
Abstract
Fathers report feeling sidelined and being treated as secondary parents in healthcare settings. Despite their vital caregiving contributions, fathers remain underrepresented in pediatric palliative care research, particularly outside oncological contexts. This qualitative study, using a phenomenological hermeneutical design, explores the lived experiences of Norwegian fathers raising children with progressive life-limiting conditions. Thirteen fathers of children aged 1–18 years participated in in-depth, semi-structured interviews conducted online or in person. All children had received a diagnosis at least 12 months prior, lived at home, and received varying levels of care support. The analysis followed a modified version of Ricoeur’s interpretation theory, as described by Lindseth and Norberg in their three-step phenomenological hermeneutical method, and revealed four themes: (1) “Balancing between grief and relief,” where fathers described emotional ambivalence during the diagnostic phase; (2) “Searching for stability in an unpredictable life,” where fathers often turned to information and peer support to manage uncertainty; (3) “Feeling homebound yet making space for life,” where many felt confined to the home but made deliberate efforts to create meaningful experiences for their children and themselves; and (4) “Juggling between being a dad, caregiver, and breadwinner,” where fathers navigated complex and often conflicting roles. The findings highlight the emotional and practical challenges fathers face and underscore the importance of recognizing their unique support needs. Proactive involvement in care planning, access to pediatric palliative care services, peer networks, and respite opportunities are essential not only for the child’s well-being but also to sustain fathers’ caregiving capacity.
Introduction
Fathers’ experiences of having a child with a progressive life-limiting condition are deeply complex and multifaceted. The emotional impact of the diagnosis profoundly influences their efforts to establish a new sense of normality in family life, and fathers have reported feeling like peripheral or secondary parents in healthcare settings. These insights, drawn from meta-studies based on primary research conducted over the past two decades (Fisher et al., 2021; Sjuls et al., 2023), underscore the need for greater recognition and tailored support for fathers within pediatric palliative care (PPC). Whereas the majority of children eligible for PPC have non-oncological conditions (Fraser et al., 2021), most studies on fathers’ experiences have focused on children with cancer (Fisher et al., 2021). To ensure that current practices adequately include and support all fathers, it is essential to gain a deeper understanding of their lived experiences when caring for a child with a progressive life-limiting condition beyond cancer.
Background
The role of fathers in parenting has evolved beyond the traditional perception of being solely breadwinners to encompass a more active involvement in their children’s lives, including caregiving (Cabrera et al., 2018; Novianti et al., 2023). Despite the profound impact fathers have on children’s development, there is a notable underrepresentation of fathers in parental research (Cabrera, 2020), child health research (Davison et al., 2017), and PPC research (Dutta et al., 2019; Macdonald et al., 2010). An important consideration within PPC is ensuring that parents are functioning effectively in their parental role (Benini et al., 2022). However, fathers often tend to appear outwardly as strong, concealing their emotional reactions to position themselves as supportive figures and protect others. This tendency may contribute to feelings of alienation and isolation, with many fathers grieving privately rather than expressing their emotions openly (Fisher et al., 2021; McNeil et al., 2021). Furthermore, fathers have reported experiencing financial distress alongside the ongoing challenge of balancing work commitments with spending time and attending hospital appointments with the affected child (Sjuls et al., 2023).
Categories in Children Requiring Palliative Care (Benini et al., 2022)
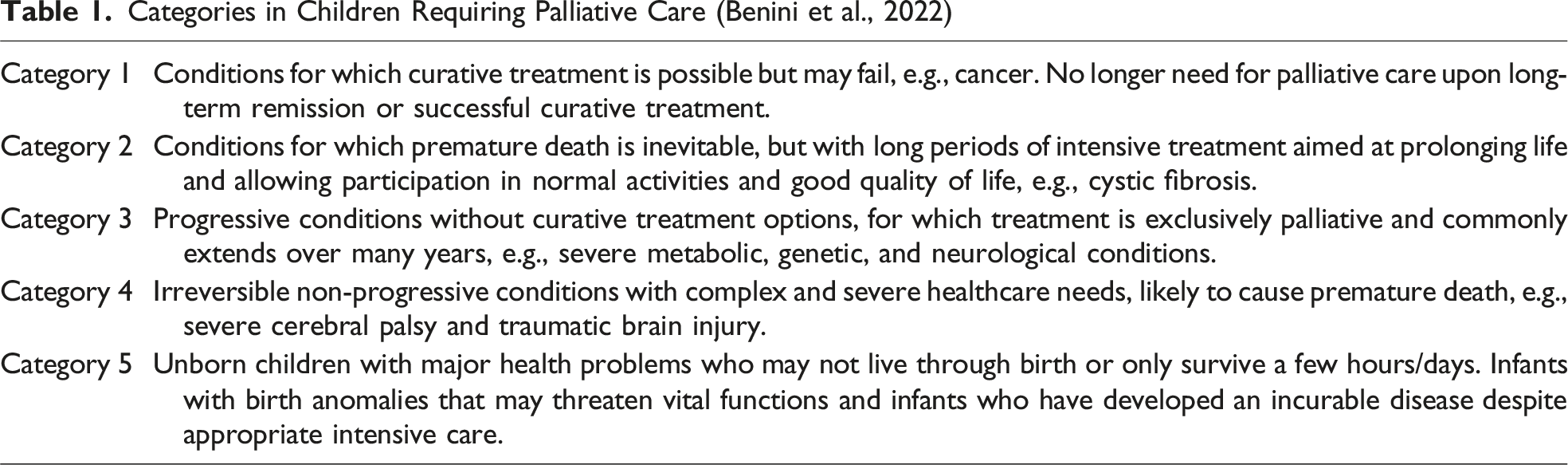
This study focuses on children with progressive life-limiting conditions (Category 3) that are typically associated with rare genetic, neurological, or metabolic conditions. These children often have delayed cognitive development, lack of verbal language, and various physical ailments including pain, feeding difficulties, epileptic seizures, respiratory challenges, and sleep problems (Pawliuk et al., 2020; Siden, 2018). Unlike other conditions requiring palliative care, these conditions are progressive, and treatment is exclusively palliative. Due to their rarity, both the disease trajectory and life expectancy are often unpredictable and many experience a prolonged delay in obtaining a definitive diagnosis (Nevin et al., 2023).
Parents of children with progressive life-limiting conditions report facing substantial daily challenges. Beyond the time-consuming demands of caregiving and the associated physical burden (Brandt et al., 2022), parents report a negative impact on sleep (Hartley et al., 2021) and psychological well-being, including stress, depression, and a diminished overall quality of life (Nevin et al., 2023). In addition to these emotional burdens, parents often face recurring experiences of loss and anticipatory mourning as their child gradually loses functions due to the progressive nature of the illness (Nevin et al., 2023; Price et al., 2022). Moreover, the rarity of many progressive, life-limiting conditions further exacerbates these challenges, as parents often face a lack of information and persistent uncertainties regarding their child’s life expectancy (Nevin et al., 2023). As a result, parents become experts on their child’s care and report feeling isolated because those around them struggle to grasp the unique challenges they face (Engel et al., 2023). However, whereas a child’s progressive life-limiting illness presents immense challenges, it can also provide an opportunity for personal growth, enabling parents to adopt new beliefs about what is meaningful and gain new perspectives on life (Nevin et al., 2023; Sjuls et al., 2023).
Despite the significant challenges parents face, research on fathers’ experiences in the context of having a child with a progressive life-limiting condition remains limited (Fisher et al., 2021; Sjuls et al., 2023). To address this research gap and provide insights that can enhance support and PPC for fathers, this study aimed to explore fathers’ experiences related to the diagnostic process and their experiences of living with a child with a progressive life-limiting condition.
Methods
Design
To understand fathers’ lifeworld from their own perspective of being in the world, the present study was grounded in phenomenological hermeneutics (Ricoeur, 1975). Following Brinkmann and Kvale (2018), we designed a qualitative study based on in-depth, semi-structured interviews.
A phenomenological hermeneutical approach allowed us to explore fathers’ experiences not only in terms of what was said but also in terms of the meanings embedded within the narratives (Ricoeur, 1976). According to Ricoeur (1976), discourse that becomes text mediates between language and lived experience, making interpretation possible. By treating the interview transcripts as autonomous texts, we were able to establish an analytic distance (distanciation) from the fathers’ immediate self-expressions, which enabled the development of a nuanced interpretation that moved beyond mere description to reveal underlying patterns of meaning in their experiences (Ricoeur, 1973, 1976). Moreover, the method developed by Lindseth and Norberg (2004, 2021) allowed a hermeneutic movement between the whole and the parts in the analysis, ensuring that individual statements were interpreted within the broader context of fathers’ lived experiences, while still acknowledging the uniqueness of each account.
Setting, Participants, and Recruitment
Norway has a publicly financed healthcare system, in which each health region is obliged to provide regional and local PPC teams, often in close collaboration with municipalities and non-profit foundations that also offer PPC services. The majority of children with life-limiting conditions live at home with their family, and several of these children have access to self-directed personal assistance for a certain number of hours per week, depending on the child’s medical complexity. In addition, municipalities may grant respite care based on the needs of the child and their family. However, access to local and community-based PPC services may vary across health regions and depends on families’ place of residence (Rud et al., 2023; Winger et al., 2024).
The inclusion criteria were as follows: fathers who had been living at home with their child (1–18 years) with a recognized or confirmed diagnosis of a progressive life-limiting condition (Category 3 of life-limiting conditions requiring PPC) for at least 12 months. In the context of this study, we defined a father as an individual in a caregiving role who self-identified as a father, encompassing biological fathers, stepfathers, adoptive fathers, co-fathers, and foster carers (Oxford English Dictionary, 2016). In adherence to ethical considerations and the well-being of families involved, exclusion criteria were bereaved fathers and those with children who were terminally ill and expected to die within a short timeframe (days or weeks).
Purposive sampling was used to identify fathers from respite care facilities and from a foundation offering PPC services. Given the rarity of progressive life-limiting conditions in children, the purposive sampling was followed by a convenience sampling strategy, whereby all fathers who met the inclusion criteria were invited to participate (Patton, 2002). Under the guidance of the first author, healthcare professionals from PPC services approached eligible fathers and provided oral and written information about the study. Those who agreed to participate were referred to the first author, who then contacted the fathers to arrange a suitable time and place for the interview. A dedicated web page also provided information and the possibility to sign up for participation. The web page was advertised through social media and shared by relevant user organizations, healthcare institutions, and individuals. This contributed to additional snowball sampling, as we were aware that many parents followed and shared content with user organizations and participated in peer support groups online. Fathers who volunteered through the website underwent clarification calls with the first author to confirm their eligibility for inclusion.
Data Collection
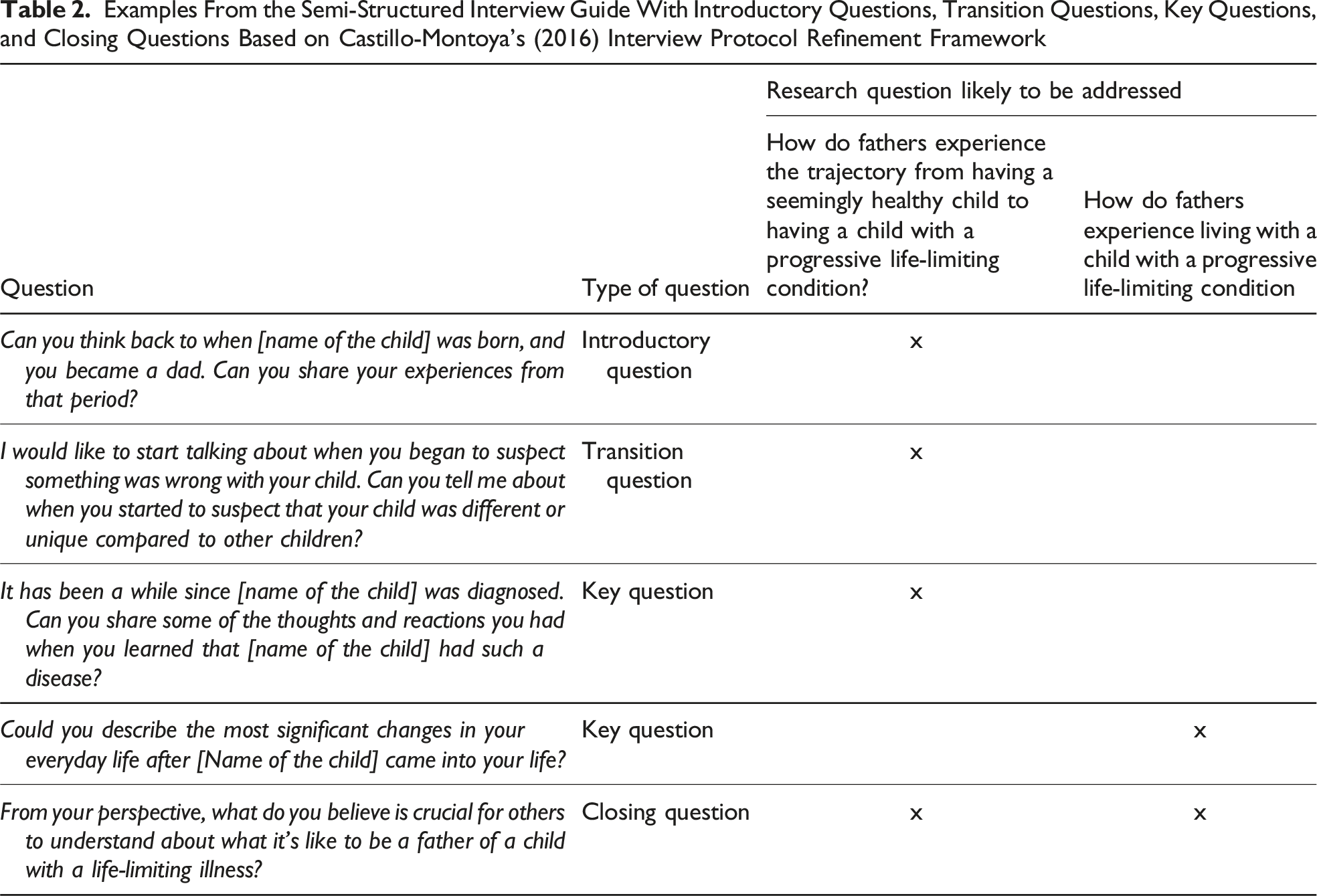
Examples From the Semi-Structured Interview Guide With Introductory Questions, Transition Questions, Key Questions, and Closing Questions Based on Castillo-Montoya’s (2016) Interview Protocol Refinement Framework
Data Analysis
Grounded in Paul Ricoeur’s (1976) interpretation theory and guided by Lindseth and Norberg’s (2004, 2021) three-step method for researching lived experience, we first read through the transcribed interview text as a whole with a phenomenological and open attitude, referred to as a “naïve reading.” This initial reading of the text allowed us to form a preliminary understanding of the fathers’ lived experiences as expressed in the interview text, providing a foundation for the subsequent structural analysis.
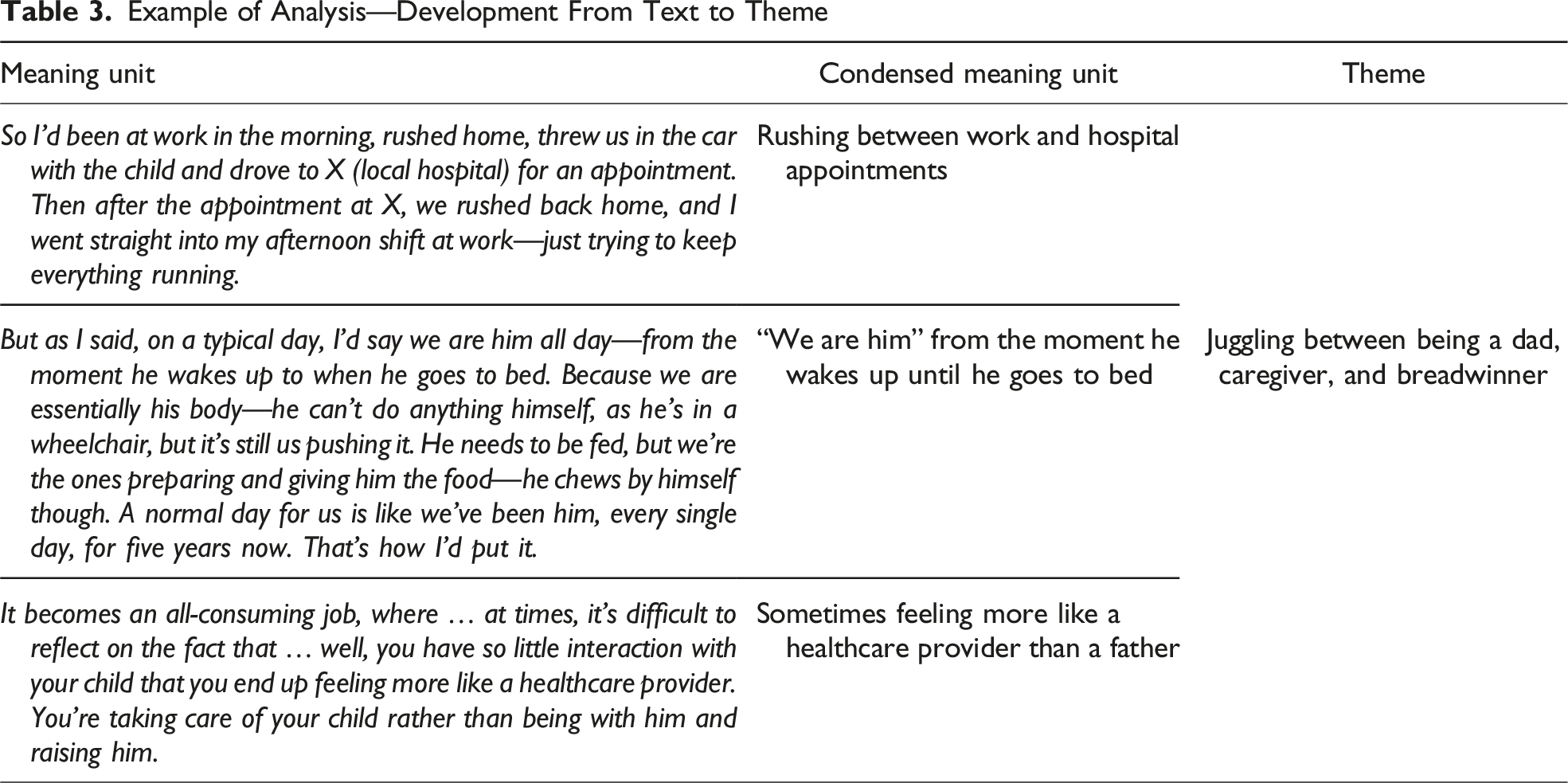
In the second step of the analysis, we uploaded the transcribed interview texts to software for qualitative analysis (NVivo, version 12) (QSR International Pty Ltd, 2018) and performed a structural analysis. The text was derived into meaning units by the first author.
The further development of themes was an iterative and reflective process. The condensed meaning units were systematically reviewed and compared to identify patterns, similarities, and differences. Throughout this phase, we continuously reflected on how the emerging themes aligned with and validated the naïve reading, and vice versa. This reciprocal process strengthened the interpretive depth and ensured coherence between initial impressions and the structured analysis (Lindseth & Norberg, 2004, 2021).
Example of Analysis—Development From Text to Theme
In the third step of the analysis, to illuminate various aspects of the interview text and gain a comprehensive understanding of fathers’ experiences, the themes were reflected on as a whole against our preunderstanding, theory, and previous studies on PPC in the Discussion section (Lindseth & Norberg, 2004, 2021).
Rigor and Reflexivity
Lincoln and Guba’s (1985) criteria of credibility, transferability, dependability, and confirmability provide a structured approach to evaluating the trustworthiness, rigor, and integrity of qualitative studies (Polit & Beck, 2014).
To demonstrate credibility, we reflected and evaluated how subjectivity and context might have influenced the research, encompassing personal, interpersonal, methodological, and contextual reflections (Olmos-Vega et al., 2023). Interpretation is inevitably shaped by the authors’ preunderstanding (Lindseth & Norberg, 2004, 2021), which is based on our professional and personal experiences. This interview study forms part of the first author’s PhD project investigating fathers’ experiences in PPC. The first author, an intensive care nurse with a background in both pediatric and critical care, conducted and transcribed all interviews. The co-authors are experienced qualitative researchers with backgrounds as pediatric and/or intensive care nurses. All authors are mothers and identify as female, making it essential to reflect on how gender differences may have influenced the interview setting and subsequent analysis. The interview context may have positioned fathers in a vulnerable role, potentially challenging their sense of control and masculine identity (Holstein & Gubrium, 2003; Schwalbe & Wolkomir, 2001). Traditional gender roles, where men are seen as breadwinners and women as caregivers (Cabrera et al., 2018), may have shaped both how fathers expressed themselves and how we, as female researchers, interpreted their expressions. Some fathers may have upheld such roles in interviews, resulting in more guarded and shallowed accounts. Others, however, might have felt freer to disclose feelings and vulnerabilities because they were interviewed by a woman rather than a man (Holstein & Gubrium, 2003). While we cannot generalize, our overall impression is that fathers openly shared their experiences, with some needing breaks or expressing emotions during the interviews.
Given the sensitive nature of PPC, the emotional impact on the interviewer (MS) was inevitable. The interviewer experienced emotional responses, including being moved, saddened, and occasionally angered on behalf of the fathers. Emotional reactions were managed through debriefing and reflection with co-authors after the interviews. The interviewer was also challenged by the need to remain a researcher rather than a nurse, as the impulse to suggest interventions or improvements arose when fathers spoke about experiences they found difficult. However, efforts were made to maintain a neutral attitude during the interviews, for example, by adhering closely to the interview guide and by being aware that the fathers had been informed prior to participation that they could seek support from their general practitioner if needed.
Referring to how the findings are applicable in other settings or groups, transferability was supported through thick descriptions and detailed methodological explanations (Stahl & King, 2020). To maximize heterogeneous patterns of fathers’ experiences, geographical variations were addressed by conducting online interviews. Online interviews also increased the number of fathers participating in the study. At the same time, we encountered challenges in controlling the online interview setting and experienced for at least one occasion that the mother was present, and the father seemingly looked at her over the screen to validate his answers. Learning from these experiences, we encouraged the fathers to choose a private space for the interviews and inquired about the presence of others before the interview started. Compared to phone interviews, online interviews allowed observation of non-verbal cues, such as facial expressions and gestures. However, we acknowledge potential limitations in capturing all nuances online (Archibald et al., 2019).
Regarding dependability, the first author maintained a research log and reflexive journal to support ongoing reflection on preunderstandings and emotional responses (Connelly, 2016). The interviewer also used probing questions to deepen participants’ reflections and verifying interpretations with member checking during interviews with clarifying questions like “Am I understanding you correctly if …?” Preliminary results were shared with a reference group of user representatives and healthcare professionals, enhancing the dependability of the findings by providing feedback and helping us interpret and contextualize the fathers’ accounts. This study also shows high information power due to a highly specific sample and in-depth analysis, conducted alongside a well-established theoretical foundation. Consecutive transcription enabled continuous reflection, improving the quality of subsequent interviews (Malterud et al., 2016). To enhance confirmability and avoid relying solely on one researcher’s interpretation of the data (Connelly, 2016), all four authors participated actively in the analysis process. This collaborative approach ensured that the interpretation of the fathers’ experiences reflected a shared understanding rather than an individual perspective. Moreover, we have supported our findings with relevant quotations from participants, to enhance the transparency of our interpretations.
Ethical Considerations
The study received ethical approval from the Regional Committee for Medical and Health Research Ethics (REK) (reference number: 262247). All interviews were audio-recorded. The data storage plan was approved by the Norwegian Agency for Shared Services in Education and Research (SIKT) (reference number: 700106) and handled in accordance with the regulations outlined in the Norwegian Personal Data Act (2018) and Health Research Act (Helseforskningsloven, 2021). Comprehensive written and oral information was provided regarding who to contact if fathers needed follow-up after the interview, the option to withdraw from the study at any point, and details about data security. To avoid unnecessary pressure to participate, fathers were not approached by their child’s primary caregiver regarding informed consent.
Results
Characteristics of Included Fathers and Children
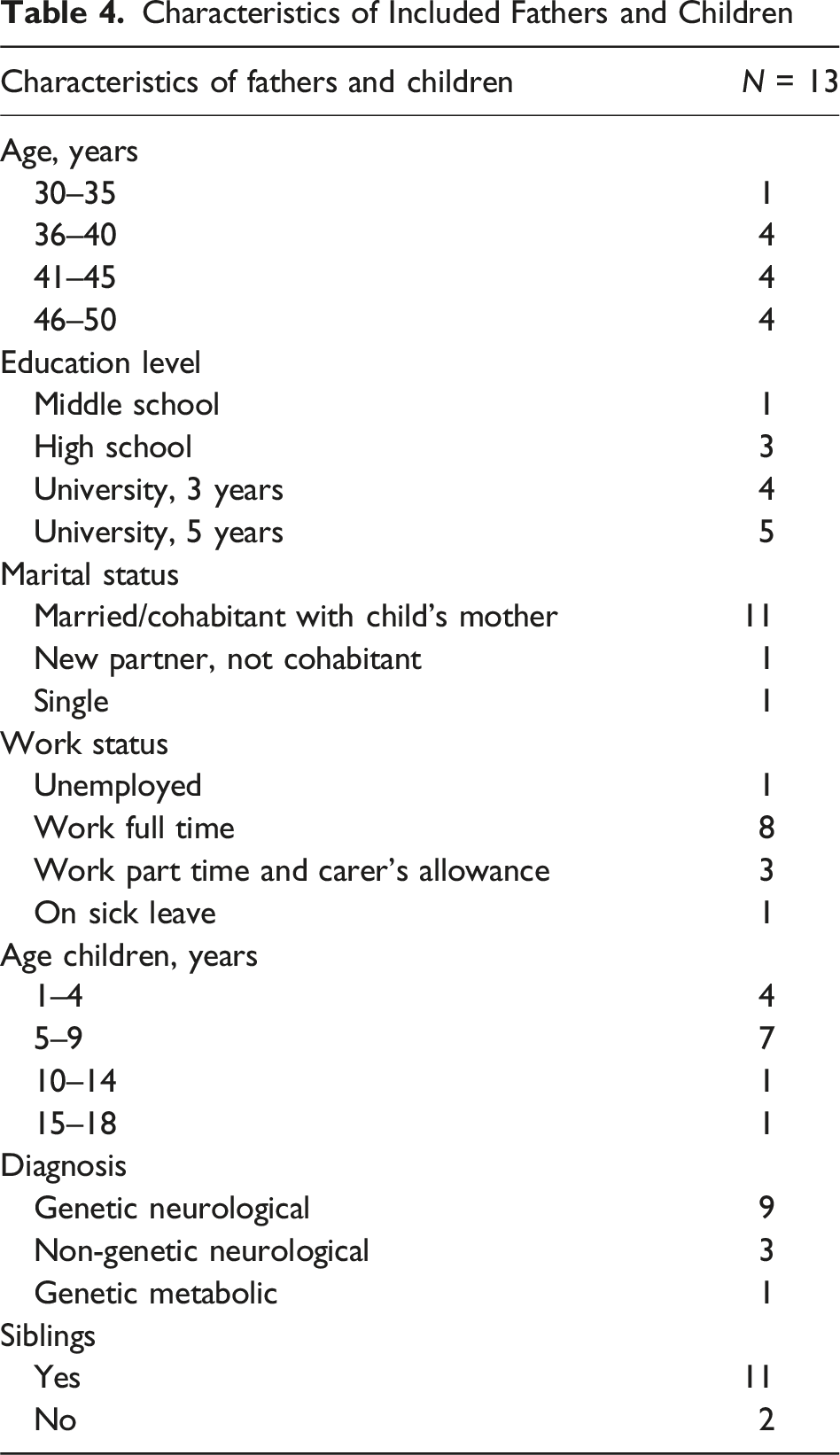
The interviews were conducted between October 2022 and October 2023 (11 online and 2 at home). The duration ranged from 53 to 82 min, with an average of 67 min. The interviews, totaling 14 h and 15 min, were transcribed into 224 pages of text.
Through the naïve reading, it became evident that for fathers, coming to terms with and reorienting their lives after having a child with a life-limiting condition is a lengthy and ongoing process. Through the structural analysis, we developed the following four themes reflecting fathers’ in-depth experiences: (1) balancing between grief and relief; (2) searching for stability in an unpredictable life; (3) feeling homebound yet making space for life; and (4) juggling between being a dad, caregiver, and breadwinner. In the following sections, we will elaborate on these four themes.
Balancing Between Grief and Relief
For fathers, balancing between grief and relief encompassed both the sorrow of realizing that their child had a life-limiting condition and the sense of relief that came with a diagnosis that provided an explanation for their child’s symptoms.
Some fathers knew from ultrasound that their unborn child had congenital anomalies, whereas others had children who were born extremely prematurely. However, most of the children appeared healthy at birth, making it difficult for fathers to initially accept that something was “wrong” with their child. Fathers described how their child was falling behind compared to other children, and how they felt as being in limbo when they knew something was wrong, but not how serious the condition was. The trajectory from having a seemingly healthy infant to diagnosis often evolved over several months or years, and fathers expressed anger and frustration when specialists focused on direct symptom treatment instead of finding a diagnosis, or when they experienced lack of competence at their local hospital. One father said: Then I barged into the office of a doctor named NN, she is a paediatrician there, and I said: “I won’t put up with this. You need to stop now. It can’t be about pride in figuring out what this is. Either you refer her to the regional hospital now, or I’ll do it myself. This can’t go on, for goodness’ sake!” (F12)
For some, the long journey to diagnosis was experienced as a gradual process. However, for most fathers, the final diagnosis still came as a shock evoking a range of emotions. In their view, psychological support was essential to handle the situation, but often offered too late, after the initial shock phase. Several fathers described that, although they were quieter than their partner and took on the role of “the strong one,” they still experienced the same feelings as the child’s mother. As one father put it: A father who isn’t allowed to share his opinions or contribute his experiences and knowledge, it’s a ticking time bomb that eventually explodes … […] It takes a toll on our mental health because we’re not as strong as everyone might think. If we walk around with thoughts we can’t express, we also become mentally ill. And I think that part is often forgotten. (F5)
Despite the initial shock, a diagnosis provided fathers with an explanation for their child’s clinical symptoms. They described feeling a sense of relief, metaphorically described as “pieces falling into place.” Although a diagnosis offered an explanation, it was also a pivotal moment in fathers’ perception of control over the situation, intensifying their need for information. How the diagnosis was presented played a crucial role in how fathers coped. A key factor was whether doctors took the time and were available to answer questions, which made fathers feel supported and reassured. In contrast, one father said: It was a brief meeting with three doctors. […] It felt like a black hole. I hardly remember any of it. The information was delivered quickly and concisely, straight to the point. Then they thanked us for the meeting, and I was left alone with a million questions. And essentially no place to turn to afterwards or the ability to move forward. (F4)
Searching for answers, some fathers expressed how religious beliefs influenced their experiences of receiving a diagnosis. For those fathers, their child’s condition could be perceived in two contrasting ways: as a punishment from God or as a source of solace. Another source of solace was receiving a genetic diagnosis. Fathers found reassurance in the fact that a genetic condition was beyond their control: If you’re driving and get into an accident, I would really struggle with feelings like “this is my fault” and overthink everything, wondering whether you made a mistake or if you could have done something differently. […] But in this case, it was a situation where nothing could have been done differently, yet it still went wrong. And that, at least for me, makes it easier to accept. (F13)
Searching for Stability in an Unpredictable Life
From the time of diagnosis and throughout their child’s illness trajectory, fathers described their lives as unpredictable. In response to this uncertainty, they sought information, prepared for medical emergencies, and turned to their partners and peers for emotional support.
The rarity of the disease and the unpredictable disease trajectory were sources of frustration, often making fathers feel as though they were losing control. Illustrating the anxiety, fear, and helplessness over the situation, the uncertainty about their child’s life expectancy was described by a father as playing a game of “Russian roulette.” To gain a sense of stability, many fathers emphasized the importance of seeking information and being as prepared as possible for the disease’s progression. In their search for information, several fathers spent considerable time searching the internet: And there’s basically no literature to be found about the disease. I’ve been sitting with Google Translate, reading publications in French and German and so on … (F4)
Despite the limited information available on their child’s condition, fathers found PPC teams and facilities to be valuable sources of guidance. These professionals provided insights into what to expect in a palliative disease trajectory regardless of the specific diagnosis. Although fathers had come to terms with the fact that their child would eventually die, the term pediatric palliative care was difficult to accept, particularly when their child was in a stable condition and not expected to die within a short time frame. Many chose to focus on the present rather than dwell on the inevitable. In everyday life, you have to try to put those feelings in a separate box. Open it and look at them now and then, but otherwise, you try to keep it closed because … well, you still have a life to live. (F8)
To establish stability in their everyday life, several fathers took on the role of the “guardian of continuity.” This meant coordinating hospital appointments, communicating with respite care facilities, attending meetings with carers, and managing paperwork for the Labour and Welfare Administrations. Additionally, fathers described being in a constant state of readiness. They ensured the availability of sufficient medication and medical equipment and remained vigilant for potential emergencies, such as unintentional tracheostomy removal or epileptic seizures.
Fathers described how their relationship with their partner was affected in various ways. Although many found formal support settings, such as family counselling centers, valuable for learning tools to strengthen their relationship, others struggled with feelings of imbalance. Most fathers described growing closer to their child’s mother due to their shared understanding of the situation. However, care commitments and long hospital stays often placed significant strain on their relationship, ultimately leading to divorce for one of the fathers. Despite these challenges, most fathers described becoming each other’s therapist, engaging in difficult conversations and offering support, such as providing positivity when their partner felt discouraged.
Aside from the child’s mother, fathers felt that no one could truly grasp their situation unless they had experienced it themselves. Seeking support from peers in similar circumstances, whether through social media or face-to-face interactions, was seen as highly valuable, providing immediate understanding, practical advice, and the opportunity to learn from others’ experiences. However, connecting with peers could be challenging for some, particularly when their child’s conditions was rare. Despite this, many fathers were eager to give back, which served as a strong motivation for participating in research or reaching out to others in similar situations. Several fathers expressed a wish for dedicated “father meetups.” These gatherings would provide a safe space for fathers where they could share their experiences and open up about the unique challenges they faced: […] Of course, there can be a place for mothers, that’s not the issue. But they often have an easier time or more opportunities to find that release in daily life. I think … it might sound a bit prejudiced, but I think some men might need a little push to dare to open up, to talk about things, and to face the emotions that might come up. Emotions that not everyone experiences because they’re not living in a situation like this with the same challenges as we are. (F3)
Feeling Homebound, yet Making Space for Life
Fathers described how their child’s medical complexity required various adjustments to integrate into everyday family life. Although they often felt homebound, they also sought to create space for life, both in terms of providing their child with a fulfilling life and by making time for themselves. This included spending time with family and friends and maintaining those relationships.
Following the diagnosis, fathers emphasized the importance of enabling their child to live a meaningful life, free from pain and filled with meaningful moments and activities. However, this often evoked a sense of grief over what their child was missing, as they perceived shortcomings in the support system when their child received what was needed to survive but not what was sufficient to create a good life with meaning. Some fathers emphasized the importance of including their child in family activities regardless of their complex care needs, and others described how their child had gradually become excluded as they could no longer participate in the same way. Leaving the house required extensive planning and preparation, and left fathers feeling homebound. One father noted: You notice how rarely you see children like this in public spaces. They’re hidden away, probably by their parents, for practical reasons—it’s difficult to bring them everywhere […] There are more families in this situation than you realize. Once you get to know it, you see it. But for those who’ve never encountered it, it’s like this non-existent group. (F11)
Fathers noted that their child was often most comfortable at home due to the need for peace and familiar surroundings. As a result, one parent would typically stay at home with the child while the other attended events or took holidays with the siblings. Such separation created a sense of loss, as fathers mourned the memories they were unable to create together as a family. Nonetheless, siblings were seen as important because healthy siblings forced them to maintain a sense of normality and get out of the house. One father said: For heaven’s sake, if people find themselves in this situation with their first child, get started on number two. Damn it, I think that’s the best thing you can do in such a situation. You’re forced to live a normal life. You’re forced to go to trampoline parks and go out and do all those things … to get out, you know. So that’s my advice, at least. (F10)
Fathers emphasized the importance of getting out of the house and creating space for life. Although some expressed feelings of guilt about leaving their spouse to manage responsibilities alone, activities such as hunting, hobbies, meeting friends, sports, and being among colleagues were described by fathers as important ways to disconnect. One father noted: […] Think about yourself a bit before you think about everyone else. Like on an airplane, you’re told to put on your own oxygen mask first for a reason. If you stop functioning, it’s much worse for those around you. So being a little selfish is healthy in a situation like this. (F11)
To create a space for life, fathers emphasized the importance of close relationships with friends and family. They often found that their social network shrank, as friends and family either found it difficult to meet or had difficulty understanding their situation. Despite this, fathers described how their vulnerability and openness made their remaining relationships grew stronger and were deeply moved by how friends and family stepped up to support them. One father described it as having “sorted through his group of friends and figured out who he’d want to go to war with” (F6).
Juggling Between Being a Dad, Caregiver, and Breadwinner
Fathers felt they were in a conflicting role of being a father, caregiver, and breadwinner. These were roles that were not necessarily possible to combine, and they were alternating between the different roles toward the child and the rest of the family depending on the circumstances.
Several fathers expressed that there were times when they had not experienced a sense of fatherhood or personal connection to the child. This could be because they were afraid of forming an emotional bond, knowing that the child’s life expectancy was limited, or because the child’s demands were so overwhelming that they felt more like healthcare providers than fathers to their child. Seeing other parents doing things with their child that they never could was especially painful. But still, when you see other children of the same age sledging, playing outside, and going on holiday, whatever it may be, he doesn’t get to have those experiences in the same way. It’s heartbreaking. (F7)
Caring for their child, fathers described how they became physically exhausted from balancing both fatherhood and caregiving. The children often required their full attention, and fathers were often responsible for heavy lifting and physical labor, particularly as their child got older and heavier. In addition to the physical strain, fathers acknowledged that chronic sleep deprivation affected their daily lives. Many took on roles similar to those of healthcare professionals, assessing the medical risks of caring for their child at night. Valuing their privacy, some chose not to have night-time care at home, reasoning that if something were to happen during the night, it was meant to be, and in the child’s best interest to be allowed to pass away. Beyond the lack of sleep, fathers also described experiencing persistent exhaustion and the mental strain of caregiving. Witnessing their child’s pain and discomfort was described as particularly challenging.
As their child’s condition gradually worsened and required increased respite care, it took time to come to terms with the idea that they were falling short in their role as fathers and could no longer care for their child entirely on their own. The growing need for respite care also served as a verification that the child’s condition was deteriorating. Fathers experienced mixed emotions: on the one hand, a sense of giving up on their child, and, on the other, relief that someone else was taking over some of the responsibility. Several fathers expressed a wish that healthcare professionals had raised the issue of respite care earlier: I wish someone had talked to us earlier and said, “Do you realize how big of a job you’re taking on? Do you realize how exhausted you might become? How many struggles this could involve?” And maybe, at that point, they could have at least brought up, if not offered, the alternative, saying that the responsibility is so immense that it shouldn’t be seen as a failure if you decide that your child should live permanently in a care home. (F6)
In most families, fathers took on the role of breadwinner. Fathers often felt guilty that their spouse had to assume the primary caregiving role at the expense of her own career. However, it was usually financially advantageous for fathers to continue to work while the mother stayed at home to care for the child with a carer’s allowance from the Norwegian Labour and Welfare Administrations. For those who were able to reach an agreement with their employer, adjustments such as modified job tasks, flexible working hours, and remote work were highly valued in balancing work and caregiving responsibilities. Despite the financial advantages of continuing to work, several fathers expressed frustration with some user organizations and broader societal structures that they felt reinforced traditional gender roles and positioned fathers as breadwinners and mothers as primary caregivers.
Discussion
In this study, which explored fathers’ experiences of living with a child with a progressive life-limiting condition, we found that in the period leading up to the child’s diagnosis, fathers experienced a sense of being in limbo. Fathers described balancing between grief over their child’s serious condition and the prospect of a limited life, and simultaneously relief at receiving a diagnosis that offered an explanation. Living with the child often made fathers feel homebound, yet they simultaneously sought to create a space in which to live their new life. Over time, this process evolved into a constant search for stability in an unpredictable life, as they also attempted to juggle their roles as caregivers, dads, and breadwinners.
The emotional dynamic of balancing between grief and relief in the diagnostic phase was a central theme. During this particularly challenging period, fathers expressed vulnerability and frustration over the absence of emotional support, navigating the diagnostic odyssey largely on their own (Le et al., 2025). Their grief was less visibly expressed, often adopting a protective role as they balanced their own emotional needs with their desire to support their family. This balancing act is consistent with numerous review studies that suggest fathers’ emotional responses receive less attention in healthcare settings, partly because fathers tend to grieve privately and position themselves as “the strong one” to support their partner (Fisher et al., 2021; Postavaru et al., 2020; Sjuls et al., 2023). Despite international standards of PPC emphasizing the importance of providing family members with professional support and opportunities to express and process their emotions (Benini et al., 2022), our findings suggest that fathers may nevertheless remain in a blind spot when it comes to emotional support. Although healthcare professionals cannot be expected to intuit unspoken emotional needs, it is crucial, as indicated by our findings and existing literature, to proactively engage fathers in emotional support conversations (Fisher et al., 2021; Postavaru et al., 2020; Sjuls et al., 2023). The complexity of balancing grief and relief becomes even more pronounced in the context of genetic conditions. Although some fathers report relief that the condition passed on is genetic, others experience a sense of grief and personal responsibility (Davies et al., 2004; Mole et al., 2025; Von Der Lippe et al., 2022). This duality of balancing grief and relief underscores the need for healthcare professionals to proactively address the emotional consequences of diagnosis, particularly in cases involving genetic conditions.
In fathers’ search for stability in an unpredictable life, the key strategy was similar to what other father-studies within PPC have pointed out: gaining as much information as possible about their child’s condition and progression (Fisher et al., 2021; Sjuls et al., 2023). Fathers highlighted especially PPC teams and peers in similar situations as valuable sources of information. According to international standards that emphasize that PPC is a right for children and their families facing life-limiting conditions (Benini et al., 2022), children with non-malignant conditions and uncertain prognoses are less likely to receive timely access to PPC (Holder et al., 2024). Our findings support this observation, highlighting that PPC is often mistakenly associated only with end-of-life care rather than a broader approach aimed at enhancing quality of life (Holder et al., 2024; Mitchell et al., 2021). Healthcare providers may face similar dilemmas, as the timing of introducing PPC can be complex, as some of them fear that raising the topic too early might undermine parental hope and harm trust in the relationship between healthcare providers and parents (Holder et al., 2024; Winger et al., 2022). Despite this, parents, regardless of gender, value honest and transparent communication about their child’s illness trajectory and prognosis (Nevin et al., 2023).
An additional strategy for fathers in creating stability in an unpredictable life was connecting with peers, as they provided a space where fathers felt understood without the need for lengthy explanations (Engel et al., 2023; Nygård et al., 2024; Sjuls et al., 2023). Consistent with existing research (Nygård et al., 2024; Von Der Lippe et al., 2022), fathers in our study utilized social media platforms for peer connection, benefiting from quick responses and support without needing in-person interaction (Baumbusch et al., 2019). They expressed interest in father-specific peer support groups, viewing them as potential safe spaces to share their experiences. However, other studies have indicated that male-only settings may present barriers, as social norms around masculinity can discourage emotional openness (Postavaru et al., 2020; Ware & Raval, 2007). Instead, it has been suggested that social gatherings or support services based on activities instead of formal support groups could be advantageous for men (Robb, 2025; Vatne et al., 2022).
Another finding was that many fathers found themselves grappling with a profound tension between the feeling of being homebound while simultaneously striving to create space for life. Being homebound, fathers grieved the loss of opportunities to create shared family memories. The right of all children, regardless of health status, to participate in play and recreation is incorporated in the UN Convention on the Rights of the Child (United Nations, 1989), and fathers in our study and previous studies on parents highlight the importance of creating opportunities for their child to engage in meaningful activities despite illness (Kittelsen et al., 2024; Vatne et al., 2022). Nonetheless, the experience of being homebound and the limitations it imposes on family memory-making are well documented within families of children with complex needs and those receiving PPC (Nygård et al., 2024; Price et al., 2022). The emphasis on creating space for life and shared experiences is not only about quality of life in the present but also about laying emotional foundations for coping with loss in the future. Reflecting on meaningful memories with the child has been identified as an important bereavement strategy for parents (Polita et al., 2020). If PPC, as defined by international standards, aims to enhance quality of life and support families in accordance with their values and priorities (Benini et al., 2022), then enabling opportunities for shared family experiences despite the challenges of complex care must be considered an essential aspect of holistic support.
Fathers in our study also highlighted the importance of making space for life on a personal level. For many, this did not mean extraordinary activities but rather reconnecting with everyday practices such as playing sports, going for a walk, or meeting a friend. These activities were described in our study and previous research on fathers within PPC as essential for restoring a sense of normality (Sjuls et al., 2023). Prioritizing mental health is important for fathers when they have a child with a life-limiting condition or complex care needs (Vatne et al., 2022). However, despite recognizing this need, many find it difficult to justify taking time for themselves, often giving up previous pursuits and exercise (Hartley et al., 2021; Sjuls et al., 2023). Further, parents might experience ambivalent feelings when creating space for life for themselves and not always being present and create joyful experiences for the child (Kittelsen et al., 2024). However, evidence also suggests that parents who are able to spend time apart from their caregiving role tend to report better overall psychological well-being and quality of life (Nevin et al., 2023).
Finally, in our last theme, we found that fathers are adopting various roles, including that of being a dad, caregiver, and breadwinner. To care for themselves, fathers in our study relied on access to respite care, as it provides much-needed relief from heavy caregiving responsibilities (Murphy et al., 2021; Nevin et al., 2023). Despite the necessity of respite care, it can also trigger feelings of guilt (Murphy et al., 2021; Nygård et al., 2024), and our findings indicate that fathers are burdened by the perception of falling short in their roles as dads. Fathers in our study also expressed a desire for healthcare professionals to address their respite care concerns early in the disease trajectory and offer reassurance that using such services does not reflect inadequacy in their fatherly roles. Additionally, this support could enable them to maintain energy and patience while juggling their roles as dads and caregivers in their everyday lives (Murphy et al., 2021).
While juggling the roles of being a dad and carer, fathers often also take on the role of being breadwinners. In several countries, having a child with a life-limiting condition is associated with financial burdens and concerns for parents (Dutta et al., 2020). In contrast, the publicly funded healthcare system in Norway, combined with support from the Norwegian Labour and Welfare Administration, appeared to mitigate such challenges for most fathers in our study. Nevertheless, most fathers continued working, as this arrangement was financially more advantageous than the alternative, where the mother worked while the father stayed at home on a care allowance. Although work can provide a sense of normality and a break from caregiving duties, it may also evoke ambivalence about leaving their child, especially when they are aware of the limited time they have with them (Kittelsen et al., 2024). This ambivalence is reflected in reports of regret among fathers who, after their child’s death, wished they had spent more time together (McNeil et al., 2021). The Nordic countries are well known for progressive gender equality policies, including paid and earmarked parental leave for fathers, which the majority of men utilize (Brandth & Kvande, 2019). Novianti et al. (2023), in a systematic review of paternal roles across cultures, point out that the Norwegian context reflects an ideal of the father as emotionally present and highly involved in child-rearing, challenging traditional views of the father as solely a breadwinner or “secondary” parent. Despite this, in families with complex care needs, our findings align with previous research suggesting that fathers often report mothers as the primary caregivers (Postavaru et al., 2020) and themselves as the primary breadwinners (Schneider et al., 2011; Sjuls et al., 2023).
Limitations
Several limitations must be taken into consideration when reading the study. Our homogeneous sample is a limitation. With only one informant representing an ethnic minority, strategies for broader representation should be considered in future studies, given the increased prevalence of life-limiting conditions among ethnic minority groups (Fraser et al., 2021). Additionally, as most participants were married or cohabiting, the study does not represent single fathers, whose experiences may differ. Our study focuses on fathers in Norway, where healthcare and social support, such as a carer’s allowance, are publicly funded. Research from countries without such systems could offer broader perspectives on fathers’ experiences within PPC.
Conclusion
This is one of few studies exploring fathers’ experiences within PPC and offers valuable insight into fathers’ experiences when caring for a child with a progressive life-limiting condition. Our findings illuminate the complex and often overlooked emotional landscape navigated by fathers, who balance grief, caregiving responsibility, and the desire to maintain a sense of normalcy within their families. Importantly, the study underscores the necessity for healthcare professionals working within PPC to recognize fathers not merely as practical caregivers but as individuals with unique emotional and support needs.
Our research highlights that PPC teams and peer networks serve as a vital source of support, emphasizing the importance of early referral to PPC services and facilitating opportunities for peer connection. Furthermore, the study underscores the need for enabling fathers to create space for life, not just for their child but for themselves. Facilitating respite care and supporting fathers in caring for themselves is not merely advantageous, it may also be crucial for sustaining their long-term caregiving capacity.
Footnotes
Acknowledgements
We extend our heartfelt gratitude to the fathers who generously took time to participate in this study. We also thank the institutions that facilitated the recruitment of participants, as well as the project reference group for valuable feedback.
Ethical Considerations
Our study was approved by the Regional Committee for Medical and Health Research Ethics (REK) (approval no. 262247). All participants provided oral and tape-recorded consent (online interviews) or written consent (in-person interviews) prior to enrollment in the study.
Author Contributions
All authors contributed to the study design, the development of the interview guide, and the data analysis. MS led the recruitment and conducted the interviews with participating fathers, transcribed the interview data, and served as the primary author of the manuscript. LF, MSL, and NR provided critical feedback throughout the writing process and contributed substantially to the manuscript’s revision. All authors reviewed and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Norwegian Association for Children’s Palliative Care. (The organization was dissolved in 2023.)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the authors used ChatGPT-40 (OpenAI, 2025), GPT UiO (University of Oslo, 2025), and Copilot (Microsoft, 2025) in order to improve the readability and language of the manuscript. After using these tools/services, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.