
Abstract
Background:
Hospices provide multidimensional care. In the Netherlands, patients with <3 months estimated life expectancy have access to hospice care. Insight into patients admitted to hospices and the care provided is lacking. In preparation for a national multicenter study, a pilot study was performed.
Objective:
The primary objective was to test the appropriateness of the study procedures and the availability of hospice patient records (HPRs), and patient and care characteristics.
Method:
A cross-sectional pilot study was performed using a descriptive exploratory design. Sixteen hospices were invited to participate, and HPRs from 8 deceased patients per hospice were selected. Data were collected using self-developed electronic case report forms.
Outcomes:
(1). Appropriateness of procedures: availability of HPRs and identified barriers and strategies. (2) Availability of patient and care characteristics in HPRs.
Results:
In total, 104 HPRs of patients from 13 hospices were enrolled. Various types of HPRs were found with different availabilities: nurses’ records were most available (98%) compared to volunteers’ records (62%). Overarching barriers were as follows: ethical issues, lack of knowledge, and lack of communication. Information about the illness was most available (97%), whereas descriptions of experienced symptoms were least available (10%).
Conclusion:
Collecting HPRs is difficult and time-consuming. Specifically, data from separate records of home care nurses and general practitioners were difficult to come by. Patient and care characteristics were alternately present, which led to an extension of data collection in HPRs to 3 time periods. Piloting is essential to adjust study procedures and outcome measures to ensure a feasible national multicenter hospice study.
Introduction
In 2017, approximately 149 400 people died in the Netherlands, and this number will increase to over 200 000 in 2050.
1
Estimating that more people will die a non-sudden death, the need of palliative care will become more important.
2,3
The Netherlands has approximately 300 hospices,
4
which are divided into 3 types: Volunteer-driven hospices (VDHs), where care is provided by trained volunteers and family members and medical care by the patient’s own general practitioner (GP) and district nurses
5
Professional-driven hospices- hospice unit nursing homes (HUs), which are specialized wards in nursing homes. Professional driven hospices- stand alone hospices (SAs), which are small-scale care organizations. Care is provided by a multidisciplinary team, consisting of a nursing staff, specialized palliative care nurses, physicians specialized in palliative care (of geriatric medicine), and (trained) volunteers (Figure 1).
6
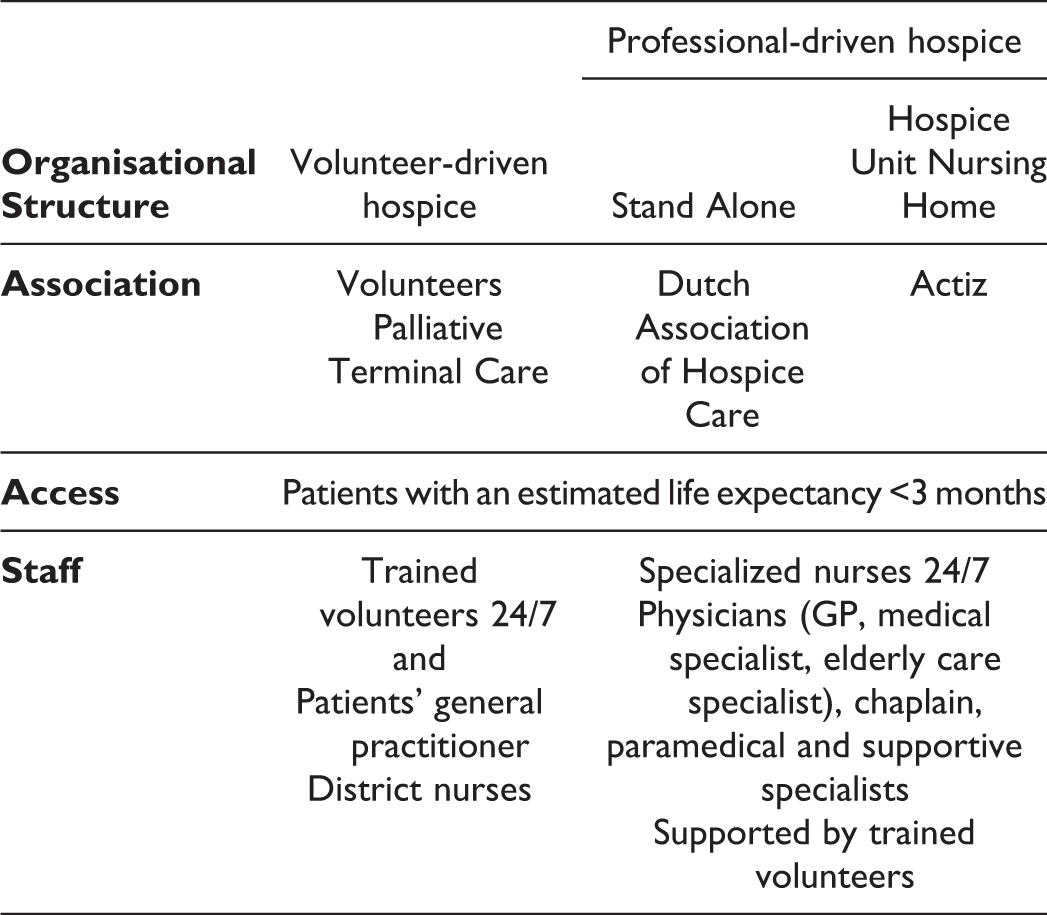
Palliative and hospice care in the Dutch healthcare system 6 .
Hospice care (HC) is multidimensional care, aiming to diminish physical, psychological, social, and spiritual suffering. 6 The organization of care differs among VDHs, HUs, and SAs. Therefore, insight into patient and care characteristics is needed. 7 Although no differences were found in age, gender, and main diagnoses between the types of hospices, 8 a complete image of which patients are admitted and which care is provided is missing. To examine similarities and differences between the types of hospices, a national retrospective multicenter study will be performed, examining hospice patient records (HPRs). This study is part of the HOPEVOL study and will examine patient and care characteristics of 240 HPRs per type of hospice. 7
Hospice care is a complex intervention entailing multiple components and is performed by a multidisciplinary team. 9 The Medical Research Council (MRC) developed a framework to support the development of complex interventions. 10 Although piloting in the MRC framework is mostly related to the evaluation of an intervention, the performance of a pilot study in preparation of a national retrospective multicenter study in a complex field, which has rarely been studied, could contribute to a successful study. 10 Moreover, a broad variety in HPR is expected, due to different disciplines, each of which maintain their own HPR, available at their own workplace. Therefore, knowledge of the availability of HPRs, possible barriers, and necessary actions to obtain HPR are crucial in preparation for the multicenter study. This pilot study aims to inform and adapt study procedures and outcomes to fit the variance in current hospice practices and to ensure study success for the national multicenter study. 11
Methods
Design
An exploratory, retrospective, descriptive, cross-sectional pilot study was performed from December 2017 to June 2018 using a quantitative approach.11,12
Setting and Population
Convenience sampling was used to select hospices among all 3 types of hospices, namely, VDHs, HUs, and SAs. The population consisted of patients who received HC and died in 2017.
Ethical Considerations
The research protocol (reference-number WAG/mb/18/004837) was assessed as not subject to the Medical Research Involving Human Subjects Act by the Medical Research Ethics Committee in Utrecht. File research applies to the legislation of the Agreement on Medical Treatment Act and General Data Protection Regulation. 13 According to these laws, no informed consent is required if patients are deceased. 14 In line with the principles of Good Clinical Practice, local consent from hospices was obtained. Full anonymization was not possible due to reaccessing records in the final study. 7 Therefore, data were collected and stored in a closed online database and key data were stored on a different server.
Outcomes and Measurements
Primary outcomes were defined as the appropriateness of study procedures and the availability of HPRs and of patient and care characteristics. The secondary outcomes were descriptions of patient and care characteristics.
Availability of HPR
First, the availability of HPR was determined (dichotomous), including the time it took to recover the HPR. Second, if HPRs were not available, barriers and necessary actions were collected. Finally, if HPRs were available after actions were deployed, HPR availability was denoted.
Availability of patient and care characteristics
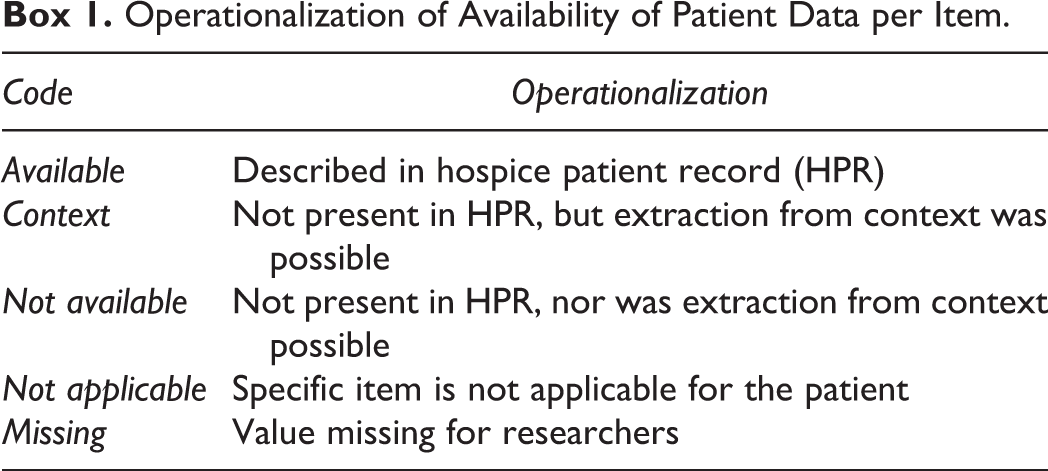
The availability of characteristics was defined as the description of specific items in HPRs, categorized as in Box 1. Patient characteristics were operationalized into demographics, illness characteristics, and experienced symptoms. Care characteristics were defined as the indications for deployment of (non-)pharmacological interventions and assessment tools used.
Operationalization of Availability of Patient Data per Item.
Description of patient and care characteristics
Besides the availability of patient and care characteristics, a substantive description of these characteristics was provided. Therefore, experienced symptoms were assessed using the 4-dimensional Utrecht Symptom Diary (USD-4D). 15 The USD is a Dutch-adapted translation of the Edmonton Symptom Assessment System, enriched by 5 spiritual and social items. 16 Symptoms were defined as present when scored 1 or higher and clinically relevant when scored 3 or higher on USD-4D. Care characteristics were collected from the first 72 hours after admission.
Data extraction forms were specifically designed for this study. Availability of HPRs was measured using a case report form (CRF). Availability of characteristics and secondary outcomes were measured using an electronic CRF (eCRF) (Online Appendix 1). Before data collection, (e)CRFs were tested and adjusted. The first 5 cases were discussed within the team to reach consensus on assessment and notation of items. Thereafter, agreed rules of notation were described in a codebook and study procedures.
Procedures
Hospices were invited via the umbrella organizations. After agreement to participate, an appointment was made for data collection. To gain in-depth information, hospices selected 4 HPRs that they felt were a reflection of patients admitted to their hospices. In addition, 4 HPRs were selected at random on the day of data collection using Research Randomizer (version 4.0). 17 When HPRs were not stored in hospices itself, randomization was performed before the day of data collection. An anonymized overview of patients was sent by means of a secured file by email. After randomization, researchers contacted the concerned GP and home care organization(s). If they agreed to participate, agreements were made as to how HPRs were to be conveyed to the hospice. Data collection was performed at the hospice site by 2 researchers. A confidentiality statement was signed by the researchers per hospice.
Statistical Analysis
Quantitative data were analyzed using descriptive statistics. Data were checked on normality using histogram plots. Missing items were not imputed since missing data were part of the primary outcomes. Presented barriers for collecting HPR were analyzed through open, axial, and selective coding. Other qualitative data were categorized, quantified, and analyzed using descriptive statistics. Data were analyzed using SPSS Statistics (version 25).
Results
Of all 16 hospices approached, 13 participated in the study, consisting of 5 SAs, 6 HUs, and 2 VDHs. Additionally, 3 VDHs did not participate in the study, because home care organizations and/or GPs were not willing to participate. Median admissions in 2017 were 75 (interquartile range [IQR]: 27.8) patients per hospice. Hospices had an average capacity of 8 beds (standard deviation [SD]: 2.5). Twelve hospices (92%) used a digital HPR system.
Availability of HPRs
In total, 95% of the records from physicians, 98% of the records from nurses, and 62% of the records from volunteers were available for data collection. It took 21.7 days (SD: 14.9) on average to obtain HPRs. On average, the time to obtain HPR in VDH (
Barriers Presented During Data Collection.
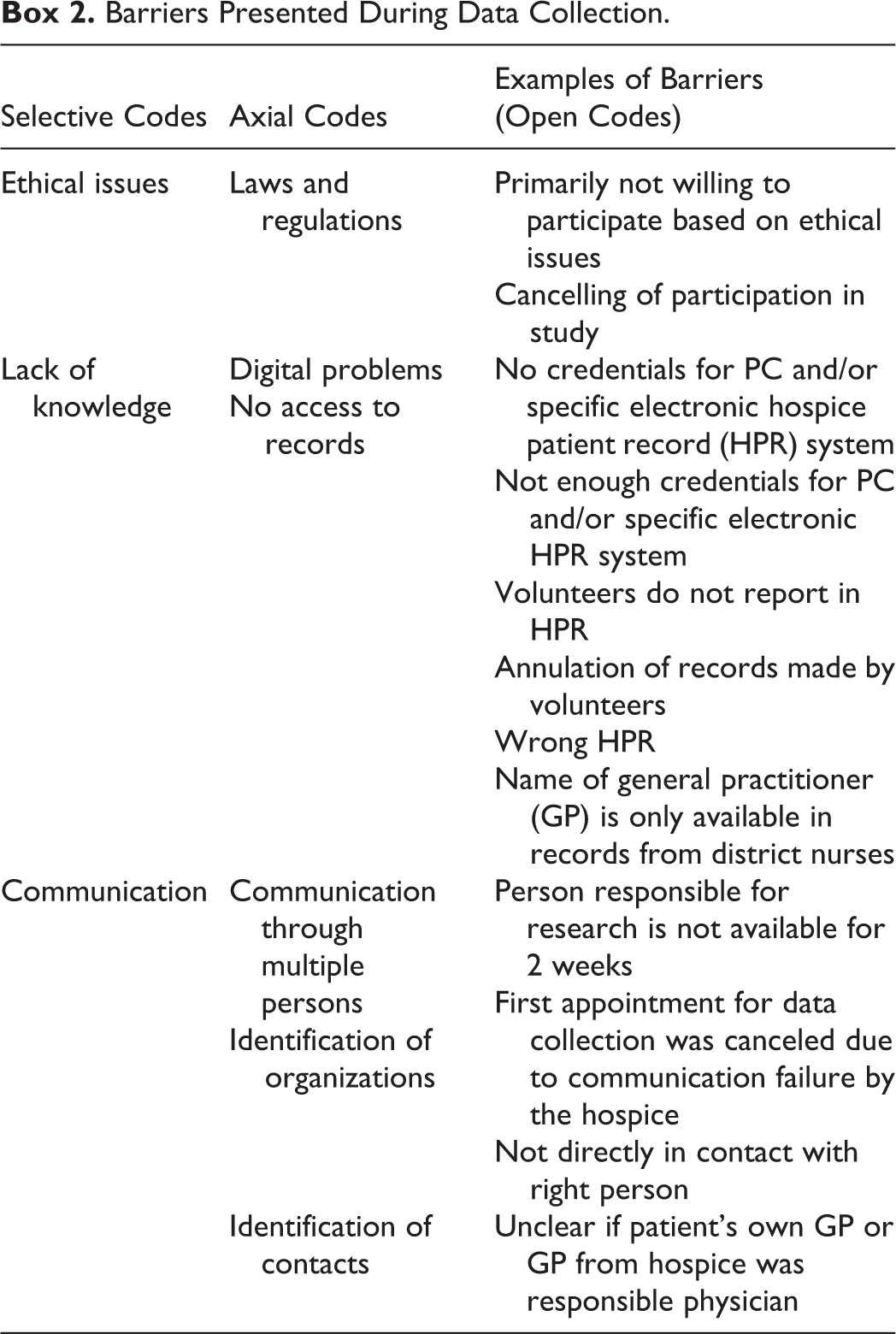
Actions necessary for gaining access to HPRs were (1) conversations with legal employees, (2) contact with technology departments for credentials, (3) contact with medical secretary departments, (4) telephone contact to provide more information about the study, and 5) signing a hospitality statement.
Availability of Patient Characteristics
Demographics
Age and gender were always described in HPRs. Marital status was described in 98 (94%) HPRs. Length of hospice stay was described in 100 (96%) HPRs, extracted from context in 3 HPRs and not available in 1 HPR, due to missing of the date of dismission. An overview of the available demographics is provided in Table 1.
Demographic Data of Hospices.
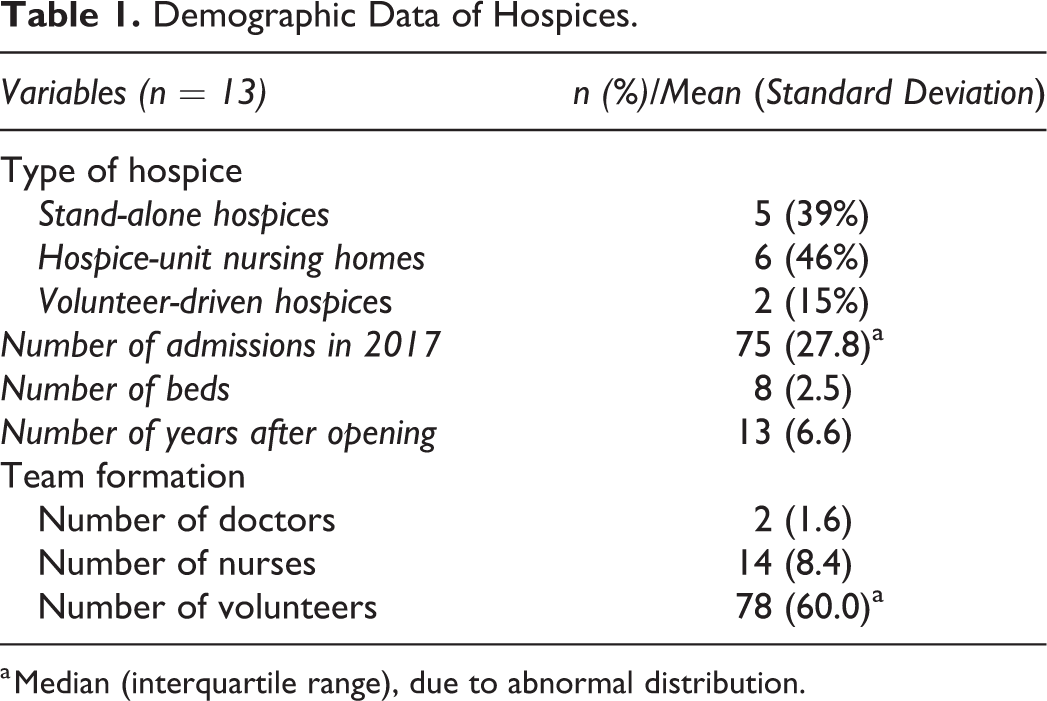
a Median (interquartile range), due to abnormal distribution.
Illness characteristics
In total, 14 of 24 variables of illness characteristics were available over 50% in HPRs. All variables are given in Table 2. Illness characteristics were mostly available (97%), with 100% availability of information about primary diagnosis. In contrast, variables regarding the physical, psychological, social, and spiritual status were available in 47% of HPRs. Patient worries were described only in 22% of HPRs. Information about the dying phase was available in 68% of HPRs, of which individual variables were high in availability, except for the preferred location of dying (53%) and changed preferred location (13%). The stage of the illness was mostly extracted from the context (48%). The availability of information describing problems during admission was 85%.
Availability of Patient and Illness Characteristics.a
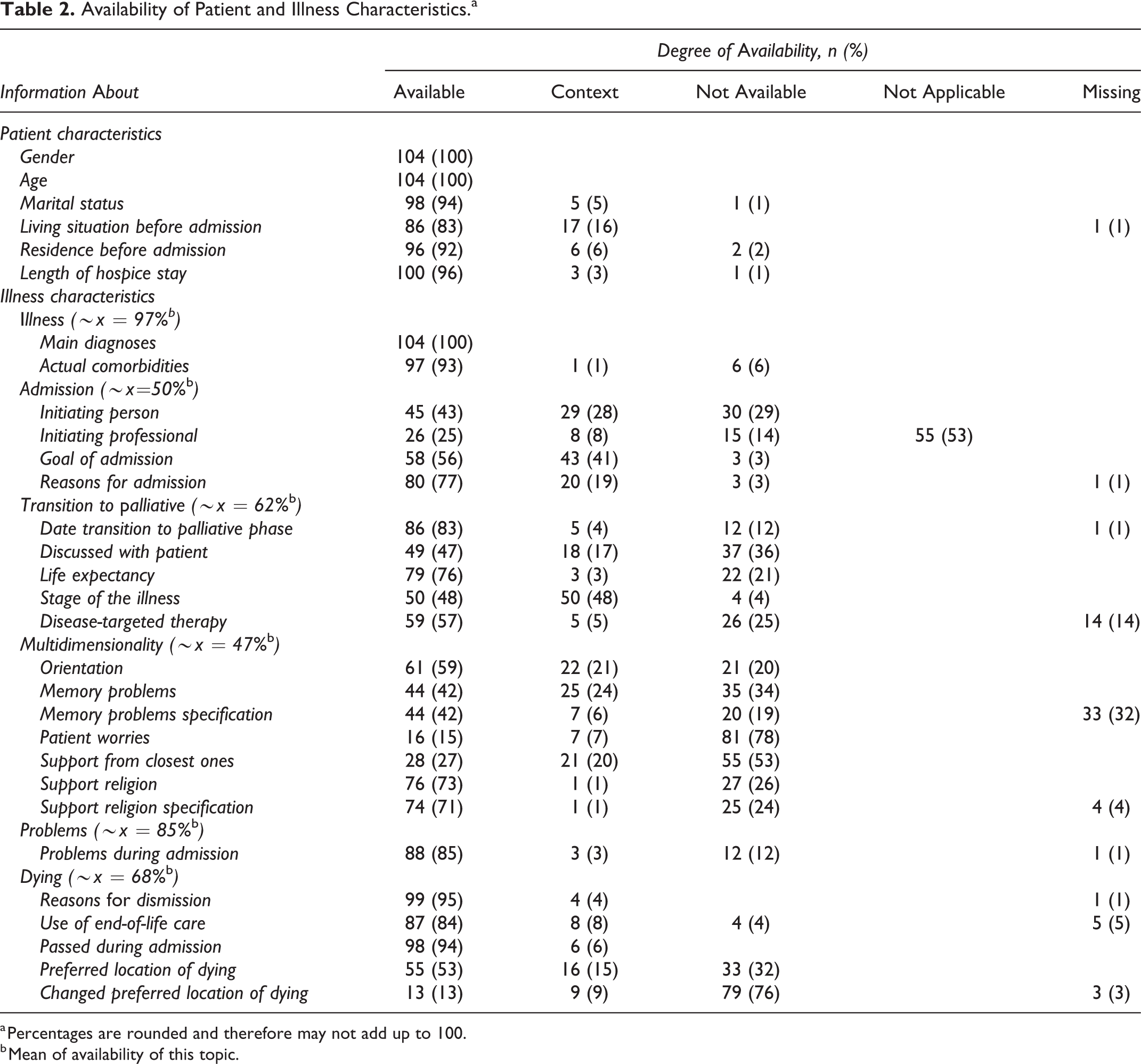
a Percentages are rounded and therefore may not add up to 100.
b Mean of availability of this topic.
Experienced symptoms
Information describing experienced symptoms in notes from volunteers and professional caregivers was available in 10 HPRs (10%).
Availability of Care Characteristics
Indications for deployment of (non-)pharmacological interventions
In 96% of HPRs, indications for deployment of (non-)pharmacological interventions were available. In 3 HPRs, interventions could be extracted from the context, and in 1 HPR, there were no indications for interventions.
Assessment tools used
In 44% of HPRs, assessment tools used were available, and in 53% of HPRs, they were not available. In 3 HPRs, information on assessment tools used was missing.
Description of patient characteristics
In total, HPRs of 104 patients were obtained, of which 58% were female. Patients’ mean age was 73 years (SD: 15.4). Although marital status of patients was predominantly married/registered partnership (41%), most patients lived alone (45%) before admission. Before admission, patients stayed mostly in hospitals (51%) or at home (37%). In 51% of the situations, patients themselves and/or their family took the initiative for hospice admission. The aim of admission was predominantly last resort (96%). Once admitted, patients stayed for a median of 20 days (IQR: 47.5).
The primary diagnosis for 80% of patients was cancer. Upon admission, 8 patients were in the dying phase and 86% received symptom-targeted palliation. The most prevalent symptoms were anorexia (20%), dry mouth (18%), and constipation (14%). Furthermore, delirium (29%), pressure ulcers (23%), and edema (21%) were most frequently described care problems. Within the social dimension, 42% of the patients felt supported by their family. Spiritually, 37% experienced support from their religion. In total, 50% of patients were sedated and 5 patients died by means of euthanasia. All patient and illness characteristics are described in Online Appendix 2.
Description of Care characteristics
During the first 72 hours after admission, 630 interventions were described in HPRs, of which 297 were pharmacological and 333 were nonpharmacological, which represents 6 interventions per patient on average. Interventions were mostly deployed in the physical dimension (n = 408, 65%) and least in the spiritual dimension (n = 8, 1.3%). Of the 630 interventions, most focused on pain (14%), primary and secondary prevention of pressure ulcers (9%), and dyspnea (5%).
A total of 11 different assessment tools were used in 44 patients’ daily care. The Karnofsky Performance Score (n = 20, 45%) and USD (n = 10, 22%) were used most frequently.
Discussion
The aim was to pilot test whether study procedures and outcomes are appropriate to be used in a national retrospective multicenter study on HC and hospice patients. Therefore, an insight into the availability of HPRs was examined. Hospice patient records by nurses were most available and by volunteers least available. Three main categories of barriers were ethical issues, lack of knowledge, and lack of communication. Demographics were mostly available in HPRs or could be extracted from the context. In total, 14 of 24 variables of illness characteristics were available in over 50% of the HPRs. In contrast, information describing symptoms experienced was available in 10 HPRs (10%). Deployment of (non-)pharmacological interventions was described in 96% of HPRs, and assessment tools used were available in 44% of HPRs. Utilization of the USD-4D could contribute to score and monitor the most prevalent symptoms. Unfortunately, the use of the USD-4D is not a part of the standard care in all hospices, and, if so, not all USD-4D were available within the first 72 hours after admission.
Strength and Limitations
The strength of this study is the performance in a realistic setting, which gives a glimpse of the current practice in hospices. In addition, multiple cases were discussed within the research group, consensus was reached, and rules of notation were described in a codebook. Furthermore, a full scope of all possible classifications was obtained, due to open variables, which were categorized and quantified.
However, some considerations must be made. First, items were selected through previous research and based on a specific electronic patient system. 6 Some specific items were not available in other kinds of electronic patient systems. Second, only data from the first 72 hours after admission were collected, due to feasibility of the study. Underdocumentation of specific characteristics is expected, for example, patient worries and support from closest ones. Third, using the USD-4D as a monitoring instrument of patient-reported outcome measure for symptoms experienced resulted in a low availability. And lastly, generalizability is limited due to the small numbers of VDH in the sample.
Hospice Patient Records
In total, 104 HPRs instead of the planned 120 HPRs were collected. Hospice patient records made by volunteers were least available, possibly due to the following: (1) volunteers did not write reports, (2) reports were annulled, or (3) reports were given to the bereaved family. Furthermore, aforementioned overarching barriers influence one another, which results in not having access to HPRs. For example, a lack of knowledge on research and the new law of general data protection regulation 18 combined with communication through multiple persons caused that some home care organizations and GPs were holding back or refusing participation. At times, approaching hospices from a higher level of influence was needed, for example, by a network of coordinators or members of the umbrella organizations.
Despite this, in our study, 92% of the hospices worked with an electronic HPR system; most hospices work with multiple systems for documentation by physicians and nurses. Therefore, in VDH per patient, documentation was obtained from multiple sources. Records from GPs had to be obtained at the general practice or were sent to the hospice. The same applies for records from home care organizations. In conclusion, no HPR is the same and collection of HPR took more time than anticipated.
Patient Characteristics
For clinical practice, it is striking that hospices strive for multidimensional care, while availability of multidimensional characteristics is minimal, specifically with regard to the social and spiritual dimension. This corresponds to previous studies that show that psychological, social, and spiritual dimensions are underdocumented. 6 Most striking is the low availability of symptoms experienced. It remains unclear whether patients did not express their symptoms, were not invited to express them, or did not experience symptoms. A possible reason for underdocumentation might be that nurses only describe these items when problems with regard to this matter occur. 6,19 Since previous studies showed that patients experienced 7 symptoms concurrently, at least a few of these symptoms would be expected within this hospice patient population. 6 Furthermore, information about transition to the palliative phase was available for less than half of the patients (47%), possibly because these conversations took place before hospice admission. However, for the continuity of care, this information is vital for optimizing care and guidance of hospice patients and their families.
Care Characteristics
Interventions were mostly deployed in the physical dimension and least so in the spiritual dimension. This corresponds to previous research that physicians are trained to address physical problems primarily. 6 Besides, other interventions were not documented because nurses interpreted these interventions as standard care. 6,19
Assessment tools were available in less than half the HPRs. Previous research showed that 10 of 12 professional-driven hospices used assessment tools. 6 Although this study involves the 3 types of hospices, there is still an underrepresentation of VDH in the sample.
Piloting
To the best of our knowledge, no previous research has been performed on the availability of HPRs and patient/care characteristics in HC. Even though piloting is not common for this kind of research, the MOREcare statement urges the application of the MRC framework in end-of-life care studies. 20 Developing HC as a complex intervention, piloting has a crucial function in testing the feasibility of methods, procedures, protocols, and outcomes. 11,19,21 This study showed that it takes effort and time to obtain HPRs from hospices, home care organizations, and GPs.
Recommendations
For the subsequent study in the overarching national hospice study, it is recommended that extra attention be paid to communication with hospices by providing extra information on concerns on ethical issues preventing communication through other persons. Changes have been made in the provision of information not just to hospices but also to GPs and home care organizations. Furthermore, calling hospices a day before data collection could ensure that everything is arranged properly and prevents new barriers. This study required a longer time span for obtaining HPRs from VDHs. Therefore, planning should be adjusted for the final study. To overcome this, there are 3 different scenarios in place for contacting hospices. First, all hospices are selected at random. Second, when numbers are not met after 2 months, a new sample will be selected at random. Third, when numbers are not met after 2 months, all hospices will be contacted, making it a convenience sample.
Within the secondary outcomes, there may have been a bias due to the fact that hospices could select half of the HPRs themselves. After inquiry, hospice staff said they selected complex HPRs, which is a possible cause of high sedation numbers. For the national multicenter study, all HPRs will be selected at random to prevent this from happening. Also, data collection is extended to not only the first 72 hours but also the second 72 hours and last 72 hours of hospice admittance.
Conclusion
Little research is performed in HC, which means that a research culture is lacking. This made it difficult and time consuming to obtain HPRs from different locations among different caregivers. Study procedures are operable for the final study, but data collection requires time, communication, and flexibility. Barriers presented during this study were ethical issues, lack of knowledge, and lack of communication. Patient and care characteristics were alternately present, which led to an extension of the period of data collection. Piloting was an important step to inform and adjust study procedures and outcomes to ensure study success of the national multicenter study.
Supplemental Material
Supplemental_Material - Who Are Hospice Patients and What Care Is Provided in Hospices? A Pilot Study
Supplemental_Material for Who Are Hospice Patients and What Care Is Provided in Hospices? A Pilot Study by Remco M. Koorn, Merel van Klinken, Everlien de Graaf, Rick E. G. W. Bressers, Adri P. Jobse, Frederieke van der Baan and Saskia C.C.M. Teunissen in American Journal of Hospice and Palliative Medicine®
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.