
Abstract
Keywords
Introduction
Having a critically ill loved one can induce symptoms of depression and anxiety, and decrease quality of life.1,2 Therefore, support for family caregivers is an essential component of palliative care and should start at the time of diagnosis and continue after the patient’s death. 3 According to the Clinical Practice Guidelines for Quality Palliative Care, such support entails anticipating, preventing, and managing physical, psychological, social, and spiritual suffering to optimize quality of life. The guidelines recommend assessing and addressing emotional and spiritual support needs, providing education on what to expect around death, involving family caregivers in discussions regarding care for the patient, and providing access to bereavement support. 4
Interventions aiming to support family caregivers can reduce burden and improve quality of life.5-7 However, previous research also shows that support for family caregivers is under-resourced in many healthcare settings, and that there is often no system in place to offer support to all family caregivers.8-12 More detailed information on what support is provided by individual healthcare professionals is needed to understand current practice. An understanding of what hinders and what facilitates supporting family caregivers is needed to improve it. Facilitators and barriers have been identified in cancer settings, 13 end-of-life home care, 11 and hospital-based bereavement care. 14 An overarching mapping of facilitators and barriers across settings and illness trajectories is needed to improve support for family caregivers across a wider range of circumstances.
The Behavior Change Wheel (BCW) is a tool that can be used to design an intervention to enhance behavior, including supporting family caregivers. Central to the BCW is the Capability-Opportunity-Motivation-Behavior (COM-B) system, which suggests people need capability (C; physical and psychological), opportunity (O; physical and social) and motivation (M; automatic and reflective) to perform a behavior (B). 15 Mapping facilitators and barriers to the COM-B system allows for linking these to several intervention functions (i.e., education, training, modelling), which can help to develop an intervention to improve the practice of supporting family caregivers. 15
The aims of the present study are 1) to assess current practice of support for family caregivers of patients with life-threatening diseases in hospitals, nursing homes, and hospices, and 2) to identify facilitators and barriers to the provision of support for family caregivers as perceived by healthcare professionals.
Methods
Study Design
A two-phase study was conducted with a survey and focus groups among healthcare professionals. The Medical Research Ethics Committee of LUMC declared the study exempt from the Medical Research Involving Human Subjects Act (WMO; no. N21.072). To the extent possible, the consolidated criteria for reporting qualitative studies (COREQ) were applied. 16
Survey
Current practice of supporting family caregivers was assessed using a self-developed survey (Appendix A) in 2017. The survey was administered electronically and anonymously in 2017 through Google Forms in healthcare institutions located in urbanized Western Netherlands within the area of the regional palliative care consortium. We targeted physicians, nurses, and nurse assistants through the means of convenience sampling. The survey comprised demographics and 23 (8 closed-ended, 15 open-ended) items on supporting family caregivers before and after the patient’s death. The open-ended questions offered respondents the opportunity to explain or elaborate on their answers to the preceding closed-ended questions. Responding to the survey took approximately 5 minutes. The data were analyzed using descriptive analyses in SPSS (Version 25).
Focus Groups
Subsequently, a topic list (Appendix B) to guide focus groups was developed in 2018 to identify facilitators and barriers to providing support for family caregivers, as perceived by healthcare professionals. We targeted nursing staff and physicians working in nursing homes and hospitals through convenience sampling by giving survey respondents the possibility to disclose their name to sign up for focus groups. The research team phoned or e-mailed them and sent a study leaflet. Two focus groups were conducted with nurses and nurse assistants working in nursing homes, one with nurses working in hospitals, and one with physicians working in hospitals. The focus groups lasted 2 hours and were moderated by MCT (female, MSc) or JTS (female, PhD) who both had experience with conducting focus groups. The moderators did not have a prior relationship with the participants. At each focus group, one of the other researchers (JAB, MCT, YML) was present to note observations. The focus groups took place at the LUMC-campus in Leiden or The Hague. All participants provided written informed consent to participate in the focus groups.
Qualitative Data Analyses
The focus groups were audio recorded and transcribed verbatim. Member checks were performed with summaries of the focus groups. The data were analyzed by HEH using ATLAS.ti software (Version 9), supervised by JTS and IDH, both experienced qualitative researchers. The analysis was mainly deductive, using a codebook approach to thematic analysis17,18 with the COM-B system 15 as a framework that provided the initial codes. Open coding was used to identify specific barriers and facilitators as sub-codes. In the final stage, JAB and HEH discussed the results and reached consensus on final codes.
Results
Current Practice
Characteristics of Healthcare Professionals in The Survey Sample; n = 374.
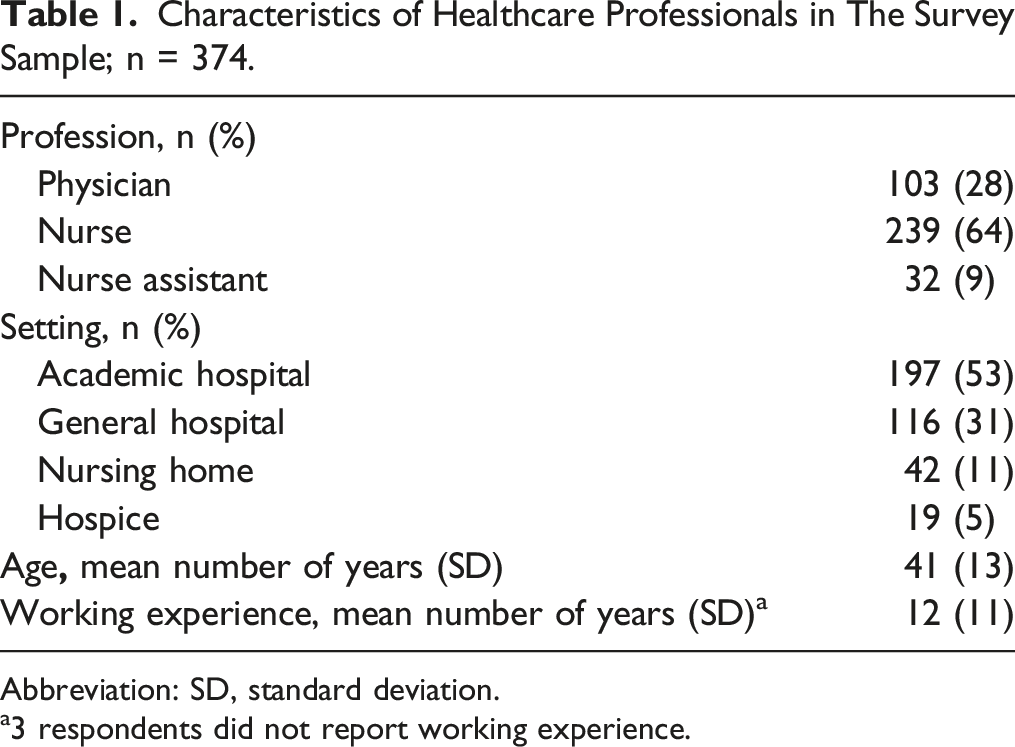
Abbreviation: SD, standard deviation.
a3 respondents did not report working experience.
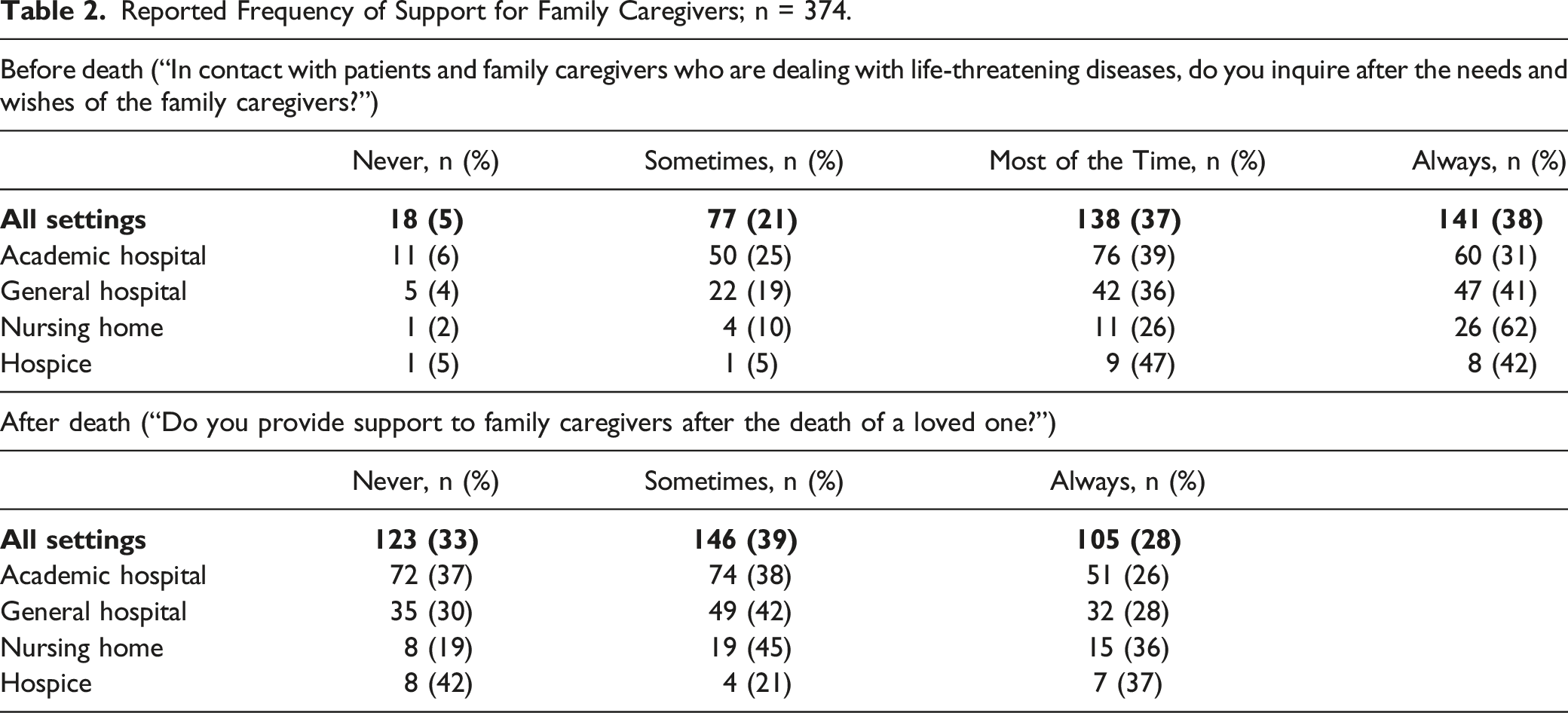
Reported Frequency of Support for Family Caregivers; n = 374.
Determinants of the Provision of Support After Death; n = 146. a
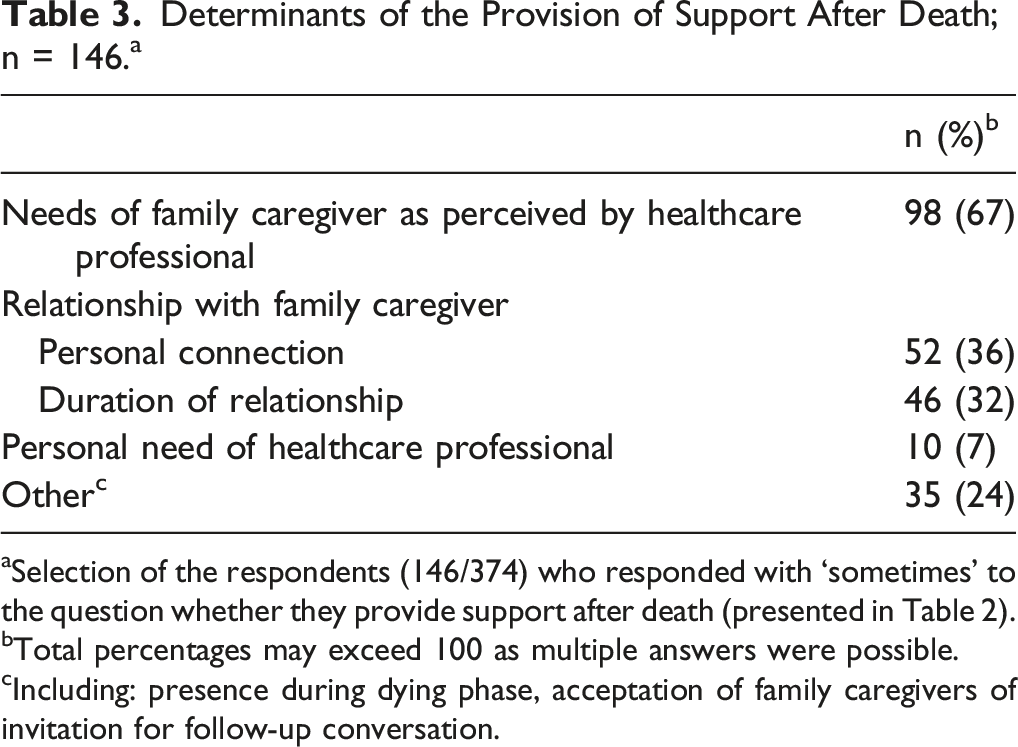
aSelection of the respondents (146/374) who responded with ‘sometimes’ to the question whether they provide support after death (presented in Table 2).
bTotal percentages may exceed 100 as multiple answers were possible.
cIncluding: presence during dying phase, acceptation of family caregivers of invitation for follow-up conversation.
Type of Support Provided After Death.
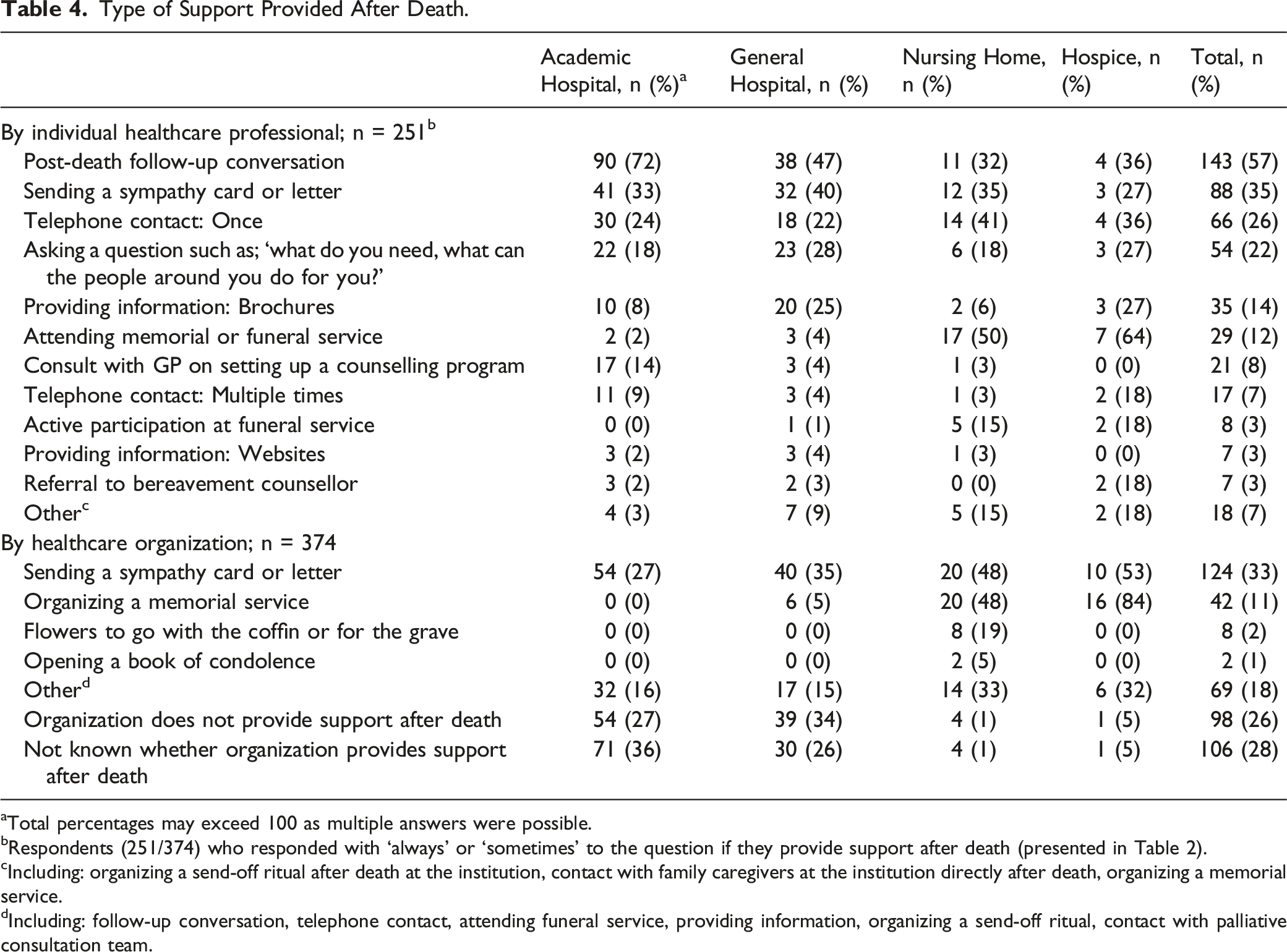
aTotal percentages may exceed 100 as multiple answers were possible.
bRespondents (251/374) who responded with ‘always’ or ‘sometimes’ to the question if they provide support after death (presented in Table 2).
cIncluding: organizing a send-off ritual after death at the institution, contact with family caregivers at the institution directly after death, organizing a memorial service.
dIncluding: follow-up conversation, telephone contact, attending funeral service, providing information, organizing a send-off ritual, contact with palliative consultation team.
Services that Family Caregivers with Needs for Additional Support Were Referred to and Reasons Not to Refer; n = 374.
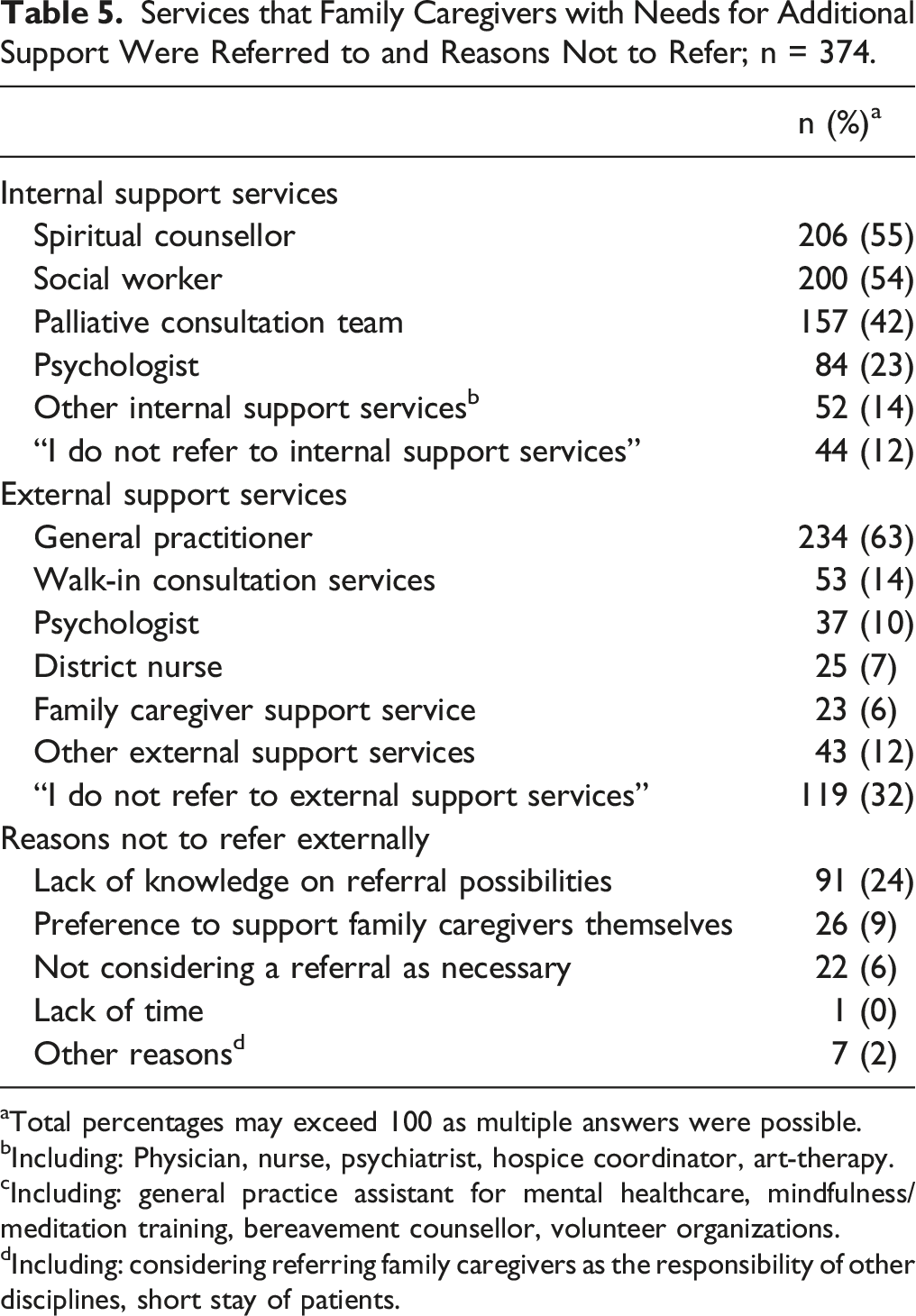
aTotal percentages may exceed 100 as multiple answers were possible.
bIncluding: Physician, nurse, psychiatrist, hospice coordinator, art-therapy.
cIncluding: general practice assistant for mental healthcare, mindfulness/meditation training, bereavement counsellor, volunteer organizations.
dIncluding: considering referring family caregivers as the responsibility of other disciplines, short stay of patients.
Facilitators and Barriers
Perceived Barriers and Facilitators by Healthcare Professionals to Providing Support for Family Caregivers Before and After Death.
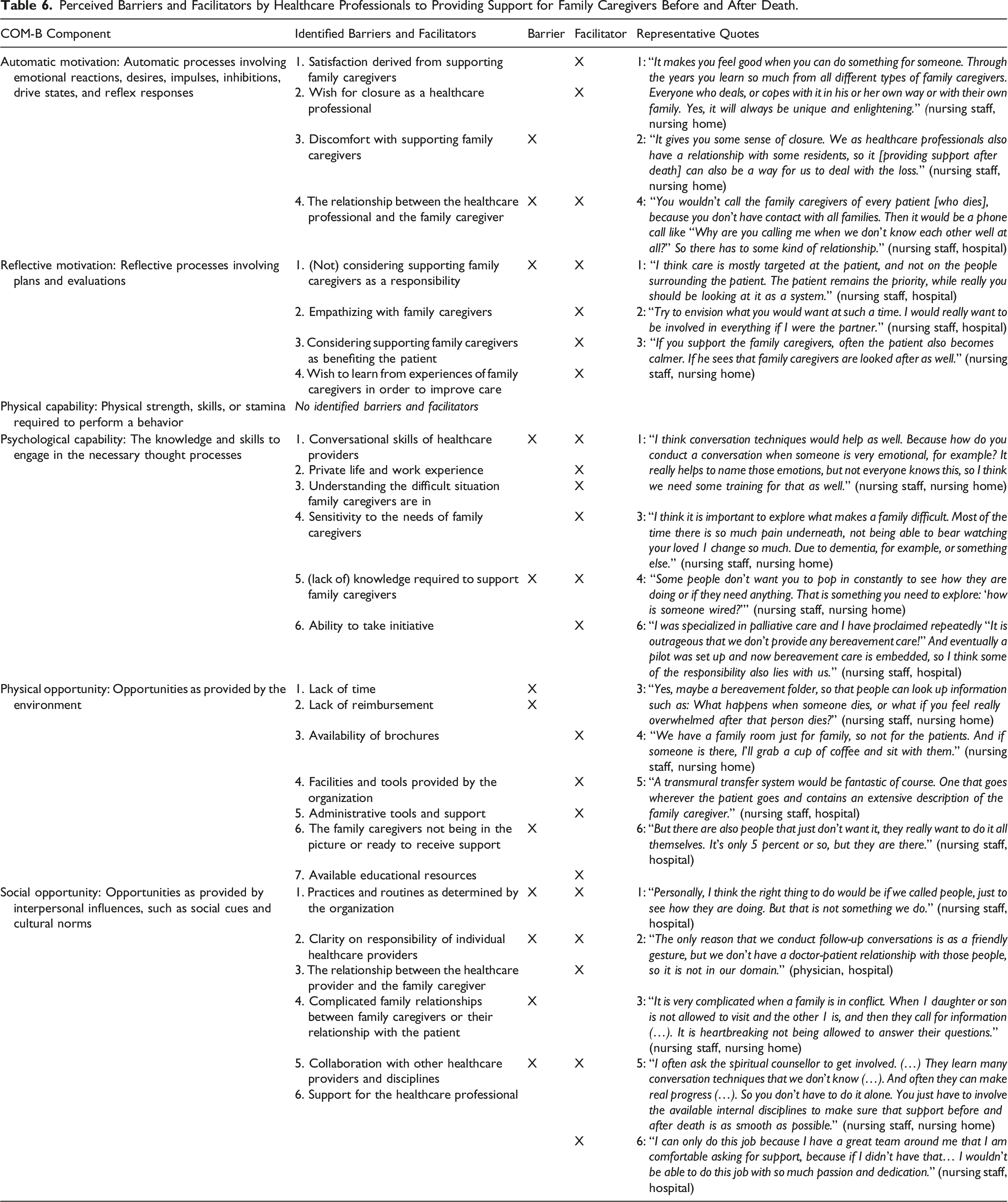
Motivation: Automatic
Participants were motivated to support family caregivers as they derived satisfaction from it and perceived it as rewarding. They appreciated witnessing the resilience of family caregivers. Supporting family caregivers after the patient’s death also helped to achieve a sense of closure for themselves. A barrier reported for themselves and witnessed with colleagues was discomfort with supporting family caregivers. A strong or longstanding relationship with the family caregiver increased motivation.
Motivation: Reflective
Many participants were motivated to support family caregivers as they considered this an important aspect of high-quality care and therefore their responsibility. However, some had noticed among colleagues that their priority remained strongly with the patient. Some participants mentioned that empathizing with family caregivers helps them to realize the importance of supporting them.
Another motive to support family caregivers was the beneficial effect on the patients. Family caregivers can provide additional information that improves tailored care, and patients feel reassured when their loved ones are cared for too. Some mentioned to be motivated to conduct a follow-up conversation after death, as family caregivers’ reflections can help improve future care for patients and family caregivers.
Capability: Psychological
According to the participants, mastering conversational skills facilitates providing support. Some reported to struggle themselves, or had noticed colleagues struggling with conducting conversations on death and dying and dealing with the emotions of family caregivers. Private life and work experience were reported to help in conducting such conversations.
The participants also mentioned the need to really understand the unique and difficult situation that family caregivers are in and what their corresponding needs are, and approach them with a non-judgmental attitude. For example, forgiving family caregivers for acting unfriendly due to their distress, or realizing that understanding medical information may be difficult for them. Furthermore, they mentioned the necessity to be sensitive to the unique needs, wishes, and capabilities of each individual family caregiver. For example, whereas some family caregivers may desire more attention, others may prefer to be mostly left alone. In addition, family caregivers in need for support do not always express this clearly, which requires some senstivity to subtle expressions of needs. Some participants mentioned that healthcare professionals may need to set aside their own opinions, wishes, and needs to make room for those of the family caregiver.
Knowledge regarding a variety of subjects (complicated grief (identification), referral options, cultural beliefs and rituals) was mentioned as a prerequisite to providing support. Additionally, knowledge was desired of the different approaches that may be required under different circumstances. For instance, an unexpected death versus an expected death, or the death of an older person versus the death of a young parent may require different approaches. Lastly, it was mentioned that strong initiative from individual healthcare professionals can be necessary to improve practice of supporting family caregivers within a healthcare team or on an individual level, rather than waiting for existing procedures to change.
Opportunity: Physical
The participants reported that supporting family caregivers would mean working (unpaid) overtime. The unavailability of reimbursement of support for family caregivers formed a barrier.
The availability of brochures to give to family caregivers was mentioned to facilitate providing support. Such brochures should provide information about the organization, the palliative phase and what to expect of the dying phase and after death, and possibilities for additional support. Facilities offered by the organization were also mentioned to be helpful, such as a separate ‘family room’ where informal conversations can be held with family caregivers, or the possibility for family caregivers to stay overnight. A checklist for conducting follow-up conversations after death was mentioned as a helpful tool. Some participants stipulated that such a checklist should be presented and used as a helpful guide rather than a scripted format as they prefer to conduct such conversations without strict guidelines.
Furthermore, administrative tools were reported to be helpful, such as the possibility to extensively report on the network around the patient in the electronic medical file and this information being accessible to every involved healthcare professional, including external disciplines. One participant also mentioned giving family caregivers access to the medical file, as it gives them control over when to retrieve information, decreasing dependence upon healthcare professionals. Administrative support from a secretary to send reminders and plan follow-up conversations after death was also mentioned.
The participants stipulated the necessity of family caregivers being in the picture while the patient is undergoing treatment, as well as the family caregivers being ready to receive support, which both were not always the case. Some participants also mentioned that they are often not notified of the death of a patient, which complicates providing support after death.
Lastly, support for family caregivers was suggested to be included in healthcare training and continued education. Courses on conversational skills were mentioned, but also on cultural rituals, and one that stimulated healthcare professionals to reflect on their own last phase of life to make them more aware of the family caregivers’ situation.
Opportunity: Social
Standard routines embedded in healthcare organizations were reported to substantially affect the extent to which, and how family caregivers were supported. For instance, some organizations structurally invited family caregivers for a follow-up conversation, other organizations did not. The same goes for attending funerals, reporting on family caregivers in the medical file, or sending a sympathy card. However, the participants felt that designing a one-fits-all protocol would not meet the diverse needs and wishes of family caregivers. Some protocols can also interfere with supporting family caregivers, such as a protocol that dictates family to remove all personal belongings from the room within a few days after the patient’s death.
Responsibilities of individual healthcare professionals with regard to supporting family caregivers were unclear. Some participants questioned whether supporting family caregivers fit their function description at all, and others wondered when they should refer to external services or leave it to the initiative of the family caregivers.
A strong and longstanding relationship between the family caregiver and the healthcare professional was reported to help understand the family caregiver’s needs and to start conversations about sensitive topics. Complicated relationships between family caregivers or between patient and caregiver(s) formed a barrier as it can cause tensed social situations.
Another facilitating factor was easily accessible collaboration with other healthcare professionals, for example between nurses and physicians, but also between healthcare teams and other disciplines, such as palliative consultations teams, transfer agencies, spiritual counselling, psychologists and the GP. Multidisciplinary meetings were reported to facilitate such close collaboration.
Lastly, to deliver high-quality support for family caregivers, the healthcare professionals felt they also needed support themselves. They needed to be aware of their personal boundaries and be sure not to cross those. Personal connections with team members and a safe environment in which difficulties can be discussed helped participants to feel supported. Close contact with colleagues also offers opportunity to learn from each other.
Discussion
This study showed that most, but not all healthcare professionals working in institutional settings in the urbanized western part of the Netherlands occasionally or more frequently inquire after the wishes and needs of family caregivers of patients with life-threatening diseases, but one-third does not provide support after death. These findings are in line with previous literature demonstrating that support for family caregivers is provided ad hoc and depends on circumstances, preferences, and intuition of individual healthcare professionals.8-12 The identified barriers in this study, such as the experienced discomfort of healthcare professionals when dealing with family caregivers or not feeling responsible for their wellbeing, limited knowledge and conversational skills, and shortage of resources, help to understand why support for family caregivers is not part of routine practices. These results correspond with previous literature in more specific target populations.11,13,14
Interventions aiming to improve family caregivers’ outcomes have proven effective.5-7,19,20 However, the barriers experienced by healthcare professionals may have to be overcome first, or parallel to implementing such an intervention, which requires a certain extent of organizational change. Organizational support is necessary to provide the necessary time, money, tools, and facilities, and to train and educate healthcare professionals. Furthermore, the organization holds a responsibility to care for their employees.21,22 When these preconditions are met, healthcare organizations can work towards a more systematic approach to providing support for family caregivers. Support after death appears to be in most need of improvement, but also during the illness-trajectory healthcare professionals should feel sufficiently comfortable, knowledgeable and motivated to support family caregivers. Structured use of needs assessment tools may help to achieve this.6,23,24
Examples of Possible Interventions Based on the Identified Barriers and Facilitators and the Behavior Change Wheel.
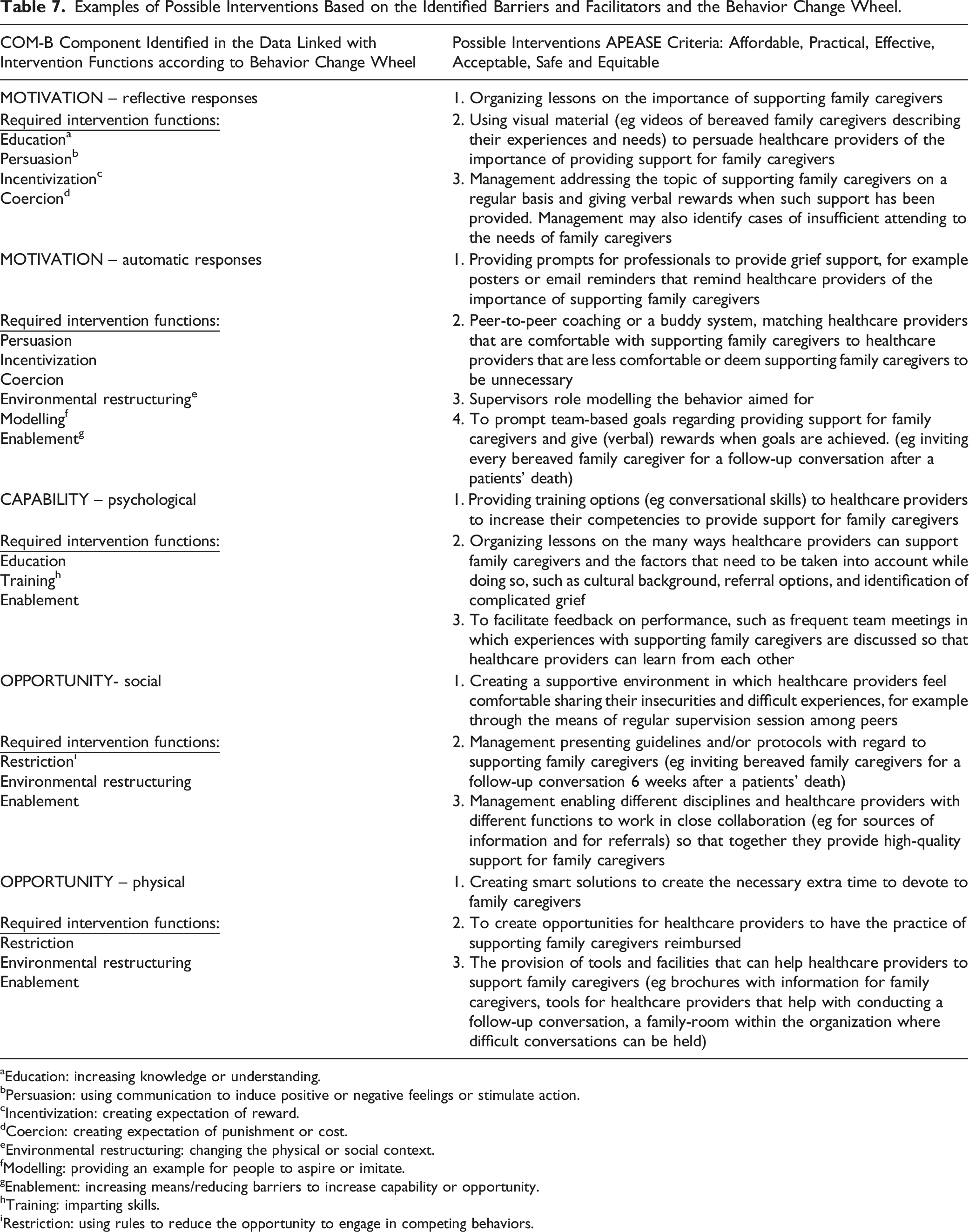
aEducation: increasing knowledge or understanding.
bPersuasion: using communication to induce positive or negative feelings or stimulate action.
cIncentivization: creating expectation of reward.
dCoercion: creating expectation of punishment or cost.
eEnvironmental restructuring: changing the physical or social context.
fModelling: providing an example for people to aspire or imitate.
gEnablement: increasing means/reducing barriers to increase capability or opportunity.
hTraining: imparting skills.
iRestriction: using rules to reduce the opportunity to engage in competing behaviors.
Strengths and Limitations
Our study has several strengths. The survey was multi-professional and covered multiple settings, and its sample size was relatively large. Further, the use of the Behavior Change Wheel framework allowed for practical, actionable suggestions to improve support for family caregivers within healthcare organizations based on the identified barriers and facilitators. The study also has limitations. First, as the survey was self-developed and not pre-tested, we cannot report on its validity and reliability. Further, due to the retrospective nature of this study and use of self-reported questions, it is possible that participants were unable to fully recall the support delivered to caregivers. Third, only a few survey respondents worked in hospices. Fourth, the response rate to the survey was low. Therefore, we might overestimate the proportion of healthcare professionals that structurally support family caregivers. Last, the urban setting of the study differs from rural settings in a relevant manner, as the frequency or normalcy of informal care and community support, and thus the (expected) role of the family caregiver, can differ.27,28
Future Research
Based on the current findings, an intervention can be developed, implemented and evaluated in a variety of healthcare settings to reach more structurally embedded support for family caregivers in palliative care. Suggestions made based on the Behavior Change Wheel (Table 7) can inspire interventions. 15 Further research could also investigate barriers and facilitators specific to the home care setting. Our study did not include professionals practicing in home care settings, yet supporting family caregivers in this setting may come with specific challenges such as disconnection with family caregivers during hospitalization of the patient, and extra vulnerability as the dying phase approaches. 29
Supplemental Material
Supplemental Material - Practice of Supporting Family Caregivers of Patients with Life-Threatening Diseases: A Two-phase Study Among Healthcare Professionals
Supplemental Material for Practice of Supporting Family Caregivers of Patients with Life-Threatening Diseases: A Two-phase Study Among Healthcare Professionals by Hinke E. Hoffstädt, MSc, Jannie A. Boogaard, PhD, Marcella C. Tam, MSc, Leti van Bodegom-Vos, PhD, Arianne Stoppelenburg, PhD, Iris D. Hartog, PhD, Yvette M. van der Linden, MD, PhD, and Jenny T. van der Steen, PhD, FGSA in American Journal of Hospice and Palliative Medicine®
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Netherlands Organization for Health Research and Development (ZonMw) under grant numbers 844001312 and 844001706.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.