
Abstract
Background:
As the demographics of caregiving in United States evolve toward multigenerational, distributed family structures, the ways in which individuals and their families experience serious illness are changing. As part of a project to create an innovative model of supportive care for serious illness, a series of user interviews were conducted, forming the basis for this article.
Objective:
To understand the experience of caregiving for individuals with serious illness from an intergenerational family perspective.
Methods:
Twelve semistructured group interviews were conducted with patients, families, and professionals. Transcript data were analyzed with descriptive coding, looking for major themes and subthemes related to family experiences.
Results:
Seventy-three individuals participated in group interview sessions. While both families and individuals encountered caregiving challenges, the family unit experienced care in several unique ways. It accommodated differences in temperament and readiness, managed internal conflict, and strived to emerge as a cohesive unit. Individual struggles were often magnified or, more often, ameliorated by family context. Caregiving itself formed a legacy for future generations. Finally, care was seen as bidirectional, being tendered both by the family caregivers and in turn by the patient.
Conclusions:
When talking about care for serious illness, individuals report both rewards and challenges, often in a family context. The family enterprise manages a loved one’s care, negotiates the health-care system, and adjusts its own internal dynamics. Integrating the family narrative provides a more balanced view of the family system that provides the day-to-day care for individuals with serious illness.
Introduction
Informal, unpaid care for individuals with serious, chronic illness represents an American enterprise that parallels Medicare and Medicaid in its population reach and cost, when valued in terms of the hours of work provided. 1,2 Within the world of caregiving, families are a substantial supplier of care to the seriously ill. The scenario of a single caregiver living alone and caring for their spouse represents a minority of care situations. While 1 in 10 care for a spouse, the average age of a caregiver for an adult is 49, and about half of all caregivers are attending to a parent or parent in law. Forty percent of adults receive their care in a home other than their own, reflecting a trend among older Americans to reside with or in proximity to nonspouse family. 3,4 As America ages over the next 3 decades toward a demographic profile more like current Europe, we see older Americans providing more support to both their adult children and their aging parents. 5
Despite new initiatives, the United States is less supportive of family caregivers than other developed countries. Only 11% of US companies allow paid time off for family caregiving. Support is piecemeal rather than integral to the fabric of health care. 6 Without clear economic drivers, policy follows American cultural norms of self-reliance that hold families responsible for care, a view generally shared by the majority of citizens. 5,7 Revisiting the importance of the family’s role is appropriate at a time when the Affordable Care Act offers opportunities to innovate, for example, through the Money Follows the Person Rebalancing initiative. Lack of readiness on the part of caregivers to provide services—frequently cited as a contributor to caregiver burden—could be one such target for innovation. 8 –11
Finally, revisiting the family is appropriate in view of demographic forces. An aging population, low birth rate, women working full-time, nontraditional family configurations, and multigenerational, noncolocated families lead to profoundly different scenarios of caregiving compared to the increasingly mythical nuclear American family. 12
The current study examines family-related experiences reported by caregivers in the course of serious illness. The interviews were part of a human-centered design approach to creating a supportive care model for serious chronic illness. 13 –15 The group interview sessions were designed to explore experiences of caregiving for patients and families; for that reason they were relatively open-ended. A previous paper dealt with caregiver experiences in this data set, including rewards and challenges. 16 This paper will illuminate the family contexts that shape critical experiences in the course of caring for serious illness.
Methods
Participants and Procedures
Twelve semistructured group interviews were conducted with groups of 2 to 8 participants between March 3 and June 30, 2012. Participants with personal experience dealing with chronic medical conditions as patients, caregivers, or both were recruited by a local public television station to participate in recorded sessions intended for documentary use. They came from a wide variety of settings, including senior living communities, churches, provider organizations, and disease advocacy associations. The participants are characterized in Table 1. They included 23 patients, 29 family, and 19 professionals. Caregivers were all spouses or adult children of the patients. Two physicians, 1 social worker, and 1 chaplain had palliative training. The remainder included physicians and advance practice nurses (5), nurses (2), chaplains (6), social workers (2), occupational therapist (1), and administrator (1). Patient diagnoses included dementia (28), cancer (16), chronic respiratory disease (11), heart failure (5), and other (3). Participants received no compensation.
Interview Participants.
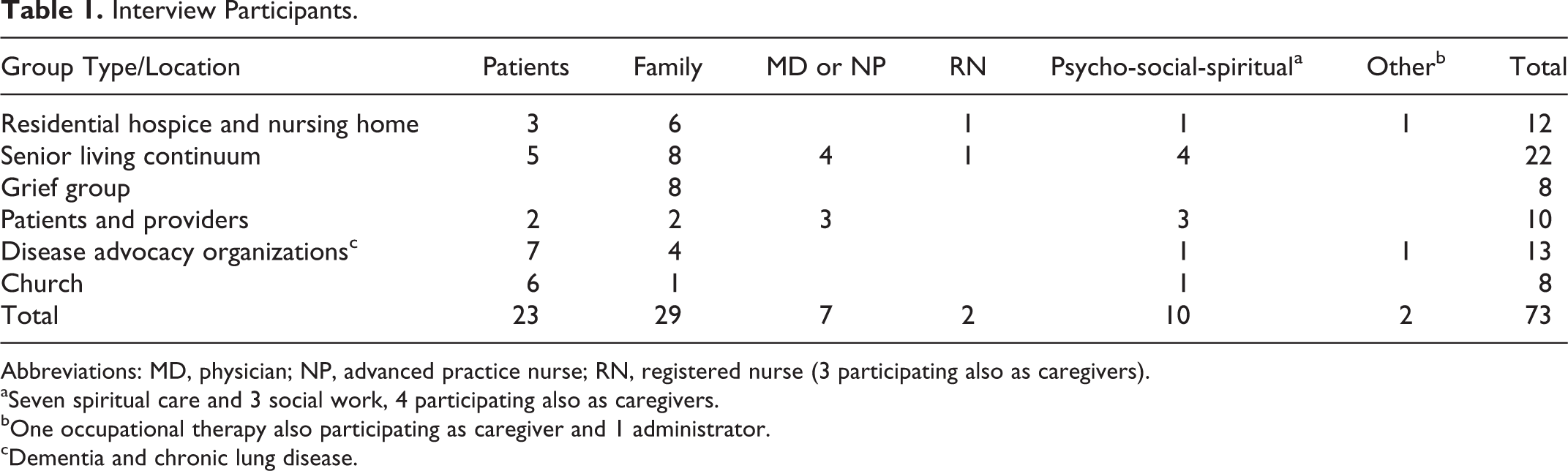
Abbreviations: MD, physician; NP, advanced practice nurse; RN, registered nurse (3 participating also as caregivers).
aSeven spiritual care and 3 social work, 4 participating also as caregivers.
bOne occupational therapy also participating as caregiver and 1 administrator.
cDementia and chronic lung disease.
Interview groups were facilitated by a family physician using a semistructured discussion guide and lasted between 90 and 120 minutes (Appendix A). A public television crew filmed the interviews. Dialogue from videos was transcribed for textual data. Participants signed media releases, and approval for the study and use of the transcripts was obtained from Quorum Review institutional review board.
Analysis
To establish trustworthiness, the analysis was triangulated. 17 Two researchers (E.W.A. and K.M.W.) conducted first-order coding on the data from all 12 semistructured group sessions. Initially, an inductive approach was used to generate the codebook. A final determination of codes was derived through an iterative, reflexive dialog to capture meaning related to family experience. Once completed, all transcript data were coded from a family perspective; comments about experiences of care that were not set in a family context were excluded. Professionals’ comments were coded only if the individual was speaking from family experience caring for serious illness.
Each researcher analyzed and subcoded 20% of coded transcript contents to generate the subcodes for second-pass analysis, repeating the reflexive dialog. Completion of second-pass coding was independently performed by assigning textual content to the major codes and subcodes. Coding was then reconciled between investigators. The data were numerically represented by enumerating the one-to-many relationships between quotes and domains. 18 NVivo (version 10) software was used to manage data analysis. 19 Deidentified transcripts and coding assignments are available from the authors.
Results
The 12 interviews yielded 511 quotes relating to experiences arising in the course of serious illness. These data yielded 1243 coded segments, representing an average of 2.43 coding assignments per quote. Several major themes emerged from examination of the coded passages. In response to interview questions, families commented on how they had adapted, individually or collectively, and how they employed new thinking or behavior to deal with challenges. Items relating to experience were identified and grouped broadly under 2 major themes: family learnings or adaptations and family systems. These major themes are described in more detail.
Family Learnings and Adaptations
The theme of learnings and adaptations included statements of understanding and personal change arising in response to experiences of caregiving. These insights influenced family functioning, and they helped to shape care going forward. Table 2 provides subthemes and quotes that illustrate the experiences shared within learnings and adaptations.
Family Learnings.
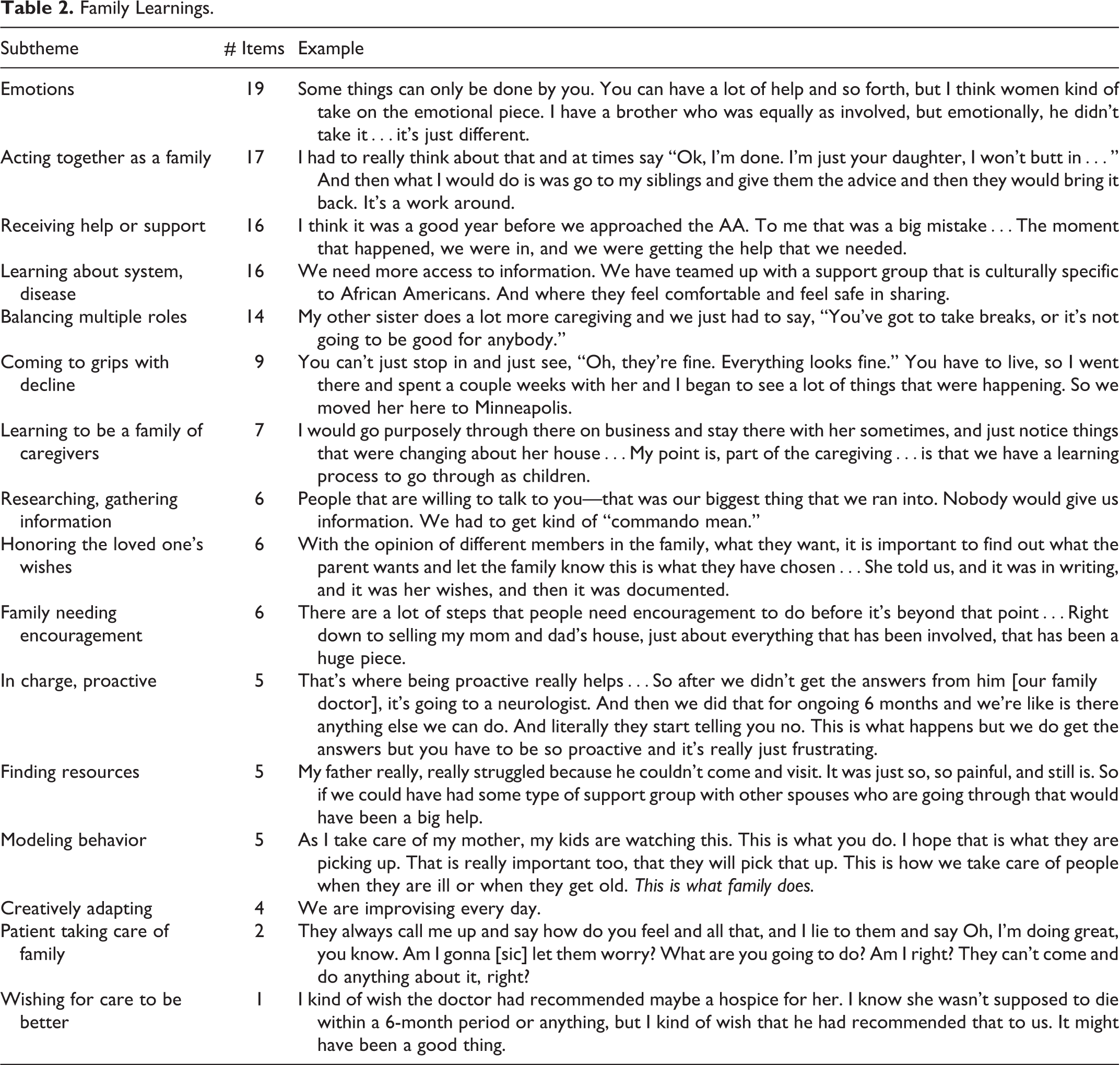
Reflections on emotions included witnessing cognitive decline, missing opportunities for closeness, feeling surprised when death finally comes, and recalling the loved one with deep sadness. Family members commented on different levels of emotional response, for example, “I think it was hard because my daughter and I were not at the same path that he was.” As with individual perspectives, supportive resources and faith were cited as positive emotional reflections.
Conflict arose in a number of settings. Gender issues within families were reported by women, who felt they shouldered the emotional work of serious illness. Families worked to avoid or manage conflict; this was often modeled by the patient being clear about their wishes: [Her choices] eliminated that kind of discussion, or what could arise—problems with the siblings: “Why not me, I’m the oldest boy?” or whatever. So that is a non-issue. It was her choice.
Reaching out to others for support was often task-specific, such as help with an advance directive. Families commented on lack of support from health systems but also acknowledged the help of advocacy organizations and support groups. One commented on the serendipitous nature of support: “Oftentimes it is not the people you expect. It’s one person in hospice care that maybe is the music therapist or it’s—you never know where it is going to come from.” Encouragement as a specific aspect of caregiver support was idealized as an ongoing process that offered practical advice. Whether from community organizations, the family doctor, or peers, participants asked for encouragement, “every step of the way.”
Disease progression and decline were experienced both as gradual processes of change and as abrupt changes in status. Families were challenged at both ends of this trajectory spectrum, from learning a diagnosis to end of life: “It’s not a very smooth cycle all the time. I’ve noticed that where [we] have hope that things are very normal again, and then all of a sudden it starts to degrade again.”
The majority of quotes depicted families coming together for the task, finding resources, and learning caregiving skills. Specific strategies included observing the parent at home, making care decisions on behalf of the loved one, and seeking organizational support. Gaining that support required researching information and exercising newfound assertiveness, including being “commando mean” at times.
Many of the self-described “sandwiched” caregivers learned from their experiences balancing competing demands of family and parents. While overwhelmed at times, they also described family as mediator or support in helping one another manage stress. One caregiver described both the personal learnings and the consequences of family support: Earlier this month I had the opportunity, I went to California for 5 days, to a retreat I had signed up for last July…And a brother stepped up and came from Portland Oregon to stay with my mother for those 5 days…I came back and it was a really hard reentry. And I think what happened, it was like the proverbial frog, in the pot of cold water…I left, I came back, and it was like jumping into the boiling water. I hadn’t realized what a toll it was taking and how much my life revolved around it.
The “Other” category was comprised of 19 varied quotes. They included: the world on our shoulders, having fun along the way, timing of when to move the parent, connecting to social community, having time to get to know the person, support from faith, the lifestyle and health of my ethnic community, or complementing professional staff.
Finally, several quotes addressed learnings about generations. Participants saw their loved one’s efforts to prepare for death and bereavement, taking it as an object lesson for themselves: “It would be words to the wise for all of us to do that for our children.” Others commented on caregiving in a 3-generation household. Finally, participants spoke of passing on a legacy of caregiving, eloquently stated as, “As I take care of my mother, my kids are watching this. This is what you do…This is what family does.”
Family Systems and the Caregiving Experience
Table 3 classifies quotes within the major theme of a dynamic family systems framework. Intended to guide clinical practice, this framework takes into account the ecology of families—the biopsychosocial, cultural, and spiritual influences acting on the family unit. Families are followed developmentally as they respond to emerging challenges, multiple stressors, and important nodal life events. 20
Family System Subthemes.
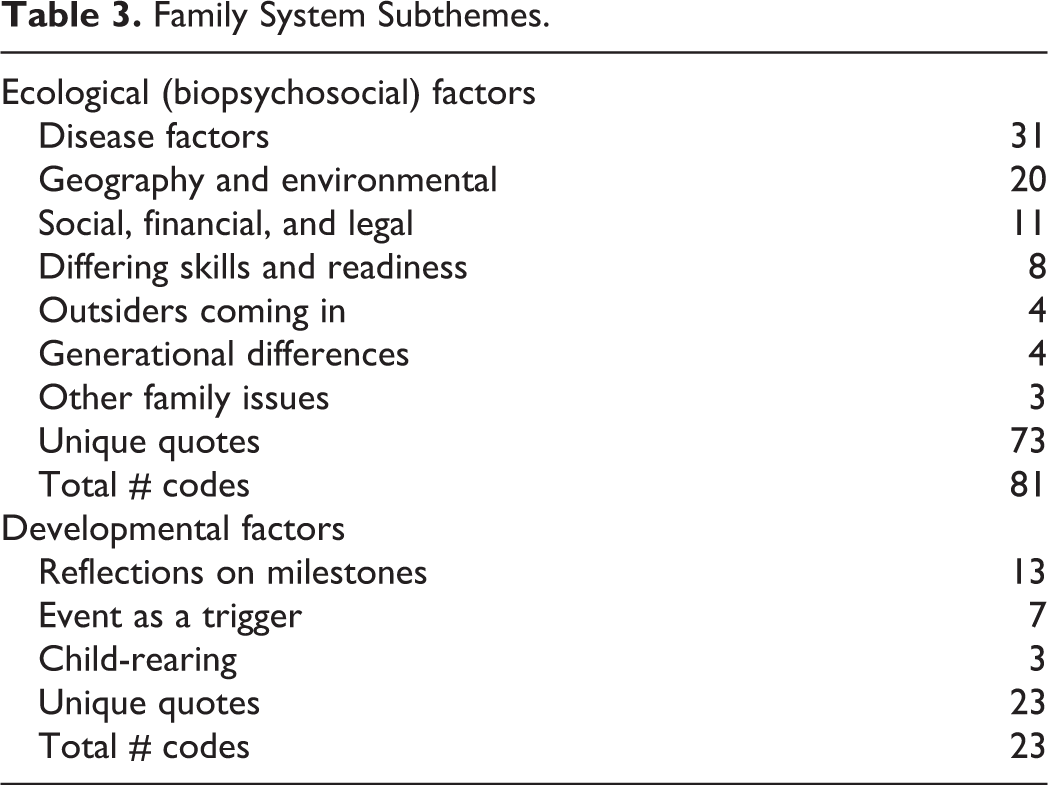
The broad subtheme of biopsychosocial factors includes the intrapersonal, physical, societal, and cultural forces acting upon the family that influence its ability to cohere and respond. The disease process itself was the most frequently cited factor in the family’s experience of care. Progressing illness produced varied emotional responses among family members, it often required action in crisis, it produced suffering the family could not diminish, and it truncated opportunities to understand the loved one’s wishes (Table 4).
Examples of Family Systems Subthemes.
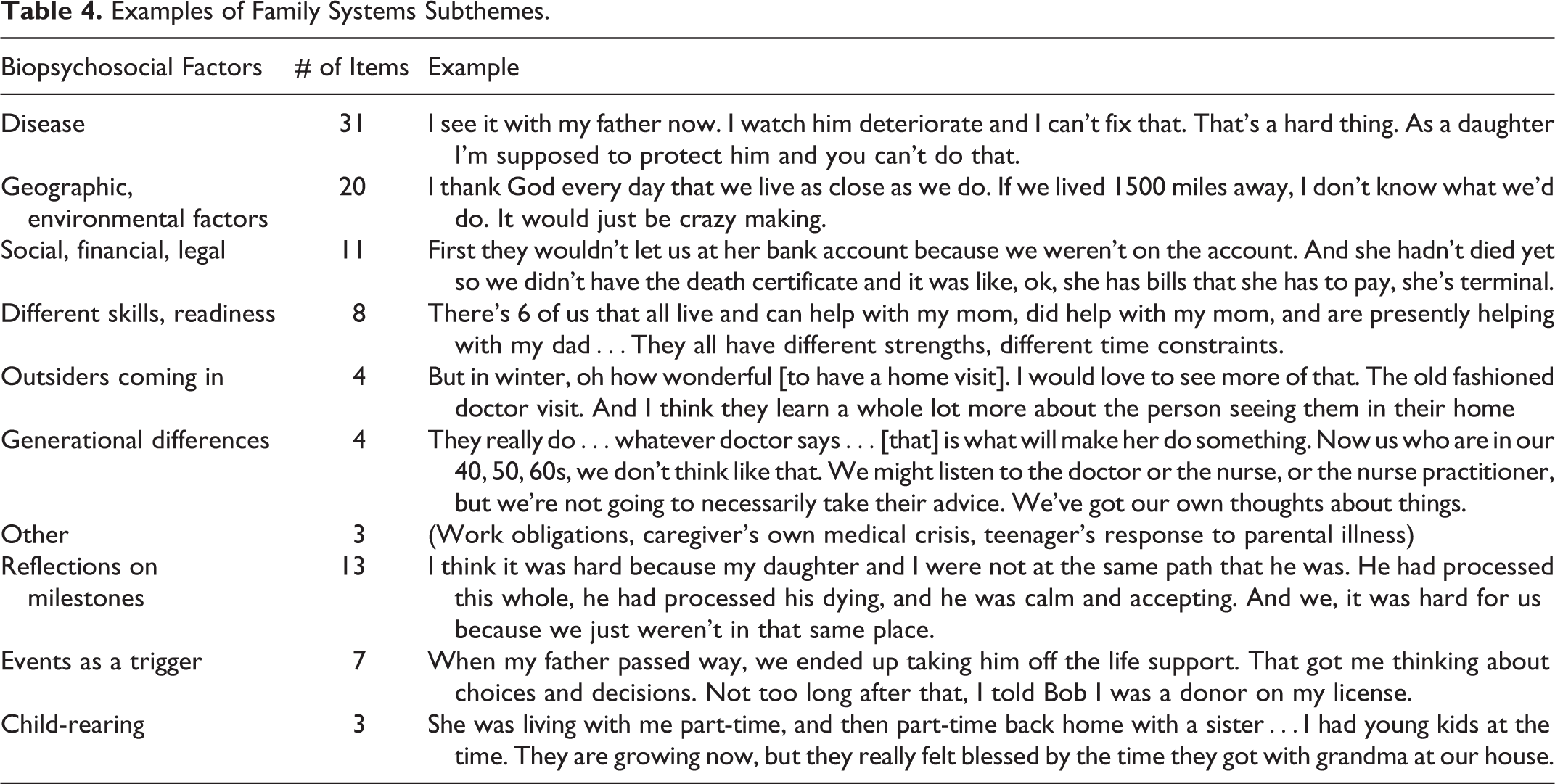
Geographic factors arose when moving the ill person, sharing caregiving among siblings, and hiring care locally. The third largest category included a combination of nonmedical factors—social/cultural, financial, and legal. Families remarked on their ability to manage assets, find nursing home placement, preserve the loved one’s independence, or overcome cultural barriers to seeking outside help.
Participants noted their family’s complement of skills and readiness. Most felt support from family, but engagement was unequal. In several comments, the participants described how they shepherded family members to a higher level of involvement.
A smaller number of quotes described effects of outsiders coming into the family setting or generational differences in family response. Outsiders could represent a potential threat to the loved one’s independence. They could also be a welcome presence, such as a physician home visit or friends helping a depressed spouse with caregiving. Caregivers consciously weighed generational differences in their approach to care, noting when their parents showed extreme deference to physicians, eschewed technology, or expected to die in their own home.
The second broad subtheme—developmental factors—included nodal events or processes such as death, marriage, and child-rearing. The dying process—a family milestone common to all the participants—led to reflections on self and family. The examples in Table 4 reflect the major subthemes of deep self-reflection, gratitude, and a sense of participating in shared, transformative experiences. Families described being changed as a result of living through these events, setting own house in order, recognizing past family grief resurfacing, and anticipating future events. Finally, child-rearing, while not a discrete milestone event, was often described in contrast to death occurring at the other end of the family age spectrum. Mixing generations in the home was a rich experience, while families struggled to explain terminal decline to their children.
Discussion
From a set of semistructured group interviews, over 500 responses were analyzed in an attempt to understand the caregiving experience of families. Despite inherent differences in caregiving skill and emotional temperament, family members forged a cohesive team that advocated for the loved one. They reported rewards and challenges, described learnings gained from their labors, and often depicted their family as a dynamic, adapting system under stress. Family values became manifest in the act of caring.
The insights about challenges and how families rise to meet them, as described in this study, are consistent with conclusions that serious illness affects caregivers, noncaregiving family, and the family system as a whole. 21,22 Adaptability, cooperation, and emotional engagement have been identified as family factors contributing to positive clinical outcomes in chronic illness. 23,24 Families in the present study encountered challenges in all these areas. They also commented on geographic separation, intergenerational households, working spouses, and adequate support for the hands-on caregivers, all of which stress family systems trying to adjust. 12,25 Others note that the growing cohort of baby boomers find themselves providing help to both their aging parents and adult children. 26 Pressure from noncaregiving family can further stress the active caregiver, particularly in dementia. 27 Family may reduce their involvement when an outside agency such as hospice is engaged, despite the need for ongoing emotional support. 28
Families bring a rich universe of meaning to caregiving that informs the family experience of illness. This shared family culture includes individual experiences and differences, the meaning of crises, the sense of mastery, and beliefs about the causes of suffering and the nature of healing. 22 If we think of families as mere adjuncts to the patient, it will perpetuate the tendency for health-care professionals to identify families as generally dysfunctional, to marginalize the family’s role in care, and to share a pervasive societal impression that the family is weakening despite evidence to the contrary. 12,29,30 In a study of bereaved hospice families who provided care at home, they valued personal and spiritual inquiry by the hospice team more than physical aspects of care, emphasizing the supportive power of understanding the family story. 31 An analysis of the Health and Retirement Study demonstrated that caregiver health was related to family factors—having a spouse or being a parent—and that caregiving itself was not a predictor of health in multivariate analysis. 32 Families in the present study spoke positively about their accomplishments. Positive psychological states aid in coping on the individual level. Rewarding emotions are posited as fundamental to the human ability to flourish, providing windows of opportunity to broaden responses and integrate adaptive behavior. 33 –35 It is probable that families respond in a similar fashion, evolving to new levels of competence. Relevant in this study were families who created a legacy of caregiving, a form of passing on values by role modeling. 36,37 Not surprisingly, others have called for a deeper appreciation of family involvement in caregiving. 21,38
Several themes from this study inform supportive strategies for serious illness. Families see themselves as the primary provider of care; they wished to be recognized as such. They are heartened in their task when there is a trusted, personal relationship with members of the health-care system. They ask for practical advice at each step. A recent review of family-centered interventions suggested that effective strategies include actionable information, practical support such as care transitions, emotional support to caregivers, and individualizing the care plan. 39 Demonstration projects using more comprehensive transition and family support demonstrate positive outcomes for quality of life and use of resources. 40,41 User focus groups have identified the need for a “medical advocate” to improve medication adherence, a concept more fully developed with the trained lay palliative care health worker in this study. 42
The authors acknowledge limitations to this study. It is a secondary analysis of data collected from group interviews intended to gain insights for developing a new clinical model; it was not a direct solicitation about family experiences per se. However, these data contained multiple references to family systems issues in which common themes appeared across the contrasting site group interviews. The analysis of these data relied on triangulation of data sources, including types of individuals, geographic sites, and multiple data collection sessions; on dual coding and analysis; and on dialog and reflexive practice in order to reduce threats to trustworthiness.
Conclusions
When asked about caregiving for a loved one with serious illness, individuals report both rewards and challenges, but they often do so in the context of an intense family enterprise. This choreography of care for serious illness is performed on the stage of an intergenerational family story—a story that comes to include the profound experience of caring for the dying. The meaning of care for a loved one is seen through many lenses, including that of an individual providing most of the physical care, that of a family team that sets about dividing up tasks, the lens of grandchildren living with the loved one in their home, and finally the perspective of the ill person themselves, sometimes actively participating to ease the burden of others. Understanding the experiences of affected family members is a necessary step to creating the adaptive adjustment and programmatic solutions that will better support caregiving family systems.
Footnotes
Appendix A
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by a grant from the Robina Foundation.