
Abstract
Background:
Meatoplasty is a surgical procedure that is used to treat chronic ear conditions such as chronic otitis media, cholesteatoma, and external auditory canal stenosis. Despite its widespread use, there is a lack of comprehensive analysis of the effectiveness of different meatoplasty approaches and their long-term outcomes. This systematic review aims to systematically analyze the existing studies to evaluate the effectiveness of meatoplasty and its approaches with a focus on surgical outcomes, postoperative complications, and patient satisfaction across diverse surgical approaches and patient demographics.
Methods:
The searches from databases like PubMed and Google Scholar for studies on meatoplasty in chronic ear surgeries from 2010 to 2024. Seventeen studies were selected based on predefined inclusion criteria, focusing on success rates, complications, and long-term outcomes. Data were extracted on patient demographics, surgical techniques, and outcomes, and the quality of evidence was assessed using the Newcastle Ottawa Scaleand the Cochrane risk of bias assessment tool.
Results:
The analysis of the included studies revealed diverse patient populations and varying meatoplasty approaches for treating chronic ear conditions. Most studies reported positive outcomes, with significant improvements in ear dryness, hearing, and symptom relief. Postoperative complications, such as meatal stenosis and granulation tissue, were rare and manageable, while the long-term follow-up was crucial for preventing restenosis. However, meatoplasty proved effective in restoring ear canal function, with both one-cut and Z-plasty techniques showing favorable results.
Conclusion:
Advancements in meatoplasty and related surgical techniques have shown great success in managing chronic ear conditions, alleviating symptoms, enhancing hearing, and improving overall quality of life. Their effectiveness is evident in high graft success rates and low complication rates, with innovative approaches and careful postoperative care effectively managing rare issues like stenosis, ensuring favorable long-term results.
Keywords
Introduction
Meatoplasty is a surgical technique designed to enlarge the external auditory canal (EAC) and facilitate the formation of a skin flap for neocavity epithelialization. It plays a critical role in open-cavity tympanomastoidectomy procedures and surgeries involving stenosis of the EAC. 1 Often performed as an adjunctive phase, meatoplasty is incorporated into canalplasties, tympanoplasties, and various other otoneurological surgeries. The reconstruction of the new meatus involves manipulation of skin, cartilage, subcutaneous tissue, and bone. The specific surgical planes are determined by the underlying pathology, the primary procedure being performed, and the required diameter of the external opening. Conditions commonly necessitating meatoplasty include suppurative chronic otitis media (COM), cholesteatomatous COM, congenital or acquired EAC stenosis, refractory infections, traumatic damage, neoplastic growths, and iatrogenic injuries.2,3
Meatoplasty plays a vital role in the functional restoration of the ear and enhances the effectiveness of open-cavity procedures, making it a cost-effective option for the management of cholesteatomas. 4 A sufficiently wide meatal opening ensures easy access to the auditory canal, tympanic membrane, and open neocavities, while also reducing the need for intensive postoperative care.5–7 Based on clinical experience, open-cavity tympanomastoidectomy combined with meatoplasty is recommended for cholesteatoma treatment, as it provides functional outcomes comparable to those achieved with closed techniques.8,9 Moreover, maintaining proper ventilation of the ear canal or cavity—facilitated by meatoplasty—is essential for preventing otorrhea, particularly in tropical climates where activities like swimming are common and may increase the risk of epithelial desquamation, granulation tissue formation, and fungal infections.10,11
Although functional rehabilitation through meatoplasty offers significant advantages, long-term follow-up is crucial to prevent postoperative complications. Infections, particularly otorrhea, can occur.12,13 Postoperative infections may occur within the reconstructed open cavity—which includes the EAC, attic, and mastoid in canal wall down (CWD) procedures. These infections are better described as postoperative cavity infections rather than acute mastoiditis, given the loss of anatomical separation. Therefore, regular follow-up and patient education on preventing infections and maintaining clean ear canals are essential for achieving the final goals of hearing loss care. However, in some cases, other procedures may be necessary to combat recurring issues, such as canal restenosis or persistent otorrhea,14,15 it is essential to provide comprehensive care and patient education to ensure successful outcomes.
While meatoplasty is commonly used in chronic ear surgeries, there is a lack of knowledge about the success, failure, and complication rates, based on various approaches of meatoplasty. Previous studies have focused on the benefits of open-cavity tympanomastoidectomy and the significance of adequate ventilation, but a few comparative studies were published in assessing the outcomes of meatoplasty in the prevention of chronic ear conditions. Meatoplasty is most commonly indicated in chronic inflammatory ear conditions, particularly chronic suppurative otitis media (CSOM) and cholesteatoma. Although it is also performed in cases of acquired EAC stenosis, trauma, or congenital anomalies, these are only considered in this review when the indication overlaps with chronic disease or functional impairment requiring long-term canal patency and drainage. Thus, the purpose of this systematic review is to determine the outcomes, success rates, and complication profiles associated with different meatoplasty techniques when performed alone or as an adjunct to tympanoplasty, canaloplasty, and mastoidectomy in chronic ear surgeries and to identify effective management approaches to enhance long-term results.
Methodology
Search study
To execute this systematic review and literature search, the most recent articles and abstracts that are accessible through paid databases, based on the success rates of meatoplasty, were considered prioritized using Google Scholar, PubMed, and Science Direct. The terms were carefully selected from the 2010 to 2024 studies in the literature search to obtain comprehensive results. These keywords include “Meatoplasty” AND “chronic ear surgeries,” “Meatoplasty” AND “tympanomastoidectomy” AND “COM,” “Meatoplasty success” OR “success rates of meatoplasty” AND “chronic ear surgeries,” AND “postoperative complications” OR “otorrhea,” “Meatoplasty” AND “canal stenosis” OR “long-term outcomes,” and “Open-cavity tympanomastoidectomy” AND “cholesteatoma.”
Selection criteria
The studies that focused on patients who underwent various types of chronic ear surgeries, including tympanomastoidectomy, canaloplasty, modified radical mastoidectomy, ossiculoplasty, cochlear implantation, and other otoneurological procedures requiring meatoplasty were selected. Studies were assessed based on the following predefined inclusion and exclusion criteria to ensure the relevance and quality of the evidence.
Inclusion criteria
Only full-text articles published in peer-reviewed journals between 2010 and 2024 were included in this review. Clinical studies, clinical trials, observational studies (cohort and cross-sectional), and randomized controlled trials (RCTs) were eligible for inclusion. Studies were included to determine whether they reported success rates of meatoplasty, postoperative complications (e.g., otorrhea, infections), long-term outcomes, functional recovery, or prevention of canal stenosis. Only cases where meatoplasty was performed in the context of chronic disease management (e.g., CSOM, cholesteatoma, acquired EAC stenosis with recurrent otorrhea) were included. Studies with mixed etiologies, such as congenital and acquired were eligible if: (i) outcome data for the chronic disease subgroup were reported or could be extracted; or (ii) the cohort explicitly included chronic disease-related cases even if not stratified.
Exclusion criteria
Articles published in languages other than English were excluded to avoid translation errors and ensure accurate data interpretation. Studies with abstracts or full texts containing unclear or ambiguous information regarding key outcomes, such as success rates or complications related to meatoplasty were also excluded. Non-clinical studies, including animal studies, in vitro research, or laboratory-based investigations, were deemed ineligible. Furthermore, articles that were not peer-reviewed, unpublished, or presented as conference abstracts with insufficient detail were excluded. Studies focused on canaloplasty for congenital anomalies unrelated to chronic ear disease or procedures in other specialties (e.g., ophthalmology, urology) were excluded. Additionally, articles that did not address chronic ear conditions requiring meatoplasty, such as non-chronic ear infections or cosmetic ear surgeries, were not considered.
Data extraction
The data for this systematic review were extracted from peer-reviewed articles published between 2010 and 2024. The primary data included findings on the success rates of meatoplasty in chronic ear surgeries, complications associated with different approaches, and surgical outcomes such as postoperative hearing improvement, canal stenosis prevention, and infection control. Key data points extracted were sample size, demographic details (e.g., gender distribution, age range), underlying conditions, preoperative symptoms, surgical interventions performed, follow-up durations, and postoperative outcomes. Relevant statistical data, including complication rates, success percentages, and long-term maintenance requirements were also documented.
To enhance the consistency and comparability of data across the included studies, key clinical outcomes were operationally defined for this review. This approach allowed for the standardized evaluation of surgical success and complications, given the variability in reporting across the literature. Surgical success was defined using a combination of objective and subjective measures. Specifically, success was considered present if one or more of the following criteria were met: (1) achievement of a dry ear, characterized by the absence of persistent otorrhea or discharge during the postoperative follow-up period; (2) maintenance of meatal patency, reflected by an adequately sized and epithelialized EAC with no evidence of restenosis; (3) hearing improvement, particularly a measurable reduction in the air-bone gap (ABG), with an ABG closure of ⩽20 dB considered clinically significant; (4) graft success, indicated by an intact tympanic membrane graft without perforation or medialization; and (5) patient-reported satisfaction, including improved comfort, cosmetic outcomes, and facilitation of hearing aid use, where applicable. Postoperative complications were categorized as minor or major based on their severity and the need for further intervention. Minor complications included granulation tissue formation, transient otorrhea, mild hyperemia, and temporary cosmetic deformities such as a cupped ear. These were typically self-limiting or manageable with conservative measures. Major complications, in contrast, involved more significant adverse outcomes such as meatal stenosis requiring surgical revision, persistent infection or discharge unresponsive to medical therapy, flap necrosis, and cholesteatoma recurrence. The need for revision meatoplasty or additional reconstructive procedures was also considered a major complication.
Quality assessment
We use the Newcastle-Ottawa Scale 16 to assess the quality of non-randomized studies, as it evaluates key domains such as selection, comparability, and exposure/outcome to determine the risk of bias. For RCTs, we apply the Cochrane Risk of Bias assessment 17 to evaluate the reliability of the studies by examining factors like random sequence generation, allocation concealment, blinding, and handling of incomplete data.
Results
The 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines were employed to identify, screen, assess, and include studies for this systematic review on the success rates of meatoplasty approaches in chronic ear surgeries (Supplemental Table 1). 18
Search results
The systematic search identified a total of 1450 records. After duplicate removal (n = 401) and automation-assisted exclusion of irrelevant records (n = 168), 881 records were screened for eligibility. Of these, 367 articles were excluded due to being older than 14 years, written in languages other than English, or irrelevant to the scope of the study. A total of 514 studies were assessed for eligibility, of which 497 were excluded due to incomplete data or a non-clinical nature. Ultimately, 17 studies meeting the inclusion criteria were included in this review (Figure 1).

PRISMA flow chart for article selection.
The demographic characteristics of the included studies
The reviewed studies explore a range of surgical and conservative treatments for conditions impacting the EAC and middle ear. These conditions include COM, congenital and acquired EAC stenosis or atresia, cholesteatoma, and related disorders. Patient ages range from young children to older adults, with follow-up durations extending from weeks to several years. Surgical interventions frequently discussed include various types of meatoplasty, tympanoplasty, mastoidectomy, and canaloplasty, each tailored to the specific condition being treated. When described, conservative treatments often involve antibiotics, corticosteroids, and aural toileting. The outcomes and follow-up data emphasize the long-term effectiveness of these treatments, with an analysis of surgical techniques, gender distributions, and patient outcomes based on underlying conditions.
The included studies comprised 1 RCT, and 16 prospective/retrospective studies accounted for the majority (93.8%). This predominance reflects the observational nature of research in this field. Collectively, the studies included a total sample size of 824 patients, illustrating a broad range of patient demographics and surgical methodologies (see Table 1).
The demographic characteristics of included studies.

The main findings of the included studies
Preoperative symptoms
Preoperative symptoms commonly reported across studies include chronic ear discharge, highlighted by Zafar and Kumar, 21 Diarra et al. 31 and Sonvane et al. 33 Hearing loss was a predominant symptom noted by Hovis et al. 5 Abdulrahman, 23 Fu et al. 24 Carnevale et al. 25 Guo et al. 26 Mantsopoulos et al. 27 Kara et al. 28 Suker et al. 30 Diarra et al. 31 Stultiens et al. 32 and Sonvane et al. 33 Otalgia was reported by Abdulrahman, 23 Suker et al. 30 and Sonvane et al. 33 while cholesteatoma was noted by Zafar and Kumar, 21 Gumban and Almazan, 22 and Kara et al. 28 EAC stenosis was highlighted by Chen and Zang, 19 Fu et al. 24 Mantsopoulos et al. 27 and Nagaoka et al. 29 Tympanic membrane perforation was specifically reported by Chen et al. 20 Additionally, severe complications, including abscesses and meningitis, were described by Gumban and Almazan 22 (Table 2).
The main findings of the included studies.
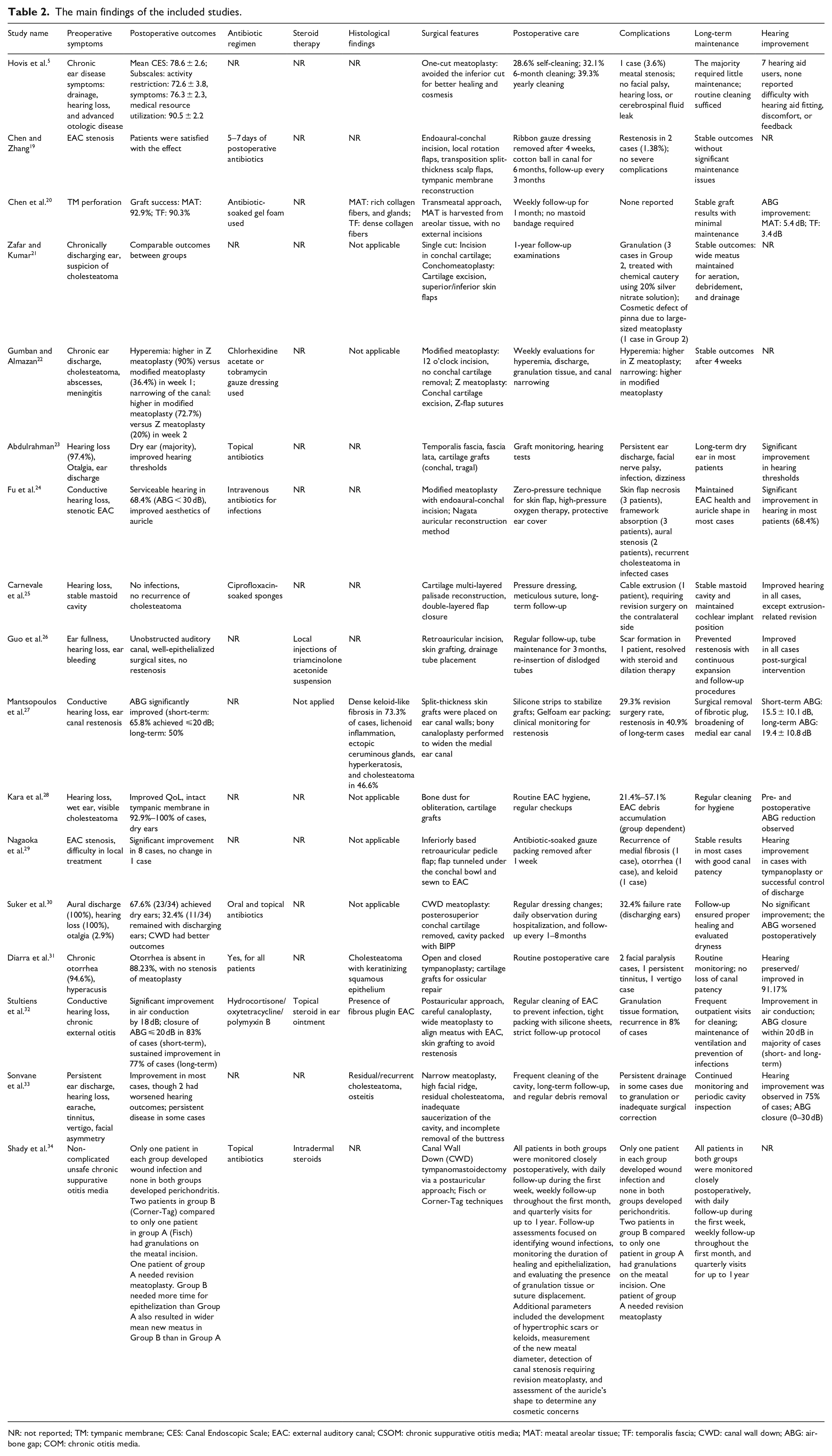
NR: not reported; TM: tympanic membrane; CES: Canal Endoscopic Scale; EAC: external auditory canal; CSOM: chronic suppurative otitis media; MAT: meatal areolar tissue; TF: temporalis fascia; CWD: canal wall down; ABG: air-bone gap; COM: chronic otitis media.
Postoperative outcomes and complications
Postoperative outcomes were generally positive, with the majority of patients experiencing significant improvement in hearing thresholds, dry ear status, and symptom resolution. Significant hearing improvements were reported in multiple studies, such as Abdulrahman 23 observed improved thresholds, and Stultiens et al. 32 noted an 18 dB air conduction improvement with ABG closure ⩽20 dB in 83% of cases (short-term). Fu et al. 24 highlighted serviceable hearing (ABG < 30 dB) in 68.4% of patients. These findings underscore the efficacy of surgical interventions in restoring functional hearing.
The majority of studies highlighted the achievement of dry ears as a key outcome, with Abdulrahman 23 and Suker et al. 30 reporting dry ears in 67.6% of patients. Furthermore, Diarra et al. 31 emphasized the absence of otorrhea in 88.23% of cases. Similarly, Kara et al. 28 reported intact tympanic membranes in 92.9%–100% of cases, accompanied by dry ears and improved QOL. These results reflect the success of surgical procedures in improving both physical and QOL outcomes for patients.
Additionally, high graft success rates, as reported by Chen et al. 20 (meatal areolar tissue (MAT): 92.9%; TF: 90.3%), and Fu et al. 24 noted improvements in auricle aesthetics. Surgical sites were well epithelialized with no restenosis in Guo et al. 26 although Mantsopoulos et al. 27 observed restenosis in 29.3% of cases. Minimal surgical complications were reported overall, with Carnevale et al. 25 noting no infections or cholesteatoma recurrence, and Zafar and Kumar 21 reported no perichondritis or stenosis, despite a few cases of granulation or cosmetic defects.
Hovis et al. 5 reported that meatal stenosis occurred in 3.6% of cases, while no cases of facial nerve palsy or cerebrospinal fluid leaks. Granulation tissue formation was noted in a few studies, 21 where patients required chemical cautery to manage the issue. These complications were generally manageable and did not significantly affect the overall success of the surgery. Moreover, the incidence of severe complications like hearing loss or infections was low. Together, these results suggest the overall safety and effectiveness of surgical approaches, with limited complications and substantial patient benefit (Table 2).
Histological findings and surgical features
The studies reported a range of histological findings relevant to ear conditions and surgical interventions. Chen et al. 20 observed rich collagen fibers and glandular structures in MAT grafts and dense collagen fibers in TF grafts, highlighting material-specific differences. Mantsopoulos et al. 27 identified dense keloid-like fibrosis in 73.3% of cases, along with lichenoid inflammation, Dense keloid-like fibrosis in 73.3% of cases, along with lichenoid inflammation, ectopic ceruminous glands, hyperkeratosis, and cholesteatoma in 46.6%. Diarra et al. 31 described cholesteatoma with keratinizing squamous epithelium, while Sonvane et al. 33 reported residual or recurrent cholesteatoma and osteitis in cases with narrow meatoplasty. Additionally, observations included fibrous plugs in the EAC. 32
The surgical techniques employed varied significantly based on clinical needs and case complexity. Hovis et al. 5 reported improved healing and cosmesis with a one-cut meatoplasty that avoided inferior cuts. Gumban and Almazan 22 compared modified meatoplasty using a noon incision (a 12 o’clock endaural incision without removal of conchal cartilage and allowing healing by secondary intention) to Z Meatoplasty, where cartilage excision and Z-flap sutures were employed. Chen and Zang 19 utilized endoaural incisions, local rotation flaps, and transposition split-thickness scalp flaps for complex reconstructions. Chen et al. 20 noted a transmeatal approach using areolar tissue grafts, avoiding external incisions entirely.
Several studies highlighted innovative techniques to prevent complications. Mantsopoulos et al. 27 performed bony canaloplasty with split-thickness skin grafts to widen the medial ear canal. Stultiens et al. 32 reported the postauricular approaches and skin grafting to prevent restenosis. Suker et al. 30 described the CWD approach with cartilage removal and cavity packing using BIPP. Fu et al. 24 utilized Nagata auricular reconstruction method, while Carnevale et al. 25 achieved success with cartilage multi-layered palisade reconstruction and double-layered flap closure. Retroauricular pedicle flap, 29 temporal fascia and cartilage grafts, 23 and Bone dust for obliteration, cartilage grafts 28 were also noted as effective approaches. However, inadequate saucerization and high facial ridges were associated with residual disease in some cases (Table 2). 33
Comparative effectiveness of meatoplasty approaches
Comparative studies evaluated different meatoplasty techniques and found that modified meatoplasty and Z-meatoplasty generally provided similar outcomes in terms of surgical success. Hovis et al. 5 documented varying cleaning schedules: 28.6% of patients had no cleaning, while others required cleaning every 6 months or yearly. Chen et al. 20 implemented weekly follow-ups for the first month, and Fu et al. 24 utilized a zero-pressure technique along with protective ear covers and high-pressure oxygen therapy. Regular dressing changes and close follow-up were emphasized in studies like Suker et al. 30 with Mantsopoulos et al. 27 opting for silicone strips and Gelfoam packing for graft stabilization. Gumban and Almazan 22 conducted weekly evaluations to monitor for complications such as hyperemia, discharge, and canal narrowing. Additionally, Guo et al. 26 recommended tube maintenance for up to 3 months to prevent restenosis, underlying the importance of routine evaluations across studies.
The retrospective comparative study by Shady et al. 34 evaluated the outcomes of two different meatoplasty techniques—classic “Fisch” and “Corner-Tag”—performed after CWD tympanomastoidectomy in 48 patients with unsafe CSOM. Patients were evenly divided into two groups: Group A underwent the Fisch technique, and Group B the Corner-Tag technique. All surgeries were performed at Benha University Hospitals between 2021 and 2023. Both techniques had comparable rates of postoperative complications, including wound infection, granulation tissue, hypertrophic scarring, and canal stenosis. Only one patient (4.2%) in the Fisch group required revision surgery. The Corner-Tag technique resulted in a significantly wider meatal diameter after 1 year (10.50 ± 1.02 mm) compared to the Fisch group (9.63 ± 1.41 mm, p = 0.02), although it also required a longer time for epithelialization and healing (7.33 ± 0.96 weeks vs 6.5 ± 0.88 weeks, p = 0.003). Minor cosmetic deformities (cupped ear) were seen temporarily in 16.6% of Corner-Tag patients but resolved within 3 months. No long-term cosmetic issues were noted in either group. In conclusion, both techniques were effective and safe, but the Corner-Tag technique offered a better long-term canal diameter at the cost of slightly slower healing. The authors recommend further research with larger sample sizes and longer follow-up durations to validate these findings (Table 2).
Long-term maintenance
Long-term outcomes consistently showed stable results with minimal maintenance in most cases. Zafar and Kumar 21 reported that a wide meatus was maintained, allowing for effective aeration, debridement, and drainage. Gumban and Almazan 22 also found stable outcomes 4 weeks postoperatively. Carnevale et al. 25 ensured the stability of the mastoid cavity and cochlear implant positioning, while Nagaoka et al. 29 observed good canal patency with the use of antibiotic-soaked gauze packing. Stultiens et al. 32 highlighted the importance of routine cleaning to ensure patient EACs and ventilation. Long-term dryness and ear health were maintained in studies by Abdulrahman 23 and Fu et al. 24 with the routine follow-up being emphasized in all cases (Table 2).
Patient-reported outcomes and quality of life
Patient-reported outcomes were largely positive, with many studies reporting significant improvements in QoL following surgery. Hovis et al. 5 found that their technique facilitated hearing aid fitting. Chen et al. 20 reported an ABG improvement of 5.4 dB for MAT grafts and 3.4 dB for TF grafts. Mantsopoulos et al. 27 reported a significant short-term ABG improvement (15.5 ± 10.1 dB) and long-term improvement (19.4 ± 10.8 dB). Abdulrahman 23 and Fu et al. (2020) observed significant improvements in hearing thresholds, with Fu et al. 24 noting a 68.4% success rate. Diarra et al. 31 found that hearing was improved in 91.17% of cases. Stultiens et al. 32 noted a significant closure of the ABG within 20 dB in most cases. However, Suker et al. 30 reported a worsening of the ABG postoperatively in their cohort, indicating variability in outcomes (Table 2).
Comparative analysis between different meatoplasty techniques
Table 3 outlines the various meatoplasty techniques identified in the reviewed studies, categorizing them by their key procedural characteristics and primary references. Each approach—such as one-cut, Z-meatoplasty, modified techniques, and more advanced reconstructive methods like retroauricular flaps or bony canaloplasty—is defined by its incision design, tissue manipulation, and reconstructive goals. The diversity of approaches demonstrates the adaptability of meatoplasty based on underlying pathology (e.g., cholesteatoma, congenital stenosis) and the desired postoperative anatomy. These variations reflect both the evolution of surgical innovation and the importance of tailoring the technique to each patient’s anatomical and clinical needs.
Comparison between different techniques.
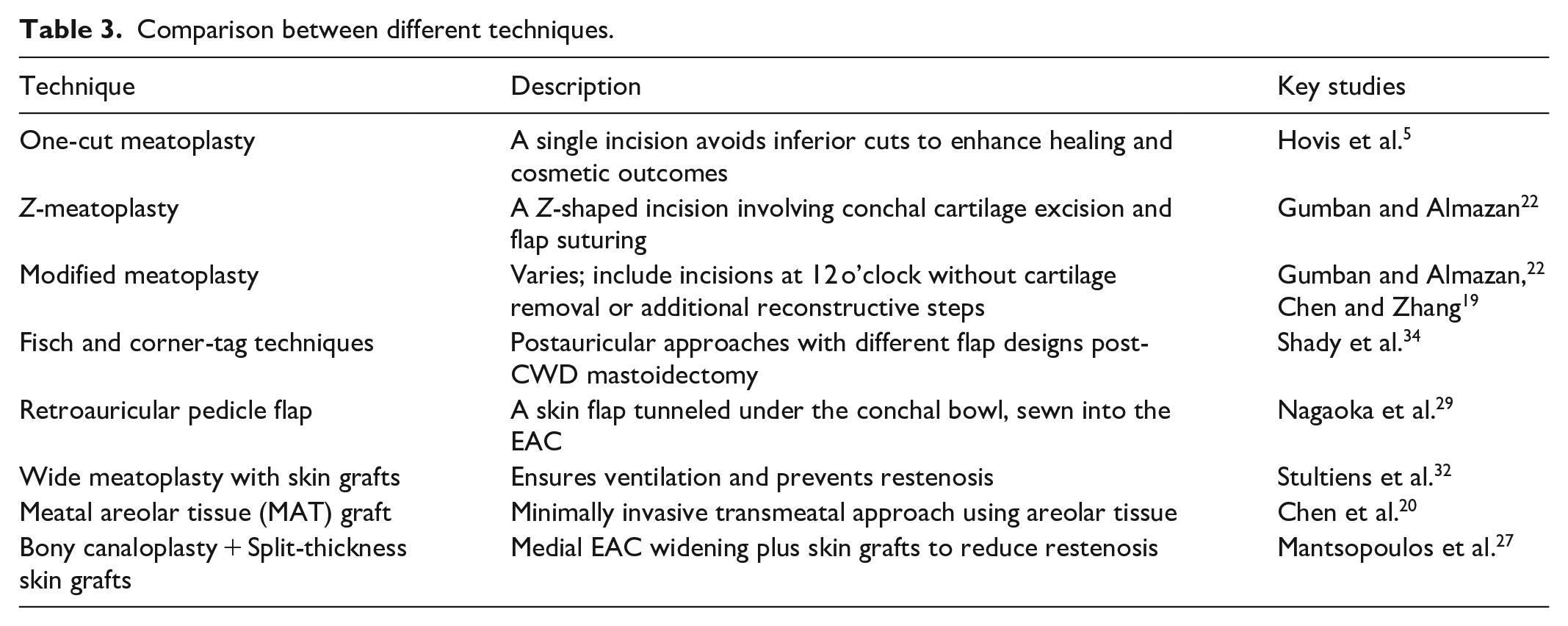
Table 4 compares the main outcomes and characteristics of the different meatoplasty techniques, including healing time, cosmesis, complications, and long-term effectiveness. The one-cut and modified techniques showed excellent healing and cosmetic results, while more complex approaches like the Corner-Tag or Z-meatoplasty offered improved canal patency at the cost of slower healing or transient cosmetic effects. Restenosis was more commonly associated with procedures requiring extensive canal manipulation, such as bony canaloplasty. Importantly, patient satisfaction was generally high across all techniques, highlighting that with appropriate technique selection and follow-up care, favorable outcomes are achievable regardless of the surgical variation used.
Comparison between the outcomes of different meatoplasty techniques.

Qualitative descriptors (e.g., good, moderate, excellent) were assigned based on the terminology and outcome summaries used by the original study authors. Where numerical outcomes were provided (e.g., percentage of dry ears or ABG closure), interpretation was based on general clinical benchmarks. However, no standardized scoring tool was applied across studies, and heterogeneity in reporting is acknowledged.p values of <0.05 were considered statistically significant in bold.
Regarding functional outcomes, across the reviewed studies, functional outcomes following various meatoplasty techniques were largely positive, particularly in terms of hearing improvement and the achievement of a dry ear. All surgical approaches demonstrated improvements in the ABG, indicating enhanced auditory function postoperatively. Notably, the use of MAT grafts, as explored by Chen et al. 20 resulted in a mean ABG improvement of 5.4 dB, reflecting both graft integrity and functional efficacy. A comparative analysis of the Fisch and Corner-Tag techniques by Shady et al. 34 showed comparable hearing restoration between the two; however, the Corner-Tag approach yielded a wider postoperative meatal diameter, which may facilitate better canal aeration and hygiene. Stultiens et al. 32 further corroborated the success of meatoplasty in hearing outcomes, with 83% of patients achieving an ABG closure within 20 dB in the short term—demonstrating significant auditory gain in a majority of cases. Dry ear status—another vital outcome in chronic ear surgery—was consistently achieved across the techniques, with multiple studies reporting high rates of postoperative dryness. Diarra et al. 31 found that otorrhea was absent in 88.23% of cases post-surgery, underscoring the procedure’s effectiveness in controlling chronic ear discharge. Similarly, Zafar and Kumar 21 observed sustained dry meatuses in patients over a full year of follow-up, reinforcing the long-term stability of meatoplasty outcomes. These results reflect the success of the procedure not only in anatomical correction but also in restoring critical physiological functions of the EAC.
Regarding the histological outcomes, the choice of graft material and surgical reconstruction technique plays a pivotal role in the success of meatoplasty, with distinct histological and structural features influencing outcomes. In comparative analyses of graft materials, MAT grafts were found to contain abundant glandular structures and rich collagen fibers, which are favorable for rapid and robust epithelialization of the ear canal. 20 In contrast, temporalis fascia (TF) grafts were characterized by dense collagen fibers but lacked glandular components, possibly affecting integration and surface moisture regulation. These tissue-specific histological differences suggest that MAT may offer a slight advantage in healing dynamics, especially in minimally invasive approaches. Advanced reconstructive strategies were applied in more complex cases, particularly those involving congenital anomalies or significant canal deficits. Fu et al. 24 utilized the Nagata auricular reconstruction method for patients with congenital aural stenosis, achieving both aesthetic and functional restoration of the external ear canal. Carnevale et al. 25 reported the use of a cartilage palisade technique combined with double-layered flap closure in patients undergoing cochlear implantation post-meatoplasty, ensuring long-term stability of both the neocanal and implant sites. These sophisticated reconstructive techniques highlight the adaptability of meatoplasty in managing a broad spectrum of anatomical and pathological presentations while reinforcing the importance of individualized surgical planning.
Table 5 summarizes the major advantages and limitations of each meatoplasty technique, assisting in clinical decision-making. Simpler techniques like the one-cut or modified approaches offer ease of performance and good cosmetic outcomes, but may fall short in severe stenosis cases. In contrast, techniques like the Corner-Tag and Z-meatoplasty provide superior canal enlargement but require greater surgical precision and longer healing periods. Understanding these trade-offs is vital for surgeons when selecting the most appropriate method based on individual patient factors, surgical goals, and expected complications.
Comparison between different techniques in advantages and limitations.

Quality assessment
The NOS evaluates study quality across Selection, Comparability, and Exposure/Outcome domains. High-quality studies (7 stars: Zafar and Kumar, 21 Fu et al., 24 Nagaoka et al., 29 8 stars: Shady et al., 34 ) demonstrate robust methods and reliable results. Moderate-quality studies (5–6 stars) show sound methodology but with some limitations, requiring cautious interpretation. Low-quality studies (3–4 stars) lack rigor and are less reliable. Overall, high-quality studies should guide conclusions, with moderate-quality studies providing context and low-quality studies treated as exploratory (Table 6).
NOS for non-randomized studies.

asterisks (*) indicate the number of scores awarded for meeting specific quality criteria (maximum 9 stars: Selection up to 4, Comparability up to 2, Outcome/Exposure up to 3).
The Cochrane Risk of Bias assessment for Gumban and Almazan 22 shows a low risk in key domains such as random sequence generation, allocation concealment, blinding of participants, and handling of incomplete data. However, unclear risks in outcome assessor blinding, selective reporting, and other potential biases highlight the need for cautious interpretation despite the study’s generally strong methodology (Table 7).
The Cochrane risk of bias assessment for RCTs.

Discussion
The review underscores significant advancements in meatoplasty techniques and related surgical approaches for treating chronic ear conditions. Procedures such as modified meatoplasty, Z-meatoplasty, CWD mastoidectomy, bony canaloplasty, and innovative reconstruction methods like cartilage multi-layered palisade techniques and Nagata auricular reconstruction have shown remarkable efficacy. These interventions address key symptoms, including chronic ear discharge, hearing loss, otalgia, cholesteatoma, and tympanic membrane perforation, while achieving notable postoperative outcomes such as improved hearing thresholds, dry ear status, and enhanced quality of life.
High graft success rates, stable long-term outcomes, and minimal complications were consistent across studies, with approaches such as transmeatal techniques, split-thickness skin grafting, and retroauricular pedicle flaps contributing to surgical success. Although complications like meatal stenosis, granulation tissue formation, and restenosis were occasionally observed, they were typically manageable through diligent postoperative care and innovative surgical strategies.
The findings highlight the critical role of tailored surgical methods, meticulous follow-up, and routine maintenance in ensuring enduring patient benefits. These advancements in meatoplasty and its associated approaches confirm their effectiveness in not only restoring ear function but also significantly enhancing the overall quality of life for patients with chronic ear conditions. These results align with previously published reports that represented the advantages of meatoplasty in restoring the patency of the ear canal and resolving chronic ear symptoms such as discharge, hearing loss, and pain.13,21,32 It is important to interpret the outcomes of meatoplasty in light of the underlying pathology. For example, in CSOM or cholesteatoma, meatoplasty facilitates drainage, and infection control, whereas in congenital stenosis, it aims to establish or maintain canal patency. Therefore, comparisons across indications are not absolute but provide an overview of technique adaptability and safety.
The demographic characteristics of the patient populations in the included studies had a wide range of variability ranging from pediatric patients with congenital ear conditions to adults and elderly individuals. Consequently, the gender distribution had a predominance of male patients in most of the studies but with a proportion of males that varied between 45% and 70%. These results represented the wide versatility of meatoplasty among different patients and emphasized the need to tailor treatment approaches according to factors such as age, gender, and the condition in question. Moreover, conditions such as COM, cholesteatoma, and EAC stenosis were common across the studies, reinforcing the broad range of conditions for which meatoplasty is considered an effective intervention.
One of the most significant observations is the wide variation of surgical techniques used in the different studies. Some studies applied one-cut meatoplasty, while others applied Z-plasty or modified approaches with graft materials, such as TF, cartilage, or free skin flaps. The variability in the surgical techniques reflects the flexibility of the procedure based on the pathology being treated. For instance, in cases involving severe canal stenosis or cholesteatoma, more extensive procedures such as tympanoplasty or mastoidectomy were often required alongside meatoplasty. Regarding outcomes, both techniques of one-cut and Z-plasty meatoplasty proved to be effective, but some minor differences in postoperative complications, such as hyperemia or canal narrowing, can influence the choice of technique in clinical practice.
The postoperative outcomes were largely positive, with most of the patients having improvements in dryness of the ear, hearing, and the resolution of chronic ear discharge. These are aligned with the primary goals of meatoplasty that involve restoring normal anatomy and function of the ear canal. Research, such as that conducted by Zafar and Kumar, 21 observed a high rate of dry ear achievement after surgery; hence, meatoplasty can be an effective remedy to deal with one of the most distressing symptoms of chronic ear conditions. Follow-up over a long period showed that most patients maintained their results and showed no recurrence of infections or cholesteatoma. However, some patients required revision surgeries due to restenosis or cosmetic issues, indicating that while the procedure is generally successful, ongoing care is essential for optimal results.
Moreover, the complications following the meatoplasty were significantly rare. Meatal stenosis, formation of granulation tissue, and keloid development are the most common postoperative complications. These complications can easily be managed with follow-up interventions like chemical cautery or, in some cases, revision surgeries. The incidence of severe complications such as loss of hearing or infections was low, which is quite encouraging and supports the safety profile of the procedure. However, long-term follow-up and maintenance care cannot be overemphasized, as several of the studies have stressed routine follow-up to avoid complications like restenosis or recurrent infections. Most studies suggested a follow-up between 3 and 12 months with continued cleaning and monitoring for signs of stenosis or infection. Patients with complicated conditions such as EAC atresia or cholesteatoma would especially benefit from these follow-ups because their condition carries a higher risk of developing complications.
However, meatoplasty can be considered an effective surgical intervention for treating a wide range of ear conditions, with favorable outcomes in terms of symptom resolution and QoL improvement. Moreover, the choice of surgical technique should be tailored to the individual patient’s condition, and long-term follow-up is critical to ensure lasting success. Although postoperative complications may arise, there is enough evidence to consider the safety and efficacy of meatoplasty, which necessitates further research on techniques and improved patient outcomes.
Limitations and future directions
While this systematic review contributes valuable insight into meatoplasty and its role in chronic ear surgeries, several important limitations must be acknowledged. First, there was significant heterogeneity among the included studies in terms of design, patient populations, surgical techniques, and outcome measures. This variability limits the comparability of results and precludes firm conclusions about the relative efficacy of individual meatoplasty approaches. Second, the presentation of data across studies was often dense and unstructured, making it difficult to extract consistent, quantifiable endpoints—particularly when outcomes were reported qualitatively or without standardized criteria. Third, the absence of a meta-analysis or pooled statistical synthesis of outcomes limits the strength of the review’s conclusions. While the diversity of study designs made formal meta-analysis unfeasible, its absence reduces the analytical depth and overall impact of the review. Moreover, some studies contain small sample sizes (less than 7 patients). A key limitation of this review is the difficulty in isolating the direct effects of meatoplasty from the outcomes of the broader surgical procedures in which it was performed. In nearly all included studies, meatoplasty was conducted alongside interventions such as tympanoplasty, mastoidectomy, or canaloplasty, which themselves contribute significantly to clinical improvements like dry ear status, resolution of infection, and hearing restoration. As a result, outcomes such as the absence of otorrhea, graft success, or improved ABG cannot be definitively attributed to meatoplasty alone. This limitation restricts the ability to assess the standalone efficacy of meatoplasty and underscores the need for future studies with more controlled comparisons or study designs that evaluate meatoplasty in isolation or with minimal procedures. Future research should focus on standardized protocols for meatoplasty approaches and long-term follow-up studies to assess the durability of outcomes. Additionally, comparative studies between specific surgical techniques of meatoplasty are needed to establish best practices in chronic ear surgery.
Conclusion
The advancements in meatoplasty and related techniques have proven highly effective in treating chronic ear conditions and improving symptoms, hearing, and quality of life. High graft success rates and minimal complications highlight their efficacy, while innovative strategies and diligent postoperative care address occasional issues like stenosis, ensuring excellent long-term outcomes. In conclusion, the comparative analysis of meatoplasty techniques reveals that while all approaches are effective in restoring auditory function and achieving a dry ear, their specific advantages and limitations vary based on surgical complexity, patient pathology, and anatomical considerations. Simpler techniques like the one-cut and modified meatoplasty offer excellent cosmetic outcomes and ease of execution, making them suitable for routine cases. In contrast, more advanced methods such as Z-meatoplasty, Corner-Tag, and bony canaloplasty provide superior canal patency and are particularly advantageous in managing stenosis, fibrosis, or complex reconstructions. Graft selection, notably the use of MAT or TF, plays a crucial role in epithelialization and healing, while advanced reconstructions like cartilage palisade techniques are invaluable in anatomically challenging cases. Overall, the evidence underscores that no single technique is universally superior; rather, the optimal choice should be guided by the individual patient’s condition, the surgeon’s expertise, and long-term maintenance goals to ensure durable, functional, and aesthetically favorable outcomes.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251376179 – Supplemental material for Effectiveness of meatoplasty techniques alone or as adjunct to other surgeries in chronic ear disease: A systematic review
Supplemental material, sj-docx-1-smo-10.1177_20503121251376179 for Effectiveness of meatoplasty techniques alone or as adjunct to other surgeries in chronic ear disease: A systematic review by Mariam Aljehani, Ibrahim Tawfiq, Fida Al-Muhawas and Abdulrhman Alsanosi in SAGE Open Medicine
Footnotes
Acknowledgements
Not applicable.
Ethical considerations
Not applicable.
Author contributions
Mariam Aljehani: Conceptualization, Methodology, Data curation, Investigation, Validation, Visualization, Writing – original draft, Writing – review & editing, Supervision, and Project administration. Ibrahim Tawfiq: Conceptualization, Investigation, Validation, Visualization, Writing – original draft, and Writing – review & editing. Fida Al-Muhawas: Investigation, Data curation, Validation, Writing – original draft, and Writing – review & editing. Abdulrhman Alsanosi: Methodology, Data curation, Writing – original draft, and Writing – review & editing. All authors approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.