
Abstract
Self-care is increasingly recognized as a central aspect of mental health recovery, yet its meaning and enactment among individuals who engage in non-suicidal self-injury (NSSI) remain poorly understood. Existing conceptual models emphasize self-care as behavioral regulation, awareness, and autonomy but may overlook the emotional and relational complexities that shape this process in psychiatric contexts. This qualitative study explored how individuals receiving psychiatric care for NSSI conceptualize and understand self-care in their everyday lives. Twenty-six semi-structured interviews were conducted with twenty-five adults (ages 20–55) currently engaged in self-injurious behavior and receiving outpatient psychiatric treatment in Sweden. The material was analyzed using reflexive content analysis. Six interrelated categories were identified, reflecting self-care as a multidimensional and relational process: bodily and practical maintenance; emotion regulation; strategies driven by cognitive insight; self-directed emotional support and doing what feels good; engagement in work and daily activities; and relating to others. Participants described self-care as an ongoing effort to balance control and acceptance, effort and rest, and independence and connection. Although many articulated a clear understanding of what self-care involved, they often struggled to implement these practices consistently. Self-injury was at times described as a paradoxical form of care—an attempt to manage overwhelming emotions or regain control when other strategies felt unavailable. These findings extend existing frameworks by demonstrating how self-care, within the lived experience of NSSI, entails continual negotiation between vulnerability and agency, and self-criticism and self-compassion. Understanding self-care in this way can inform more compassionate, recovery-oriented, and person-centered approaches within mental health practice.
Self-care is increasingly recognized as a vital component of mental health, encompassing the practices individuals use to promote and maintain their own health, prevent disease, and cope with illness (World Health Organization [WHO], 2024). Despite its widespread use as a concept, self-care has been defined in diverse ways across disciplines.
In the chronic illness field, self-care has been conceptualized as a dynamic and goal-directed process comprising three components: self-care maintenance (engagement in health-promoting behaviors), self-care monitoring (awareness of one’s health status and its changes), and self-care management (taking action in response to symptoms) (Denyes et al., 2001; Riegel et al., 2012, 2019). This model highlights self-regulation and decision-making in everyday health management and has been instrumental in advancing research on self-care behaviors and outcomes, particularly in physical health contexts.
Building on and extending this behavioral foundation, Martínez et al. (2021) propose a broader psychologically oriented model that integrates both internal and external aspects of self-care. They define self-care as the ability to care for oneself through awareness, self-control, and self-reliance to achieve, maintain, or promote optimal health and well-being. Awareness refers to attunement to one’s needs and internal states—a capacity for self-observation that precedes and motivates action. Self-control involves the regulation of thoughts, emotions, and behaviors in ways that sustain health and prevent harm, while self-reliance denotes initiative and perseverance in taking responsibility for one’s own care. Collectively, these dimensions position self-care as a cognitive–emotional and motivational process, complementing the more behaviorally anchored model.
However, both frameworks have been developed primarily in somatic and general health contexts, leaving open questions about how self-care operates in psychiatric settings (Riegel et al., 2021). For individuals living with mental health difficulties, self-care often entails navigating fluctuating motivation, self-concept, and emotional distress—factors that complicate the linear progression of maintenance, monitoring, and management.
Recent participatory work further illustrates this gap. In a systematic review and co-development study, Truscott et al. (2024) found that academic definitions of self-care in young people’s mental health literature were largely inconsistent and primarily focused on general wellness or health promotion. However, when young people with lived experience were included, self-care was described as a process of self-awareness, self-compassion, and active strategies to achieve emotional balance. This experiential perspective builds on the internal dimensions emphasized by Martínez et al. (2021), while extending them toward a relational and emotionally grounded understanding of caring for oneself.
Together, these conceptualizations trace a movement from external regulation to internal experience, and from prescribed behavior to lived meaning. This trajectory highlights the need for empirical work that attends to how self-care is articulated and taken up in everyday life among individuals receiving psychiatric care for non-suicidal self-injury (NSSI), and to the range of practices and orientations that may be encompassed within this concept.
In psychiatric care, NSSI is frequently associated with significant psychological distress and broader patterns of impairment in emotional, social, and occupational functioning (Nilsson et al., 2021; Selby et al., 2012; Zanarini et al., 2010). NSSI is defined as the deliberate infliction of harm to one’s own body without suicidal intent (Nock, 2010) and is closely linked to emotion regulation difficulties and self-directed negative affect, such as shame, self-hatred, and feelings of worthlessness (Gratz, 2003; Klonsky, 2007). Among those who self-injure, experiences of internalized shame, harsh self-criticism, and a deep-seated sense of being undeserving of care are not uncommon (Gilbert et al., 2010; Nilsson et al., 2022; Xavier et al., 2016). For some, caring for oneself can evoke cognitive dissonance or emotional discomfort, particularly when it conflicts with entrenched beliefs of being unworthy or flawed (Bjärehed et al., 2025). These affective states may not only undermine the motivation or perceived legitimacy to care for oneself but may also directly conflict with the fundamental principles of self-care, which many self-care models implicitly assume: that individuals have some degree of self-preservation and self-value.
For these individuals, self-care may be experienced not as a right or a need but as something foreign, threatening, or even morally inappropriate. These dynamics have been discussed in therapeutic literature, where interventions such as compassion-focused therapy have been shown to help individuals with high levels of shame and self-criticism develop a more accepting and caring stance toward themselves (Gilbert & Procter, 2006). As such, the relationship between self-care and NSSI is likely to be both complex and fraught, potentially characterized by ambivalence, avoidance, or distorted interpretations of what it means to care for oneself.
These dynamics could be further compounded by stigma. Individuals who self-injure often internalize societal or psychiatric stigma, which can manifest as self-judgment, secrecy, and diminished self-worth (Meheli & Banerjee, 2022). These internalized stigmas may further erode the perceived right to engage in care for oneself, reinforcing patterns of neglect or self-punishment. Understanding how self-care is experienced in this population therefore has the potential not only to inform treatment approaches but also to challenge stigmatizing narratives and support recovery narratives.
To date, research on self-care has primarily focused on physical health conditions or broader aspects of mental health. Few studies have examined self-care as a subjective and lived experience among individuals with more severe psychiatric symptomatology, and even fewer have focused specifically on those who engage in self-injury (e.g., Bjärehed et al., 2025). This gap is striking given the growing emphasis on recovery-oriented and person-centered approaches in mental healthcare, which highlight the importance of agency, identity, and self-directed well-being (Davidson et al., 2021; Melillo et al., 2025).
The present study aims to describe and categorize the activities, routines, inner strategies, and ways of relating to oneself that individuals receiving psychiatric care for NSSI identify as self-care. Using a descriptive qualitative approach, the study seeks to systematically organize participants’ accounts of self-care in order to provide an empirically grounded characterization of the construct as it is articulated within this clinical group. Such knowledge is essential for expanding the theoretical scope of the concept and for informing more compassionate, recovery-oriented clinical practices that align with the individuals’ own frameworks of meaning and agency.
Method
Study Design
The study used a qualitative design—employing reflexive content analysis (RCA) as described by Nicmanis (2024)—to describe what individuals receiving psychiatric care for NSSI identify as self-care. RCA is a researcher-driven approach for systematically describing and condensing manifest content in qualitative data that involves systematically coding and organizing the data into a hierarchical structure of codes, subcategories, and categories, while remaining close to the manifest meaning of the data. It emphasizes reflexivity and transparency throughout the analytic process and is particularly suited for generating descriptive, surface-level insights into participants’ expressed experiences.
Participants and Procedures
Twenty-five individuals participated in the study: 21 identified as women, two as men, and two as non-binary. One of the participants was interviewed on two occasions. Hence, a total of 26 interviews were conducted. Ages ranged from 20 to 55 years. Inclusion criteria were (1) current engagement in self-injurious behavior, defined as having self-injured within the past six months, and (2) sufficient proficiency in spoken Swedish to participate in an interview.
Participants were recruited from an outpatient psychiatric clinic located in the southernmost region of Sweden. The clinic serves a geographically defined catchment area of approximately 200,000 inhabitants, including a larger urban center and surrounding towns and suburban areas. The clinic provides specialized outpatient care for individuals with self-injurious behavior, suicidality, and personality disorders. Thus, in addition to NSSI, most had co-occurring diagnoses. Self-reported conditions included personality disorders (primarily borderline personality disorder), mood (including bipolar) disorders, anxiety disorders, trauma-related disorders (including posttraumatic stress disorder), and neurodevelopmental disorders (e.g., autism spectrum disorder and attention-deficit/hyperactivity disorder). The sample reflected a broad range of clinical and demographic characteristics. Living situations varied from independent housing to supported accommodation and, in some cases, inpatient care. Participants also differed in employment status, with some working or studying and others on sick leave or engaged in structured daily activities provided by health or social services.
Throughout the manuscript, the term NSSI is used as an established clinical and research term. In the interviews, participants most commonly referred to their experiences using the term self-injury or related expressions. In some instances, participants also spoke more broadly about self-destructive behaviors; however, such descriptions primarily occurred in general reflections and typically included direct self-injurious acts.
When describing self-injurious behavior, participants in the vast majority of cases did not refer to suicidal actions. Such behaviors were instead described using distinct terminology. The use of NSSI in the present study reflects its close behavioral correspondence with what participants referred to when discussing self-injury, as well as its role as a shared clinical framework within the treatment context. The terminology used here therefore represents an attempt to balance participants’ language with conceptual clarity in relation to existing clinical and research conventions.
Potential participants were identified by their treating clinicians and received initial verbal information about the study. Those who expressed interest were contacted by the research team and provided detailed written information. Written informed consent was obtained before the interview, and a brief clinical assessment was conducted at the start of each interview to confirm recent self-injurious behavior.
Data Collection
Data were collected in two rounds of semi-structured interviews conducted in Swedish, either in person at the clinic or via secure video conferencing. The first round took place between January and March 2022, and the second between February and March 2023. Interviews were conducted individually by four trained research assistants as part of their master’s program in psychology, under supervision of the research team.
The research assistants were final-year master’s students in a professional psychology program prior to licensure as psychologists. At the time of data collection, they had completed their formal clinical training, including supervised clinical placements and direct patient work within the university’s training clinic. Within the research project, the interviewers received weekly supervision from one of the authors (J.B.), and one author (M.N.) was available in close temporal proximity to the interviews. Both J.B. and M.N. are licensed clinical psychologists with extensive experience working with the patient group, and M.N. also holds a senior clinical leadership role within the outpatient clinic.
Given the sensitive nature of the topic and the clinical vulnerability of the participant group, several measures were in place to safeguard participants during the interview process. All participants were receiving ongoing psychiatric treatment at the clinic, and the study was known within the clinical service. Participants provided informed consent in accordance with established ethical guidelines and were reminded that they could pause or discontinue the interview at any time without consequence.
During the interviews, the research assistants monitored participants’ emotional responses and assessed any signs of distress or dysregulation. No instances of significant discomfort requiring interruption or additional support were noted. As interviews were conducted within or in close connection to the clinical service, participants had access to their treating clinicians if needed.
Due to the recruitment procedure, one participant was interviewed on two separate occasions, once in each round of data collection. Participants were informed about the study by their treating clinicians, and as some patients had contact with more than one clinician, this participant expressed interest in participation in connection with both recruitment waves. At the time of the second interview, neither the participant nor the interviewer appeared to be aware that the participant had previously taken part in the study, and the overlap was not identified until after the interview had been completed.
The research team discussed whether one or both interviews should be excluded from the analysis. As no substantive reasons for exclusion were identified, and in recognition of the participant’s contribution, both interviews were retained and coded as separate data sources.
The semi-structured interview guide was developed by the research team based on clinical experience and relevant literature, focusing on participants’ understanding and experiences of self-care as well as contextual background factors. The guide was revised slightly before the second round of interviews to refine the wording and allow for incorporating emerging insights from the first round.
Interviews lasted between 25 and 78 min, were audio-recorded, and were transcribed verbatim. Quotations presented in this article have been lightly edited for readability while preserving participants’ intended meaning.
Data Analysis
The analysis was conducted in Swedish using NVivo (version 15.2.1). Coding was guided by the research question, What activities are described as self-care? Initial descriptive, self-defining codes (e.g., “Making my bed”; “Formulating goals and a plan”; “Injuring myself to distract from intrusive memories”) were generated by one researcher (E.S.) based on participants’ explicit statements.
These codes were then collaboratively developed by the research team (E.S., J.B., and M.N.) into subcategories (e.g., Maintaining daily routines; Establishing goals or structure; Self-injury is self-care) and further organized into broader conceptual categories (e.g., Self-care through bodily and practical maintenance; Self-care through cognitive insight; Self-care through emotion regulation). Data segments were assigned more than one code if it captured multiple aspects of participants’ experiences. In such cases, the same excerpt was coded separately (e.g., as both a hygiene routine and an activity associated with enjoyment or relaxation), with each code then contributing to its respective subcategory. Thus, while individual data segments could be double-coded, each code itself was assigned to a single subcategory.
Following the iterative principles of RCA, the research team developed a total of 343 descriptive, self-defining codes capturing participants’ manifest descriptions of self-care. These codes were subsequently organized into 26 subcategories based on shared features and conceptual coherence. Through further iterative refinement and consolidation, the subcategories were grouped into six overarching categories that together structured the final analytic framework. During this process, a small number of codes (n = 6, derived from seven different interviews) did not cluster meaningfully with other codes and could not be interpreted in a conceptually coherent way in relation to the emerging categorization. These codes were therefore treated as analytic outliers and not included in the final categorization. Their exclusion was discussed within the research team as part of the reflexive analytic process.
Reflexivity was an integral part of the analytic process. All three authors are licensed clinical psychologists with extensive experience of providing treatment to individuals with NSSI and related psychiatric conditions, as well as of developing and evaluating clinical services tailored to this population. The research team represents different psychotherapeutic orientations, including psychodynamic and cognitive-behavioral traditions, which informed analytic discussions and contributed to a plurality of perspectives when organizing and interpreting the data.
Throughout the analysis, the authors engaged in ongoing reflexive discussions regarding how their clinical training and professional experiences might shape analytic attention and categorization. For example, discussions focused on how to understand the prominence of negative and self-critical self-concepts within this patient group, and how such features should be interpreted in relation to other clinical populations. Reflexive deliberations also addressed the distinction between participants’ explicit cognitive understanding of self-care and their reported difficulties in translating such understanding into everyday action, in order to avoid overemphasizing insight at the expense of lived practice. These discussions were used to critically examine analytic decisions and to remain close to the manifest content of the data, in line with the descriptive aims of the study.
The research team did not include members working from a lived experience perspective of NSSI, which may have influenced the analytic lens and is acknowledged as a potential limitation.
Ethical Considerations
The study was approved by the Swedish Ethical Review Authority (Dnr 2021-05054 and Dnr 2022-06058-02). Participation was voluntary, and participants were informed that they could withdraw from the study at any time without affecting their ongoing psychiatric treatment. All transcripts were anonymized during transcription, and all identifying information was removed to protect participants’ confidentiality.
Research on NSSI involves particular ethical and emotional considerations, given the high prevalence of trauma histories and the potential risk of distress during qualitative interviews. Recent methodological discussions have emphasized the importance of trauma-informed approaches in qualitative NSSI research, highlighting the need for participant safety, interviewer sensitivity, and appropriate support structures for both participants and researchers (Karmakar & Duggal, 2024).
In line with these considerations, the present study was conducted within an ongoing clinical context. Interviews were carried out by trained interviewers under close supervision, with attention to participants’ emotional state during the interview process and access to clinical support if needed.
Results
Self-Care Categories and Subcategories, With the Number of Interviews and Coded Segments in Which They Occurred
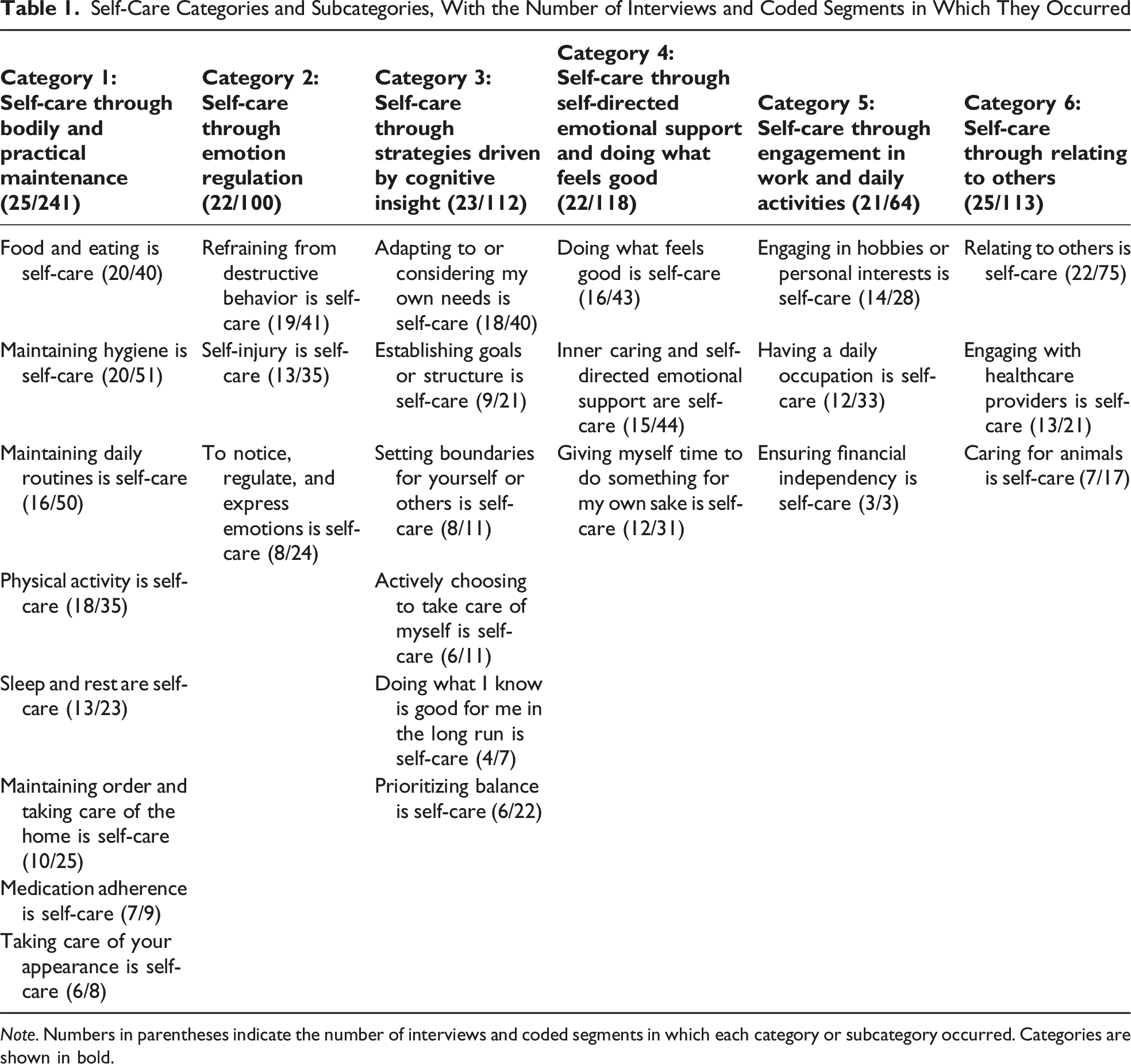
Note. Numbers in parentheses indicate the number of interviews and coded segments in which each category or subcategory occurred. Categories are shown in bold.
However, across interviews, a recurring pattern of ambivalence, uncertainty, and discrepancy between insight and action also emerged. Participants often demonstrated awareness of what self-care entailed, yet described difficulties in putting these insights into practice, as expressed by one participant: “So sleep, food and physical activity are important (…) to get better or feel good, and I do none of that” (P33). These tensions are not the primary focus of the present categorical presentation but form an important backdrop to how self-care was narrated and experienced. In the following sections, each category and its subcategories are described in detail.
Category 1: Self-Care Through Bodily and Practical Maintenance
In this first category, participants described self-care as maintaining physical health, basic functioning, and daily structure, including food, hygiene, sleep, medication, physical activity, and household tasks. While widely valued as contributing to participants’ well-being, the practices were often seen as difficult to sustain in everyday life. The category comprises eight subcategories, which capture different aspects that are described below.
Food and Eating Is Self-Care
Eating regularly and sufficiently was emphasized as self-care, though often described with ambivalence or difficulty. One participant expressed, “At a minimum, I try to eat twice a day” (P28).
Maintaining Hygiene Is Self-Care
Hygiene-related practices—such as showering, brushing teeth, skin care, and personal grooming—were described as forms of self-care. Hygiene was described as both a practical necessity and as serving a social function of avoiding negative comments or attention from others, as described by this participant: “If I’ve showered and taken care of things like that, I don’t feel ashamed to go outside, because I feel that no one will comment on me or think that I’m unclean” (P23).
Maintaining Daily Routines Is Self-Care
This subcategory captures how participants described self-care as efforts to establish and sustain everyday routines, such as getting up and dressing in the morning, making the bed, or following through with daily plans. Participants emphasized that such routines contributed to a sense of structure, stability, and control in daily life. As one participant noted: “I need routines for my well-being, so routines for me are about taking care of myself” (P8).
Physical Activity Is Self-Care
This subcategory centers on physical activity as a form of self-care. Engagement in regular exercise or just taking walks was part of participants’ self-care routines. One participant expressed, “(…) you go out and exercise, to do something that is good for the body physically” (P29).
Sleep and Rest Are Self-Care
Participants described sleep and rest as essential forms of self-care that help maintain emotional balance and prevent overload. Sleep was viewed as a physical necessity, while rest referred to intentional pause to sustain well-being. As one participant expressed: “I know that sleep greatly affects how much my mood changes. So (…) sleep is a way of taking care of myself and it’s a way of ensuring that it gets perhaps a little easier during the day” (P14).
Maintaining Order and Taking Care of Your Home Is Self-Care
Keeping the home environment clean, organized, and aesthetically pleasing was described as an important form of self-care. Everyday tasks—such as doing the dishes, laundry, or making the bed—were seen as ways to create stability. For some, a tidy space carried psychological significance: “(…) self-care is very much about having it neat and tidy, because otherwise there will be chaos in my brain” (P26). Others described efforts to make their home appear “perfect on the surface” to signal self-sufficiency, to themselves or others.
Medication Adherence Is Self-Care
Participants described how managing prescribed medication and seeking medical care were essential aspects of self-care. These behaviors were often framed as particularly important during periods of heightened psychological difficulty. For some, adherence to medication was described as foundational, something that enabled other forms of self-care to be possible. As one participant put it: “Taking my medicine is actually the biggest thing I should do. When I don’t, everything goes wrong and then I can’t take care of myself at all” (P1).
Taking Care of Your Appearance Is Self-Care
This subcategory captures participants’ descriptions of self-care as attending to their outward appearance (such as dyeing their hair, applying make-up, and dressing up). Feeling fresh or looking good was described as contributing to confidence and well-being, but also as a way to avoid shame or conceal signs of psychological distress.
Category 2: Self-Care Through Emotion Regulation
The second category captures how participants described activities related to emotion regulation or self-soothing as key aspects of self-care. A wide range of strategies were mentioned for managing affect and to reduce emotional distress. Some of these were adaptive, while others reflected ambivalence or short-term relief. Even behaviors typically seen as problematic—such as self-injury—were mentioned by about half of the respondents as a form of self-care, mostly referred to as an attempt to manage overwhelming emotions. The category consists of three subcategories.
Refraining From Destructive Behavior Is Self-Care
Participants described conscious efforts to resist engaging in harmful behaviors such as NSSI, misusing medication, or other self-destructive coping strategies. As one explained: “It’s about keeping myself away from things that are destructive and make me feel bad in the long run. (…) Taking care of myself is about keeping myself away from what harms me” (P30).
For some, self-care meant catching destructive impulses before acting on them or trying to move on afterward: “The optimal self-care is when I manage to catch it before [I act on it], and to let it go and move on if I have self-injured, without putting too much emphasis on it” (P32).
Respondents also described using therapeutic strategies or deliberate distractions to break destructive patterns. These practices highlighted self-care as a difficult balancing act, requiring boundary-setting, impulse control, and sustained emotional regulation.
Self-Injury Is Self-Care
Participants also described self-injury as a form of self-care. Although recognized as harmful, it was framed as a way of managing overwhelming emotions, grounding themselves, or regaining control, especially in the context of trauma. For some, it was experienced as a source of temporary energy or relief. One participant expressed it in the following way: “Yes, so sometimes it feels like I’m taking care of myself when I self-injure, I get energy from doing it so it can be effective” (P13). Others highlighted the paradox of tending to wounds afterward as a substitute for care: “I like the whole thing of taking care of it afterwards (…) it’s like I can keep myself from self-injuring thoughts very well when I have wounds that already need looking after” (P25). Accounts often reflected ambivalence, with some respondents openly acknowledging the tension: “Self-care for me is still abusing myself in some way. Because I feel better then. Strangely enough” (P30).
Although self-injury was explicitly mentioned in most of these segments, participants also referred to other destructive or self-regulatory behaviors, such as skipping meals, which could result in feelings of numbness or emotional detachment. Some described tending to existing wounds as a way of managing urges or replacing acts of self-injury, while others mentioned preparatory acts—such as storing medication or keeping razor blades available—as strategies for maintaining a sense of control.
To Notice, Regulate, and Express Emotions Is Self-Care
This subcategory captures self-care strategies that allowed participants to externalize or manage difficult emotions through verbal, written, or creative expression. Activities such as journaling, blogging, painting, or simply “venting” were described as ways to release emotional tension and clear the mind: “What I put my energy into is writing, on the blog. To get my thoughts and ideas out. It helps me. To clear my brain for a little while” (P6).
Expression was not limited to words but also involved symbolic or artistic practices that provided a safe outlet for inner experiences: “For me, it is a big thing to sit down and paint. And get the feelings out. It means a lot to me. (…) it’s my way of dealing with my emotions, getting emotions out in a non-destructive way” (P28).
Participants also emphasized the importance of allowing and being present with emotions. This could include deliberately changing environments—such as going to the gym or being out in public—not primarily for the activity itself but for the emotional shift it enabled. Such acts were described as ways to gain perspective, interrupt negative thought patterns, and explore alternative coping strategies.
Category 3: Self-Care Through Strategies Driven by Cognitive Insight
The third category includes acts of self-care that involve conscious reflection, internal decision-making, and structuring of one’s life or thought patterns. These strategies were often described as ways to take control, stay focused, or remain oriented during emotional turbulence. The category is composed of six subcategories.
Adapting to or Considering My Own Needs Is Self-Care
This subcategory reflects respondents’ efforts to tune in to their own capacities and adjust behavior accordingly. Rather than following rigid expectations, self-care was described as recognizing limits, allowing rest, or taking preventive steps such as contacting mental health services. One participant emphasized, “Taking care of yourself is perhaps also the realization that now I can’t take care of myself” (P3). Others framed this as listening to the body and responding with flexibility: “Today I’m really tired, then I take a day when I sit around and do something calm. Or today I’m energetic, well then I do things. That, I would say, is taking care of yourself” (P26).
Establishing Goals or Structure Is Self-Care
This subcategory captures participants’ descriptions of setting goals and milestones or creating structures as a self-care strategy. This included both long-term and daily intentions. Structuring the day, setting sub-goals, or simply approaching tasks one at a time was framed as ways to support continuity, reduce stress, and maintain focus during difficult periods. Some spoke of using tools such as whiteboards or written checklists to divide things into small, achievable steps. For some, achieving even a small goal served as a meaningful affirmation: “I write down a to-do list every day—small things like making the bed or making coffee. Just checking things off, no matter how small, makes me feel good” (P12).
Others emphasized the motivational power of having something to look forward to or the value of low-pressure goals to avoid overwhelming themselves: I try not to set a goal that I have to do every day (…) Because if I set that goal, I put too much pressure on myself. So instead I just set a goal that I will get out of bed every day. (…) And then I can give myself a lot of praise for that. (P28)
Setting Boundaries for Yourself or Others Is Self-Care
This subcategory reflects a cognitive and intentional stance in relation to one’s own needs, limits, and behavior. Respondents described how self-care sometimes required standing up for oneself or asserting needs in interpersonal contexts—for instance, by saying no to social invitations or voicing discomfort rather than acting impulsively. One participant expressed this: “I think taking care of yourself is also about standing up for yourself (…). I might have had a harder time with that when I was younger, I simply let others take advantage of me and things like that” (P7).
Setting boundaries was also directed inward: respondents emphasized the importance of respecting their own mind and body, taking personal responsibility, and actively choosing to interrupt unhelpful patterns, such as passivity or excessive screen time. As one participant expressed: “I take more responsibility for myself (…) like not drinking a lot of Coke Zero (..) before I go to bed because like, well, I have to be able to fall asleep” (P9).
Actively Choosing to Take Care of Myself Is Self-Care
Participants emphasized the mindset of making conscious internal decisions to take care of oneself. These choices were described as both practical and existential, such as deciding to engage in care-related behavior, voluntarily admitting oneself to inpatient care, or choosing to pursue a future. Reflections also included considering the consequences of one’s actions and recognizing that every choice has an impact: “I also try to be active in my choices and tell myself, ‘No, I can’t do it—but I’ll do it anyway’, because I know that otherwise there might be consequences for me” (P32).
One participant expressed that to be able to make the inner decision to take care of yourself, you must have a feeling of being worth caring for. The statements highlight the cognitive and volitional aspects of self-care—where respondents actively commit to behaviors that support their well-being, even when doing so may feel difficult or ambivalent.
Doing What I Know Is Good for Me in the Long Run Is Self-Care
This subcategory captures descriptions of a mindset that is also characterized by the aspect of choosing, but here it highlights that self-care is about engaging in activities that might feel difficult in the moment but are known to bring long-term or delayed positive effects. I'm thinking a lot about doing things that might be a little difficult [in the moment] but that are good for me in the long run. About ‘valued direction’ that we've talked a lot about in therapy (…) so then I try to apply that, like working out and continuing to study even though it's hard. Or going to therapy and stuff like that, which is hard but will be good for me in the long run. (P13)
This kind of reflective self-care was described as helping individuals stay aligned with their values and long-term well-being. Several participants described reminding themselves of the positive feelings that follow such efforts—relief, calm, or self-respect—as motivation to act despite resistance: Showering makes you feel good regardless of whether you're depressed or not, it's a nice feeling. Afterwards I feel clean and then I feel a little better about myself (…). I try to think about that when it's difficult to [motivate myself to] shower, that yes, but it's so nice afterwards. (P23)
Prioritizing Balance Is Self-Care
Participants emphasized maintaining psychological and practical balance as a central aspect of self-care, often described as a struggle between doing too much and too little—between action and avoidance, and effort and rest. As one participant reflected: “When it comes to my hobbies, where is the line between self-care and avoidance? If I sit with my coloring book for nine hours, maybe it’s not self-care but avoidance. Finding that balance is difficult” (P32).
Several participants described striving for a “functioning everyday life,” avoiding excessive demands, and managing energy to balance personal needs with responsibilities to others. Reflections on balance were not confined to a single domain but recurred across accounts of emotional regulation, daily routines, self-compassion, and in relationships—indicating that the pursuit of equilibrium was a pervasive concern in participants’ understandings of self-care. As one participant put it: I have a hard time with balance in my relationship with my family. Because I want to meet them and I kind of love them, but I also get more memories and annoying reminders of things that have happened when I hang out with them. It comes with the fact that they are not always very nice. So it’s hard to know where the balance lies—whether it is self-care to meet them or self-care not to. (P13)
Category 4: Self-Care Through Self-Directed Emotional Support and Doing What Feels Good
This fourth category captures how self-care was described as an internal relational stance—learning to treat oneself with kindness, patience, and acceptance. For the participants, it also seemed linked to allowing themselves to engage in things that made them feel good. The category is composed of three subcategories.
Doing What Feels Good Is Self-Care
This subcategory captures participants’ descriptions of how they actively sought out activities, environments, or routines that promoted a sense of well-being and joy. This included both small everyday pleasures, such as watching a favorite show or listening to music, and more structured efforts such as planning fun weekly activities: I have things planned for the week that I think are fun. And then I do regular body care and stuff like that because I think it's quite nice and cozy to do. (…) I choose to put my energy into things that make me happy, instead of focusing on something negative. That's the basis of self-care, I guess, focusing your energy on what makes you feel good. (P25)
What is salient in this subcategory are the descriptions of these actions as meaningful practices in their own right. One participant reflected as follows: [Self-care is] taking care of yourself and your mind, I used to think (...) self-care is brushing your teeth, washing yourself or exercising. But self-care for me is that I draw something. It's not that it's going to improve my body in any way. It's just something that makes me feel good and creative. (P29)
Inner Caring and Self-Directed Emotional Support Are Self-Care
This subcategory encompasses respondents’ internal efforts to emotionally support and care for themselves. These included consciously practicing self-acceptance, self-validation, and speaking kindly to oneself, which was described as thus: “[Self-care is] to be kind to myself and I practice validating myself verbally as well (…). I try not to blame myself if I’ve injured myself (…)” (P32).
Participants also described working to break negative thought patterns, forgive themselves, and develop a sense of being worthy of care. Some used therapeutic techniques to support this process, one mentioned employing imaginative strategies—such as personifying parts of the body or the home—to make care feel more attainable. By imagining the recipient of care as someone else, the participant could engage in nurturing acts that might otherwise feel uncomfortable or undeserved when directed toward themselves. Writing down positive thoughts or reminders of progress also served as emotional anchors in times of distress, reflecting an ongoing effort to cultivate a more caring stance toward oneself.
Giving Myself Time to Do Something for My Own Sake Is Self-Care
This subcategory captures the notion that self-care means giving yourself time and space and highlights the important aspect that actions are meaningful simply because they are done for their own sake, whether it was preparing a favorite meal, enjoying a foot bath, or simply taking time to breathe. One respondent expressed this: “[Self-care] can be about respecting my own time. Like having morning coffee, watching the sunrise. I’d say that’s a way of taking care of myself, because I know it makes me feel calm” (P14).
The activities were not performed out of necessity or obligation but because they felt meaningful, comforting, or rewarding. Some respondents expressed the importance of making room for themselves, not just for tasks or others, as is articulated in the following quote: “Start being a little selfish and don’t just take care of others, I do things for my own sake. Not for someone else’s” (P28).
Category 5: Self-Care Through Engagement in Work and Daily Activities
This category captures participants’ descriptions of self-care as engagement in work, studies, or hobbies. While the specific reasons for emphasizing such activities varied, participants commonly described them as ways to add structure to daily life, create a sense of purpose, or provide a reason to get up in the morning. For others, the value lay in simply being occupied or finding enjoyment in meaningful activity. The category comprises three subcategories.
Engaging in Hobbies or Personal Interests Is Self-Care
In this subcategory, participants described how engaging in hobbies and personal interests was an important part of self-care. Some activities mentioned were dancing, painting, reading, gardening, and horseback riding. For some, the activity had a creative or expressive dimension. “Hiking, photography, painting, drawing, I’m very creative. So that’s been my biggest way of actually taking care of myself” (P28).
Having a Daily Occupation Is Self-Care
Participants described the importance of engaging in structured daily activities—such as going to school, studying, working, or participating in other meaningful vocations—to support their mental well-being. These activities provided structure to the day, created a sense of purpose, and contributed to feelings of autonomy and self-worth. For some, simply having a place to go or something to do (even on sick leave) was essential to avoid passivity or isolation. Others highlighted the emotional value of doing something that felt meaningful or enjoyable, as described in the following quote: I have great colleagues, interesting work tasks. It broadens your horizons all the time. So, it means a lot to me to be able to be there. You get confirmation and a feeling that you are needed. And that you are seen. And that you see others. (P20)
Ensuring Financial Independency Is Self-Care
Participants described self-care as tied to financial self-sufficiency and independence. Having an income or looking for a job to be able to take care of oneself financially was described as a way of maintaining independence and supporting oneself: “So taking care of yourself—for me—also means ensuring that you can be financially independent and self-sufficient” (P33).
Category 6: Self-Care Through Relating to Others
In the final category, self-care was described as enacted through connection with others. Participants emphasized relational behaviors—such as reaching out, accepting help, or caring for others—as central to their well-being and as meaningful expressions of self-care. Relationships, whether with people or animals, were experienced as sources of comfort, motivation, and grounding. The category comprises three subcategories.
Relating to Others Is Self-Care
Relationships played a central role in participants’ accounts of self-care. Seeking help, having the courage to reach out, and being surrounded by understanding others were often described as vital sources of support: “Seeing my mom is good, it’s also self-care for me. She’s the person who’s been there for me the most … she was in the hospital every day and she took sick leave from work and stayed with me” (P25). Being needed by others also gave purpose and reinforced self-worth. Small but meaningful connections—such as texting a friend or calling someone for company—were likewise seen as self-care: “I just broke up with my boyfriend (…) so I’ve mostly just tried to reach out to old friends. I see that as self-care” (P29).
Engaging With Healthcare Providers Is Self-Care
Self-care was also described as actively seeking and accepting support from the healthcare system. This included voluntary psychiatric admissions to prevent deterioration, attending appointments, reaching out for professional help, and allowing oneself to “take up space” in care settings: [Self-care for me is that] I come here to the psychiatric clinic and get help. Because it's very easy to underestimate [the severity of my symptoms], or to think that I’m not feeling bad enough, or that I’m wasting other people's time. I make an effort to let myself take my place and take time from my psychologist. (P13)
Engaging with healthcare was not only practical but also emotional—signifying recognizing one’s own worth and accepting help as a legitimate form of care.
Caring for Animals Is Self-Care
Spending time with and caring for pets and other animals—for example, spending time in a stable—was described as a meaningful form of self-care, offering calm, connection, and responsibility. The routines of tending to pets provided structure and purpose, while their presence offered comfort and distraction from inner distress. As one participant noted: “In order for me to be able to take care of my horse, I somehow need to take care of myself. (…) In order for me to be able to ride her and take care of her, I need, just like a horse eats and sleeps, you give them food and all that, I need to do the same to myself as well” (P7).
In summary, the six categories described above capture a range of activities, strategies, and orientations that participants described as self-care. These included practices related to bodily and practical maintenance, emotion regulation, cognitive reflection, self-directed compassion, engagement in everyday life, and connection with others. Across categories, participants described self-care as involving ongoing efforts to manage everyday demands and psychological distress, often highlighting tensions between knowing what they found helpful and being able to carry this out in practice. Rather than referring to a single or uniform set of behaviors, participants’ accounts reflected varied and sometimes shifting ways of engaging in self-care in their daily lives.
Discussion
In the following section, the findings are first summarized and interpreted in relation to existing conceptual models of self-care, before being situated within the broader psychological and clinical context of self-injury and recovery-oriented mental healthcare. Finally, implications for clinical practice and future research are considered.
The study explored how individuals receiving psychiatric care for NSSI understand and describe self-care in their everyday lives. Through RCA, six interrelated categories were identified, capturing self-care as a multidimensional and relational process. The six categories identified together illustrate how self-care encompasses practical, emotional, and relational dimensions. Self-care through bodily and practical maintenance reflected fundamental efforts to sustain daily functioning—such as eating, sleeping, and hygiene—practices that participants valued but often struggled to maintain during periods of psychological strain. Self-care through emotion regulation captured both adaptive and ambivalent strategies for managing affect, including refraining from destructive behaviors and, paradoxically, using self-injury as a way to soothe or regain control. Self-care through strategies driven by cognitive insight represented conscious reflection and intentionality—participants described structuring their day, setting goals, and making deliberate choices to act in line with long-term well-being, even when motivation was low. Self-care through self-directed emotional support highlighted the internal, compassionate stance that some participants sought to cultivate, including validating themselves and countering self-criticism. Self-care through engagement in work and daily activities reflected the stabilizing role of meaningful occupations and structure, while Self-care through relating to others emphasized the importance of interpersonal connection and receiving care through relationships. Across categories, self-care appeared as a dynamic process of maintaining stability, emotional balance, and meaning in daily life. Together, these aspects capture self-care as a behavioral, psychological, and relational endeavor.
Conceptually, the participants’ descriptions align partly with established models of self-care, yet they also extend and complicate them. In Riegel et al.’s (2019) framework, self-care involves maintaining, monitoring, and managing health-related behaviors. Martínez et al. (2021) further conceptualize self-care as the ability to act through awareness, self-control, and self-reliance—highlighting the cognitive and motivational processes that precede and sustain self-care behaviors. While examples of behaviors as well as elements of these dimensions were frequently mentioned in participants’ narratives (e.g., awareness of needs, regulation of impulses, and efforts toward independence), the present findings suggest that for individuals living with psychological distress and NSSI, self-care cannot be fully understood as a linear or autonomous process. Instead, it emerges as negotiated and relational, shaped by fluctuating emotional states, self-concept, and social context.
This interpretation resonates with recent work by Truscott et al. (2024), who argue that conventional definitions often frame self-care as a matter of personal responsibility and behavioral regulation, whereas people with lived experience describe it as an experiential and emotional practice—rooted in self-awareness, self-compassion, and the effort to restore emotional balance. The present study supports and expands this view by showing how participants’ practices of self-care involved not only performing caring actions but also managing ambivalence, shame, and fluctuating motivation. Self-care was thus not merely about doing what is “healthy” but about navigating the complex psychological terrain between caring for oneself and living with mental health difficulties.
Findings that were particularly salient and likely characteristics for this group of participants were the results found in the subcategories Self-injury is self-care and Refraining from destructive behaviors is self-care, where participants described self-care as both an effort to resist and, paradoxically, to manage distress through self-injury. In the broader literature, NSSI has been conceptualized primarily as a strategy for regulating overwhelming negative emotions and restoring a transient sense of control or relief (Klonsky, 2007; Nock, 2010). Participants in this study echoed these mechanisms but reframed them through the language of care—describing self-injury as a way to cope, soothe, or momentarily stabilize themselves when other strategies felt unavailable. This way of understanding self-injury is consistent with earlier qualitative work highlighting how individuals may experience self-harm as a means of managing the self, restoring a sense of control, or maintaining psychological coherence in the face of distress (Adams et al., 2005). Such accounts blur the boundary between care and harm and underscore the difficulty of sustaining self-care amid shame, self-criticism, and fragile self-worth—factors that often characterize the lived experience of NSSI (Klonsky & Glenn, 2009). Such complexities are rarely captured in the previous synthesis of self-care from the general health literature, which tends to emphasize adaptive and health-promoting behaviors.
These findings can also be understood through the lens of compassion-focused theory (Gilbert & Procter, 2006), which emphasizes the developmental process of re-learning safety, soothing, and self-acceptance in individuals with high levels of shame and self-criticism. In this framework, cultivating self-compassion is not a simple emotional stance but a corrective process that restores access to affiliative and caring motivational systems (Gilbert et al., 2010; Xavier et al., 2016). From this perspective, participants’ efforts to practice self-kindness, self-validation, or inner support can be seen as attempts to rebuild this capacity—to re-establish a caring internal dialogue where one’s own suffering is met with understanding rather than punishment.
These findings resonate with Spandler and Stickley’s (2011) critique of recovery models that overlook the emotional and relational dimensions of care. For individuals who struggle with internalized shame and a fragile sense of self-worth, self-care may require more than behavioral activation—it may involve re-learning the capacity to relate to oneself with compassion and dignity. This aligns with the view that self-care is not solely an individual task but often emerges through supportive relationships and compassionate environments.
In this light, the present findings situate self-care within a continuum between self-regulation and self-compassion, where caring for oneself is as much about regulating distress as about cultivating a benevolent stance toward one’s own vulnerability. Taken together, the findings suggest that while participants’ narratives reflect a conceptual alignment with previous frameworks, they also reveal lived tensions—particularly around the enactment of self-care—that are shaped by psychiatric symptoms, identity processes, and emotional barriers. Recognizing these tensions may be crucial for designing interventions that do not merely promote insight but also support patients’ capacity to translate that insight into sustainable action.
The Role of Therapeutic Influences
Another notable feature in the findings was that many of the strategies described by respondents bore clear traces of therapeutic influence. This was evident in explicit references to specific treatments, such as skills derived from dialectical behavior therapy (Linehan, 1993) including safety planning, distress tolerance, and emotion regulation techniques. It was also reflected in more implicit framings of care, such as identifying valued directions or cultivating internal dialogue—strategies commonly associated with ACT (Hayes et al., 1999) and related therapeutic approaches.
Taken together, these findings suggest that therapeutic concepts may become internalized and integrated into how individuals manage daily life, interpret their behavior, and navigate distress. This observation aligns with research showing that clients do not simply apply therapeutic tools mechanically but engage with therapeutic discourse through meaning-making—reflecting on it and adapting its ideas to their own contexts (Aleixo et al., 2021; Mellado et al., 2024). At the same time, these results raise important questions about how therapeutic frameworks shape individuals’ understanding of what constitutes valid or legitimate self-care. On the one hand, therapy can offer language, structure, and permission to engage in helpful forms of self-care. On the other, clinicians and systems may risk overlooking or devaluing self-generated strategies that fall outside established therapeutic paradigms. Individuals may develop personally meaningful ways of caring for themselves—sometimes idiosyncratic or unconventional—that nevertheless play a crucial role in daily functioning and recovery. Acknowledging and validating these strategies is essential, especially when working with populations who already experience marginalization or internalized stigma.
Strengths and Limitations
This study has several notable strengths. It draws on a heterogeneous sample from a clinically relevant and underrepresented psychiatric population, providing a broad empirical basis for describing how self-care is articulated in the context of NSSI. Individuals with experience of NSSI may be difficult to engage in research, particularly when exploring emotionally complex topics such as self-care. The breadth and depth of the material thus provide valuable insights into a population whose perspectives are often overlooked in both clinical and academic contexts.
The research team also brought diverse clinical and theoretical perspectives to the analytic process. Through ongoing reflexive dialogue, we interrogated assumptions, considered alternative interpretations, and examined nuances of meaning across cases. Analytic triangulation—discussing codes, patterns, and categorizations from multiple viewpoints—strengthened the credibility of the findings and fostered a grounded understanding of the material.
However, several limitations should be acknowledged. The coding process generated a large number of meaning units, which required substantial reduction and condensation. While common in content analysis, this inevitably entailed some loss of nuance. Certain marginal or divergent perspectives may therefore be underrepresented.
Another limitation concerns the reliance on participants’ self-reports. The data reflect what participants were able and willing to articulate about their experiences, which may not capture all dimensions of self-care. Some aspects of self-care may be implicit, habitual, or better recognized by others—such as family members or clinicians—than by participants themselves. Additionally, we cannot determine whether the narratives accurately reflect behaviors or idealized, aspirational accounts.
Although the sample was heterogeneous in age and psychiatric background, all participants were receiving psychiatric treatment at the time of the study, which may limit the transferability of findings to individuals who engage in NSSI outside formal care contexts. Moreover, all participants were recruited from Swedish psychiatric services, where care provision is embedded in a publicly funded, welfare-based healthcare system emphasizing accessibility and long-term therapeutic relationships. This sociocultural and systemic context may have influenced how participants conceptualized self-care and their reliance on professional support. Therefore, transferability to other cultural or healthcare systems should be made with caution.
Despite these limitations, the study offers a rich, empirically grounded account of how individuals with lived experience of NSSI understand and relate to self-care. It highlights both the potential and the challenges of engaging with self-care as meaningful practice in the context of mental health difficulties.
Implications for Practice and Research
The present findings suggest that self-care should be understood as an individualized and dynamic process, shaped by personal values, life history, and emotional context. For practitioners, this underscores the value of collaboratively exploring what self-care means for each individual and validating a wide range of strategies—even those that may initially appear unconventional or ambivalent. Future research should examine how self-care evolves over time, how it interacts with recovery processes, and how it is influenced by relational and systemic factors. Longitudinal and mixed-method designs may offer further insight into how self-care is maintained, abandoned, or transformed.
Conclusions
This study contributes to a more nuanced understanding of self-care among individuals with NSSI by highlighting its emotional, cognitive, and relational dimensions in the context of mental health difficulties. Rather than a checklist of healthy habits, self-care emerged as a dynamic and meaning-laden process shaped by therapeutic experiences, internal negotiations, and the challenges of daily life. Recognizing this complexity can help promote more compassionate, flexible, and person-centered approaches in both research and clinical practice.
Footnotes
Author’s Note
In accordance with Qualitative Health Research’s guidelines on research transparency, we disclose the use of NVivo software for data organization and OpenAI’s ChatGPT and Grammarly for language support. These tools were used to assist with proofreading, improving linguistic clarity, and refining the English translation of participant quotations from Swedish to English to better preserve tone and nuance. No generative AI tools were used for data analysis, interpretation, or conceptual development.
Acknowledgements
The authors would like to thank Hanna Grenner, Sara Pavlovic, Johanna Hansen, and Anna Stålmark for their valuable contributions to data collection. The authors are also deeply grateful to all participants who generously shared their experiences and perspectives, making this study possible.
Ethical Considerations
Ethical approval for this study was granted by the Swedish Ethical Review Authority (approval Dnr 2021-05054 and Dnr 2022-06058-02). All participants received written and verbal information about the study and provided written informed consent prior to participation. Participation was voluntary, and respondents were reminded that they could withdraw at any time without consequence.
Author Contributions
All authors have contributed to conception and design, and analysis and interpretation of data. All authors have been involved in drafting the article and revising it critically for important intellectual content. All authors have given final approval of the version to be submitted and agree to be accountable for all aspects of the work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was conducted within the scope of the authors’ institutional positions and received no external funding. All work was carried out as part of the authors’ regular academic appointments.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.