
Abstract
Non-suicidal self-injury (NSSI) is recognized as a public health concern owing to its chronic nature, association with suicide risk, and its growing prevalence rates across the globe. Including individuals living with NSSI in research is crucial as it offers opportunities to give primacy to participant voices and insights, further guiding therapeutic interventions. Research has established an association between history of traumatic events and adverse childhood experiences with subsequent risk of NSSI. When planning a qualitative research study with individuals with potential trauma history, researchers need to be aware of and sensitive to potential re-traumatization and distressing emotions that participants may experience during interviews, as well as complex trauma reactions that may affect individuals after study participation. The article emphasizes that researchers be cognizant of the multifaceted nature of trauma and how it can impact individuals and communities and be sensitive in their approach to interviewing vulnerable groups such as individuals with experiences of NSSI. The authors propose adopting a trauma-informed approach to ethically plan and conduct qualitative interviews exploring NSSI experiences. Trauma-informed recommendations for preparing and carrying out specific steps during different stages of NSSI interviews are detailed.
Non-suicidal self-injury (NSSI) is understood as the wilful harm caused to one’s own body tissue without suicidal intent, that is done for reasons not socially or culturally sanctioned (Nock & Favazza, 2009). NSSI includes behaviors like cutting, scratching, burning, and hitting, with most individuals using more than one method of self-injury (Lloyd-Richardson et al., 2007). NSSI is most frequent among adolescents and young adults with reported global lifetime prevalence of about 17–18% and 13%, respectively (Muehlenkamp et al., 2012; Swannell et al., 2014).
Non-suicidal self-injury is increasingly being seen as a major public health concern due to its chronicity and association with suicidal behavior (Grandclerc et al., 2016). Studies have reported that NSSI history predicts an increased risk for suicidal thoughts and behaviors (including suicidal ideation, plan, and attempts) in emerging adults (Hamza & Willoughby, 2016; Kiekens et al., 2018; Ribeiro et al., 2016). Additionally, NSSI often co-occurs with other mental health conditions like depression, anxiety, substance-use disorders, eating disorders, borderline personality disorder, dissociative disorders, and post-traumatic stress disorder (PTSD) (Cipriano et al., 2017; Lewis & Heath, 2015; Schatten et al., 2013).
Non-suicidal self-injury was listed as a separate category under “conditions for further study” in the DSM-5 (American Psychiatric Association [APA], 2013, p. 803), which led to a spurt in NSSI research globally, focusing on risk factors, functions, and consequences of self-injury (Brown & Plener, 2017; Cipriano et al., 2017; Klonsky & Muehlenkamp, 2007). In recent years, there has been a shift in focus with emphasis on including voices of individuals living with NSSI in research. Including participants’ perspectives is being seen as critical in garnering unique insights, reducing stigma, and improving mental health service delivery (Lewis & Hasking, 2019).
There is universal consensus that the benefits of conducting inquiry into experiences of NSSI must outweigh the risks associated with study participation (Lloyd-Richardson et al., 2015; Townsend et al., 2020). There are great benefits of including young adults with experiences of NSSI in research. Giving primacy to participants’ perspectives about their journeys with self-injury can aid in understanding and highlighting individual strengths and resources and enable participants to feel valued and heard. Talking about one’s experiences with NSSI might also be beneficial in fostering self-awareness and reflective understanding of past events. Additionally, participation in NSSI research can help individuals overcome stigma, seek mental health support, and share important insights about systemic challenges/barriers faced by them in their journeys of accessing professional care (Hasking et al., 2015).
While conducting research with individuals with experiences of NSSI, it is important to bear in mind that some participants may have a potential history of trauma/abuse. Therefore, researchers undertaking an inquiry in the field of NSSI might need to be considerate of trauma histories and take appropriate measures to ensure the physical, emotional, and psychological safety of participants. This article advocates for adopting a trauma-informed approach to qualitative interviews involving individuals with experiences of NSSI.
Non-Suicidal Self-Injury and Trauma
Adverse childhood experiences (ACEs) are potential traumatic events experienced during early/middle childhood. Some examples of ACEs include abuse (physical, sexual, or emotional), child neglect (physical or emotional), dysfunction in the family, such as domestic violence, substance abuse, criminal activity, severe mental illness, and absence of a parent (Dube et al., 2001). Additional adversities that have a major negative impact on children are loss of a loved one, living in poverty, facing peer rejection, social isolation, and witnessing community violence (Finkelhor et al., 2013; Oral et al., 2016).
It is well-established that experiencing trauma in childhood has long-term negative consequences with respect to one’s physical health/chronic diseases, wide range of mental health concerns (depression, anxiety, post-traumatic stress, and suicide attempts), and health risk behaviors like substance use and risky sexual behaviors (Felitti et al., 2019; Kappel et al., 2021; Norman et al., 2012). Research has shown that undergoing multiple ACEs is linked to an increased risk of NSSI and suicidal behaviors among adolescents and young adults (Angelakis et al., 2020; Russell et al., 2019; Wan et al., 2019). Specifically, child maltreatment in the form of physical abuse and neglect, emotional abuse and neglect, and sexual abuse was associated with NSSI in community samples of adolescents and adults (Liu et al., 2018; Serafini et al., 2017). With respect to child sexual abuse, studies have found a moderate association with NSSI, as both are correlated with shared risk factors (Klonsky & Moyer, 2008; Lang & Sharma-Patel, 2011). Conversely, research has also indicated that individuals living with NSSI may have a history of adverse/traumatic experiences. In a large-scale community study, about 65% of individuals with a history of NSSI had experienced at least one form of child maltreatment, while about half of them (48%) reported facing more than one form of childhood maltreatment (Brown et al., 2018).
Non-suicidal self-injury is seen across the diagnostic spectrum of PTSD, complex PTSD, and dissociative disorders (Cipriano et al., 2017; Kliethermes et al., 2014; Nester et al., 2022). A significant association is reported between childhood interpersonal trauma, PTSD, and lifetime prevalence of NSSI (Alharbi et al., 2020; Webermann et al., 2016).
Trauma and Its Impact on Individuals and Communities
Trauma can be viewed as a complex experience, including physical and psychological stress reactions, in response to a specific event or chronically repeating events that have multifaceted effects on an individual’s life. Individual trauma results from an event, series of events, or set of circumstances that is experienced by an individual as physically or emotionally harmful or life threatening and that has lasting adverse effects on the individual’s functioning and mental, physical, social, emotional, or spiritual well-being. (Substance Abuse and Mental Health Services Administration [SAMHSA], 2014a, p. 7)
The events that create the negative stress reactions can be acute or prolonged. Examples of acute traumatic events include accidents, natural disasters, unexpected loss of a loved one, or being diagnosed with a life-threatening illness. Prolonged or chronic trauma can take the form of distressing interpersonal events like repeated sexual assault, rape, intimate-partner violence, or communal, historical, cultural, and minority group–based discriminatory practices (APA, 2013; SAMHSA, 2015).
Individual trauma can also originate in the context of a community (where community is defined by shared identities such as religion, ethnicity, or geographical location). Communities are often subjected to traumatic events (natural disasters, discriminatory practices inflicted by one group on another like servitude, violence, or forced relocation), which can have prolonged effects transmitted across generations (SAMHSA, 2014a). It is therefore important for researchers to be aware of the history and the context of the participating communities and be particularly considerate of the social/historical challenges faced by individuals from Indigenous and minority groups.
Living with trauma can have long-term negative effects on individuals with respect to changes in the way they react to their environments, including constant hypervigilance, heightened arousal level, avoidance of situations, numbing, dissociation, and experiencing helplessness/vulnerability (SAMHSA, 2014a). Therefore, researchers working with individuals who may have trauma histories need to adopt a trauma-informed approach.
Trauma-Informed Approach
According to SAMHSA (2014a), a trauma-informed approach (TIA) incorporates the following defining features. A program, organization, or system that is trauma-informed
The TIA, also known as trauma-informed care (TIC), is a strengths-based approach to service delivery in mental and behavioral health settings, built on an understanding and awareness of trauma and its impact on individuals and communities, and using this knowledge to respond sensitively to individuals with potential trauma histories (SAMHSA, 2014b).
Principles of TIA
In NSSI research, adopting a TIA would mean recognizing that participants can have a history of adverse/traumatic experiences, actively recognizing signs of distress in order to adopt preventive strategies to mitigate re-traumatization, and providing a safe space for participants to share their experiences. The following are the key principles of TIA proposed by SAMHSA (2014a) that can be applied to NSSI interviews to facilitate a participant-centric, empowered, and collaborative research experience.
Safety
This principle promotes the importance of ensuring the physical, emotional, and psychological safety of individuals.
Trustworthiness and Transparency
All decisions are communicated truthfully with the goal of upholding the values of trust between all stakeholders.
Peer Support
Encouraging sharing stories of lived experiences of trauma among trauma survivors and other stakeholders is a key component in facilitating recovery, healing, and inculcating hope.
Collaboration and Mutuality
This principle emphasizes sharing of power and decentralizing hierarchy between all stakeholders to support and contribute toward collective healing.
Empowerment, Voice, and Choice
This principle highlights the strengths, abilities, resilience, and skills of individuals with trauma histories, so that they can take ownership of their stories and make their own decisions.
Cultural, Historical, and Gender Issues
This principle seeks to avoid cultural stereotypes, recognize and attempt to surpass historical trauma, and sensitively address and eliminate biases with respect to gender, sexual orientation, age, ethnicity, religion, and other identities.
Ethical Considerations in Non-Suicidal Self-Injury Research
When conducting research with vulnerable populations, researchers need to evaluate the potential risks and benefits of participation in their study. Specifically, this involves safeguarding participants’ rights, safety, and well-being by taking appropriate precautions against potential adverse outcomes (e.g., distress/re-traumatization) associated with research inquiry on sensitive issues. This is in accordance with the principle of “Beneficence and Nonmaleficence,” which entails maximizing benefits and minimizing harm for research participants (American Psychological Association, 2017).
The ethical considerations for planning research on self-injury are well-documented (Lloyd-Richardson et al., 2015). NSSI is most prevalent in adolescents and young adults, making them the most studied age group in research. Adolescents and youth are also a vulnerable/“at-risk” group due to presence of mental health co-morbidities and risk of severe/lethal self-injury in the future. The key ethical components to consider when undertaking NSSI research with adolescents and youth are seeking informed consent, maintaining confidentiality and privacy of participants, assessment of imminent risk of suicide, debriefing, and providing NSSI resources (Lloyd-Richardson et al., 2015; Singhal & Bhola, 2017). The following are some ethical principles that are critical in NSSI research.
Voluntary Participation and Informed Consent
The process of seeking informed consent includes providing relevant information about the research to potential participants so that they can freely choose whether or not they want to participate in the study. This upholds the ethical principle of voluntariness and conveys respect for participants’ autonomy to participate and/or withdraw participation from the research study.
In NSSI research, seeking active parental consent in addition to assent from adolescents is recommended. However, it is important to evaluate if seeking parental consent is posing risks to the welfare of adolescents (by disclosing NSSI to a parent who may be unhelpful or even abusive). In such cases, a request for waiver-of-consent can be made to the appropriate authorities/IRB, given that the research itself will cause less than minimal risk to the participants (Lloyd-Richardson et al., 2015). For young adults, their consent is sufficient as they are of legal age to evaluate the risks and benefits of the study and indicate their choice to participate.
Confidentiality and Its Limits
Confidentiality is a central tenet in research which entrusts researchers with the responsibility to safeguard information shared by participants within the research setting. It is important to balance the need to protect participant confidentiality and anonymity with evaluation of situations when a need to disclose self-injury may be essential. Usually, the question on whether to break confidentiality arises if participants disclose active suicidal ideation. These decisions can be based on a suicide-risk assessment protocol which considers several factors like severity, form of NSSI, or intensity and recency of suicidal ideation, along with evaluation of individual risk factors like history of abuse, difficult family relationships, levels of depression, and stressful life events. Previous research has established procedures to follow in such cases, which include documenting the factors leading to a decision to break confidentiality and responding to the identified high-risk participants through provision of resources, facilitating appropriate referrals, and assisted disclosures (Lloyd-Richardson et al., 2015; Singhal & Bhola, 2017).
Nonmaleficence or “Doing No Harm”
One of the most serious concerns that researchers may encounter when conducting NSSI research is evaluating whether the study would entail risks to participants by undertaking an investigation into distressing life experiences by inquiring about NSSI history and associated experiences. Specifically, it is important to understand whether the process of research inquiry could lead to re-traumatization through recollection of painful or negative emotional experiences.
Stein et al. (2000) summarized ethical considerations for studying psychological trauma. They highlighted that talking about one’s traumatic experiences can have therapeutic effects as well as negative influences based on the context. The participants’ experience in research may be contingent on various factors like researcher–participant rapport, whether participants feel heard and understood, and the value of research perceived by participants. Research has shown that most survivors of traumatic events like rape, domestic violence, and physical assault do not experience distress when participating in trauma research but view the experience as valuable and insightful (Griffin et al., 2003). Studies on trauma show that unpleasant reactions to research participation are temporary, decreasing a few weeks after the study, whereas positive reactions and perceptions of participation being meaningful last. Overall, studies report that despite minor discomfort/distress, participants do not regret participating in trauma research and find sharing their experiences useful for knowledge advancement (Carlson et al., 2003; Cromer et al., 2006; Legerski & Bunnell, 2010).
Iatrogenic effects in NSSI research refers to induction of negative emotions, NSSI thoughts/behaviors, or aggravation of pre-existing NSSI symptoms in participants by virtue of research participation (Lloyd-Richardson et al., 2015). A qualitative investigation about youth experiences of seeking care for self-harm (self-poisoning and self-injury) indicated that participants did not experience distress after taking part in the interview and found the research experience to be worthwhile (Byrne et al., 2021). Few other studies also found positive influences of participating in NSSI research as participants felt good about contributing to science, believed that their participation added value to research for a good cause, and improved their self-reflective abilities (Muehlenkamp et al., 2015; Whitlock et al., 2013).
Muehlenkamp et al. (2015) found that there were no immediate and short-term (up to 3 weeks) adverse/iatrogenic effects with respect to NSSI urges, behaviors, or emotional reactions in majority of participants after they responded to an online survey with detailed questions about NSSI. However, a small proportion of participants reported lasting distress after study participation. Another study with 13- to 15-year-old adolescents demonstrated that mood ratings and perception of participating in a survey on self-harm varied according to gender and history of self-harm. Responses to a visual analogue scale used immediately after participation showed that girls with self-harm history found the experience of research participation upsetting, whereas boys with self-harm history provided positive mood ratings. Overall, participants with self-harm history provided negative evaluations of participating in the study compared to participants without history of self-harm (Lockwood et al., 2018). In a qualitative study assessing the impact of participating in suicide-related research in adults, participants reported positive outcomes (experiencing catharsis and improvement in self-awareness) immediately after the interview but experienced a delayed lowering of mood which lasted for a few hours or days after participation. Follow-up interviews with the participants after months revealed that they did not regret participating in the study, and the negative effects of low mood were present for a short time period (Littlewood et al., 2021).
This indicates that individuals with experiences of NSSI can have a vulnerability toward negative stress reactions following NSSI research participation. This can be true for many participants regardless of whether there are visible signs of distress. Most studies have used subjective mood ratings to evaluate the impact of study participation. However, it is important to recognize that trauma reactions might be complex. Participants may remain in a hypo-aroused state (e.g., numbing of emotions) or hyper-aroused state (e.g., hypervigilance) for days following research participation, utilize strategies like substance use to cope with distress, or simply not report mood changes. Such varied impacts of research participation are often not inquired into and are likely to be missed.
Even if there are no long-term negative consequences by participating in NSSI research, researchers can strive to avoid/minimize participant distress during interviews, to maintain the ethical soundness of the study. We recommend that researchers undertaking NSSI research use a TIA to actively work toward recognizing potential signs of distress or re-traumatization as participants share their experiences, and seek to effectively respond and mitigate any stressful reactions. This aligns with researchers’ ethical responsibility of “avoiding harm” and prioritizing participants’ well-being (American Psychological Association, 2017).
It has also been contended that there could be substantial costs by not inquiring about trauma and abuse histories (Becker-Blease & Freyd, 2006). Asking careful and sensitive questions is necessary to convey to survivors that their experiences are important and a valuable addition to scientific knowledge. Involving trauma survivors in research and giving voice to their experiences empowers them and helps in understanding their perspectives on the phenomenon being studied (Legerski & Bunnell, 2010).
Trauma-Informed Approach for Qualitative Interviews in Non-Suicidal Self-Injury Research
Through this article, the authors (SK and CD) present recommendations for using TIA for qualitative NSSI interviews. SK is pursuing PhD in Applied Psychology. She is a psychologist with training and experience of working with individuals and families in clinical and community settings. She also received training in TIA as part of her postgraduate clinical course (MPhil in Applied Psychology). CD is the doctoral research supervisor of SK. She is a practicing psychotherapist and through community outreach initiatives works with individuals, families, and communities in urban and rural settings with a social justice and trauma-informed lens.
The current article is based on SK’s doctoral dissertation which focuses on exploring stories/journeys of young adults living with NSSI in India. NSSI is an emerging concern in India with reported lifetime prevalence of 21% among young adults and 1-year prevalence of 31–33% in combined samples of adolescents and youth (Bhola et al., 2017; Gandhi et al., 2021; Kharsati & Bhola, 2015). The suggestions presented in the article are based on the authors’ experiences and reflections of conducting in-depth qualitative interviews exploring youth journeys and experiences with NSSI. SK conducted online face-to-face interviews (via video-conferencing) with 14 young adults (19–25 years) with diverse identities, over a period of 18 months. The authors adopted a TIA (based on training as mental health practitioners) while conducting the research interviews to respond to participants’ experiences in research. The recommendations for NSSI interviews in the current article are built on TIA principles (SAMHSA, 2014a) that are supplemented and informed by feedback provided by our participants during debriefing sessions.
The authors acknowledge their position as women researchers and practitioners, with clinical training and experience providing therapy and conducting research with young adults with experiences of NSSI, representing diverse identities across gender, class, caste, sexual orientation, religion, and so on. We strive to maintain the values of inclusivity and diversity in research by ensuring participation of individuals across diverse contexts and backgrounds and encouraging sharing of their unique perspectives and experiences. We also value the importance of recognizing intersectionality among participants’ identities and acknowledging lived histories of trauma in participant stories.
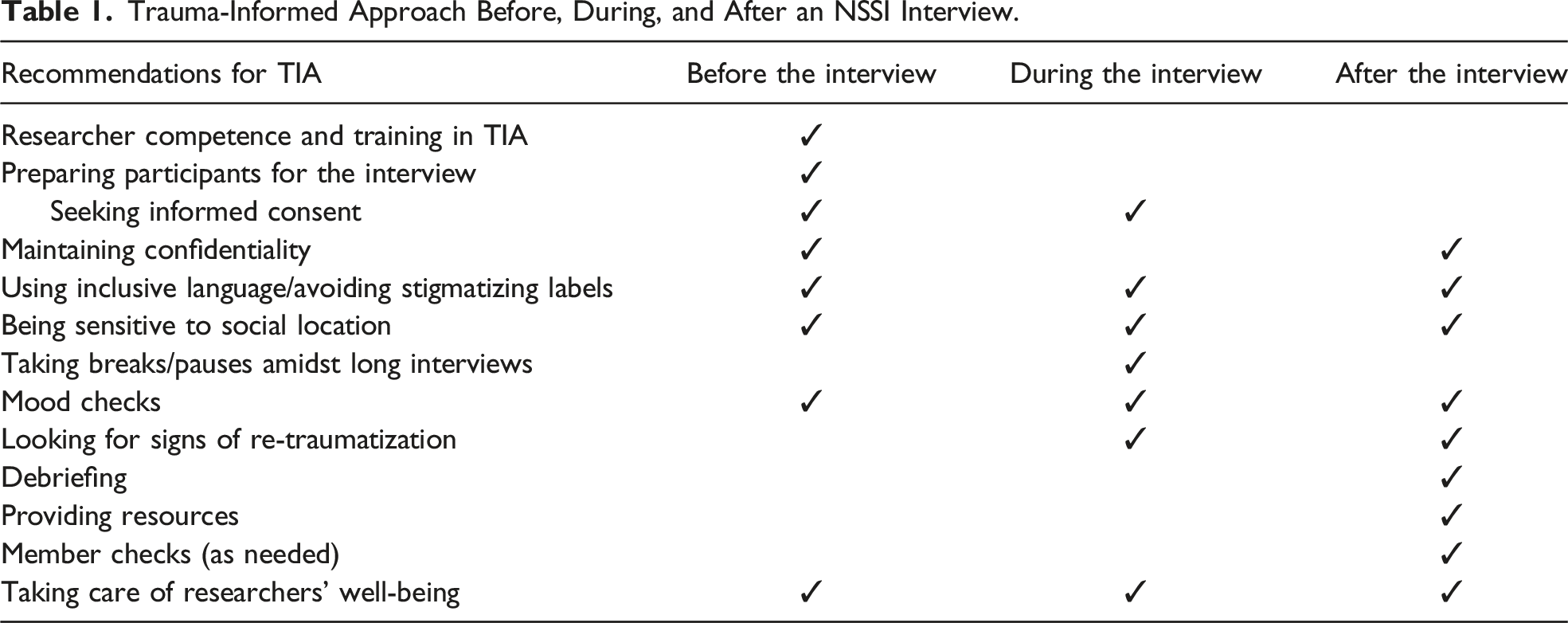
Trauma-Informed Approach Before, During, and After an NSSI Interview.
The TIA for qualitative interviews is applicable to NSSI research, globally across contexts. At the same time, we invite researchers to be mindful of unique cultural nuances and historical/community-based influences that may be relevant to participants of the research. For example, in the current research, the authors were cognizant of cultural/historical influences specific to Indian communities (e.g., being sensitive and respectful of caste identities). Additionally, we recommend being mindful of culture-specific non-verbal cues and gestures that could potentially indicate discomfort with research participation (e.g., monosyllabic replies, restlessness, and distressed body language). For instance, in India, people may find it difficult to say “no” or refuse participation, out of politeness and respect for the researcher, who may be viewed as an authority figure (especially if they are older in age). Researchers undertaking NSSI research with specific communities may therefore prefer to be mindful of the unique cultural context.
Researcher Competence and Training in Trauma-Informed Approach
Researchers involved in the study of experiences of NSSI may consider undergoing training in trauma-informed approaches, orienting their stance toward recognition of potential traumatic experiences, and taking active steps to prevent triggering negative emotions and re-traumatization. Researchers can adopt a calm, composed, and steady tone/stance to communicate a sense of continuity, consistency, and safety in the interview environment. While hearing emotionally laden and distressing events in an interviewee’s story, researchers may prefer to manage their own emotional reactions, remain calm, and express compassion and empathy to the participants (SAMHSA, 2015). This can be achieved by practicing emotion-regulation strategies and grounding techniques during clinical training and supervision that interviewers can incorporate to contain their anxieties or frustration. Cultivating knowledge of TIA creates competent trauma-informed researchers who espouse SAMHSA’s (2014a) principles of “Collaboration and Mutuality” and “Safety.”
Preparing Participants for the Interview
It is recommended to have a conversation with the participant over a phone call/initial meeting to explain the nature of the study, procedures involved, mode of data collection, and the duration and extent of participation. In face-to-face interviews, it is suggested to ensure the availability of an adequately lit and confidential space. Researchers may consider asking participants to choose where they would like to sit (some participants may prefer sitting closer to the door), checking with them if any object in the room is a potential trigger, and providing them an opportunity to hold on to a safe object. 1 It is a useful practice to make suggestions to the participants about keeping snacks and water with them (in online interviews) and informing the researcher if they need a break. This helps set the tone for the interview and communicates that participant comfort and well-being are prioritized. This is in line with SAMHSA’s (2014a) TIA principles of “Safety,” “Collaboration and Mutuality,” and “Empowerment, Voice, and Choice.”
Seeking Informed Consent
The participant information sheet (PIS) and informed consent document are crucial for ethical psychological research. Researchers can consider getting the PIS (containing details of researchers’ credentials/affiliations, objectives, and procedures of the study, as well as ethical issues pertaining to consent and confidentiality) approved by their institute’s ethics committee. In NSSI research, it is important to clearly delineate the potential risks and benefits of participation so that individuals can make an informed choice whether they would like to participate. Qualitative interviews encompass detailed exploration of participants’ life experiences. In self-injury research, it is likely that interviews may bring up discussions about potential trauma/abuse histories. It is advisable to have a written statement in the PIS and consent form about the possibility of experiencing distress while sharing personal experiences (Seedat et al., 2004). We also recommend including an explanation of what steps can be taken to manage emotions if participants feel distressed amidst the interview. This can include stating methods that might be employed to regulate emotions (grounding activities 2 and diaphragmatic breathing) so that participants know what to expect if they feel distressed.
The PIS and consent form can mention the rights of participants to not answer/skip questions they find uncomfortable or withdraw participation at any stage of research, without having to give reasons. Researchers can be trained to respond appropriately and sensitively to participants who express their wish to terminate participation. This can mean acknowledging the individual’s discomfort with the questions, responding in a non-judgmental and accepting manner to validate their feelings, and making appropriate referrals to mental health practitioners, if needed.
Participants can be encouraged to read the PIS and informed consent document carefully, before the interview, while the researcher may prefer to clarify doubts to participants’ satisfaction. Participants can be informed that they are free to ask any questions that may come up at a later stage. Researchers may also consider checking-in with participants and taking permission before asking questions related to specific sub-topics during interviews. This communicates that researchers have not assumed blanket permission and upholds SAMHSA’s (2014a) TIA principles of “Empowerment, Voice, and Choice” and “Trustworthiness and Transparency” by respecting the agency of participants in making moment-to-moment decisions.
Maintaining Confidentiality
Confidentiality is a central tenet of research. It is common practice to apprise participants that the data they share will be kept confidential and the steps that would be taken to ensure this. This information is typically elucidated in the informed consent document. When conducting research on NSSI, it also becomes imperative to discuss the limits to confidentiality which include disclosures of active suicidal plans or risk of serious harm to self or others. The conditions that would warrant a breach of confidentiality according to the study’s ethical protocol can be explained to participants prior to study initiation, so that they are aware of the steps that would be followed in these circumstances. For example, it would be helpful for participants to know that emergency services may be contacted to ensure their safety in case they disclose suicidal intent. Researchers can discuss steps involved in informing parents or family members of participants in case a decision to breach confidentiality is made. In cases where parents/guardians cannot be informed owing to difficult parent–child relationships, researchers can facilitate referrals to mental health services, with the participant’s permission (Lloyd-Richardson et al., 2015). Participants can also be asked to indicate a trusted contact (relative/friend/colleague/therapist) at the beginning of the study, whom the researchers may call if the need arises. At all times, it is crucial to keep participants informed and involve them in decision-making to maintain their autonomy and trust in the research process.
Additionally, researchers can share with participants how the data collected from them will be stored and used, along with procedures to ensure anonymity in written reports and publications. Use of pseudonyms and anonymizing identifying information are common practices. Striving to maintain confidentiality/anonymity of participants echoes the TIA principles of “Safety” and “Trustworthiness and Transparency” (SAMHSA, 2014a).
Using Inclusive Language/Avoiding Stigmatizing Labels
During all stages of NSSI interviews, researchers can communicate sensitivity and respect by using inclusive language/staying close to terms used by participants to describe their experiences. This helps participants feel heard and engage better with research. Terms like “cutter,” “self-injurer,” and “attention seeker” are best avoided as they are directed at the person living with NSSI, can be perceived as disrespectful, and perpetuate labelling/stigma associated with self-injury (Klonsky et al., 2014; Westers et al., 2021). Borrowing from the SAMHSA (2014a) principle of “Empowerment, Voice, and Choice,” researchers can attempt to highlight the strengths, resources, and skills of participants such that they feel empowered and in control of their experience.
Being Sensitive to Social Location
Before initiating the interview, researchers can consider reflecting on their social location, identities, and positionality to be mindful of any personal biases and views and how that might shape the interaction. Researchers can strive to create and communicate an inclusive space which is sensitive to the experiences of individuals belonging to different social locations with respect to their gender, sexual orientation, social class, financial standing, and educational, religious, and cultural background. This is in accordance with the SAMHSA (2014a) principle of “Cultural, Historical, and Gender Issues.”
Taking Breaks and Pauses Amidst Long Interviews
Since the nature of inquiry can be sensitive in NSSI research, researchers might consider avoiding lengthy interviews (lasting more than 3 hours). During the interview, researchers can stay in tune with the emotional and behavioral cues provided by participants. It is good practice to do periodic check-ins with participants to assess whether they are comfortable with the interview pace and if they would like a break. If participants appear fatigued or the interview duration is seeming longer than planned, we recommend pausing the session for that day and resuming the interview another day.
In trauma-informed qualitative interviews aligned with SAMHSA’s (2014a) principle of “Safety,” we encourage taking short pauses of 5–10 minutes to reorient one’s attention to the present. This is especially needed after discussion of heavy/emotional stories or after a long period of narrating one’s experiences. During this break, participants can take a screen break (in online interviews) or simply walk around, drink water, and have small snacks.
Mood Checks
The use of mood ratings in NSSI research has been shown to be useful (Lloyd-Richardson et al., 2015; Townsend et al., 2020). To work in accordance with the principle of “Safety” (SAMHSA, 2014a), researchers might consider starting with a baseline mood assessment to gauge whether the participant is calm/relaxed to proceed with the interview. This can be supplemented with periodic mood checks during the interview to assess any distress experienced in the moment. Researchers can follow up with a mood assessment after the interview by utilizing a visual mood continuum or subjective rating. It is essential that researchers use measures to mitigate negative mood (and bring the mood back to baseline levels), in case participants report distress after the interview. Some common ways to elevate mood that are known to work in NSSI research are showing cute animal pictures, using doodles, utilizing websites with interactive options (e.g., distract buttons which redirect to a neutral news webpage, showing cartoons/animations, or an activity page with options to draw/color/scribble), and watching nature videos (Arbuthnott et al., 2015; Goritz, 2007; Lockwood et al., 2018; Townsend et al., 2016). Researchers can also consider utilizing grounding techniques or breathing exercises after the interview to help participants regulate emotional reactions.
Looking for Signs of Re-traumatization
Participants in self-injury research may often deviate from the “window of tolerance” or optimal arousal level, when experiencing distressing memories or emotions related to past traumatic events. It is crucial for trauma-informed researchers upholding SAMHSA’s (2014a) principle of “Safety,” to identify these signs which may indicate that participants are triggered and their bodies/mind have activated the defense response. Experience of trauma memories can mimic the situation surrounding the original trauma and cause feelings of fear, anxiety, and a sense of danger. It is important that researchers notice any verbal or non-verbal cues suggesting activation of post-trauma responses/re-traumatization during and after the interview. Participant responses can be variable in the form of visible agitation or detachment from the interview (SAMHSA, 2015).
Some signs indicating a hyper-aroused state are tension, shaking/trembling, hypervigilance, anger/rage, racing thoughts, emotional reactivity, and feeling overwhelmed. On the other hand, some participants may also display signs of a hypo-aroused state which include reduced energy, not displaying any emotion, feeling numb, and dissociative symptoms such as staring blankly/fixed gaze, feeling disconnected, glazed appearance, confusion, prolonged silence, monotonous tone of voice, and asking the researcher to repeat what they said (Kerr, 2015).
During the interview, interviewers can consider looking for signs of re-traumatization and if present ensure that they take steps to reorient the participant to their window of tolerance and cultivate feelings of safety by bringing their attention to the present setting. Grounding techniques aid in distracting the individual from feelings of overwhelming pain from the past and focus their attention in the “here and now” (California Center of Excellence for Trauma Informed Care, 2011). A common grounding method is the “5-4-3-2-1 technique” where participants can engage the five senses of the body and feel centered in the current physical reality. The 5-4-3-2-1 method involves asking individuals to list 5 things in their immediate environment that they can see (e.g., fan, table, and picture frames), 4 things that they can feel/touch (e.g., their hair, the ground beneath their feet, and the chair they are sitting on), 3 things that they can hear (e.g., sound of a fan, bird outside the window, and their own voice), 2 things they can smell (e.g., perfume/scented candle), and 1 thing that they can taste (e.g., chocolate/chewing gum) (NHS, 2021).
It is also good practice to validate and normalize participants’ feelings if they are overwhelmed. Sensitively responding to the current feelings and letting them know that it is natural to experience upsetting emotions after discussion of sensitive issues can be helpful. For example, participants can “tear up” or cry while discussing a difficult event. In such situations, researchers may prefer to respond with empathy, reflect what the participants are feeling in the moment, and give them time and space to respond. Offering to take a pause, drinking water, and engaging in grounding activities and diaphragmatic breathing can help create a sense of safety and calm. Researchers with clinical training can also consider providing brief psychosocial support to respond to participants' distress. Checking with participants prior to the interview what helps them when they are upset can be a useful exercise, which researchers may utilize if needed (SAMHSA, 2015). Researchers may prefer to closely observe participants’ emotional cues. If they appear too distressed to continue, they can be politely reminded of their rights as participants and asked whether they would like to resume the interview another day or withdraw participation. In either case, participant safety should be ensured before termination and appropriate referrals to mental health centers can be facilitated.
A decision to terminate the interview can be taken in collaboration with participants if there are signs indicating re-traumatization. In this context, it is important to understand whether participants can freely indicate that they want to withdraw participation, owing to power imbalances between researchers and participants. Recognizing and acknowledging non-verbal signs of discomfort in such situations becomes crucial when participants do not explicitly state that they want to discontinue participation (e.g., prolonged silences and restlessness/agitation). Recognizing these cues and sensitively checking-in with participants can be helpful in communicating that participants’ well-being is prioritized.
Debriefing
It is crucial in trauma-informed research to conduct a debriefing session after the interview to understand participants’ research experience. Participants can offer critical insights on the pace, wording, and structure of the interview and practices they found helpful during the research process. It is also important to check for any difficulties experienced by participants and take appropriate steps to mitigate that in upcoming interviews. Researchers may consider highlighting participants’ strengths and resources while concluding interviews and make linkages to participants’ resilience/courage to speak about their journeys. This aligns with the TIA principles of “Safety,” “Collaboration and Mutuality,” and “Empowerment, Voice, and Choice” (SAMHSA, 2014a).
Providing Resources
The provision of resources/reading material on NSSI to research participants is a common practice (Lloyd-Richardson et al., 2015; Singhal & Bhola, 2017). Helplines for psychological support can be provided to direct individuals to functional modes of mental health services if they need additional support after study termination. This is in line with SAMHSA’s (2014a) TIA principle of “Safety.” It might also be important to discuss with participants the procedure for contacting crisis helplines or mental health support systems (including text/chat/web-based modalities). After the COVID-19 pandemic, crisis helplines have observed a rise in distress call volumes and call durations globally (Brülhart et al., 2023; Turkington et al., 2020; Wilson, 2021). Therefore, researchers may prefer to apprise participants of the possibility of long wait times or connection difficulties that they might face while calling a helpline number. The list of resources provided can include multiple numbers of municipal, state-level/provincial, and national helplines, and participants can be encouraged to try different numbers if needed or contact a trusted friend or family member who can further help them connect to mental health services. A list of practitioners providing affirmative therapies and discounted rates of therapy for minority groups can also be included.
Additionally, researchers may also prefer to include links to helpful websites with resources related to NSSI as well as coping strategies and distraction techniques that participants can utilize to manage their distress. Examples of such resources can be found on the websites of the “International Society for the Study of Self-Injury” (itriples.org), “Self-Injury Outreach and Support” (https://sioutreach.org/), and Cornell University’s “Self-Injury and Recovery Resources” (http://www.selfinjury.bctr.cornell.edu/). Researchers can also check with participants if they have any queries regarding the list of resources and can offer to demonstrate how to access the helplines/chat features, videos, or other resources on specific websites.
Member Checks
Member checking or respondent validation is considered an important practice in some forms of qualitative research to ensure data validity/trustworthiness, rigor, and credibility by sharing transcripts or research findings with participants (Candela, 2019; Lincoln & Guba, 1985; Varpio et al., 2017). It is a useful technique to assess accuracy of meanings conferred to the data and aligning the findings with participant voices. However, it is also necessary to evaluate whether member checking is beneficial for all research participants, specifically when there could be a risk of harm by asking participants to re-live traumatic experiences. It is argued that participants’ well-being should be given precedence over data reliability (Hallett, 2012). Additionally, participants do not make significant changes to interview transcripts, with modifications largely confined to correcting grammatical errors or confirming sensitive information that needs anonymization (Rowlands, 2021). Undertaking member checking needs to be ethically guided with consideration of several aspects like potential health/risk status of participants, possibility for reliving trauma histories, and participant distress over viewing their speech in text form (Birt et al., 2016; Rowlands, 2021). Presenting synthesized data collected from all participants is a possible way of minimizing individual distress, yet giving an opportunity for providing feedback on the way their collective experiences is represented (Birt et al., 2016).
In NSSI research, where individuals may have trauma histories, researchers can consider weighing the benefits of member checking against consequences like potential re-traumatization by engaging with emotionally laden transcripts. We recommend taking permission from participants when transcripts are ready and asking them to indicate whether they would like to read their narratives. Specifying a time frame for participant response, with scope for brief flexibility, is helpful (Rowlands, 2021). The findings can be organized according to key features, themes, or timelines, that participants can verify, if they have the emotional bandwidth to engage with the research material, at the time. Helpful website links and resources can be provided which act as distractors and aid in reducing participant distress while they read their transcripts. Responsibly using member checks espouses SAMHSA’s (2014a) trauma-informed principles of “Safety,” “Trustworthiness and Transparency,” and “Collaboration and Mutuality.”
Taking Care of Researchers’ Well-Being
Researchers involved in qualitative research on sensitive topics may be susceptible to emotional risks and burdens associated with the nature of inquiry and are often unprepared for emotional disclosure by participants, if they do not have clinical training or experience (Dickson-Swift et al., 2008; Mckenzie et al., 2017). Research assistants working on suicide and NSSI-related research reported feeling “shocked,” “distressed,” and “disturbed” after learning about sensitive and graphic details of participants’ self-injury. They also reported being emotionally invested in participant stories, becoming aware of tragic events or dysfunctional family patterns, feeling frustrated with lapses in mental health delivery systems, and experiencing emotional exhaustion after engaging with the data for long periods (Mckenzie et al., 2017).
It is likely that researchers engaged in NSSI research may experience secondary trauma through exposure to highly distressing accounts. They may encounter challenges like burnout, feeling desensitized, losing motivation, and tuning out from the research after repeated engagement with traumatic participant recollections. Individuals conducting NSSI research may also have personal history of trauma, in which case hearing similar accounts can be triggering.
Researchers often rely on informal support from family or friends or use personal coping strategies and distractions to distance themselves from the emotional effects of research. While this may be helpful in the short term, it is recommended to have provisions for formal and professional supervision which trains and prepares researchers undertaking sensitive research for the nature of data they might receive and how to cope with the associated distress (Mckenzie et al., 2017).
Researchers may prefer to debrief about their experience and emotional burden with supervisors and peer researchers (who may help in providing a sense of community by sharing similar experiences). The role of research supervisor in creating an accepting, safe, and validating environment embedded in SAMHSA’s (2014a) TIA principles of “Safety” and “Peer Support” is important for the welfare of researchers.
Additional steps to maintain a healthy mind–body connection include journaling, exercising, eating/sleeping well, cultivating a hobby, meditation, and self-reflection. Awareness of personal stressors and striving for work–life balance by taking periodic breaks from work and fostering connections with one’s family, community, and personal interests could be effective in promoting researchers’ well-being (The National Child Traumatic Stress Network, 2018).
Discussion
The current article attempts to elucidate trauma-informed approaches to navigate different components encountered in qualitative research interviews involving individuals with experiences of NSSI. As seen earlier, including participant voices in NSSI research is a great way to inculcate their unique insights in the literature and inform effective therapeutic interventions guided by their experiences.
In qualitative interviews involving individuals with experiences of NSSI and potential trauma histories, the research environment encompasses a complex interplay of various identities, emotional states, and cultural and historical backgrounds that the researcher and participant bring to the setting. Many individuals may have a history of experiencing community-based trauma or discriminatory practices tied to specific identities. Trauma histories are often linked to human rights violations with respect to both individual and collective/community-based violence or negligence. We recommend that researchers adopt a human rights–based perspective and be sensitive to the intersection of various social locations and how they interact in a research context. As an ethical practice, qualitative researchers are encouraged to reflect on their own positionality and associated views that they bring to the research setting with respect to their identity and historical backgrounds.
Considering this nuanced understanding of complex trauma histories, in addition to potential history of early childhood adversities faced by individuals with experiences of NSSI, researchers have an ethical responsibility to be trauma-informed and adopt strategies to mitigate the effects of potential re-traumatization. We advocate that researchers be adept in principles of TIA and actively strive to integrate them in all stages of qualitative research, from conceptualization of the study to distribution of findings. The recommendations for TIA presented in this article are an attempt to invite qualitative researchers to consider the ethically appropriate measures for their study within a trauma framework to minimize risk for participants living with NSSI. While the suggestions presented uphold all the principles of TIA, it is important to note that many of them are related to SAMHSA’s (2014a) principle of “Safety.” This is based on the understanding that effects of trauma reactions can be prolonged and complex. Participants with potential trauma histories can have difficulty trusting their environment, be on the lookout for signs of danger, and can be triggered by different elements in the research environment. Trauma-informed researchers may consider taking active steps to reassure participants of the methods followed to ensure their safety and build trust during the research experience.
Finally, it is important to reflect on the potential impact of planning a study on NSSI during times of crisis, like the COVID-19 pandemic and its associated challenges. The pandemic negatively affected mental health and social well-being of individuals worldwide, with reported increase in depressive and anxiety disorders (Santomauro et al., 2021). Researchers may consider making informed choices whether a study likely to create emotional distress should continue during a universal pandemic, when individuals might be distraught with multiple challenges. Townsend et al. (2020) recommend contextualizing ethics of studying sensitive topics like suicide/self-injury during a pandemic, by utilizing mood-mitigation measures and ensuring that updated information is provided about the format in which mental health services used for participant referrals are operating.
Conclusion
There is significant value in studying the experiences of individuals living with NSSI, as they offer important insights into their life stories, gaps in service provisions, and useful strategies that aid help-seeking. Undertaking qualitative research interviews in the area of NSSI must be informed by an acknowledgment and awareness of potential trauma histories in participant stories. We advocate that researchers be trauma-informed, ethical, and integrate sensitivity to different social locations within a TIA framework while planning a qualitative study on NSSI.
Future Directions
The implication of presenting trauma-informed suggestions for qualitative NSSI interviews is to create a dialogue about the nuanced and complex nature of trauma and its effects. This article attempts to encourage training of researchers in TIA so that they are aware of and sensitive to social injustices and prevalence of varied forms of trauma histories in different social groups. The trauma-informed recommendations presented can be extended to qualitative research inquiring into experiences of other vulnerable groups/communities and highlight special considerations of using TIA for different qualitative methods like observation, focus groups, or ethnography. Researchers can consider expanding the ethical framework in trauma-informed research to include relational, feminist, and indigenous ethics to integrate the interplay of various participant identities with community trauma. Finally, researchers can consider including individuals with experiences of NSSI in advisory groups while planning/developing research and using their insights to inform and enrich guidelines for trauma-informed qualitative research.
Footnotes
Acknowledgments
We would like to sincerely thank the research participants who shared their stories of NSSI and showed great courage in talking about their journeys. The motivation for preparing trauma-informed recommendations for qualitative inquiry into experiences of NSSI was based on participants’ experiences and interactions during research interviews.
Author Contributions
SK and CD conceptualized the content of the article. SK drafted the manuscript and revised subsequent drafts. CD provided critical feedback for revision. Both authors approved the final version of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.