
Abstract
Keywords
Background
Dying matters. Death is both a uniting inevitability and source of great anxiety, fear and uncertainty. Good end of life (EoL) care should be a basic human right.1,2 The view of good dying as part of a holistic view of health has been the basis of the Public Health Palliative Care movement. 3 Since its inception by Alan Kellehear, 4 this approach aimed to tackle perceived weaknesses in traditional services: over professionalisation, 5 community disempowerment, 6 inequity 7 and lack of capacity. 8 In so doing they aim to return dying to being a natural community led event attended by confident family, friends and neighbours supplying basic caring functions and human companionship supported by professionals, in keeping with the needs of the dying person. 9
This Public Health approach has driven efforts to improve access to Palliative Care from an epidemiological perspective 10 and develop the caring capacity of communities.1,11 Interventions to develop ‘collective social capital’ 12 in communities have been widely implemented from Frome, England 13 to Victoria, Australia. 14 These initiatives demonstrate positive impact.13,15
National surveys suggest that although we are becoming more comfortable with the subject, 16 death and dying is still a difficult topic for many in the United Kingdom. A 2018 YouGov survey commissioned by Co-op Funeral Care found 33% of UK adults were ‘not at all comfortable’ or ‘not very comfortable’ discussing death. 17 The Departure Lounge project (2019) demonstrated the most common reasons for this were: thinking that death is a ‘depressing or morbid subject’, and being ‘worried that talking about death will upset others’. 16
Tackling this taboo is likely to bring benefits for both individuals and society in increasing the confidence and capacity of lay carers and furthering the aims of developing a compassionate network within a community. Better communication and planning improves outcomes at EoL and reduces invasive and unwanted treatment.18-20 Helping people feel more comfortable about the subject of death and dying is crucial to supporting compassionate communities. This term has been used to describe ‘communities that are compassionate in their support of people through the difficult times associated with care, deteriorating health, dying and bereavement’. 21 This change is led by communities themselves, rather than outsiders or professionals and therefore requires a knowledgeable, caring and motivated public.
The Coronavirus Pandemic meant millions of people worldwide have faced death, bereavement and enforced social isolation. Overwhelmed health services, inequitable treatment, and blanket Do Not Attempt Cardio-pulmonary Resuscitation orders 22 have exacerbated fears about EoL treatment. Rapid review of deaths in the First Wave of COVID-19 demonstrated the benefits, and lack, of Advance Care Planning (ACP) in the community 21 with recommendations to enable earlier conversations. Embedding compassion in communities will be an important factor to dispel inhibiting taboos. 22
Changing attitudes and behaviours about death and dying in the healthy population is little researched. Community interventions can be successful in prompting people to discuss EoL p. 15. ACP, in the healthy population, enables better decision making and respect for autonomy in unexpected illness with loss of capacity for decision making. 23
The Omega Course (Omega) was designed by a palliative medicine consultant and a probation officer/coach, outside of their professional spheres, to increase death literacy, dispel taboos and upskill members of their Kenilworth community and environs. Participants are offered the opportunity to talk freely about death and dying in a friendly and safe atmosphere. Healthy adults undertake 14 hours of experiential learning over 4 evenings and a full day, with social events for health and wellbeing (Appendix 1: Structure and content of Omega).
24
Utilising group discussions, presentations and scenario-based role play, the course acknowledges personal mortality and the opportunity to live life to the full meanwhile. Planning for the future, recording wishes and the technicalities of making them legally binding after one loses capacity, are explained. A day of communication skills training by role play aims to ensure attendees are not lost for words in the face of a dying friend or bereaved person. The course ends by looking at the pain of bereavement and how to help. Postcards with personally recorded intentions are sent back to participants 6 weeks later. The overall intention is to increase death literacy to support compassionate and caring communities (Ambition 6 quoted below). ‘Each community is prepared to help and people recognise we all have a role to play in supporting each other and are ready and willing to have conversations about living and dying well and give emotional and practical support’.
Ambition 6 of Ambitions for palliative and end of life care
25
Aims
To assess the impact of Omega on the attitudes, behaviour and actions of participants and thereby its potential efficacy as an intervention.
Methods
Course participants were recruited via local printed and social media adverts from the local general population and by word-of-mouth recommendations from previous participants. They were not recruited from patient groups or healthcare services. People with intellectual disabilities and children under 18 were excluded as content and delivery would require adjustments for the course to be suitable.
A mixed methods study design was used with analysis of qualitative and quantitative data from a questionnaire to evaluate Omega 2.5 years post course institution. Warwick Medical School Biomedical Scientific Research Ethics Committee granted approval. Anonymous questionnaires were distributed between 3 and 27 months after completion of the course using an emailed Qualtrics link, or via post if preferred. Due to academic deadlines the questionnaire was open for 21 days, without reminders.
The questionnaire included twenty-two questions in total: 5 demographic questions, 4 quantitative questions using a Likert scale between 1 (never) and 10 (frequently) and 4 qualitative questions (Appendix 2: Questionnaire questions).
Quantitative data was analysed using a paired two-tailed T test to compare ‘before’ and ‘after’ responses. Qualitative data was analysed by Thematic Analysis using Nvivo. Coding and theme development were reviewed with an experienced supervisor.
Results
Characteristics of Respondents
23 questionnaires were returned, a 37% response rate. There were more female questionnaire respondents than male: F70% (16), M30% (7). This reflected course participants: F73% (45), M27% (17). The most common age groups in both questionnaire respondents and course participants were 50-60 and 60-70 (Figure 1). There was no significant difference between questionnaire respondents and course participants in both age (P = .08) and gender (P = .79) using Fisher’s exact test. Respondents were well educated, with 60.9% having attended university Age profiles of study respondents, course participants, Kenilworth and Warwickshire populations. Results of paired 2 tail t-test comparing ‘before’ and ‘after’ likert questions. Box and whisker plot showing change in responses of ‘before’ and ‘after’ Likert questions. Results of Thematic Analysis Showing Themes And Associated Codes.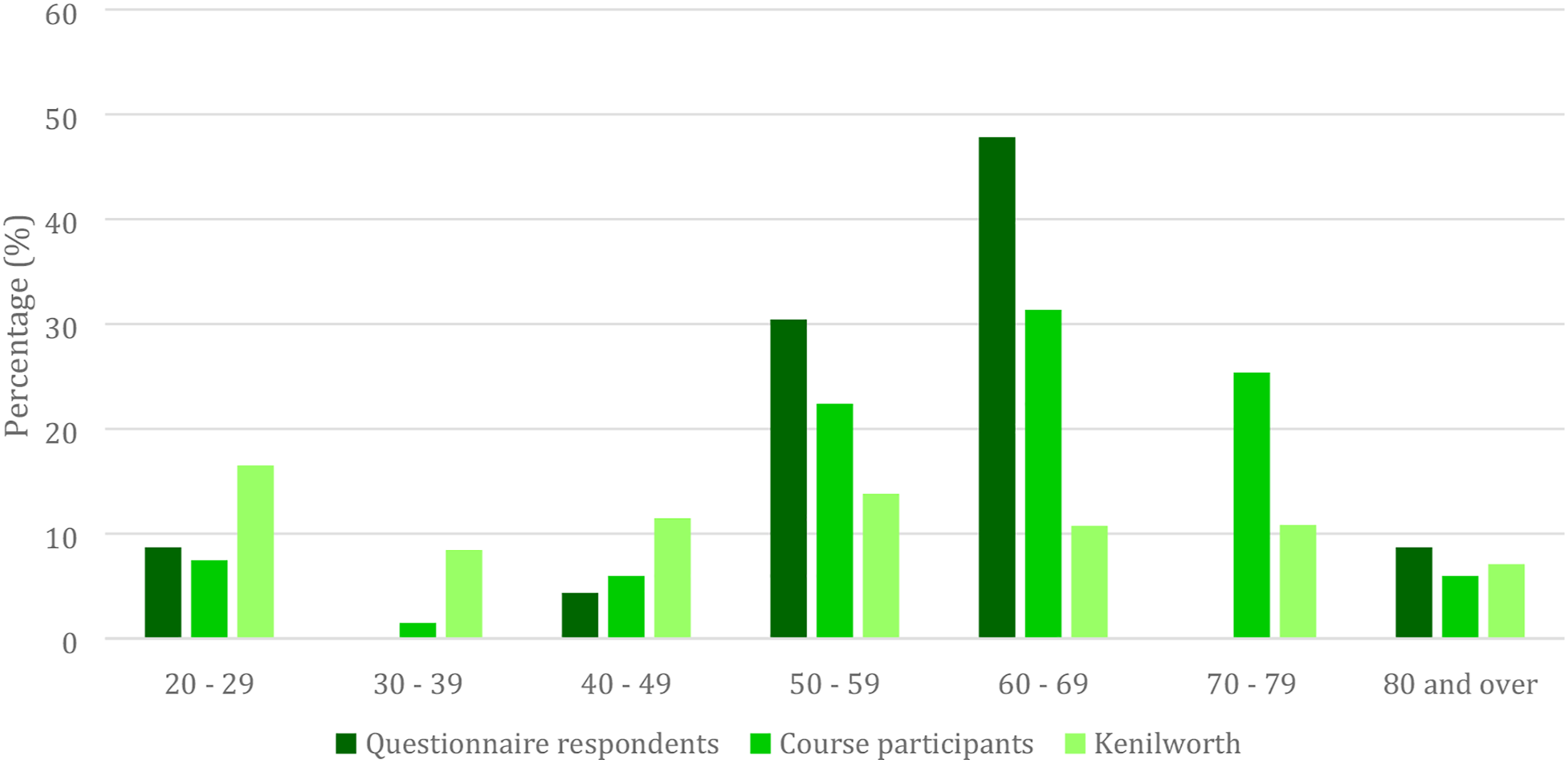
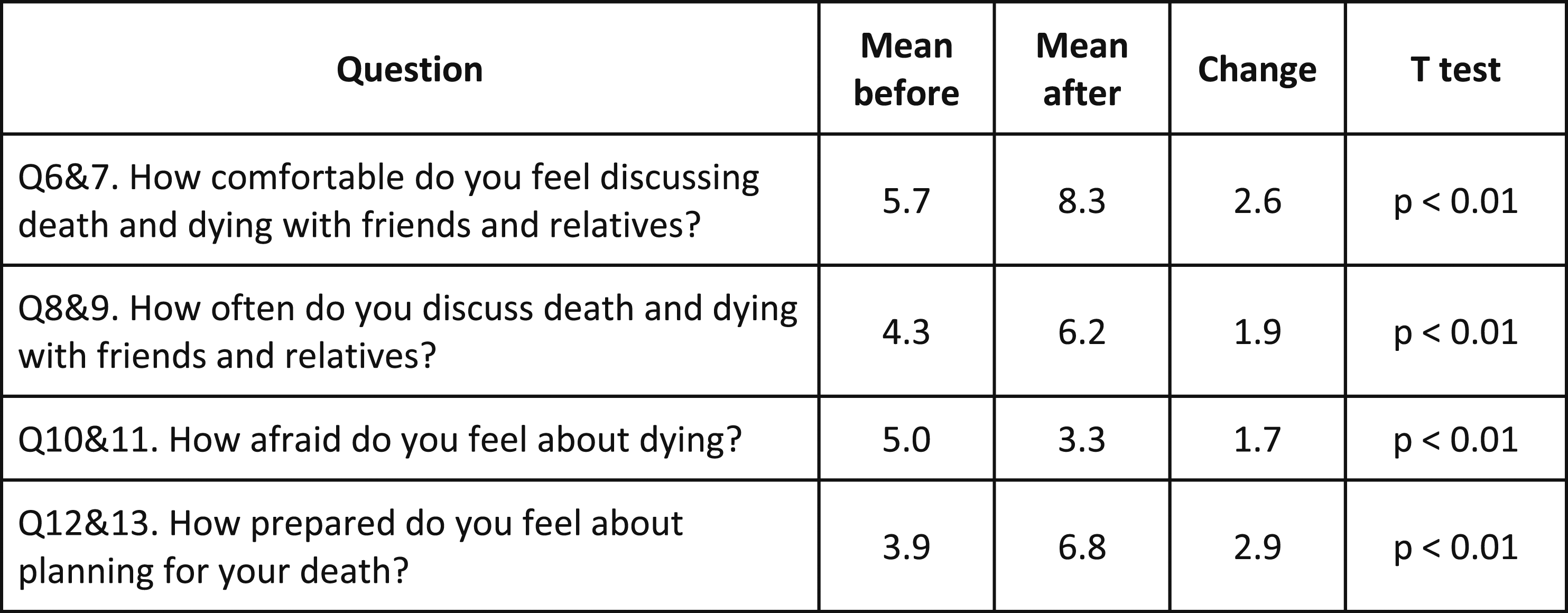
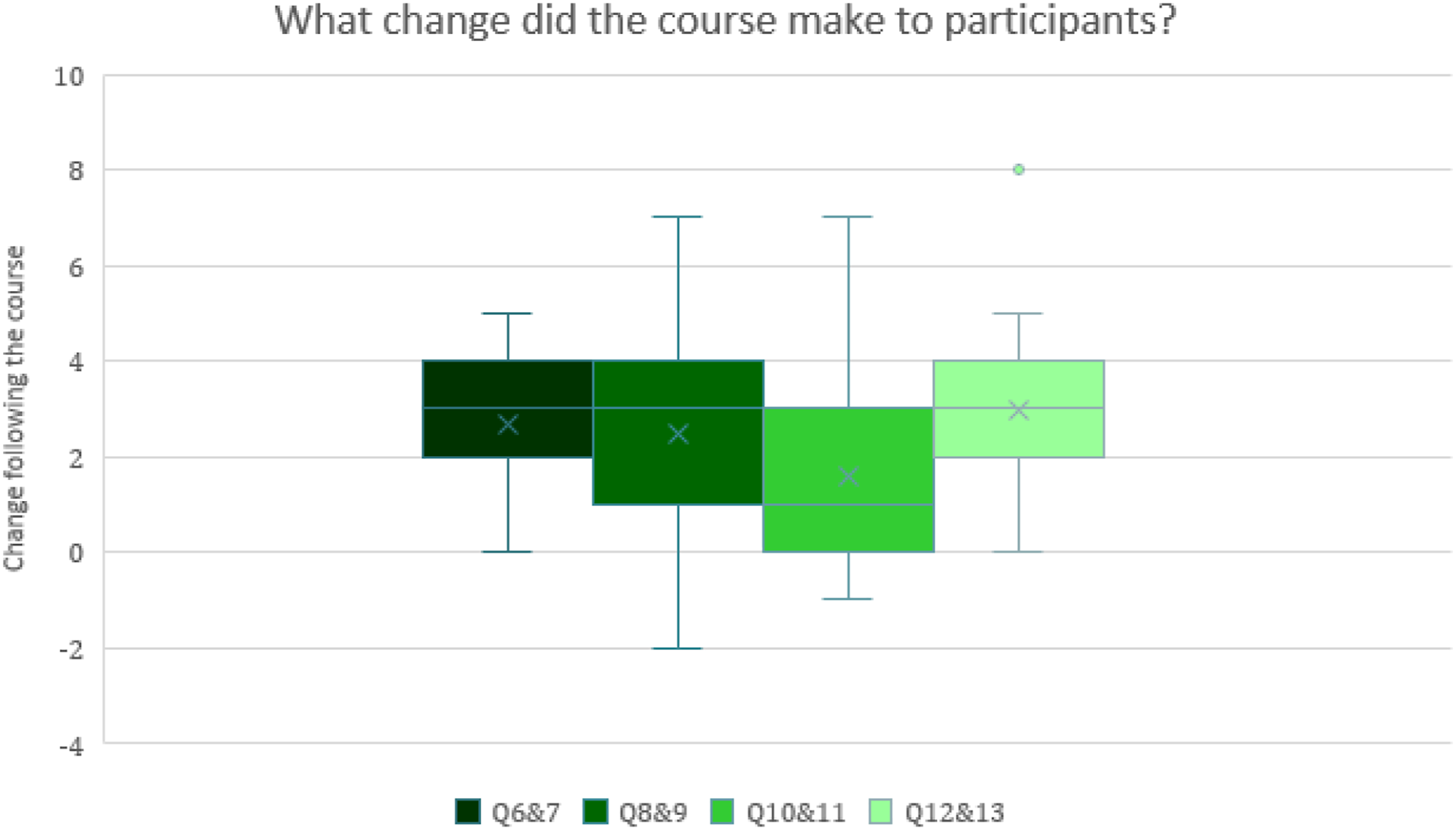
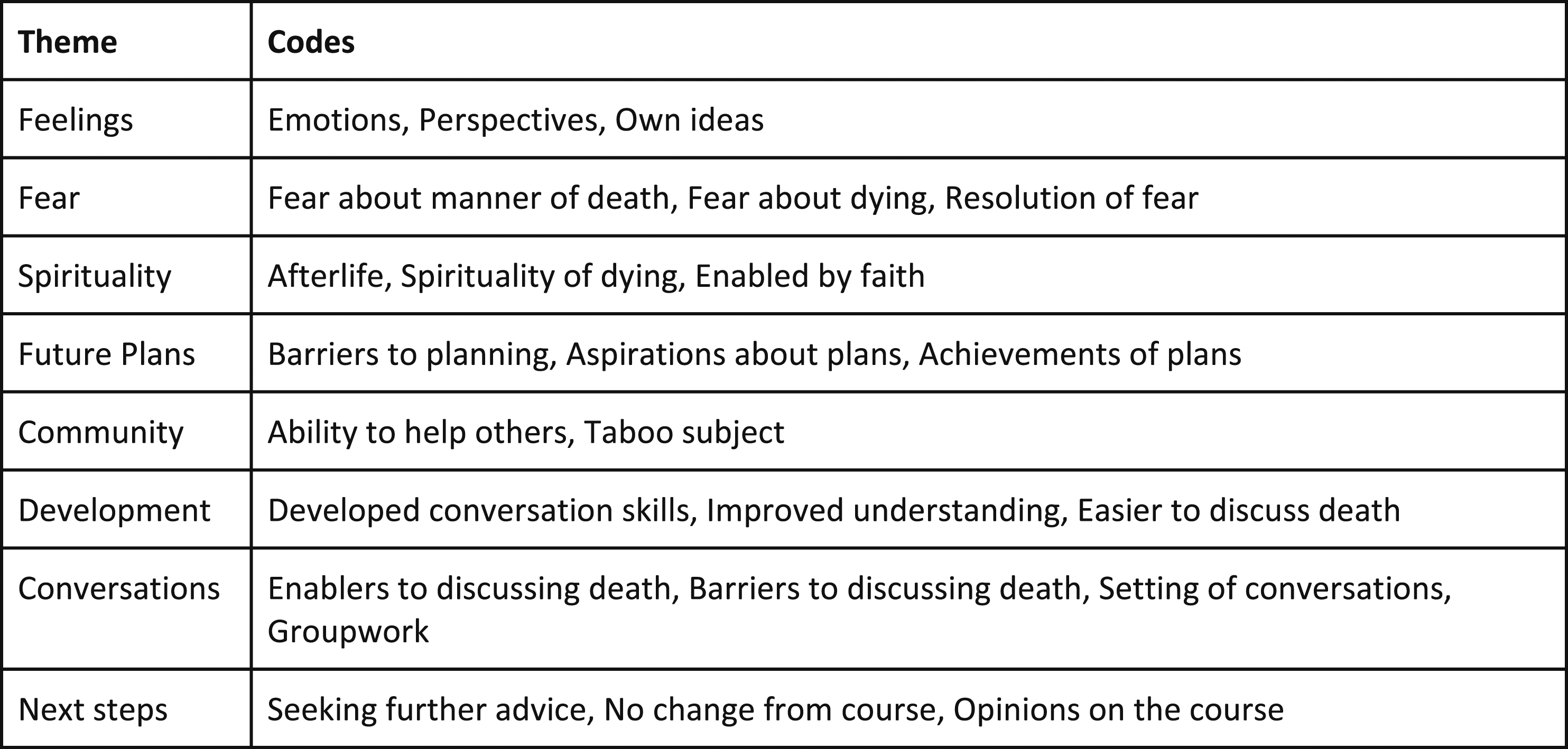
Participants’ scores suggested significant improvement in all 4 domains. Preparation to plan for death (increase of 2.9/10) and comfort discussing death (increase of 2.6/10) improved the most. Fear of death improved least (1.7/10) (Figure 2 and Figure 3). The course was rated 9.1/10 for achieving its aim ‘to enable people to talk about death and dying in a safe environment’. Thematic analysis yielded eight themes (Figure 4).
Changes to Attitudes
Respondents described prior feelings and fears. These included pain or suffering during death (quote 1), and fear about deaths of close relations. Some cited fear of loss of autonomy and overzealous medical treatment (quote 2 and 3), whilst others feared the end of their lives more than death itself, fearing their life ending prematurely or having regrets. Solace was derived from belief in an afterlife but fear of suffering during dying remained. ‘‘Fear would be inability to help others or long drawn out pain for myself’’ (Q16, respondent 11, Quote 1) ‘‘The fear is in the prolonged pain and disability and the powerlessness that accompanies it, the determination of the medical profession to keep me alive at all costs is not attractive’’ (Q16, respondent 7, Quote 2) ‘‘[I fear] a long drawn out process when one has no independence or autonomy’’ (Q16, respondent 13, Quote 3) Respondents cited increased awareness about planning being reassuring, and feeling more comfortable with uncertainty surrounding death after the course (quote 4). ‘‘[I feel] more aware of what I can do to influence the process and my treatment’’ (Q18, respondent 13, Quote 4)
Particular fears mentioned were: suffering during death, dying prematurely, death of others and powerlessness during death. There were no comments that the course had exacerbated fears.
Fears benefitted from: enabling conversation, educating about planning and encouraging new friendships. Respondents felt resigned to some fears, feeling troubled by ongoing uncertainty surrounding death that they would have to tackle personally (quote 5). ‘‘I have to accept that I may be in pain and that I may find myself in an environment where I may not be treated with compassion’’ (Q18, respondent 20, Quote 5)
The course raised awareness and encouraged respondents to confront their own mortality (quotes 6 and 7). This encouraged acceptance and practical thinking about EoL planning. Subsequent reflection on their life so far had made respondents consider their future plans (quote 6). ‘‘[the course] focussed the mind on how far you are in life, how short it is and on trying to achieve goals’’ (Q19, respondent 17, Quote 6) ‘‘The course made me more aware of this issue, although in a positive way’’ (Q18, respondent 19, Quote 7)
Changes to Actions
Respondents described barriers preventing them discussing death and dying. They feared upsetting other people or felt other people would not want to discuss death and dying, describing the topic as a ‘taboo’ (quote 8). ‘‘Society regards it as a taboo subject and stifles discussion. One is reluctant to broach the topic for fear of appearing maudlin’’ (Q10, respondent 8, Quote 8)
Another common barrier was respondents’ lack of confidence or unreconciled fears. They were restricted by not knowing what to say, or not wanting to say the wrong thing. Those who felt comfortable discussing death prior to the course drew confidence from their occupations, previous experience, or their faith. All these respondents expressed that the perceived unwillingness of others prevented them discussing death. Knowing relatives that had previously attended the course enabled discussion.
Communication skills training gave respondents insight into other people’s views. This helped them understand that similar feelings and fears were shared and this facilitated conversation (quotes 9 and 10). Respondents became more confident approaching the subject after development of their communication and listening skills (quote 11). ‘‘It’s not usually about what you say, but what you don’t. It’s more important to be available for people to listen. We need to normalise these conversations because they are important’’ (Q11, respondent 2, Quote 9) ‘‘It confirmed that what I feel, in terms of uneasiness, is common, and is therefore able to be considered and overcome’’ (Q14, respondent 7, Quote 10) ‘‘I felt more confident to try and start a conversation, having done or watched role play’’ (Q14, respondent 23, Quote 11)
Respondents improved their proficiency in planning for EoL and this subsequently enabled discussion of their wishes with family members (quote 12); making or updating their wills; and planning for their funeral. ‘‘Highlighted that you’re never too young to do things like tell people your wishes (which I have actually done) but I’m still unlikely to make a will any time soon, I have nothing of value!’’ (Q22, Respondent 4, Quote 12)
Where respondents had already made plans prior to the course, they were encouraged to update these plans or make further arrangements. Others described that whilst the course had raised their awareness of planning, they were yet to action these plans (quote 13) although some had made notes about plans they would like to make. ‘‘Helped me to talk about the plans but not as yet been proactive in putting plans down- something I am now reminded that I need to do!’’ (Q22, respondent 1, Quote 13)
Encouraging Community Development
The need for community social support and fear it would not be available was expressed. Respondents primarily feared loss of autonomy and dignity at EoL. They also feared receiving impersonal care, unresponsive to their needs (quote 3). The prospect of isolation and loneliness when dying was a challenge (quote 14). ‘‘[I fear] a long drawn out process when one has no independence or autonomy’’ (Q16, respondent 13, Quote 3) ‘‘[My fear is] being alone when I die, I am now widowed and live on my own, I have no children’’ (Q16, respondent 5, Quote 14). Some responses referenced development of elements of social capital.
26
New friends were made on the course and respondents felt better able to help others (quote 15). ‘‘It helped me to be able to stand alongside friends and relatives going through traumatic times in their lives’’. (Q14, respondent 10, Quote 15)
Discussion
Omega Course Outcomes
This study found that the course was appreciated and well-received by respondents, rated 9.1/10 for achieving its aims. Respondents deemed group work and scenario-based role-play effective, improving their communication skills and providing opportunities for practice. They appreciated the supportive, unthreatening environment15,16 which was effective in improving comfort of discussing death, dying and future planning. Respondent’s scores for ‘comfort discussing death and dying’ increased (mean 5.7 cf. 8.3, P < .01), and they had discussions more often (mean 4.3 cf. 6.2, P < .01). After the course, respondents rated themselves as feeling more comfortable discussing death compared to how often they actually did so, suggesting that respondents are inhibited by external factors. As in previous research, respondents perceived ‘unwillingness of others’, and ‘the situation not arising’ as discussion barriers.16,17
Fear of death improved least; reflecting the highly personal nature of this fear and the uncertainty that necessarily persists, despite pre-planning, when any future illness is as yet unknown. Similar education in patient groups, dying from a known illness would make a useful comparison.
Before the course participant’s fears reflected national survey data.16,17 Feeling afraid, powerless, or lacking knowledge prevented respondents making plans. The course helped acceptance of mortality and empowered respondents to feel more in control of the process and open to advance care planning. After the course respondents reported improved proficiency in EoL planning and were more prepared to plan for death, intending to act, or making notes in preparation to discuss their wishes with family members. They were writing or updating wills and making funeral plans. These early practical outcomes are indications of success.
These results suggest that the course encouraged initiation of ACP in healthy adults despite the challenge of unpredictable illness.
27
ACP is important in health, not just in old age, chronic disease or terminal illness. Even younger respondents, as in other studies, acknowledged the need for ACP in case of sudden illness or incapacity left family with distressing decisions and uncertainty.23,27 ‘The value of planning is partly about increasing knowledge, developing realistic expectations and so being better prepared to adapt and respond to circumstances as they evolve.’ p. 39 A Road Less Lonely
28
Encouraging community development
Respondents feared loss of autonomy and dignity at EoL, receiving impersonal care unresponsive to their needs, as well as isolation and loneliness. Social networks within caring communities would be best placed to meet these needs and so fulfil a principle of Public Health Palliative Care. 4 Social capital 26 increased during the course through new friends, enablement to offer help, better listening and talking skills. The group environment fostering group discussion and support suggests group dynamics are integral to the success of the course.
Some respondents had not fulfilled their intended plans indicating more follow up after the course may be beneficial in promoting action. Community development so early in course delivery is harder to demonstrate but social capital developed.
This independent course was not affiliated to any healthcare or educational institution, despite overtures to the statutory and voluntary sector. This echoes professional services’ unease with non-professional community ventures. 29
Strengths and Limitations of the Study
This early evaluation study is small, and hence its findings require cautious interpretation. The respondents were broadly representative of Omega participants demographically. Those attending Omega and responding to the survey had a median age of 64 years, with around 70% being female. It is recognised that despite the known value of ACP for healthy young adults, 23 older female adults are more likely to engage with it than other demographic groups,30,31 and therefore have fewer burdensome interventions at EoL.30-32
Kenilworth is an affluent area with few ethnic minority residents, only 1 participated in Omega. The level of education was high and known to be an important factor in engaging with ACP. 32 This may influence reproducibility in other more diverse communities.
The relatively low response rate of 37%, in part, reflects the study design, without reminders after the initial request for participation, and a short time frame. The response rate raises the question of non-responder bias, responders possibly answering more favourably. Furthermore, retrospective enquiry about ‘pre-course scores’ may incur recall bias, exacerbated by varying intervals after course completion. Validation of the research questionnaires will be important.
The results pertain to 1 delivery team. Training more facilitators will be important for course expansion and assessing reproducibility. The personal, experiential nature of the course makes finding suitable facilitators challenging, particularly teaching technicalities of ACP, and communication skills training. A facilitator manual is being tested and films used for parts of the course when skills are lacking.
These limitations highlight the importance of further research into reproducing the approach, and ongoing efforts to assess the effectiveness of the intervention.
Conclusion
This complex intervention of facilitated group discussions, presentations, and role play about death and dying, supported by social functions, seemed to be effective in providing a safe environment for discussion, delivering knowledge and the chance to practice skills. The uptake of ACP is especially low in the pre-morbid population but this pilot study may suggest The Omega Course could be effective in encouraging discussion, promoting planning and enhancing individual autonomy for ACP in healthy adults. Future research should focus on reproducibility between facilitators, deprived and ethnically diverse populations, gender utilisation and comparison with patient groups.
Supplemental Material
Supplemental Material - Do Healthy People Engage With Education About Death, Dying and Advance Care Planning? An Early Evaluation of the Omega Course
Supplemental Material for Do Healthy People Engage With Education About Death, Dying and Advance Care Planning? An Early Evaluation of the Omega Course by Ieuan Davies, Chantal Meystre, and Jeremy Dale in American Journal of Hospice and Palliative Medicine
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.