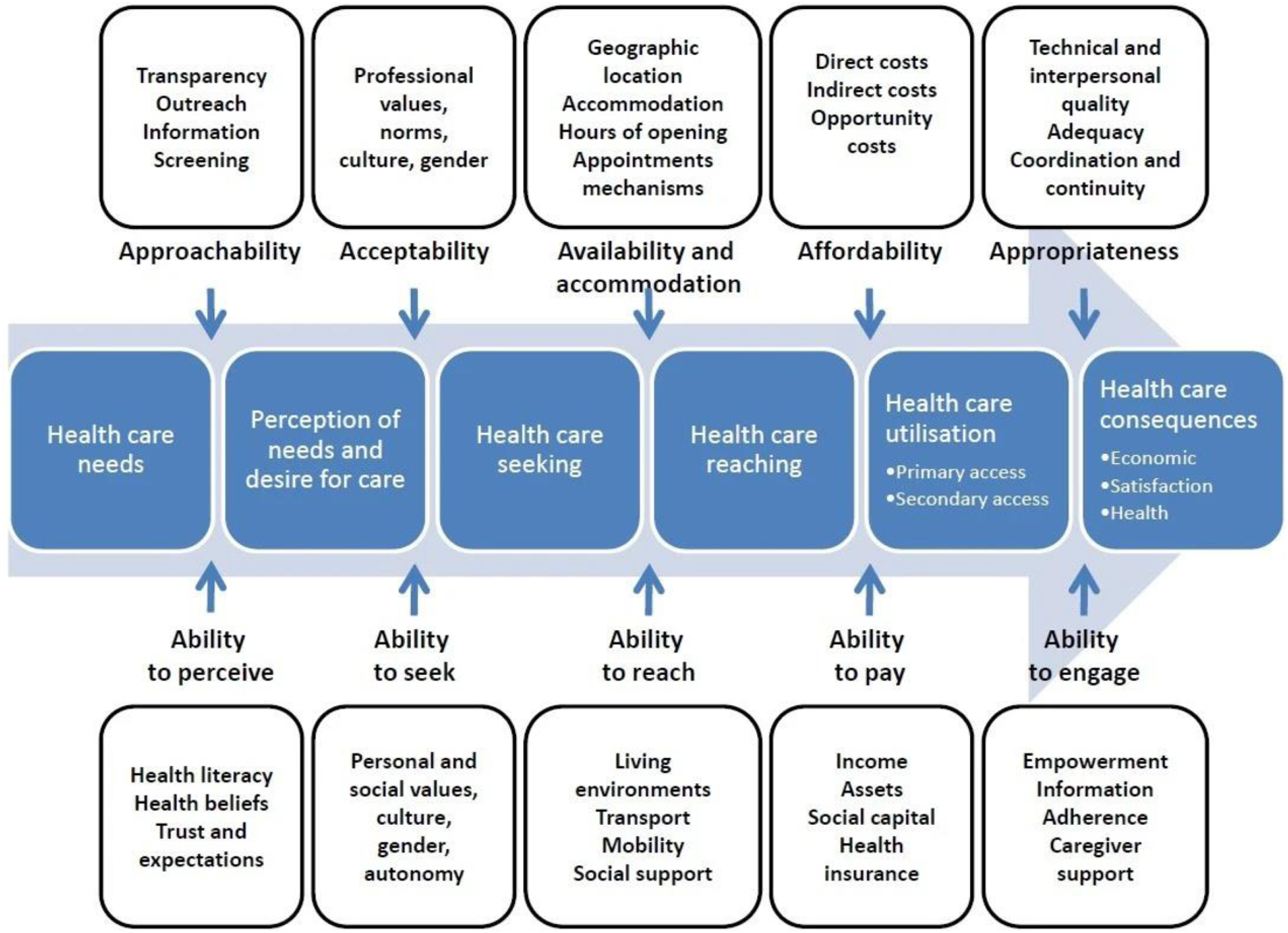
The framework proposed by Levesque and colleagues (Figure 1) has been described as one of the most comprehensive patient-centred approaches in equity studies to date and has been used to appraise health service accessibility in many contexts for various health services globally. It conceptualizes ‘access’ as a dynamic interface between five system dimensions (approachability, acceptability, availability and accommodation, affordability, and appropriateness), with five corresponding healthcare user abilities (ability to perceive, seek, reach, pay, and engage). Conceptual framework for access to health.
19
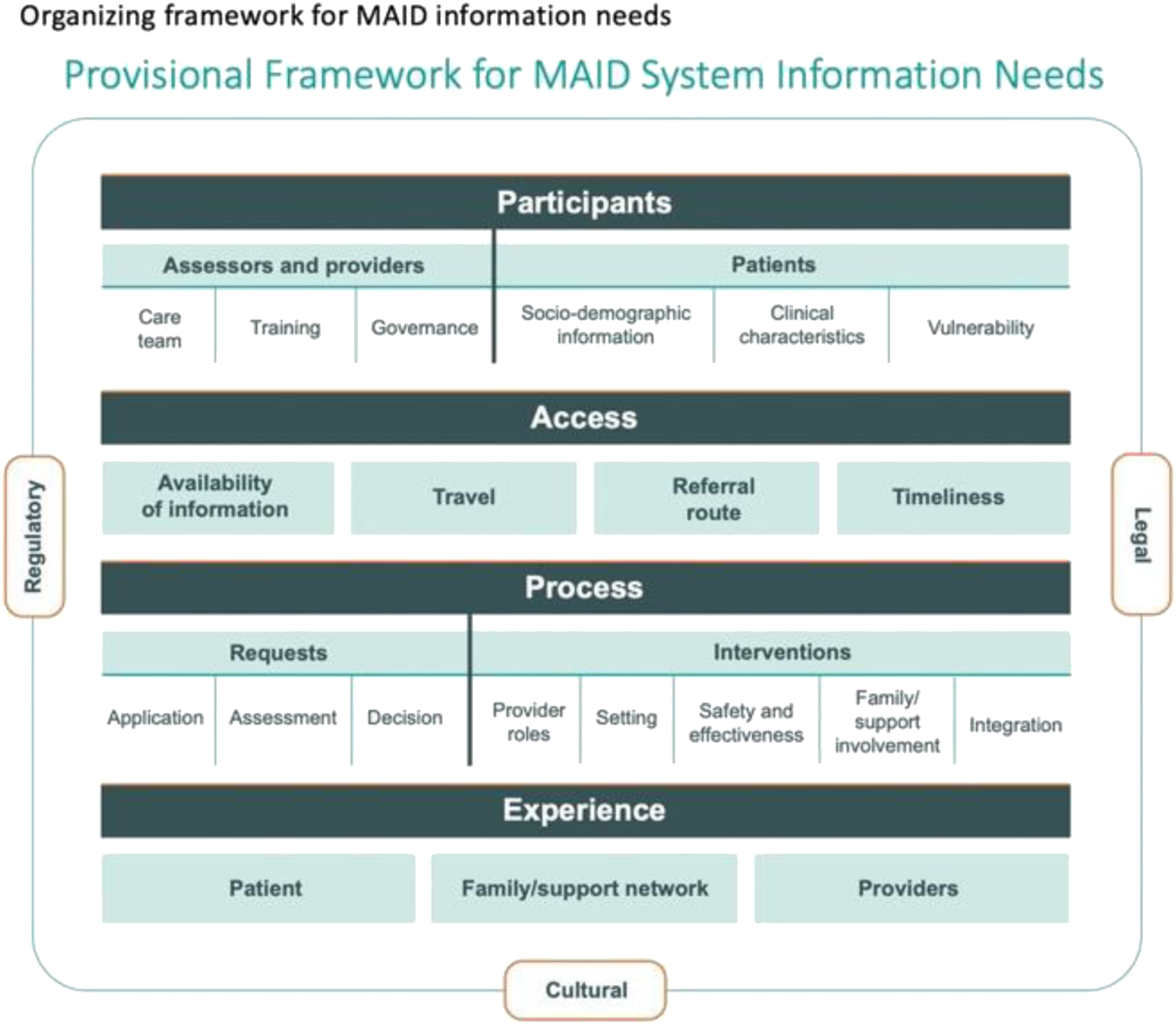
On the other hand, the CIHI (Canadian Institute for Health Information) Provisional Framework for MAiD System Information Needs was formulated with the aim to support MAiD implementation in Canada and help researchers, policymakers, healthcare providers, and other stakeholders across the country to determine knowledge gaps as policy and practice evolve. This framework envisions four access-specific dimensions, availability of information, travel, referral route, and timeliness (Figure 2), which we employ within this analysis. CIHI Provisional framework for MAiD system information needs.
20
Interpreting evidence at the intersections of the two frameworks, we identify below areas of concern for MAiD access emergent from our dataset, with the hope to prompt future scholarly investigation and policy improvement endeavours.
Findings and Discussion
Our findings indicated that access issues evident within media narratives and grey literature related most strongly with the two CIHI dimensions travel and referral route (Figure 3), although all dimensions were found to interact with each other and should not be viewed in isolation. Below, we organize our discussion under Levesque et al's five health access dimensions,
19
while interpreting their relationship with the CIHI framework,
20
as relevant. Most of our analysis focuses on the first four access dimensions, which were found most pertinent within the data. Relevance of institutional MAiD abstinence for access dimensions.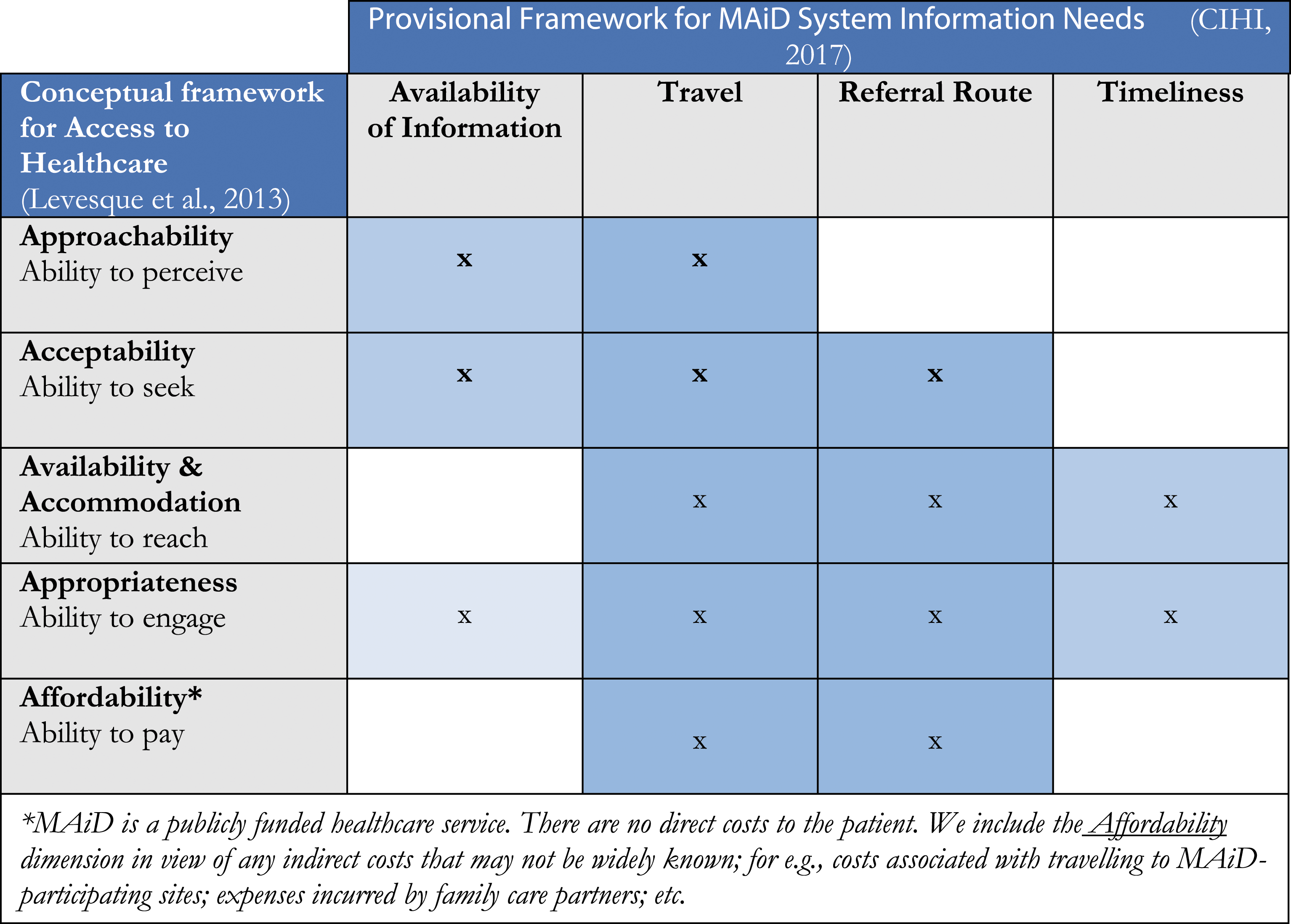
Approachability (Ability to Perceive)
According to Levesque et al, the approachability of the health system relates to how people perceive their healthcare needs and recognize the presence of health services to meet these. 19 Individuals seek MAiD at a time when they believe an advanced illness to be intolerable—with suffering, progressive loss of control, and diminishing autonomy as the most commonly reported reasons 21 —to the point where an assisted death seems to them the most appropriate medical response. This threshold is further ensured through the application of stringent procedural safeguards, alongside the requirement that patients must directly request MAiD themselves. 5 Therefore, this is not a situation in which the patient is incognizant of or uneducated about their health status; rather, their ability to perceive relates to whether the health system appears responsive to the needs they identify.
In our data sample, right-to-die activists across the country, some physicians in rural areas, and individuals in communities served by religiously affiliated healthcare sites perceived an inadequacy of MAiD services due to institutional non-participation. In part, this can be attributed to the CIHI dimension,
Approachability also depends on the transparency and trustworthiness of public health messaging about both health problems as well as the medical services available to address them.
19
In relation to the CIHI dimension
Since MAiD inception, provincial healthcare bodies have dedicated webpages to explain the process for initiating MAiD requests in each province and finding the local coordinating team’s contact numbers. Yet, some individuals may be unaware of this information and its precise location. This could reflect the general lack of conversations on death and dying within mainstream society,1,2 and by extension, lack of discussions on its more contentious facets, like assisted dying. There may also exist a ‘digital gap’ 25 that most strongly affects older adults and frail individuals living with debilitating illness. Furthermore, the digital gap may be widened by deficiencies in the usability of health messaging platforms and online formats for particular audiences. 26 In this respect, some patient advocates noted the value—and worrying absence—of physical materials such as MAiD information brochures at in-patient palliative care facilities, both with and without a religious affiliation (personal communication, 10 Feb 2022).
Acceptability (Ability to Seek)
Acceptability is associated with the sociocultural norms and values that make healthcare services acceptable to people. 19 Here, the ability to seek care depends on the personal autonomy and capacity of different individuals to obtain particular health services. Vulnerable groups (eg, ethnic minorities, older adults) or individuals seeking services long bridled with social stigmata (eg, abortion, gender reassignment surgery, and arguably, assisted death) may face greater hindrances in healthcare access.11,27,28
Intriguingly, MAiD illustrates the challenge of variable acceptability among healthcare provider segments, rather than the population which may potentially wish to seek this service. We found that some physicians, healthcare organizations, and members of the public in our data sample expressed reluctance in accepting MAiD as a legitimate practice within palliative medicine—or within the medical professions in general. For example, relating to the CIHI dimension
The organization of services in the health system—and the structures that moderate their access—can also make them unacceptable to the public.
19
Here, MAiD service organization pertains to the CIHI dimensions
Overall, resistance from providers may generate feelings of unease among the public, discouraging patients from openly expressing their needs and being able to navigate the MAiD system smoothly. These frictions suggest that the unacceptability of MAiD within the medical professions (and prominently, among palliative care providers) may deepen the cultural silence surrounding death and dying, prove discriminatory towards vulnerable healthcare users, and reinforce long-standing paternalism in modern medicine.
Availability & Accommodation (Ability to Reach)
Availability and accommodation refer to whether health services (either the physical setting or the individuals working in health care roles) can be reached physically and in a timely manner. Equitable distribution of services, modes of service provision, and the capacity of both healthcare facilities and healthcare professionals to meet patient needs constitute the factors influencing healthcare users’ ability to reach healthcare services.
19
Here, three CIHI dimensions,
The ability to reach health care involves the notion of personal mobility, availability of transportation, occupational flexibility, and knowledge about health services that would allow a person to physically reach service providers. Restricted mobility of older adults and people with disabilities, or the inability of casual workers (especially, family caregivers) to be absent from work to consult medical providers are some examples. 19 There are geographic variabilities in MAiD service regulation and organization across Canada. Many abstaining sites initially espoused policies restricting the ability of staff to discuss MAiD comprehensively with patients, although this situation has altered considerably in the last six years. Some provinces, for example, Alberta, have had successful negotiations with these sites, as a result of which staff can now direct patients to local MAiD coordinators and eligibility assessments can take place on some abstaining sites. However, there is little systematic evidence on whether there is universal uptake of these intended changes across the country, or indeed, how many sites remain where onsite eligibility assessments are still difficult to perform. We note that the administration of MAiD procedures itself remains prohibited at most abstaining sites throughout Canada, even if externally employed medical practitioners are available to perform it.
Recently, in the province of Ontario, certain physician groups (including the Christian Medical and Dental Society of Canada, the Canadian Federation of Catholic Physicians’ Societies, Canadian Physicians for Life, and several individual physicians) moved the Ontario Court of Appeal with a view to gain exemptions from having to provide MAiD referrals. These groups claimed that even though a physician may legally decline direct participation in MAiD, being required to provide a referral to a MAiD-favouring physician would make them complicit in an act they are morally opposed to. In 2019, as part of the decisive judgement in this case, the court ruled against the plaintiffs, citing the need to uphold patients' rights to equitability in MAiD access. 37 While this ruling will doubtless serve as an important precedent, the case may signal further litigation possibilities by similar lobbies of MAiD-opposed healthcare providers in future.
Appropriateness (Ability to Engage)
Appropriateness refers to the technical and interpersonal quality of healthcare services and their timely, integrated, and continuous nature.
19
With many healthcare providers not offering MAiD, CIHI’s
According to Leveque et al, the ability to engage in care further depends on patient involvement in medical decision-making, communication, and empowerment.
19
In this regard, all CIHI dimensions
Affordability (Ability to Pay)
Affordability involves an individual’s economic capacity to devote resources and time to utilize appropriate healthcare services. It relates to the direct prices of services and associated expenses, as well as opportunity costs resulting from loss of income (including that of family caregivers).
19
MAiD is a publicly funded service in Canada and fully incorporated within its overarching system of socialized healthcare. There are no direct costs to patients and families for receiving MAiD. We found no evidence in our dataset indicating that affordability may be a barrier to access. However, it remains possible that there may be indirect costs in relation to the CIHI dimensions,
However, most people who utilize assisted dying services are likely to be financially stable, 41 and as such, these costs are not expected to impede MAiD access. Future research about the sociodemographic characteristics of MAiD-seeking individuals may reveal whether indirect cost burdens affect vulnerable groups differently. On the other hand, some patients' financial dependence on caregivers may unduly influence their decisions to seek MAiD. In general, it is unlikely that financial considerations substantially hinder MAiD access, although richer data in relation to economically vulnerable populations would be useful for better understanding the relationship between indirect socioeconomic factors and MAiD access.
Conclusion
This study has strengths, but it is not without its limitations. To our knowledge, this is the first study to consider MAiD provision through the use of robust frameworks for assessing healthcare access and health service improvement priorities. However, this work must be viewed within its speculative context and its goal towards triggering health research and policy questions on a frequently understudied subject, rather than offering a definitive report on the actual state of MAiD access in Canada. Secondly, given that national print media and grey literature are overwhelmingly in English, we draw our interpretations from English language data. It is possible that we may have overlooked some information in French, the second official language of Canada, which is used primarily in the province of Quebec.
Overall, we found that institutional abstinence from MAiD often presents a view of the health system as opaque, convoluted, and inconsistent with regard to accessing MAiD or obtaining the requisite information about it. Although provincial MAiD care coordination structures are well-positioned and available to support patients throughout the process, it is possible that many elements obscure their presence and distort public perceptions about service access routes and procedures. Moreover, given their precarious health and the time-sensitive nature of their EoLC wishes, not all individuals can or should be expected to overcome the myriad resistances faced over the course of their healthcare journeys, including the inconvenience of being referred to willing physicians or being transferred to participating sites. At the same time, limiting the exercise of conscientious objection rights raises many ethically and pragmatically complex questions about how the point of reasonable compromise may be identified and reached.
With present legislative ambiguity and variations across Canadian provinces on collectively (institutionally) held conscientious objections, there are limited tools available to measure its impacts on equitable MAiD access. Our use of two important health access frameworks has aimed to generate a preliminary understanding of potential problems. Moving forward, systematic data is urgently needed to determine the actual impacts of institutional conscience on the MAiD-seeking population, and accordingly, to develop policy instruments for monitoring equitable MAiD access in Canada. Given that there remain no exhaustive studies on the subject to date, we urge researchers and policymakers to attend to this area, launching further inquiry on the subject.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Canadian Institutes for Health Research (grant number # 170680).
Ethical Approval
This study received ethics approval from the investigator’s institutional review board (Approval ID Pro00107062).