
Abstract
This research was conducted descriptively to determine the symptom intensities, performance and hopelessness levels of advanced lung cancer patients for the palliative care approach. The research sample consisted of 130 patients with advanced lung cancer, who were selected from 600 lung cancer populations in thoracic surgery and intensive care, outpatient chemotherapy, oncology in a university hospital in Turkey. Ethics Committee permission and the patients’ written consent was obtained. Study data were collected face to face between January 2020 and July 2020 using the Edmonton Symptom Assessment System, Karnofsky Performance and Beck Hopelessness Scale. The mean age of the patients was 62.68 ± 8.867, 72.3% were males, and 89.2% were not currently working. The most common symptom in the patients was found to be fatigue 5.46 ± 2.12, worsening in general health and well-being 5.69 ± 1.87, loss of appetite 5.40 ± 2.59, and total symptom score 47.17 ± 19.03. Feelings and expectations about the future 1.40 ± 1.66, loss of motivation 3.43 ± 2.41, hope 2.05 ± 1.75, and total score of hopelessness 7.41 ± 6.01. There was a positive correlation between the patients’ hopelessness level and their symptom burden, and a negative correlation was found with Karnofsky performance (P < .05). A significant difference was found between the patients’ age, months since diagnosis, gender, education and employment status, stage of the disease, presence of metastases and analgesic use, and hopelessness scores (P < .05). It was determined that the symptom burden of patients with advanced lung cancer increased and as their Karnofsky performance decreased, their hopelessness level further increased. Hopelessness scores are affected by the socio-demographic and disease variables of the patients.
Keywords
Introduction
Lung cancer has a high mortality rate and is among the first causes of cancer-related deaths worldwide.1,2 Patients with advanced lung cancer experience many different physical symptoms, particularly dyspnea, and also frequently experience psychological and social problems brought about by the disease and these symptoms.3,4 In a study by Sung et al, 5 it was discovered that the most common symptoms in patients with advanced lung cancer were fatigue, cough, and dyspnea. 5 Kapo found that patients with advanced lung cancer often experienced pain, apnea and fatigue; their quality of life was low, and these symptoms affected 65% of the patients. 6 Wilcock et al 7 stated that lung cancer patients are in need of palliative care because of their poor performance, so they should be admitted to the palliative care unit. 7 In a study on lung cancer, Bulbul et al stated that patients had unmet needs, and that they did not recover from pain and dyspnea. 8 In a study by Maguire et al, it was determined that dyspnea affected the physical and psychosocial lives of patients with advanced lung cancer in the short term, and in the long term it caused hopelessness. 9 A study carried out with 309 advanced lung cancer patients, stated that 89% of the patients had to apply to the hospital urgently regarding the problems they experienced, and this hospitalization rate had increased in the previous 3 months. 10 Therefore, it is very important to evaluate the symptoms and functional status of advanced lung cancer patients for the palliative care approach.
Assessment of hopelessness is also of critical importance in diseases with intensive clinical treatment such as lung cancer because hopelessness is a basic element of a depressive disorder and a predictor of suicidal tendencies. 11 Clinical results have shown that hopelessness, demoralization, and a bad mood will negatively affect the quality of life of advanced cancer patients.12,13 However, hopelessness has been predicted to increase mortality in advanced cancer patients.14,15 Hannah Ball et al suggest that the psychological problem of patients with advanced lung cancer are related to uncertainty, hope, hopelessness, stigma, guilt, family and caregiver anxiety, physical distress of the disease, experience of tragedy caused by diagnosis, unexplained distress. 10 In a systematic, it was discovered that patients with lung cancer experienced uncertainty about their future at a rate of 13–70% in the terminal period and had high levels of hopelessness. 9 Therefore, it is highly important to determine the level of hopelessness experienced by advanced lung cancer patients.
In Turkey, advanced stage lung cancer patients are followed primarily in Thoracic clinics, Thoracic Intensive Care intensive care, and Thoracic Surgery clinics of state hospitals and medical faculties. They also receive health services from palliative care services in hospitals and from internal medicine clinics. There are palliative care services in state hospitals and medical faculties in Turkey. Especially after 2014, palliative care delivery and the number of beds increased rapidly in Turkey. 16 However, it seems that the formation of a palliative care philosophy and trained health professionals and its integration into the health system will take time. In our country, as in the world, there are problems regarding the transition of advanced lung cancer patients to early palliative care. Bulbul et al determined that symptoms progressed and intensified in the advanced stages of lung cancer, and that palliative care was inadequate for most patients in Turkey. 8 In a study, it was determined that advanced cancer patients in our country applied to the emergency department with complaints of dyspnea and pain. 17 In another study, it was observed that patients with advanced non–small cell lung cancer had low quality of life, impaired psychological and physiological functions and could not receive adequate health care services. 76.2% of the patients asked the doctor to “relieve pain,” 10.4% asked the nurse to “eliminate pain and discomfort,” and 9.8% asked the psychologist to “reduce sadness and grief.” It was determined that 1.6% had expectations from a dietitian for “prevention of weight loss,” 1.3% had expectations from a social worker for “elimination of relationship disorder with relatives,” and .6% had expectations from physiotherapists for “elimination of muscle weakness.” 18
In our study, we aimed to draw attention to the symptoms, performance, and hopelessness problems experienced by advanced lung cancer patients. We wanted to provide data on symptom levels, performance, hopelessness, and the connections between them in the diagnosis of transition to palliative care in these patients. Therefore, this study aimed to determine the symptom intensities, performance, and hopelessness levels of advanced lung cancer patients for the palliative care approach.
Materials and Methods
This research is a descriptive study carried out to determine the symptom intensities and hopelessness levels of advanced lung cancer patients for the palliative care approach. The study was conducted in the following departments of a medical faculty hospital in Turkey, where advanced lung cancer patients are frequently followed up and treated: Thoracic Surgery, Thoracic Surgery Intensive Care, Outpatient Chemotherapy Unit, Oncology, Oncology Outpatients’ Department and Chest Diseases Clinic.
The population of research consisted of 600 lung cancer patients who were being treated and followed up in the medical faculty clinics. For the research sample, 130 patients with advanced stage lung cancer who met the research criteria with a 95% confidence interval and a 5% margin of error were chosen using a population-specific sampling method. Patients who were over 18 years old, conscious, cooperative and oriented, without vision or hearing problems, able to communicate verbally, and diagnosed with stage III and IV lung cancer were included in the study.
A socio-demographic form, the Beck Hopelessness Scale, the Edmonton Symptom Assessment System Scale (ESAS), and the Karnofsky Performance Scale were used as data collection tools in the research. The socio-demographic form consisted of 20 questions prepared by the researcher by scanning the literature in order to determine the socio-demographic and disease-related characteristics of the patients.19‐21 We used simple and easy-to-answer tools with validity and reliability. These tools are also frequently used in palliative care settings. The ESAS was developed to diagnose existing symptoms in patients with palliative cancer. Symptom monitoring was made by nurse with ESAS. The ESAS was developed by Bruera et al (1991) to diagnose the symptoms present in patients with advanced cancer. The validity and reliability of the ESAS in the Turkish population was tested by Usta et al in 2008, and the Cronbach alpha level of the scale was found to be >.70. The ESAS covers 9 symptoms seen in patients such as pain, fatigue, nausea, depression, anxiety, drowsiness, appetite, well-being, and dyspnea and an alternative choice of “other symptom.” It is designed in a visual analog or numerical style, where the symptoms on the scale can be marked between 0 and 10. The total score of the ESAS varies between 0 and 100 points, and high scores obtained from the scale indicate a higher symptom level.22,23 After this assessment, advanced lung cancer patients’ high symptom load and intensity on the scale indicate that the patients have palliative care approach.
The Karnofsky Performance Scale was developed by Karnofsky in 1948. This scale evaluates patients’ general and functional status on a scale ranging from 0 to 100 points. In the scale, the patients’ symptoms, ability to perform daily activities, dependency status, and need for medical care are interrogated. A score of 100 points indicates normal health status, and zero points correspond to death. According to the results of the evaluation, patients within the 80–100% category do not need special care, and can continue their normal activities and work; patients in the 50–70% category can perform their personal care with help but cannot work, and patients in the 0–40% category cannot take care of themselves and their situation may quickly proceed to death. 24
The Beck Hopelessness Scale (BHS) is a scale developed by Beck in 1974 to determine the level of hopelessness in patients with advanced cancer, and aims to measure the individual’s future expectations and pessimism levels. The scale consists of 20 items and statements expressing patients’ feelings and thoughts about the future. 25 The validity and reliability of the Turkish scale was tested by Seber (1991) and Durak (1993). 26 Patients are requested to mark the “correct” option for statements that apply to them and the “incorrect” option for statements that do not fit them. There are 11 “yes” and 9 “no” answer keys. Positive answers given to the following questions: 2, 4, 7, 9, 11, 12, 14, 16, 17, 18, and 20, score 1 point, and negative answers given to questions 1, 3, 5, 6, 8, 10, 13, 15, and 19 get zero points. There are 3 sub-scales. Items 1, 6, 13, 15, and 19 are about feelings relating to the future, and items 4, 7, 8, 14, and 18 are about expectations related to future. A high score obtained from BHS indicates high levels of hopelessness or negative expectations for the future.25,26
Research data were collected between January and July 2020. The purpose and method of the study were explained to the patients participating in the study, and their verbal and written consents were obtained. Research data were obtained by the researcher through using the socio-demographic form, Beck Hopelessness Scale, ESAS, and Karnofsky Performance Scale. The research data were evaluated using SPSS 22.00 (Statistical Program for Social Sciences) program package for analysis. The Shapiro–Wilk test was used to examine whether the data showed normal distribution. In evaluation of the data, the average scores of the scales were calculated using numbers, percentages, and frequencies. The Kruskal–Wallis, Mann–Whitney U and Pearson correlation tests were used in the analysis of the research data. The relationship between symptom burden and hopelessness was determined by the Pearson correlation test. The significance level was accepted as P < .05.
In order to evaluate the ethical suitability of the study, the approval of the Non-Interventional Research Ethics Committee of a local university (30.09.2019 - 25449) and the written permission of the Medical Faculty Hospital were obtained.
Results
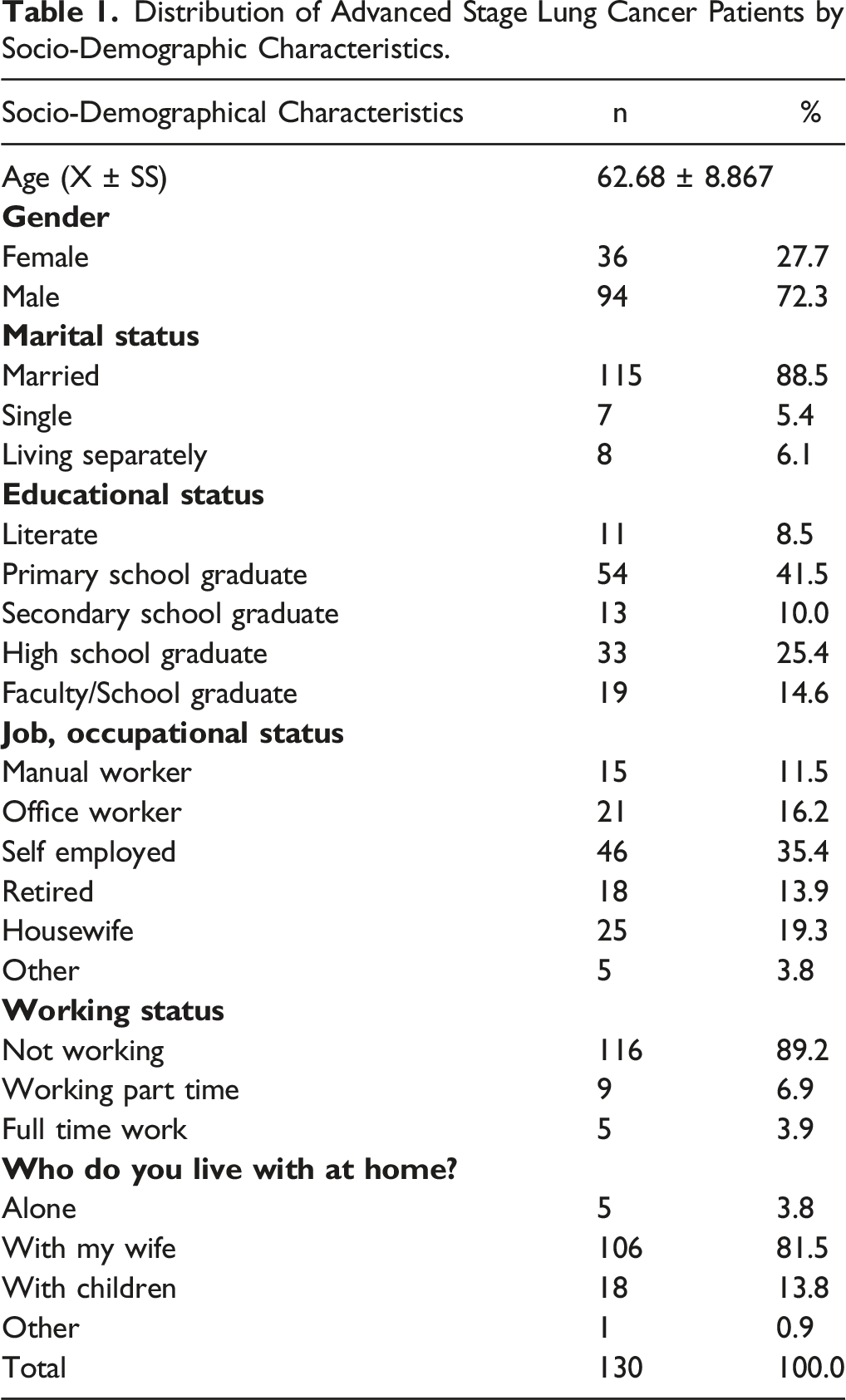
Distribution of Advanced Stage Lung Cancer Patients by Socio-Demographic Characteristics.
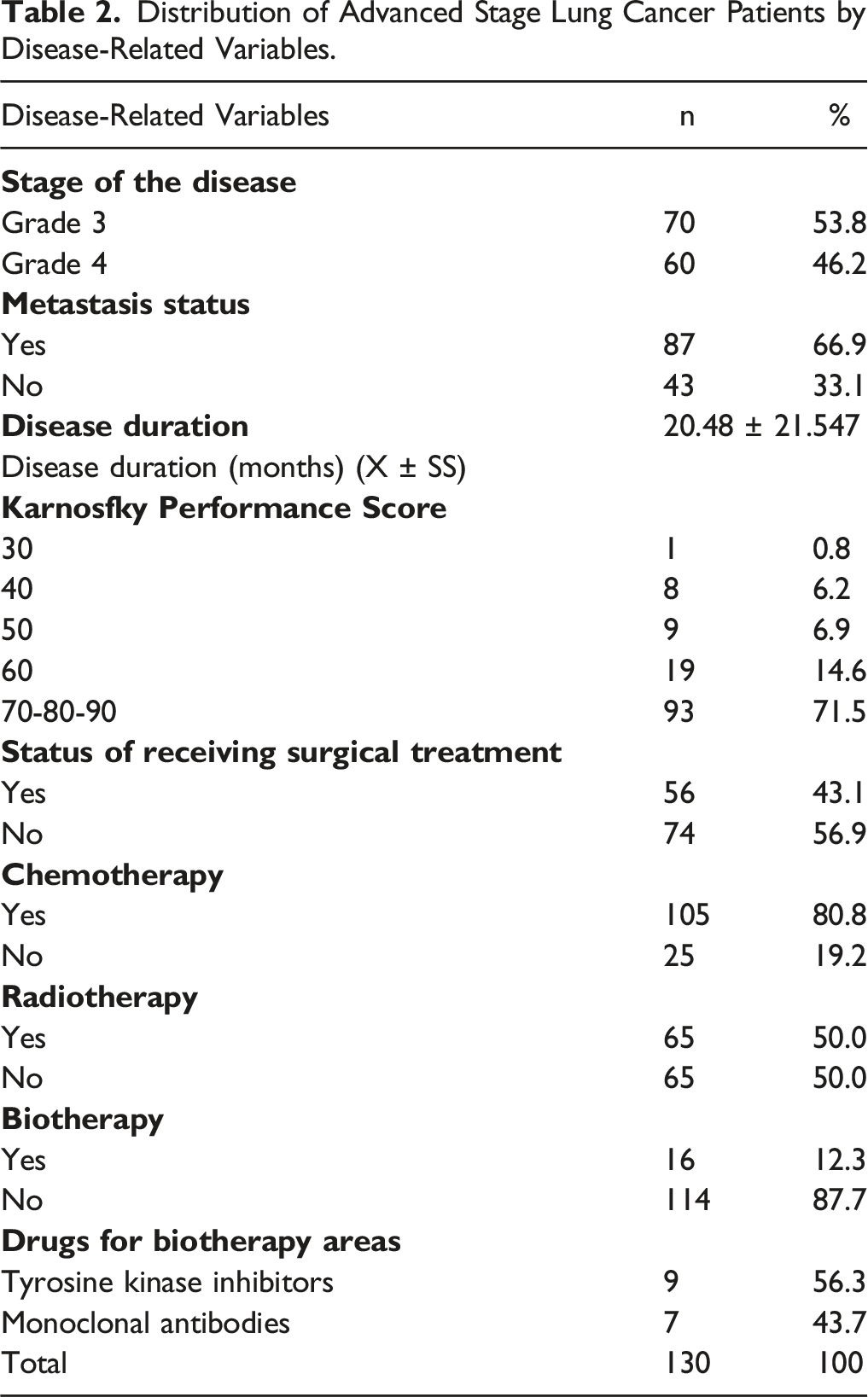
Distribution of Advanced Stage Lung Cancer Patients by Disease-Related Variables.
The Distribution of Patients With Advanced Stage Lung Cancer Edmonton Symptom Sub-Dimensions and Total Score/Score.
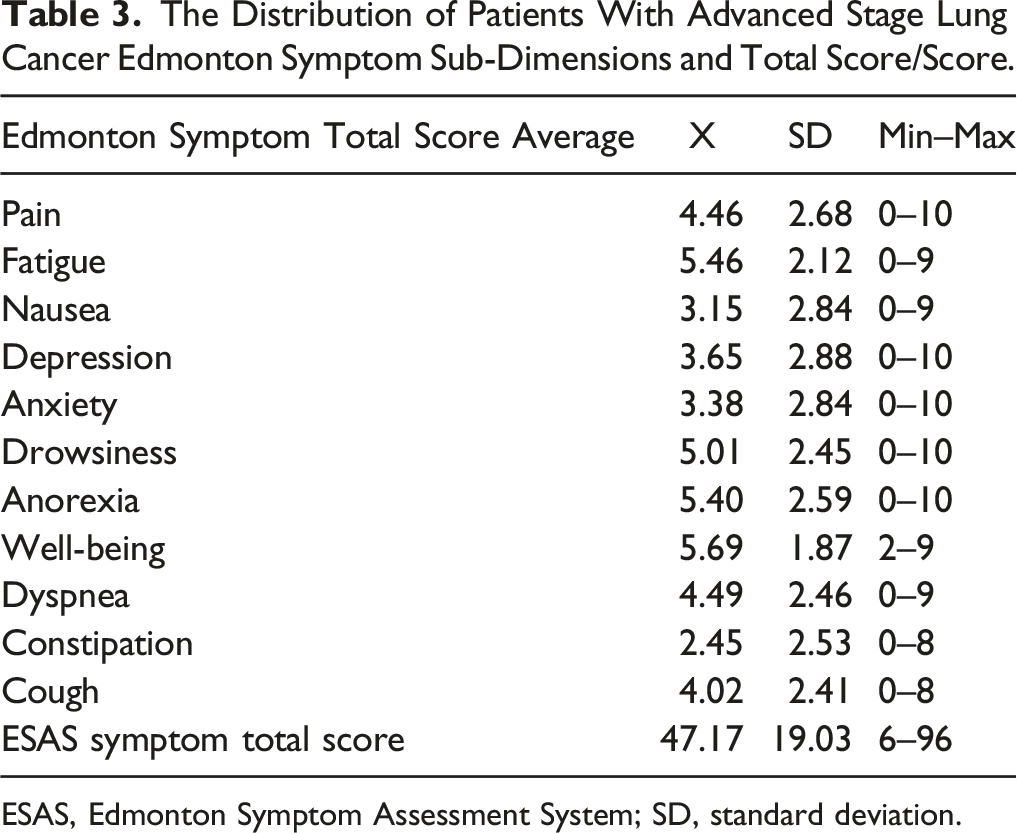
ESAS, Edmonton Symptom Assessment System; SD, standard deviation.
The Relationship Between Edmonton Symptom Total Score, Hopelessness Total Score and Sub-Dimension, Karnofsky Performance Score.
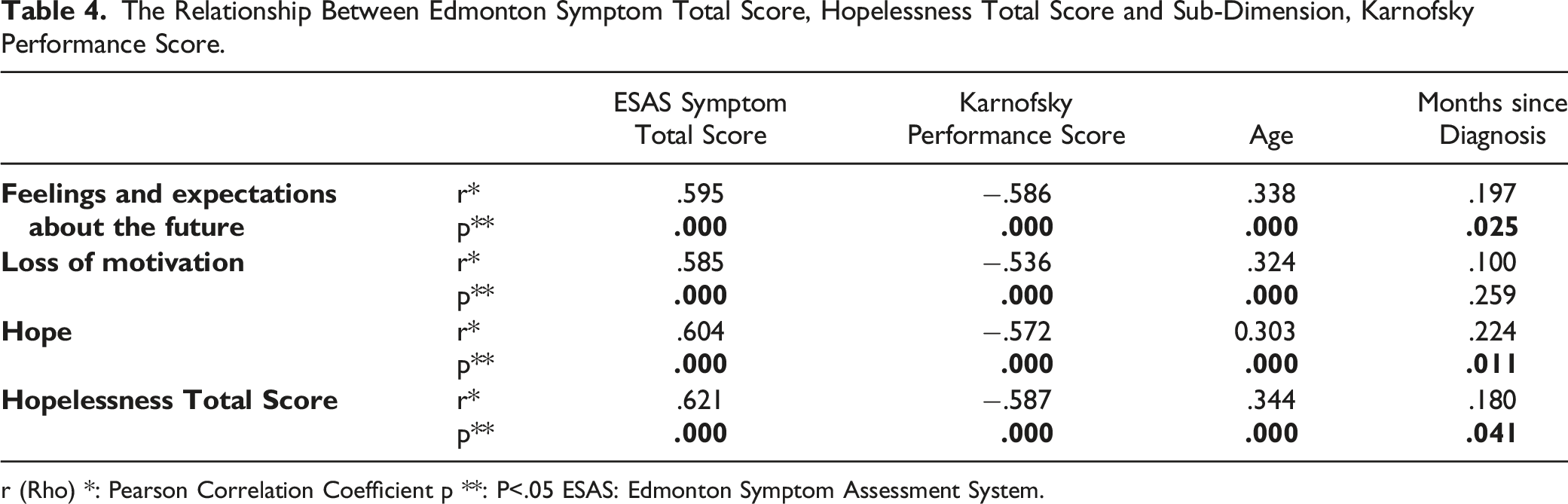
r (Rho) *: Pearson Correlation Coefficient p **: P<.05 ESAS: Edmonton Symptom Assessment System.
Distribution of Socio-Demographic Characteristics of Advanced Stage Lung Cancer Patients by Edmonton Symptom Total Score, Karnofsky Performance, Hopelessness Total and Sub-Dimensional Score Averages.
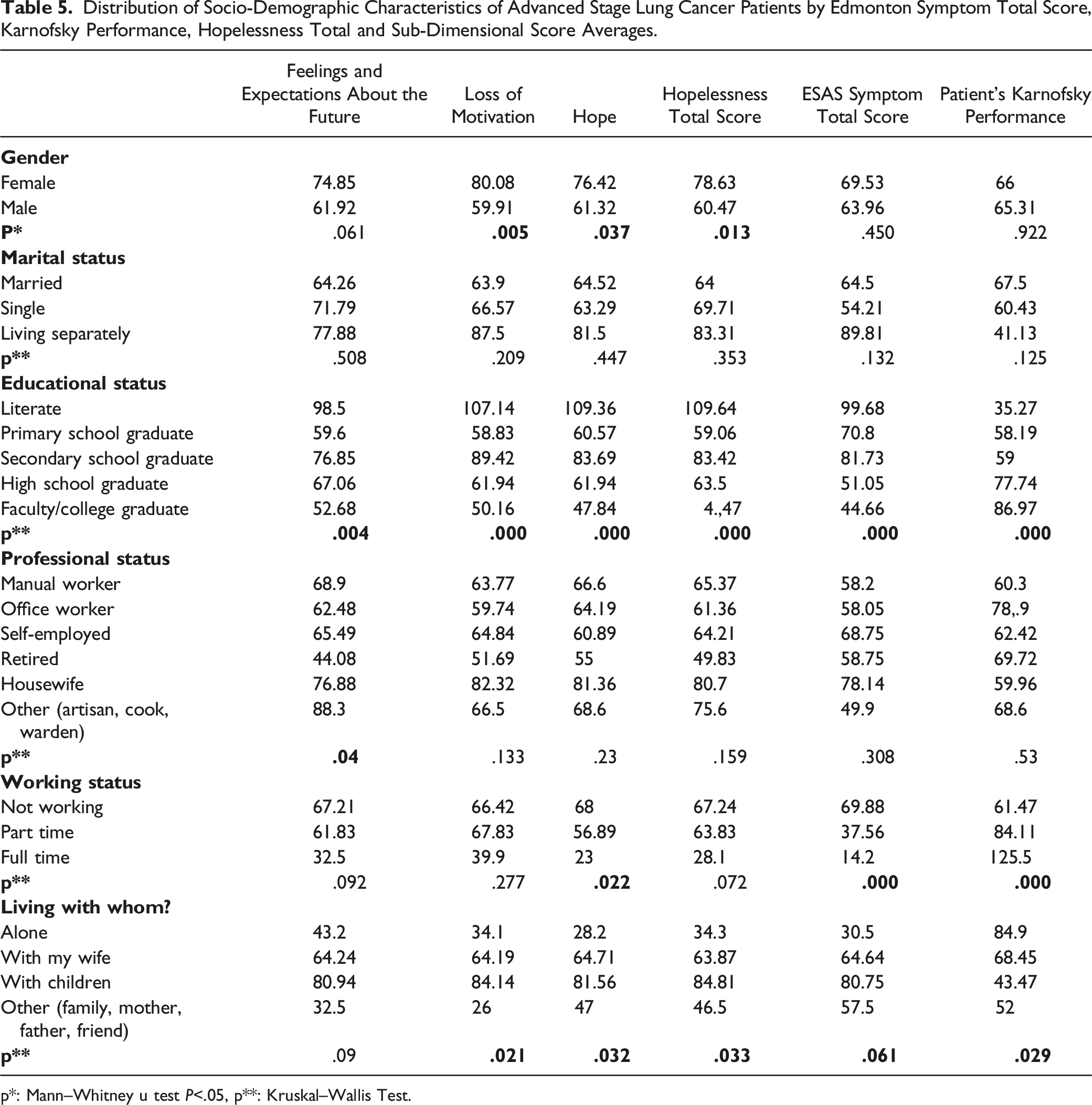
p*: Mann–Whitney u test P<.05, p**: Kruskal–Wallis Test.
Discussion
Among the symptoms that patients will apply to the palliative care approach, the most frequent and highest were as follows: fatigue, worsening in general health and well-being, and anorexia symptoms, these were followed by drowsiness, dyspnea, pain, cough, depression, anxiety, nausea, constipation, and symptom total mean score with 47.17 ± 19.03. Similar to our study in the literature, fatigue, deterioration in general health, loss of appetite, and dyspnea are the most common symptoms. In our study, unlike the literature, pain was seen at lesser rates. However, the symptom burden of our patients that needed to be eliminated was found to be high. Yogananda et al 27 discovered that 89.5% of advanced lung cancer patients reported that they experienced fatigue, 85.7% dyspnea, 85% anorexia, 82% pain, 85.6% feeling bad, 81.1% anxiety, 78.9% depression, 49.6% nausea, and 29.3% drowsiness. 27 Sung et al 5 found that advanced lung cancer patients’ physical symptoms of were similar and the most common symptoms were fatigue, cough, and dyspnea. 5 Tanaka et al 28 determined that advanced lung cancer patients suffered from dyspnea the most, followed by fatigue and pain. 28 Potter et al reported that lung cancer patients experienced pain most frequently. 29 Kapo found that patients with advanced lung cancer most often experience pain, dyspnea, and fatigue; those symptoms affected 65% of the patients. 6 Bulbul et al stated in a study carried out on lung cancer that patients had unmet needs and pain and dyspnea, and did not improve. 8
It was suggested that hopelessness experienced by advanced cancer patients admitted to palliative care would affect mortality from the disease.14,15 In our study, we found in patients with advanced lung cancer that among the hopelessness sub-dimensions, the score for feelings and expectations about the future was 1.40 ± 1.66, for loss of motivation it was 3.43 ± 2.41, and for hope it was 2.05 ± 1.75. The mean total score of hopelessness was 7.41 ± 6.01. At the same time, it was observed that the patients most frequently experienced loss of motivation and moderate hopelessness in this process. Similar to our study, there are studies in the literature that found mild to moderate hopelessness, as well as studies that found hopelessness high, especially in the terminal period. In a study carried out by Bozdogan et al lung cancer patients, the score for the hopelessness sub-dimensions of feelings and expectations about the future was found to be .87 ± 1.19, for motivation loss 3.56 ± 1.83, and for hope 1.41 ± 1.47, and the total score of hopelessness was 5.84 ± 3.55. 30 Maguire et al 9 found that patients with lung cancer experienced uncertainty about their future at a rate of 13–70% in the terminal period and had high levels of hopelessness. 9 Mystakidou et al 31 determined that 70.6% of cancer patients diagnosed with lung cancer and already receiving palliative care had poor performance and a mild hopelessness level according to ECOG performance. 31 Ball et al discovered that patients with mesothelioma and lung cancer experienced multifaceted and complex psychological distress. 10 Rodin et al 32 found that patients with Stage IV gastrointestinal and lung cancer had a Karnofsky performance scale of 81.55 and a low level of hopelessness. 32
In our study, as the symptom burden of patients with advanced lung cancer increased and as their Karnofsky performance decreased, their hopelessness level further increased. A positive correlation was found between hopelessness levels and symptom burden and a negative correlation was found with their performance. Similar to the literature, it was determined in our study that the symptoms could increase the level of hopelessness even more. In a study by Maguire et al, it was determined that dyspnea affected the physical and psychosocial lives of patients with advanced lung cancer in the short term, and in the long term it caused hopelessness. 9 In a study by Steffen et al 33 where a majority of patients had stage IV non–small cell lung cancer, they found that patients with high hope levels experienced less fatigue and pain. 33 Berendes et al 34 found that as hope decreased, pain, fatigue, cough, and depression increased. 34 It has been shown in the literature that the level of hope can be increased by reducing the burden of symptoms. These findings once again showed that hopelessness should be screened in advanced lung cancer patients.
In our study, we detected that as age and months since diagnosis increased and the disease progressed in patients with advanced stage lung cancer, their hopelessness level increased and their performance decreased. A significant difference was found between gender and hopelessness and sub-dimension scores. Women’s hopelessness levels and loss of motivation rates were higher than those of men. A significant difference was found between education and employment status, stage of disease, presence of metastasis, use of analgesics and total and sub-dimension scores. Similarly, in a study by Mystakidou et al, there was a positive relationship between hopelessness levels of patients with lung cancer and depression, age and gender, whereas there was a negative relationship between performance level and hopelessness level. 31 Temel et al 35 found that the age and gender of cancer patients can change both their cancer experiences and palliative care needs. 35 Fadıloglu et al 36 reported that there was a significant difference between the hopelessness levels of breast cancer patients over 60 years of age, and that the level of hopelessness increased as patients’ age increased. 36 Differently, Bozdogan Yesilot et al 30 found no significant difference between the age of lung cancer patients and the level of hopelessness. 30 Bener et al 37 stated that there was a significant difference between the education level of breast cancer patients and their level of hopelessness. 37 Cam et al suggested that breast cancer patients can show different and complex behavioral and emotional responses at every stage of the disease process. The reason for these reactions was the different sociocultural structure of the region where patients lived, and they were affected by this sociocultural structure. 38
As a result, it was determined that fatigue, deterioration in general health, and loss of appetite were the most common symptoms in advanced lung cancer patients and the symptom burden of the patients was high. There was a positive correlation between patients’ hopelessness level and the symptom burden and a negative correlation between performance scores. It was determined that the symptom burden of patients with advanced lung cancer increased and as their Karnofsky performance decreased, their hopelessness level further increased. A significant difference was found between the patients’ age, months since diagnosis, gender, education and employment status, stage of the disease, presence of metastases and analgesic use, and hopelessness scores.
Footnotes
Acknowledgments
The authors thank all patients for their willingness to participate.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was in accordance with the principles of Declaration of Helsinki and all subjects provided written informed consent. The study protocol was accepted by the Nigde University Ethics Committee (27.09.2019/10).