
Abstract
Loneliness is a health concern for individuals with chronic disease. Unlike most loneliness interventions that connect people to existing groups, the G
Introduction
Loneliness and its health consequences are an increasing focus for many community and hospital services (e.g., Christiansen et al., 2023). While the harmful effects of loneliness on physical and mental health are well-documented (e.g., Beutel et al., 2017; Mann et al., 2022), questions are now being raised, and solutions proposed, about how best to intervene given the wide-ranging circumstances and contexts within which loneliness can present (Morrish et al., 2023). Many of these solutions involve offering people activities to connect them socially with others in their local community, either through the support of charity volunteers or more formal community navigators who adhere to a social prescribing model (e.g., Reinhardt et al., 2021). An alternative approach is to help people build their own social capability in ways that enable them to recognize and manage loneliness. This is where the G
G4H has proven successful in reducing loneliness and depression in clinical trials (Cruwys, Haslam, Haslam, et al., 2022; C. Haslam, et al., 2016, 2019) and to have an advantage over cognitive behavioral therapy (CBT) in protecting against loneliness relapse under conditions of social threat (Cruwys, Haslam, Rathbone, et al., 2022). In this qualitative study, we aimed to extend beyond traditional clinical trial methodology to determine the program’s acceptability and usability for adults living with, or at risk of, chronic disease. Our focus was on participant experiences of the G4H program in meeting their social connection needs, while also exploring the factors that may facilitate or hinder successful participation.
Chronic Disease and Loneliness
Chronic disease is characterized as a long-term health condition that requires ongoing medical management or lifestyle adjustments, with common presentations including diabetes or cardiovascular disease, and mental health disorders such as depression or anxiety (e.g., Helgeson & Zajdel, 2017). These conditions impact general health and well-being by limiting functioning, causing chronic pain, and contributing to emotional and psychological challenges, which often reduces quality of life (e.g., Turk & Okifuji, 2002).
Loneliness predicts the development of chronic disease and increases morbidity and mortality (e.g., Hawkley & Cacioppo, 2010; Masi et al., 2011). Individuals with chronic conditions are lonelier than the general population, often because of barriers to social engagement resulting from physical limitations, the need for frequent healthcare visits, and the stigma associated with their condition (e.g., Nicoloro-SantaBarbara & Lobel, 2024). For many, loneliness is rooted in the liminal experience of adjusting to and sustaining a new normal in life with chronic disease (Cheung et al., 2025). These barriers can exacerbate feelings of loneliness, which, in turn, can worsen mental health conditions, creating a vicious cycle (e.g., Hawkley et al., 2010; Petitte et al., 2015).
Addressing loneliness and fostering social connectedness is critical in managing chronic disease, highlighting a need for interventions that go beyond medical management and consider the psychological and social dimensions of health (Theeke & Mallow, 2013). Nevertheless, the issue of loneliness in this population is often overlooked and the more common social prescribing approaches show mixed results. While some interventions have demonstrated positive effects (e.g., Masi et al., 2011), others have found no changes in reducing loneliness (e.g., Gardiner et al., 2018) or alleviating psychological distress and social anxiety (e.g., Dingle et al., 2024). Perhaps most problematic is the general lack of a strong theoretical basis to determine how best to optimize the effects of social prescribing but also sustainability challenges given their effects often diminish quickly after the intervention (C. Haslam et al., 2018). Particularly in populations already navigating the barriers associated with chronic disease, more effective and longer lasting solutions are needed.
Lasting Solutions: Building Social Capability
As illustrated above, simply offering any group activity is not a recipe for success. Rather, more consistent findings emerge where attention is paid to the nature of those group memberships and how they align with the meaning, purpose, and value people seek in their lives. Social group memberships that reflect a person’s sense of self or identity are more likely to influence health (C. Haslam et al., 2018). Accordingly, Steffens et al.’s (2021) meta-analysis found that interventions, which build and strengthen social identity (e.g., as us living with chronic disease), had a moderate-to-strong effect on health and well-being outcomes. Such a social-identity-focused approach may be especially important for individuals with chronic conditions, given their ongoing health challenges require long-term solutions to loneliness while preventing the worsening of mental and physical health symptoms (e.g., Mann et al., 2022).
Existing psychotherapy programs, such as CBT for loneliness, pay some attention to the building of social capability (e.g., Hickin et al., 2021). However, the focus of most programs is primarily on the cognitive, not social, aspects of loneliness, and as a result, the strategies employed are not guided by relevant social theorizing (S. A. Haslam, et al., 2024). Moreover, accessing these psychotherapy programs often requires a clinical diagnosis and referral, which can carry stigma and create an additional barrier for individuals. Furthermore, they tend to overlook the role of prevention in addressing loneliness early on, before it leads to more severe health consequences (Cruwys et al., 2021).
A program addressing these issues is G4H, which focuses on empowering people with the knowledge and skills needed to recognize and manage loneliness and social disconnection (Cruwys, Haslam, Haslam, et al., 2022; C. Haslam, et al., 2016, 2019). As an active psychotherapeutic intervention, G4H is theoretically informed by the Social Identity Approach to Health and leverages principles of social group identification and the psychological resources these provide to support individuals in developing and enhancing their social capabilities. (C. Haslam et al., 2018). During the program, individuals gain the knowledge, skills, and tools to actively build and strengthen social connections, initially within the G4H group, which provides an in-vivo experience, but also across their wider social group networks to support sustained meaningful connection beyond the program. An overview of the program is illustrated in Figure 1. Schematic of the G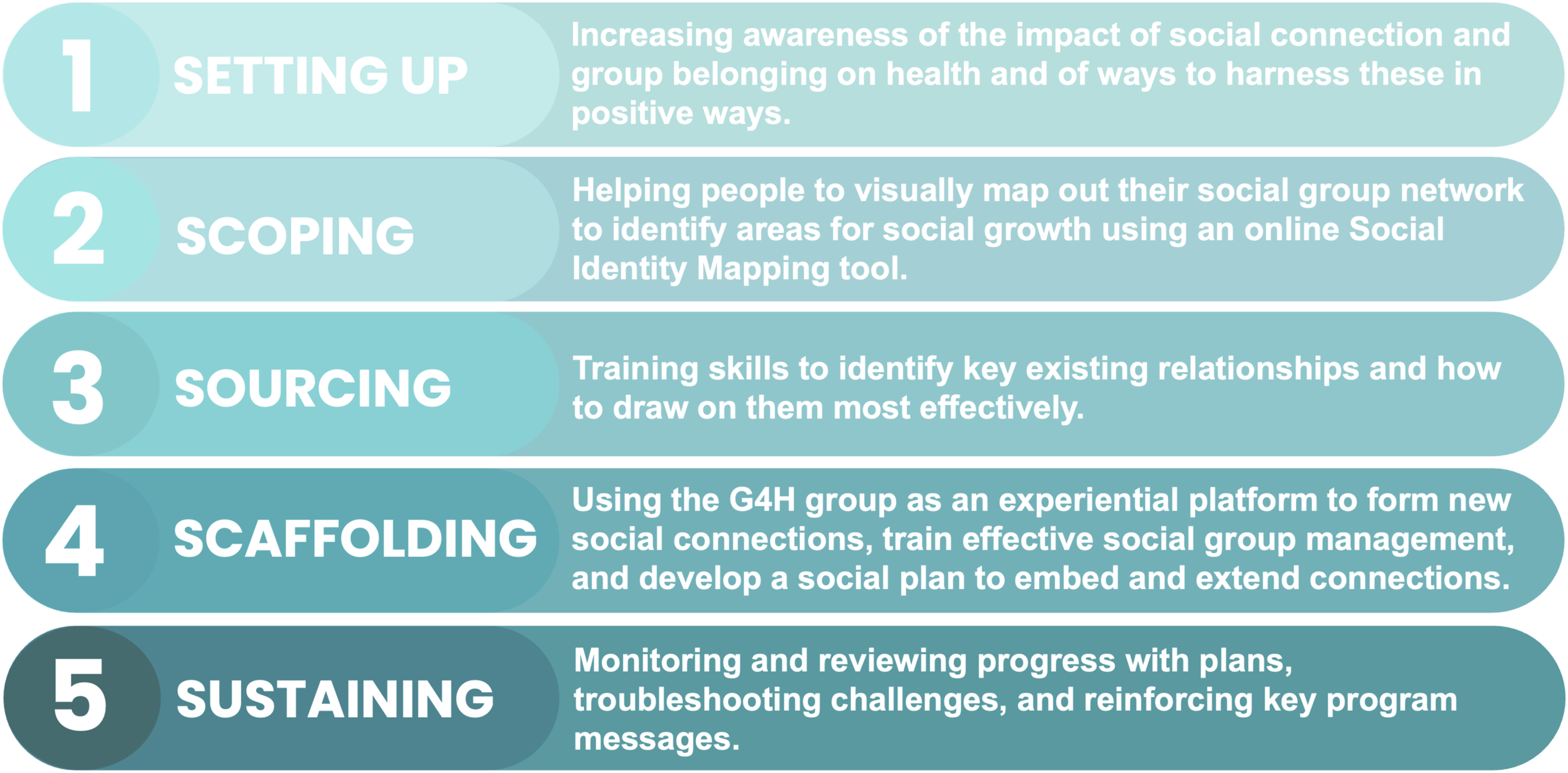
G4H has demonstrated efficacy across three clinical trials (Cruwys, Haslam, Rathbone, et al., 2022; C. Haslam, et al., 2016, 2019). These studies demonstrate that G4H significantly reduces loneliness, while enhancing mental health, well-being, and social connectedness at follow-up (i.e., after 2 months, 6 months, and 12 months). Both participants and facilitators have reported high levels of program acceptance, engagement, and feasibility (Cruwys, Haslam, Haslam, et al., 2022). While there is evidence that all participants receive some benefit from the program, G4H is particularly effective for those presenting with more severe loneliness and associated depression and social anxiety (Cruwys et al., 2023). This combination of mental health conditions is not uncommon among individuals living with chronic disease. Given the long-term nature of chronic disease, mental health symptoms often fluctuate (e.g., Lim et al., 2016), highlighting the importance of equipping participants with the skills to recognize and manage loneliness when it arises. G4H was developed to address loneliness management; however, its acceptability and participant experience have yet to be evaluated in individuals with chronic disease.
The Present Study
Individuals with chronic disease are particularly vulnerable to long-term loneliness due to the ongoing challenges of managing their condition. While existing interventions can offer temporary relief, a more effective approach would focus on strengthening individuals’ social capabilities, enabling them to recognize and manage loneliness independently. G4H meets this need, and the present study provides a qualitative evaluation of the acceptability and experience with the program within the new population of individuals with chronic disease and in the context of its integration into a broader health service framework. By understanding the factors that facilitate or hinder engagement, this study contributes valuable insights into optimizing G4H for this demographic and informs wider-scale effectiveness studies.
Methods
Methodology and Design
Our study has been informed by a constructivist approach, given its focus on recognizing and understanding the multiple realities of participants that are socially mediated and experientially based (Guba & Lincoln, 2005). Consistent with this approach, we used an inductive qualitative methodology to explore the acceptability of the G4H program among individuals with chronic disease, as well as their overall experiences engaging with the program, including barriers and facilitators to engagement. Data were collected through in-person focus group discussions (FGDs) alongside individual online interviews for those who could not attend in-person. We chose to use FGDs as they are particularly well-suited for exploring shared experiences among participants taking part (Krueger, 2014). This study received ethical approval from the Human Ethics Board of The University of Queensland (2023/HE002390).
Researcher Positionality
As an interdisciplinary team committed to reducing loneliness and advancing social justice, particularly in regional communities with limited healthcare access, our expertise spans psychology (clinical, social, and organizational), public health, social work, physiotherapy, exercise physiology, epidemiology, systems thinking, health policy, and qualitative research. We applied our expertise in complementary ways during data analysis and interpretation, using multidisciplinary language and emphasizing practical implications to ensure accessibility for diverse audiences. With one team member living with a chronic disease and four having worked in regional communities, we share some lived experiences with participants. Our discussions incorporated reflections on personal experiences with loneliness, knowledge of the G4H program, and its delivery, contributing to nuanced interpretations. During analysis, we considered our positionalities by reflecting on what stood out to us and our reactions to the data.
Participants and Data Collection
Participants were enrolled in a broader regional nursing and allied health service supporting chronic disease prevention and management in Toowoomba, Queensland, Australia. Eligibility required individuals’ participation in the G4H program. A staff member from the service introduced the study to all G4H program participants from the six groups, providing a brief verbal and written study description. While the initial four G4H groups were referred to the program based on their reported levels of loneliness when joining the health service, the final two groups were informed about the program and allowed to self-refer. Interested individuals were assured their involvement would not affect their relationship with the health service and were asked for consent. Those who consented shared their availability and were later informed of the FGD schedule. A total of 28 participants (approximately two-thirds of all participants), from all six G4H groups, were recruited. Sample size was guided by both pragmatic decisions (inviting all G4H cohorts to participate) and information power, meaning that we ceased data collection when all eligible participants had taken part in the study and when we thought that the data had sufficient information power, based on the narrow study aim, the highly specific sample, the theory-driven nature of the study, and the rich and reflective dialogue in the focus groups and interviews.
Overview of the FGDs and Interviews Participants Attended
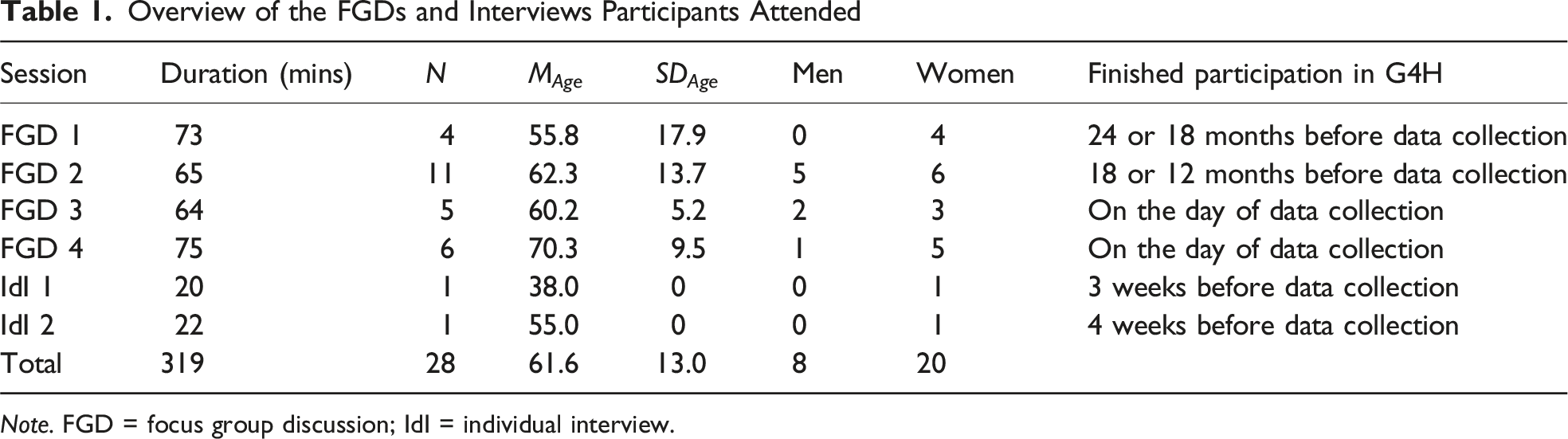
Note. FGD = focus group discussion; IdI = individual interview.
Each focus group was facilitated by two researchers, unknown to participants and with no prior involvement in the delivery of G4H. The facilitators introduced the study, emphasized confidentiality, and ensured equal speaking opportunities. Consent for audio-recording was obtained. The topic guide covered (1) expectations of the G4H program (e.g., “Did the G4H program go according to plan and meet your expectations? Why or why not?”), (2) motivation for participation (e.g., “What motivated you to complete the G4H program?”), (3) application of learned skills (e.g., “Have you continued to use the skills and strategies learned in the G4H program in your daily life? If so, how?”), and (4) additional experiences and perceptions (see Supplemental File 1). The FGDs were transcribed verbatim, checked for accuracy, and de-identified by LN.
Analysis Strategy
We used reflexive thematic analysis (RTA; Braun & Clarke, 2006, 2019) to explore participants’ experiences with G4H focusing on (dis)engagement, the program’s impact on their lives, and suggestions for improvement, while also engaging with our collective positionalities. RTA was chosen for its inclusion of researcher perspectives, which was particularly important given our understanding of G4H and our experiences working in regional areas and with individuals with chronic disease. A descriptive approach to RTA allowed us to detail participants’ experiences while suggesting practical program refinements for chronic disease management in regional settings.
While there are many ways of working with RTA, our six-phase iterative analysis began with familiarizing ourselves with the data (phase 1). Four authors read the first FGD transcript, noted initial thoughts, and discussed those over a two-hour meeting. This process was repeated for all transcripts over four additional meetings, totaling 10 hours of team discussions. The following key questions guided the discussions: (1) What are participants’ perspectives of the G4H sessions attended? (2) What factors contributed to completers’ satisfaction with G4H? (3) What aspects of participants’ responses stood out to you? (4) What can we learn about participants’ perspectives of and experiences with G4H? (5) Was there anything unexpected that caught your attention and, if so, what was it and why do you think it stood out to you? (6) How would you describe your responses/reactions to the data?
Discussions were audio-recorded and summarized by VW, who used these summaries to guide coding in NVivo 14 (phase 2). Drawing from the analytical summaries and codes, VW generated preliminary themes (phase 3). These themes were refined with NC (phase 4) and reviewed by the entire team (phase 5), with any differences in interpretation being discussed over a team meeting and through revisions to the draft results, with the view to include a range of interpretations throughout the themes and their descriptions. To mitigate potential overly positive interpretations of participants’ responses arising from the authors’ positive stance on G4H, the team attempted to remain aware of their positionalities, included an experienced qualitative researcher without a track record in G4H (NC), discussed alternative interpretations, and considered ways in which the delivery of the program could be improved for this cohort as part of the data analysis. To this end, all authors played a role in reflexive collaboration and broadening the interpretative lens through which the data was considered. The final phase involved writing and revising the results (phase 6). Braun and Clarke’s (2020) guidance informed our rigorous approach throughout.
Results
Figure 2 summarizes key themes from participant experiences with the G4H intervention within a broader health program, highlighting how factors like past trauma, life changes, social isolation, and chronic disease seemed to influence their experiences. Participants identified success factors such as group connectedness, facilitators’ expertise, support, and program quality. Barriers included personal challenges (e.g., social anxiety and caregiving), program-related issues (e.g., content accessibility and stigma), and external factors (e.g., work commitments and travel). These barriers led to suggestions for future G4H program improvements, focusing on accessibility, recruitment, length, and delivery. De-identified quotes illustrate the themes and subthemes. Overview of the identified themes and subthemes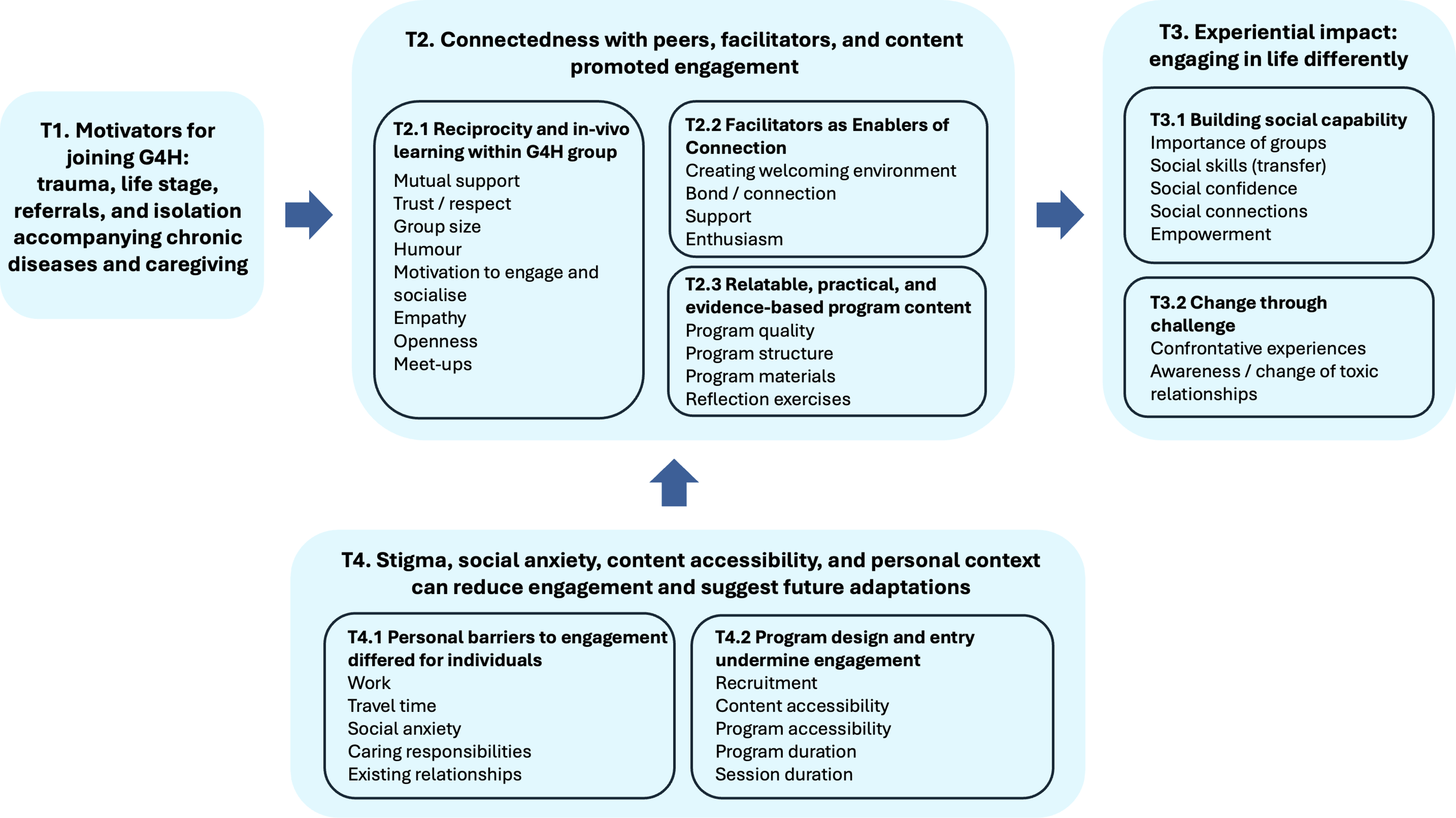
Theme 1: Motivators for Joining G4H: Trauma, Life Stage, Referrals, and Isolation Accompanying Chronic Disease and Caregiving
Participants described joining the G4H program for a range of reasons. Some were motivated to take part in response to the loneliness they felt after life transitions. Others described their motivation being driven by recognizing the impact that health issues had in undermining their sense of social connection. At times, these issues appeared to overlap with experiences of distress and earlier trauma (i.e., prior to developing chronic illness), which was also intertwined with profound feelings of isolation and loneliness. For many, loneliness was not new nor solely attributable to chronic disease. Patricia (woman, aged 59) described: I’ve had a lot of trauma right through from childhood. The last thing that happened was my partner passed away four years ago. So, coming back from that was really difficult […]. Being part of the group has been really good. Meeting lots of people and making plans and actually acting on them to keep moving forward.
Several participants, including Phillip (man, aged 64), noted that caregiving added to their isolation and motivated them to engage in the program and focus on their own well-being: I lost my wife a year ago to cancer. And we’ve had a great life together. I nursed her in her last 12 months of life. To watch someone, die a little bit every day, it’s the hardest thing you could do. And when she did pass away […]. Had a cup of tea and sat there until the sun came up and it made me realize that no matter what happens, the world spins itself. Get off your arse and do something, you know?
Participants’ expectations and motivation to engage in the program seemed to be influenced by whether they joined the program through healthcare referral (i.e., due to self-reported loneliness or being identified as at risk after questionnaire completion) or voluntary self-referral. Some individuals, mostly those who joined the program through healthcare referral, felt stigmatized and expected a more passive, socially prescriptive approach that would simply connect them to new groups. They were surprised to find that the program required active engagement, reflection, and taking part in activities to develop their social connections. Steven (man, aged 50) noted, “I thought it would be more like helping you connect with groups rather than just talking about how to socialize.” In contrast, those who self-referred generally felt “privileged” (Alex, woman, aged 55; Phillip, man, aged 64; Patricia, woman, aged 59; Martin, man, aged 56; Margaret, woman, aged 67 Group 3) and special to be part of the program, highlighting how the type of referral can shape participants’ expectations, motivation, and readiness to engage.
Theme 2: Connectedness With Peers, Facilitators, and Content Promoted Engagement
Participants’ satisfaction with the program appeared to be shaped by its design, including program quality, structure, materials, and exercises, and a strong sense of connection and support within the G4H group. Facilitators’ expertise, enthusiasm, and guidance seemed to be key in enhancing participants’ experiences.
Subtheme 2.1: Reciprocity and In-Vivo Learning With the G4H Group
Participants discussed that engaging and connecting with others and their stories was a meaningful aspect of participation. The mutual support among peers was particularly stressed and seemed to offer strength, reassurance, and a sense of shared experience in their journeys through trauma and isolation: We are all “givers.” We see someone damaged and cause that hits here [places hand on chest], we reach out to that person to try and help them. We see that so much, so we reach out to so many [participant tears up]. And having that companionship from others, like myself, we relate. It’s like, our souls have known each other before. (Grace, woman, aged 58)
Sharing such deep emotions and personal experiences required a foundation of trust and respect, as highlighted by Alex’s (woman, aged 55) remarks about Patricia (woman, aged 59) in Group 3: “You’ve opened up a lot. You’re different from when you first came into the group. Even in the big group.” Patricia’s (woman, aged 59) response to this statement illustrated the importance of trust for this to happen: “Yeah, but that’s just because of trust.” For this trust to develop, some groups recognized the importance of establishing and agreeing on rules around confidentiality and setting boundaries: “Our boundaries are what we wanted the group to be like, keeping everybody’s confidentiality and what somebody says stays there. You know, there’s a whole list of them. And it was us that made those rules for the group” (Patricia, woman, aged 59).
Participants further emphasized the importance of group size, noting that smaller groups made them feel more connected, comfortable, and better able to support one another. Stephanie (woman, aged 68) described that the smaller G4H group (5–8 participants) compared to the larger group in the health service program contributed to perceived cohesion: “There wouldn’t be enough time [in the bigger group] for all the participants to contribute or ask. If it was too big of a group, I don’t think there would have been the cohesion.”
Two other factors we observed in participant interactions were the use of humor, highlighting the sense of trust in the group, and the motivation to engage and socialize fostered through their interactions. Brian (man, aged 51) shared how G4H boosted his drive to engage and build connections: Some people can definitely say the person I was when I first started is light years away from the person I am today. And it gave me motivation to do something to myself. […]. We’re out there doing things, sometimes we may not want to, but we’re there to support each other, and that’s the greatest take of the course.
Empathy seemed to be key to the trust and respect participants expressed and experienced. A sense of reciprocity seemed to emerge as they felt heard and listened to others, creating a dynamic of giving and taking. Alex (woman, aged 55) highlighted how genuine empathy fostered belonging beyond simple sympathy: There’s people here, there’s decent people. And they all have a story. And they all need to be heard. And you can relate to a lot of people […]. [You are] so lucky to learn more about a person you don’t know. There’s a lot of empathy here. Like we don’t want sympathy. But I think it’s nice to be heard sometimes.
Alongside empathy, openness to different attitudes, opinions, lifestyles, ways of being, and life experiences appeared to be key to building trust and respect. Alex (woman, aged 55) valued the group’s non-judgmental nature, contrasting it with past experiences: Not feeling like I was getting judged. Knowing that. I’ve been a pretty good reader of people’s faces. [It was the] first time in a long time that these people weren’t going to walk out and say to someone else or text someone else “She said such and such,” or “She’s got tattoos and piercings,” and all that sort of stuff. I didn’t feel that. […] I know if I had walked in and felt judged, I may not have come back.
The sense of connection among participants appeared to contribute to some organizing meet-ups outside of G4H, which continued after the program finished. Anna (woman, aged 65) described starting a swimming group: “For our last group, we’ve actually started our own ‘Misfits swimming club’. Nearly everybody in the [G4H] group plus a few others from my class. We’re still regularly doing three days a week at the pool. It’s great!”
Subtheme 2.2: Facilitators as Enablers of Meaningful Connection
Participants highlighted how facilitators created a welcoming environment that enhanced the successful delivery of G4H. For instance, Patricia (woman, aged 59) appreciated the efforts to make the room more private and comfortable, such as using background noise for privacy: “How it was closed off, how they divided the room, and then with the radio on to muffle, […] a privacy kind of thing. That was good. Made you feel more comfortable to share.” The safe, comfortable environment seemed to particularly support participants with social anxiety. Through additional conversations with participants, we discovered that facilitators also rotated seating weekly to encourage interaction and connection.
Facilitators’ ability to foster a genuine bond and connection with the G4H group was another success factor mentioned by participants. Facilitators’ positive and respectful approach allowed participants to feel valued, acknowledged, and comfortable: I thought [the facilitators] were absolutely fantastic. They’ve explained things. […] And I find them all very helpful, you’d always see them helping someone out […] and I found myself opening up. (Alex, woman, aged 55)
Beyond fostering a sense of community, facilitators support seemed to help participants navigate the program content and support them in building connections to others. Avery (woman, aged 71) described, “I found the provision of access to helpful resources and support from the facilitators very much appreciated, and they’ve guided me towards feeling more connected socially.”
The depth of facilitator support was also reflected in the enthusiasm and commitment that program participants described as part of their interactions: “Facilitators’ enthusiasm [laughs], the educational content that was provided, made me interested to learn a bit more, and made it very interesting” (Victoria, woman, aged 38).
Subtheme 2.3: Relatable, Practical, and Evidence-Based Content
Participants further praised the program quality, emphasizing its strong theoretical foundations as central to their satisfaction. Marilyn (woman, aged 73), with a health background, highlighted her appreciation for the program’s theoretical rigor: I like the workbook and the group discussions, but it was because I feel like it’s been well researched, well documented. The way it’s presented, that’s important for me and also it wasn’t wishy-washy and airy-fairy stuff. […] That evidence-base and the research and the way the book was constructed, I found that that could make sense to my brain.
In addition to the program quality, participants seemed to benefit from the program structure. Victoria (woman, aged 38) summarized, “I mean, it was, it was very well structured and enjoyable. I think they covered a lot of the information that [G4H] was designed to cover.”
Participants also noted that the program materials effectively supported their understanding of the theory and its application. In particular, the workbook was praised as a valuable resource, offering a wealth of visuals, information, and real-life examples that could be adapted to individual needs and used throughout as well as after the sessions: “I’ve still got the workbook and still look at it and appreciate it. Yes, I think it’s a fantastic resource” (Patricia, woman, aged 59).
Participants further perceived the reflection exercises as a strength of G4H. Theresa (woman, aged 55) stated how reflecting on her existing groups offered her valuable insights into which groups she genuinely benefitted from: The course actually made us all reflect, which is why a lot of us had to take time off to really absorb everything and get it. […] Because often you just go to groups and you go back, you don’t examine and really reflect on it. And so [it is] not until you actually do that, that you really find out what you are wanting, what isn’t working.
Theme 3: Experiential Impact: Engaging in Life Differently
Participants highlighted a range of life changes, including prioritizing self-care, joining new groups, and moving away from “toxic groups.” The program seemed to help them recognize the value of positive group connections, which prompted them to refine their social skills and strengthen their relationships with such groups. This sense of progress appeared to be largely intertwined with overcoming challenges participants faced while actively engaging in the program, such as realizing that they had limited social networks at the beginning. By stepping outside their social comfort zones, participants engaged with life differently.
Subtheme 3.1: Building Social Capability
One key insight shared by participants was the importance of group belonging for their overall well-being. Margaret (woman, aged 67) explained how she came to realize that social connectedness plays a crucial role in her well-being and happiness—a shift from her initial belief that exercise was the primary factor in promoting well-being: What I’ve learned is, it’s the social aspect of your life that makes you well. And the [physical] exercise is like the icing on the cake. The important part is that you’re not alone, that you’re in this with a whole lot of other people, and it’s that socialization.
In addition to becoming aware of the importance of groups for their health, participants noted improvements in their social skills. Some participants gained greater awareness and opportunities to enhance their social skills through the program. Riley (woman, aged 30) shared how she successfully applied these social skills in daily life: One of the things that was said in the program was smiling or saying something nice to someone randomly—the cashier at the check-out, the little weird interactions you have with people during the day, actually taking note of them. Something that I do a lot more now.
Applying social skills and stepping out of their comfort zones seemed to help participants build social confidence, making them feel more at ease in social situations. Dianna (woman, aged 55) reflected on how the G4H group supported her in recognizing her own value within social settings, while also learning not to pressure herself to fit into every group: I could understand that I have a value to the community somewhere. I may not have found my spot for where I’m supposed to be, yet, but knowing that I do have things that I can offer. It’s not the end if you walk into a group and it’s not for you. Whereas in the past, I would have felt like I failed and nobody wanted me around. Just coming to the understanding that not everything is for everybody.
Participants found that G4H helped them form meaningful social connections, which played a key role in their journey of learning self-care. For Victoria (woman, aged 38), G4H was instrumental in helping her build connections outside her family and reignited her interest in joining social groups: I made friends and then felt part of a group, felt like I was contributing to a group of socializing. Got to learn about people, meet new people […] Just having people to communicate with, because I live with my husband and daughter and I’ve moved to a new area, so I don’t have a lot of friendships. […] So being able to just have people to communicate with and socialize with has made me feel less lonely. […]
This experience of connecting seemed to inspire participants to empower others by sharing their G4H experiences. Alex (woman, aged 55) described her experience as gaining “tentacles”—a metaphor for expanding connections, which helped her build her own and assist others in forming meaningful relationships: It was like we were given tentacles, to reach out to the rest of the [Health and Wellness Clinic] group because we were benefiting from that. I think when you’re helping other people, you’re also helping yourself. […] I’m not alone, because I’m out there helping somebody.
Subtheme 3.2: Change Through Challenge
Many participants described some of the initial tasks of G4H, especially the mapping exercise, as somewhat confrontational, but at the same time stated that mapping groups and reflecting on their social networks was crucial for initiating change. Marilyn (woman, aged 73) explained how this process contributed to her readiness to alter aspects of her situation: It gave me a challenge that I had to think about, I had to go home and think about. You know you’re sitting here at home, are you really doing yourself a favor when you can see that? […] And when you first [understand], what groups are you connected with—It’s confronting. I remember the exact page [in the workbook] [group laughs]. It is because you get put in these life circumstances, and then that gets whittled off, […] and all of a sudden, you’re just down to this very narrow [social network]. I think it’s also about being ready inside, ready to receive that. It’s not just another course, it’s risen.
Complementary to Marilyn’s (woman, aged 73) reflection on the value of existing positive relationships, some participants came to the realization that some of their existing groups were rather toxic. This awareness of harmful relationships enabled participants to change these toxic relationships. Victoria (woman, aged 38), for example, became aware of the toxicity of her professional relationships, ultimately leading her to quit her job and seek a new one: This [mapping] exercise, this is actually the program, and the exercise made me realize that the job I was in, is something I should be letting go because it has very bad relationships with everything else in my life. And it was a real big realization […] and I would take a huge step in my career direction. A massive realization through the activity of mapping out groups.
Theme 4: Stigma, Social Anxiety, Content Accessibility, and Personal Context Can Reduce Engagement
In contrast to the elements that enriched participants’ experience, they also shared insights into barriers that could impede engagement with the program. These related to the program’s design, including its accessibility and clarity around the rationale for potential referrals that was associated with feelings of stigma for some. Other barriers that were discussed related to factors hindering program engagement, notably social anxiety, caregiving responsibilities, and work commitments. Drawing from their experiences with these barriers, participants provided suggestions for future adaptations.
Subtheme 4.1: Personal Barriers to Engagement Differed for Individuals
A significant challenge for participants in engaging with the program and implementing what they learned appeared to be related to their work commitments. Riley (woman, aged 30) shared that she had to take time off work to attend the program and found it harder to apply the knowledge and skills gained once she continued their job: I had taken 4-6 months off work to do this program. So, when the 6-month program ended, I went back to work and […] it changed the dynamic. When I didn’t work, I had time to do this, I had time to go see friends. I had time to do stuff. Now I don’t. Back to night shift.
Travel time and social anxiety were perceived to be additional significant personal challenges to program engagement, as experienced by Alex (woman, aged 55), for whom isolation and social anxiety made participation more difficult: Driving here frightens me. It’s so big like it takes me 25 minutes to get here each time. And that’s where my mind is going to say, “Is it worth the drive?” Yes, I adore these people, and I’d love to catch up. But I’m not someone that has people at my house because I feel very threatened by people in close proximity, in closed spaces.
In addition to these challenges, several participants had caregiving responsibilities, which led to missing sessions. Theresa (woman, aged 55) shared how caring for her children with disability initially posed a barrier, but she eventually recognized the importance of taking time for herself to participate: I’ve always said, “I can’t do this because I’ve got to stay home for my children.” But then I’m thinking, “hang on, I can actually go and do that.” They’re not going to miss me for an hour. Or I’ll make sure that they’re right. I could go and do my own thing. I don’t have to be constantly hovering to make sure that they’re going to be alive next hour. Well, if they are they’re not, I’ll deal with that then [group laughs].
In some instances, existing relationships with loved ones seemed to hinder program participation. Susan (woman, aged 79) expressed her disappointment in herself for allowing her partner to prevent them from fully engaging in the program: [I am] a little bit disappointed in myself […]. I felt so good two weeks ago, and I was so motivated but […] the way my husband is, he fights back, […] he does play with his mental health now and plays the victim a little bit.
Subtheme 4.2: Program Design and Entry Can Undermine Engagement
Despite the benefits of the program, there were aspects of its delivery that got in the way of fully engaging. Recruitment was a program-related barrier encountered by participants who were referred to the program by others (Groups 1 and 2) and experienced a sense of stigma surrounding the referral. This referral path also appeared to impact participants’ readiness to engage. Steven (man, aged 50) reflected on being chosen for the program based on others’ assumptions about his needs and suggested that self-referral might be a better option: I think we were chosen based on psychological and social factors. They went you know, “you need help.” […] Maybe the criteria for why people are suggested into the course need to be altered a bit. Do you feel that you suffer from social isolation? Do you feel alone? Because then that would be ideal. For us […] it wasn’t something we needed.
Another factor undermining program engagement seemed to be content accessibility, with the predominantly written materials being perceived as exclusionary by some individuals. For example, Susan (woman, aged 79) disclosed to the G4H group during the FGD that she was dyslexic and faced challenges with tasks related to workbook and mapping exercise: I was overwhelmed today. Like Marilyn (woman, aged 73), I can’t do notes or put the pen to paper. So, all the things around the wall and that mapping today… I can’t do, I can’t read a question and relate it. […] I just know that putting ink to paper was so hard for me. As soon as I got the folder [workbook], there’s not much in there. There’s not much that makes sense to me. I’m more visual. It’s like they’re using a different language for me. […] They had examples. But I think if they had more, then I could say, “oh yeah, that one works,” “oh yeah, that I could work with,” you know, because it wasn’t coming up for myself. It’s like, someone gave me Chinese and expected me to have Chinese answers.
Stephanie (woman, aged 68) suggested implementing a buddy system in future program iterations, where participants would be paired with another group member to provide mutual support in working through the content: I would have loved someone to help me. Maybe if there was a buddy system. So, in our own time, we actually set just one thing at a time. That would have helped me, because I just go home to dogs and nothing else, and I don’t look at it because I can’t think about it. But if someone’s talked about it, it might have made it “Oh, you mean such and such,” “Oh, fair enough.” So just a clarification […] because the next time you go to class, you’re just going to get another hurricane. It’s going to hit you.
Furthermore, participants wished for greater program accessibility for other participants of their health clinic, who were not participating in G4H. Stephanie (woman, aged 68) summarized, “I think it should have been offered to every participant [of the health clinic]. It should be part of the general program. […] It would have benefited them as well.”
Participants also suggested to extend both the overall program duration and session duration. Riley (woman, aged 30) expressed that five sessions were insufficient to build connections with others and fully process the content: “I don’t think the five weeks were quite long enough. […] The five weeks to me, is only 5 hours overall. And you got to make a connection in five hours, it’s like, yeah [laughs].”
Discussion
This study explored the acceptability of the G4H intervention and factors that facilitated and hindered its delivery among individuals with chronic disease. Participants were motivated to join G4H due to past trauma, their current life stage, the type of referral, and the isolation that often accompanies chronic disease. The program’s experiential impact was reflected in participants engaging with life differently, overcoming personal challenges, and gaining a deeper understanding of the importance of group belonging, improving social skills, and feeling empowered to connect with other social groups.
These findings align with earlier research (Cruwys, Haslam, Haslam, et al., 2022; Cruwys et al., 2023), which highlights the role of G4H groups as critical spaces for practicing social skills, receiving support, and experiencing the benefits of group dynamics. However, certain factors appeared to be particularly important for participants with chronic disease. Their engagement with the G4H group, along with the trust, respect, and mutual support fostered within it, played a key role in encouraging socialization and self-expression. Likewise, the bonds formed with facilitators and the guidance they provided were essential in creating a safe and supportive environment—especially for individuals with histories of trauma or social anxiety. The development of social capabilities through the program, participants’ strong identification with their G4H group, and the process of forming new, healthier social connections while distancing from toxic ones have all been shown to protect health and well-being in prior studies—particularly among vulnerable populations facing past trauma, social disadvantage, or illness (C. Haslam et al., 2008, 2019; Walter et al., 2016). For individuals in these circumstances, the empowerment to manage loneliness themselves expands the range of health-related interventions they can access and benefit from, particularly since many of these interventions are offered in group settings. This highlights the critical role of G4H in supporting individuals with chronic disease by fostering meaningful social connections to enhance the effectiveness and outcomes of the interventions provided.
Participants also described factors undermining their engagement in G4H, including personal challenges such as social anxiety, time commitments, or a lack of readiness to participate, as well as program-related challenges such as recruitment, content and program accessibility, and program and session duration. Notably, even participants who faced these challenges reported gaining value from the program. Given the study population’s heightened social and mental health challenges, these findings align with prior evidence suggesting that G4H may be particularly impactful for individuals experiencing greater social isolation and higher levels of social anxiety (Cruwys et al., 2023). An explanation might be that those individuals, who experience greater loneliness, are more motivated and engaged in their treatment process (Cruwys et al., 2023).
Implications for Program Delivery to Individuals With Chronic Disease
There are a number of implications of these research findings for practice, and two are central. The first relates to the inclusion of G4H in service provision for people living with chronic disease. This inclusion is crucial as it not only addresses the physical health needs of individuals with chronic disease but also their psychological resources and social well-being (C. Haslam et al., 2018). Furthermore, it can enhance the effectiveness of other interventions, as individuals who are socially connected and supported are more likely to engage in and benefit from additional treatments or therapies. By integrating G4H into the care for people with chronic disease, opportunities for peer support, social connection, and shared learning are created, all of which are key factors in improving quality of life. This approach aligns with the growing emphasis on patient-centered care, which focuses on promoting overall well-being rather than simply treating symptoms (Hudon et al., 2012).
The second implication concerns best practices in program delivery for individuals with chronic disease, requiring multiple potential improvements. First, it may be worthwhile to introduce G4H on a self-referral basis to enhance participants’ motivation, readiness, openness, and willingness to engage in the program. The program could also benefit from providing more background on the active nature of G4H to manage participants’ expectations and incorporating a motivational interviewing session at the start of Module 1 to improve readiness and reduce discomfort during the mapping exercise in Module 2 (see Figure 1). Facilitators should emphasize that there is no “right or wrong” number of groups when introducing the exercise to prevent feelings of guilt or failure, which might be particularly relevant for vulnerable populations.
Second, to enhance accessibility, content and materials should be tailored to participants’ specific needs. Conducting a pre-program needs assessment could help create more personalized materials. Introducing learning hubs or buddy systems, including program alumni, could support both participants and facilitators in understanding and improving the program. Peer exchanges among facilitators would also support program improvement and success, leveraging their experience and fostering ongoing learning.
Third, extended program sessions of 1.5 hours could accommodate the emotional and physical vulnerabilities of participants with chronic disease while allowing for diverse learning styles. Finally, a sixth module, serving as a booster, could be introduced approximately three months after completion to reconnect, troubleshoot, and support ongoing strategy use. Alumni programs might also help participants stay connected and continue practicing social skills after program completion. These program delivery ideas require more detail regarding their implementation and evaluation. As our findings are preliminary in nature, further research is needed to confirm or challenge our observations and refine effective approaches to program delivery.
Limitations
Our sample predominantly included older White adult women in regional Australia with chronic diseases, mental health challenges, and high levels of social isolation. While our findings support the acceptability and feasibility of G4H in this demographic, caution is needed when considering the transferability of our findings to other populations. The program is suitable for adaptation to meet the unique needs of diverse groups, which could include consideration of factors associated with health condition, age, gender, and cultural background. Consideration of such factors will inform and enhance program applicability. Additionally, participants provided predominantly positive feedback, with few neutral or negative comments. This imbalance reflects genuine participant experiences but may also limit the range of perspectives captured and contribute to an overall positive interpretation of findings. It is also possible that individuals who had neutral or negative experiences chose not to participate in the study, which could have further reduced the diversity of viewpoints represented in the study. Furthermore, it is important to note that the time between receiving the program and participating in the study varied across cohorts, which may have affected participants’ ability to recall details accurately.
Conclusion
Findings from this study suggest that the G4H program is acceptable for participants with chronic disease and provides a meaningful learning experience to support them in managing loneliness. While facilitator expertise and the dynamics of the G4H groups played key roles in participants’ positive experience, the program’s core value appears to lie in equipping participants with the tools to recognize and manage loneliness independently. G4H empowers participants to understand the triggers and patterns of loneliness in their lives, fostering a sense of control and resilience. This approach moves beyond temporary relief, enabling the development of lasting strategies that participants can apply outside of the group setting, thereby enhancing social well-being and overall quality of life.
Supplemental Material
Supplemental Material - “It’s the Social Aspect of Your Life That Makes You Well”—Acceptability of the GROUPS 4 HEALTH (G4H) Program for Participants With Chronic Disease
Supplemental Material for “It’s the Social Aspect of Your Life That Makes You Well”—Acceptability of the GROUPS 4 HEALTH (G4H) Program for Participants With Chronic Disease by V. Vanessa Wergin, Nathalia Costa, Linda Nguyen, Maryanne Long, Stephen Woodruffe, Adam Hulme, Crystal J. La Rue, and Catherine Haslam in Qualitative Health Research
Footnotes
Ethical Considerations
This study received ethical approval from The University of Queensland’s Human Research Ethics Committee (2023/HE002390).
Consent to Participate
All participants provided written informed consent.
Author Contributions
CH, ML, SW, AH, NC, and CLR contributed to the conception and design of the study. VW and LN collected the data. VW and NC performed data analysis with CLR, LN, ML, AH, and CH being involved in the reflexive sessions. VW wrote the first draft of the manuscript. CH and NC wrote sections of the manuscript. All authors contributed to manuscript revision, and read and approved the submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: GROWTH is supported by The University of Queensland strategic funding initiative—Health Research Accelerator (2021–2028). The support provided through HERA has been crucial in enabling key research capability to successfully develop and execute the GROWTH vision and mission. Adam Hulme’s contribution to this work was supported by an Australian Research Council DECRA Fellowship: DE240100095.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Catherine Haslam is one of the developers of G
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.