
Abstract
What is it like for young adults living with metastatic/advanced cancers to engage in conversations about palliative care with healthcare providers? Often, young people are not introduced to palliative care. Instead, healthcare providers may assume that they are already well-supported, that their symptoms are aptly managed, or that introducing palliative care will somehow spoil any remaining hope they live with. While some of the benefits of palliative care have been explored in the literature, the experiences of young people living with metastatic/advanced cancers as they are introduced to these conversations have largely been ignored. Drawing on interviews with young adults, the aim of this study was to gain insights into these experiences. From their reflections, we may understand these conversations as an experience of an opening for talk, conversations as an experience of need and relief, and conversations as an experience of reflection. Having a discussion about palliative care may serve as a conversational opening not only to discuss additional support, but also to explore that which is meaningful for them as they live with serious illnesses. We may appreciate at the heart of these conversations are physical, relational, and existential needs that may be relieved by palliation. Significantly, these conversations afford personal reflections and frank discussions of dying and death. In this way, a phenomenological understanding of palliative care conversations provides healthcare providers with reflective insights and practical considerations for approaching these important conversations with young people, recognizing that the conversations themselves may be deeply personal and decidedly individual.
We may appreciate cancer as a difficult illness for anyone of any age. This is particularly true for young adults (18–39 years of age), where cancer is the leading cause of illness-related death (Canadian Partnership Against Cancer, 2017; Chen et al., 2018). Young adulthood is recognized as a time for people to develop independence, relationships, families, education, and/or careers (Arnett, 2000). A diagnosis of cancer for a person at this time may come with distinctive challenges (Bleyer, 2007; Jones, 2008), as their experiences are shaped by unique education, work, lifestyle, and psychosocial features (Canadian Cancer Society, 2009; Soliman & Agresta, 2008). More so, the biologies of cancers affecting young adults are different from those that are seen in both younger pediatric and older adult populations (Canadian Partnership Against Cancer, 2017). Young adults often receive delayed diagnoses as their healthcare providers may have little awareness or suspicion of cancer due to their age, or young people themselves may delay seeking care (Ramphal et al., 2016). As such, cancer in young adults tends to present at more advanced stages, with associated poorer outcomes and more aggressive forms of illness (Tricoli et al., 2016). There is limited research attending to these young people’s experiences (Canadian Partnership Against Cancer, 2017; Drake et al., 2023; Soliman & Agresta, 2008).
Accepted international definitions of “palliative care” are broad: “the active holistic care of individuals across all ages with serious health-related suffering due to severe illness, and especially of those near the end-of-life. It aims to improve the quality of life of patients, their families, and their caregivers” (IAHPC, 2018). For those young adults living with metastatic/advanced cancers, palliative care is recommended to be delivered alongside cancer care (Smith et al., 2017). Research has found that this coupling provides young adults and their families with multiple benefits such as better quality of life and less caregiver distress (IAHPC, 2018; Smith et al., 2017). Palliative care may contribute to acknowledgement and respect for their wishes (Smith et al., 2017); however, research suggests that young people are not routinely offered it (Lockwood et al., 2021). In the adolescent and young adult oncology literature, only one published qualitative study has looked at palliative care delivery from a young adults’ perspective (Drake et al., 2021, 2023). This work focused on the only young adult outpatient interdisciplinary palliative care clinic in Canada, which is housed in an adult healthcare system, to inform how to approach and integrate the care delivery (Avery et al., 2020a). Deficiencies were identified in processes of supporting transitions to palliative care even when a specialized young adult clinic is available (Avery et al., 2020a). Overall, there is a paucity of research directly engaging with young adults living with metastatic/advanced cancers as well as patient partners exploring their encounters with healthcare providers (Drake et al., 2021, 2023). Despite a relative lack of evidence, identified barriers to introducing palliative care conversations to adolescent and young adult patients are oncology teams’ reported difficulty in approaching the matter with young people, citing worry that bringing up the topic will decrease hope, and their assumptions that these patients are less interested in discussing these issues (Pritchard et al., 2011). Research that forefronts the perspectives and experiences of young adults living with metastatic/advanced cancers is needed.
Methodology
The aim of this study was to gain insights into the experience of what it may be like for young adults living with metastatic/advanced cancers to engage in conversations about palliative care with their healthcare providers. Specifically, we sought to openly explore the ways in which these conversations may hold meaning in the lives of young adults as far as the phenomenology of this experience. This focus on young adults’ experiences in themselves as they are lived through is distinct from one in which the aim is to psychologize, theorize, or otherwise conceptualize experiences abstractly (e.g., into models of power dynamics, psychological distress, or other aspects). We drew on Max van Manen’s phenomenology of practice, a context-sensitive form of interpretive inquiry, to inform this work (van Manen, 2016).
Philosophical Methods
Philosophical methods at the heart of phenomenology of practice research may be understood as the phenomenological attitude and the example (van Manen & van Manen, 2020). These methods are employed to develop a written work that is sensitive to the context of a phenomenon under study and explicative of it as a recognizable experience (van Manen, 2016; van Manen & van Manen, 2020). For this study, the adoption of a phenomenological attitude supported attentiveness to the ways in which a conversation may shape a young adult’s experience as lived through. A conversation was considered openly, recognizing some of such talk may be explorative of what palliative may mean to young adults while other talk may encompass aspects such as accessing palliative care, and expectations of palliative care and its delivery. This phenomenological way of seeing required a conversation to not simply be seen objectively as an interpersonal encounter, but rather to focus on the inceptual meaning of a conversation for the young adult. In other words, the focus on lived experience, meaning how an experience is lived through, expresses a focus on the phenomenology of the experience in itself (van Manen, 1997). In comparison, the method of the example presumes there is a recognizable phenomenon that is pointed to by the language we use to describe it: a conversational experience about palliative care. We gain access to the meaning of experiences through examples and examples exemplify an experience such that someone who has not had a particular experience may gain a sense of it. This study asks: What may the experience be like for a young person living with a metastatic/advanced cancer to have conversations about palliative care with healthcare providers? This work sought to explore the taken-for-grantedness of ordinary and extraordinary young adult life experiences to unveil fundamental lived meanings of this conversational experience.
Human Science Methods
Human science methods were employed to learn from young people’s concrete experiential accounts (van Manen, 1997, 2016). Specifically, experiences were sought from young adults between the ages of 18–39 years who were living with metastatic/advanced cancers in Canada and who had had a conversation with a member of their healthcare team about palliative care services in an adult healthcare setting. We chose an age range of 18–39 years to align with international definitions and the young adult oncology literature, recognizing this is a broad age range (Canadian Partnership Against Cancer, 2017). Palliative care services were understood as those that can include end-of-life care (Marie Curie, 2022), encompassing holistic aspects of well-being through support offerings that are spiritual, psychological, physical, and social in nature (Lockwood et al., 2021). Recruitment material included the text: “Have you talked to a healthcare provider about palliative and end-of-life care services?” In order to be inclusive of varied experiences, a multimodal approach was taken to support recruitment. The digital social media strategy involved posting on the first author’s social media channels (e.g., X, Facebook, LinkedIn, and Instagram) and reaching out to not-for-profits, advocates, healthcare professionals, researchers, and others who may have had an interest in sharing the recruitment information via social media or through their own mailing lists, websites, or in-person offerings. People who participated in the research interviews were also invited to share the recruitment information with other patients or through oncology communities (e.g., virtual, in person) that they were a part of, if they had interest in doing so. In this way, a snowball approach was used (Patton, 2002) to harness the power of patient communities through encouraging participants to share the recruitment information with each other.
Seven young adults agreed to participate. This number is consistent with other studies that have employed this methodology, where the primary focus is on depth rather than breadth of experiences (see, for example, van Manen, 2017). Participants varied from 25 to 39 years of age at the time of the interview. All were living with stage IV cancers, after having been diagnosed between the ages of 25 to 37 years. The most common form of cancer was breast cancer, with four of the participants living with stage IV breast cancer. At the time of participation, six participants lived in urban settings. Most identified as female, while a few identified as male and nonbinary transsexual male. Participants included individuals who identified as heterosexual and those identifying with other sexual orientations from the LGBTQIA2S+ communities. Six of the participants identified as white. Most of the young adults did not have children, but two did. Several reported being single, and a few were married or common law. A few of the participants passed away after they were interviewed, prior to the completion of the study. This highlights the ethics of attending to participants’ experiences in their words, the importance of the time through which their participation took place, and the need to tailor research methods to make participation as comfortable and easy as possible.
Participant interviews took place in 2023–2024 over the phone or over Microsoft Teams, so that young adults could participate in the way that was most comfortable for them. The approach to interviews was the same for both methods. All interview material was transcribed verbatim to produce written transcripts. We recognized that discussing palliative care with young people who are living with metastatic/advanced cancers requires tact and thoughtfulness on behalf of the researcher, to navigate a conversation about a service that is inclusive of end-of-life care with someone with whom there is none to a little pre-existing rapport. Our first author is a doctoral level student with over 15 years of experience working in adolescent and young adult oncology. Creating a respectful atmosphere for the interviews to be conducted was of upmost priority, recognizing that it is both a privilege and an honor to bear witness to these stories and to have someone take their time to participate in the study while living with an advanced illness. On the one hand, this involved starting the interviews in a conversational manner and supporting the participants for them to direct the flow of the interview. On the other hand, the interview was oriented to the question, “Can you tell me about the time you had a conversation with a healthcare provider around palliative or end-of-life care?” Additional questions were posed to guide the participant in sharing further experiential accounts and facilitate recall of their experiences (van Manen, 1997, 2016), and centered around asking the participant to walk our first author through their experience as it happened in as much detail as they could recall. While participants were not recontacted, preliminary drafts of the phenomenological text were shared with patient and caregiver partners (D.T., I.R.), recognizing these individuals have significant insights and understandings of young adults living with metastatic/advanced cancers. In addition to participating in the development of other aspects of the study (e.g., recruitment process, study documents), their feedback on the analysis supported the manuscript’s development. This approach was sensitive to progression in participant illness as well as that some of the participants passed away after they were interviewed. This activity can also be viewed as supporting the quality of the interpretative work completed.
Philological Methods
The resultant phenomenological text was constructed through engaging reflective analytic methods such as thematic reflection (e.g., whole text, line-by-line), exegetical reflection (e.g., literary sources), and linguistic reflection (e.g., tracing etymology, conceptual sources) (see van Manen, 1997 for an in-depth explanation of these approaches). These were used to explore the experiences shared in the interviews, and to support explicating direct and indirect meaning aspects of these conversational experiences. Exemplary phenomenological anecdotes were drawn from the interview material with limited editing to preserve the meaning of accounts yet also ensure intelligibility and anonymity. Throughout this text, anecdotes from the young adults’ experiential accounts serve as examples to support the reader to gain insights into the subjectivity of these experiences (van Manen, 2016; van Manen & van Manen, 2020). In this way, the aspiration was that these anecdotes have iconic validity, as plausible accounts of conversational experiences of young adults living with metastatic/advanced cancers (van Manen, 2016).
To conduct phenomenological research is to practice the art of phenomenological writing (van Manen, 1997, 2016), which began after the completion of the first interview. This process involved editing the resultant text through cyclical writing, reading, and re-writing. Max van Manen (1997) relates rigor in human science inquiry to the research text itself; rather than the application of research methods in a necessarily strict or uncompromised way. Appraisive criteria include principles of heuristic focus, rich description, interpretative insight, distinctness, and practice-of-meaning which ultimately are judged by the reader of the text rather than by following methodical procedural steps. For example, regarding the principle of distinctness, a text is said to have a rigorous focus if the text is guided by a self-critical question of distinct meaning of the phenomenon that is being described. This is achieved through the writing and rewriting of the research text. We, therefore, ask the reader to consider the rigor of this work based on their reading of the text itself. The text has been crafted with the intention to evoke and explicate understanding of an experience as it is lived through by exploring the meaning structures of this experience. The phenomenological text begins by introducing the reader into the world of the young adult and more specifically, the young adult living with metastatic/advanced cancer.
Ethical Issues
Permission to conduct this study was obtained from the university’s health sciences ethics review board. Several actions were taken to structure the study in a manner that mitigated risks and harms for participants. For example, careful selection of anecdote examples and omission or alteration of specific information that could be identifiable were strategies employed to diminish the possibility of participant identification. This included using language such as “a few” or “most” to describe demographic details pertaining to those who took part in our study, to provide the reader with an understanding of the characteristics of those who were interviewed while being cognizant not to identify specific individuals. In addition to this, the contextual information that participants provided with regard to hospital names, healthcare provider names, the age of their children, exact Canadian location, and so forth were not included. We also made the deliberate decision not to link the resultant qualitative material to individual participants by utilizing numbers or other designations. In keeping with the study methodological sources, we understand phenomenological inquiry as oriented toward iconic rather than empirical validity, whereby such designations do not add to the presentation of a phenomenological study intended to point to a plausible account (van Manen, 2016). Verbal consent was obtained from all participants, including the use of written consent documents. The consent process was supported by sending the documents to potential participants prior to the interviews with their consent revisited throughout their participation.
Analysis
Common to participants of this study was being a young adult and living with a metastatic/advanced cancer. Their bodily health had been compromised as they lived with vague discomforts, moments of pain, and more often than not tiredness. In this way, these young people were inhabiting ailing bodies, present to them as objects of provocation, worry, and uncertainty. Those day-to-day activities that embody young adulthood—early careers, intimate relationships, young families, aspirations for the future—had all been impacted on account of their cancer. Their taken-for-granted naiveté of time left ahead was lost. Celebrations, vacations, and other life events were now being planned with urgency. Idle time was being used to research medical conditions and treatments (surgeries, chemotherapy, radiation, and various medications). Clinics, hospitals, and other aspects of the health system had become habitual. Certain nurses, doctors, and other healthcare providers were familiar, acquaintances, confidants, or something like friends. It is from this first-person perspective that we approach what is it like for young adults living with metastatic/advanced cancers to engage in conversations about palliative care with healthcare providers: So, it was right after I was told I was Stage 4. I was nervous, and I was alone. And I usually go and see the nurse first before the doctor and one of the first questions I remember asking after we talked about all the other stuff. She was like, “Do you have any questions?” And I said, “Yeah, when can I access palliative care?” And, she laughed at me. And so that was my understanding: that I don’t need it. Yet, she’s like, “Why do you think you need that?” I said, “Well, because I’m stage 4 and I think I should have access to it.” And then she left, and it wasn’t discussed again, because I was embarrassed to talk about it.
What is it like for a young adult living with metastatic/advanced cancer to bring up palliative care to their nurse, physician, or other healthcare provider? What is asked in such questions? What is the meaning of the thoughts that are given words in such moments? And, of course, how may we understand such experiences when a question is brushed away, left unanswered, or not recognized in its meaningfulness?
While each young adult who participated in this study shared different perspectives and experiences of conversations with healthcare providers concerning palliative care, across these stories was a recognizable phenomenon. The following sections offer concrete experiential material from young adults alongside textual reflections orienting to the unique meaning of this lived experience: conversation as an experience of an opening for talk, conversation as an experience of need and relief, and conversation as an experience of reflection. We ask the reader to consider: What may the experience of having a conversation about palliative care be like for young adults living with metastatic/advanced cancers?
Conversation as an Experience of an Opening for Talk
So, my sister was sitting on the right and she had a binder, and she opened up the binder and she had a trajectory with a start, middle, the last … And she was sitting in front of the doctor, the doctor is angled towards me but she’s looking at my sister’s binder, and my sister’s like, can you point out where [sister] is? Is she at the beginning of her diagnosis, the middle, the last part of it? Or, is she at the end-of-life? And, she pointed to the last.
Across the participants’ stories were recollections of first conversations about endings. For some, a healthcare provider supported them to recognize where they were in their journey with cancer; for others, it was themselves, a friend, or a loved one who brought up the topic of palliative care. In such moments, we could say that palliative care was or was not pointed out, identified, or otherwise experienced as an appropriate topic for talk. For some, it was left hidden or unvoiced—we are not there yet. Other times, the topic was purposefully brought to the forefront. I just knew that sitting in that room, I wanted to fight cancer with every tool that I could find in my tool belt. I knew the doctor had a bunch of resources that she was going to present to me. But, I just wanted to make sure that everything was covered, and I remember reading an article … about having access to early palliative care, and how we need to advocate for that. So, that’s where my whole idea came from about talking about it. That was one of the main reasons why I brought it up, because I was doing research before I went into the meeting.
We may wonder, for a person who lives with advanced/metastatic cancer, what qualifies a conversation as one about palliative care? Should not all healthcare conversations be holistic? Should not all patients be deserving of care attentive to ameliorating suffering? Should not all care be palliative in a broad sense? A conversation about palliative care is an aperture to a kind of care that affords living and dying well with disease. In talking about “it,” we may appreciate that to a young adult the term “palliative care” names something that can be accessed or denied as a conversation may be opened up or shut down. I started talking about like, oh, I just wish I could know I only had this many years or this many days. And like, this was the day that it was going to happen. And then, he kind of was pressing, like, “Why is that so important to you?” He just flat out asked me like, “Why is this, kind of so, important to you?” And then, when I said that the reason why it was so important to me, because of how I wanted to leave the world. That’s when he started talking about it, and he was the one who brought it up. He’s like, “Well, have you thought about palliative care?” He had indicated, like, “I am more than happy to continue providing pain management for you.” Like, “Don’t feel it’s not something that I can do or something that I don’t want to do.” But, when we talked about sort of my rationale, he was like, “You know, that makes a ton of sense to me and you’re right. It’ll be a different level of access. So, if that would make you more comfortable, I support that decision.” And so, we kind of just went from there.
We can appreciate how deeply personal such conversations may be, and the normative need to respond positively to such conversations rather than pass over, dismiss, or shut them down. Dying as death is both a discrete event, a particular moment in time, and also what someone lives through. In this sense, we may understand conversations about palliative care as an opening to talk about time left in its existential sense: What is meaningful in death and dying? What is meaningful in living while managing an advanced cancer? How does one want to spend their remaining time? How does one want to leave the world? What does one consider as important for their legacy? In this fullest sense, conversations about palliative care afford the opportunity for a healthcare provider to introduce palliative care as a philosophy of care in addition to specialist palliative care offerings: “There’s, so much you can have access to. Social workers, psychologists, people who walk you through conversations about end-of-life, planning your like power of attorney and all of that.” Alternatively, it may provide understandings of treatment goals as affording quantity with quality of life (and dying): “The chemotherapy that I would be receiving would be palliative, not curative. That we’re not trying to like save my life. We’re trying to extend my life. We’re trying to give me quality of life.”
Though palliative care offerings vary throughout different health systems and geographic regions, a conversation about palliative care may serve as a recognition of a person’s suffering and a validation of the care they need through opening the gate to palliation. In this way, we can appreciate a conversation as an opening for further talk and further care, with a focus on living well. That’s when he’s like, “You know what? I have some pamphlets I can give you just so you can have to reference later.” And then he had handed and he’s like, “I’ll give those to you before you leave.” And that was kind of, yeah and he kind of left the door open like, you know, it’s because he could help me like if I don’t feel OK reaching out myself, he could help facilitate that as well.
Conversation as an Experience of Need and Relief
I was having issues that like impacted sort of my overall, kind of, day-to-day quality of life outside of chemotherapy treatment. I was feeling a little bit down and defeated because I was in a lot of pain, and I kind of felt like when you can feel the progression and it starts to impede your quality of life, like you really kind of feel like the cancer is winning. I was just in enough pain where having that conversation was essentially like me crying “Uncle!” I just couldn’t … She said that she would talk to the doctor about getting a referral if I was open to it, and I thought, “If I was open to it?” Like, obviously I’m open to getting better or getting relief or whatever.
We can appreciate the aggressiveness of cancer—“cancer is winning”—that affects the living heard in the manifold of oncology war metaphors (facing cancer, fighting cancer, battling cancer, surviving cancer, etc.). Young adults living with metastatic/advanced cancers are generally not anticipated to get better. There is a need for palliation. Palliation expresses alleviating symptoms, relieving suffering, or otherwise assuaging the effects of cancer without ultimately offering a cure, even though palliation can be offered alongside curative treatments. The etymology of palliation is from the Medieval Latin palliatus, literally “cloaked,” from past participle of Late Latin palliare, “cover with a cloak, conceal,” from Latin pallium “cloak” (Harper, 2001). Following, we can understand palliation as ensconcing care toward comfort. In other words, it is a responding to need to provide relief.
Amidst the unrest nexus of need and relief in those with metastatic/advanced cancers, the word “hope” stands out as a beacon signaling the prospect of change, reprieve, and peace. And yet, hope can mean different things to different people and vary by context. Young people living with cancer live Between Two Kingdoms (Jaouad, 2021), dwelling in the kingdom of the sick and the well (Sontag, 1978, para. 1). The lifeworlds they occupy comprise both medical contexts where they navigate a serious illness and also non-medical contexts where they inhabit the world as a young person. Moreover, it is not just that they may hope for relief from the bodily effects of cancer and treatments. They may hope for their partner, children, family, and friends. And yet, such hope cannot help but be tempered by uncertainty and pain: Who will take care of my parents after I am gone? How will my children remember me? What will my legacy be?
We may appreciate how a young adult’s sense of the future, life to come before and after they are gone, affects their experiencing of the world in the present. In this way, hope is an expression for anticipating a possible future from a present situation of being a young adult living with metastatic/advanced cancer. We may understand hope in this context as phenomenologically related to need and relief, whereby a conversation about palliative care expresses an understanding for need and relief over time. In other words, hope imbued by palliation affords the possibility for the relief of needs whether they be physical, relational, material, or existential. So, she left the room. My sister and I looked at each other with a sigh of relief. I think we may have said like, “What the F? Like, what the F? She gets it.” We clapped our hands. It was like a human conversation that we had. It was natural and relaxing, and I started crying as soon as she told me, “Yes, we can get you access.” It was just a weight off my shoulders. I just started crying cause like finally someone understood. I took a breath of relief and she said, “I get it.” She came back in the room. She had a form. She said, “I have a fax form that we just need to fill out, and we’ll send it to the local community palliative care team in your region.”
The hope for a young adult may be expressed as a hope for a future in which they can live well—however short or long such a future may be—until their last breath. Psychologically, we may say the young adult brings to a conversation their concerns regarding the fear they are carrying. Phenomenologically, the meaning is deeper: Because like that was another reason why I was also thinking about MAID [Medical Assistance in Dying]. I want to stay as close to like the person I am now, and I don’t want them to remember me when I’m like, super sick. So, it’s just like I want to go kind of on my terms and it’s just like I want to make sure that people can help me. So, I’m not just like a complete shell of myself, you know?
For a young adult, cancer may affect their sense of who they are in their present and their future. And they have present and future needs which may be deeply personal as they relate to who they are. Young adults voiced during these conversations a desire for their needs to be anticipated and their healthcare team to support them accordingly. Following, they expressed a need for healthcare professionals to walk the road with them on the journey to whatever may be their transition out of this world and into whatever may come next. As he was talking, because I’m very like if I have a plan, I feel better. So, like the way that he was explaining it to me and it’s just like what they can help with, it really put me at ease at the end. I felt almost like a relief, like a weight off my shoulder. And it just was also good knowing that I could rely on someone to help with those things that’s not my family. So, it’s not like an extra burden … She was concentrating on it, like this is what they can do right now, not eventually, this is what they can do ….
How a young adult copes with their illness and confronting their future varies. Hope is not a fixed entity, and how a young adult hopes in this context may vary depending on a variety of features: how they view their illness, how their disease has been progressing, their outlook on events, and so forth. In addition, their needs and what may offer them relief may differ. Still, across their words, we may tentatively say that the relationships young adults have with their healthcare providers are intertwined by hope realized in timely yet tactful conversations about palliative care.
Conversation as an Experience of Reflection
I was literally thinking that I am closer to dying than I realized … I know everybody is gonna die, but like, literally … now I’m thinking I’m dying and then he says, “We’re going to send you to the clinic.” He kind of brushes it off and then leaves before, you know, he always says, “Do you have any other questions and whatever?”
Most young adults are able to live their lives without an omnipresent awareness of their own mortality. Instead, they are “just” able to engage in their daily life, without being concerned by just how much time they may have left. While they may or may not take daily medication, few young adults need to concern themselves with the thoughts of participating in off-label clinical trials; of seeking out second, third, and fourth medical opinions; of researching new medications and other interventions; or, of otherwise actively engaging in efforts to find something that will bide them more time. Rather, a young person may be reminded of their mortality when faced with a health scare, when they lose a loved one, or perhaps if they are caregivers for someone with a serious medical illness. However, these moments of reflection concerning their own mortality tend to be momentary as exceptional or passing thoughts triggered by life events rather than a variably persistent presence.
Across the participants’ stories were implicit and explicit recounts of how conversations about palliative care were coupled with reflections on their dying and death, their own mortality. These moments served as an acknowledgement that these young people are “living condensed (Craig, 2015, para. 4).” That to varying degrees, their lives were expected to be shorter than others. The conversations can make death’s presence feel imminent; and for some, this experience was anticipated and acknowledged by their healthcare provider. Yet, we may wonder what happens when the door is closed and the conversation ends without these potential thoughts being acknowledged? What happens when the breadth or intent of palliative care is not explained? What are the existential consequences of not supporting a young adult with metastatic/advanced cancer to reflect on their dying and death?
A conversation around palliative care while inclusive of end-of-life matters may also explore other related aspects of care: quality of life, comfort, pain, worry, depression, faith, fatigue, legacy, and so forth. I do remember being like, surprised in that moment, because I didn’t know at that point that palliative care was anything other than sort of end-of-life … I was like, OK, I think that’s end-of-life. There’s nothing else we can do? … I didn’t realize that there was a pain management component.
In the life of a young adult, these conversations are not necessarily commonplace, and they may also not be so for the healthcare provider. For some young adults, they may present to the conversation without a clear understanding of palliative care offerings or how these services may be applicable to their own medical situation. Through the conversation, the provider has the opportunity to acknowledge the end-of-life aspects of palliative care explicitly and the misinformation that exists around it in society. I think she was aware that my mind was going to go there right away. Yeah, she definitely was like, “They do that end-of-life stuff, but you will work with them for many, many years and they’re great with pain management. They always have these great suggestions that we didn’t think about or like, we didn’t apply to that.” She explained it really clearly and it made me feel a lot better. So, I remember being surprised. She did say, “You know, we can have you introduced to them early, before it’s anything like that … You could get this relationship started and then you’ll like work with them … for years.” And she kind of said, “You know, it’s a bit like the name of it … I think it doesn’t apply the way that society thinks of it.”
Young adults may variably cope with their advanced cancer diagnosis, and have varied thoughts and reflections on life, death, and dying. The point is the conversation serves as a space for reflection as both death and dying may be explored, questioned, or acknowledged, where the young adults may have space and time to explore difficult questions around their thoughts. This is when I asked the question about timeline for survival … I asked my oncologist, “Like if this is a four-quarter sports game, like what quarter are we in?” And she was able to indicate like, “Well, we’re probably like halfway through the second,” which gives me a bit of an idea of where I am in the trajectory versus what that means timewise. I was crying hysterically a little bit. It’s a really tough experience to be in. To have people telling you, you know, the nurse never says like you’re dying. I don’t have any active lesions or anything right now. But then, they keep saying like, “Your medicine will stop working eventually. You know, eventually it will go somewhere else. It will spread.”
Even with a diagnosis of metastatic/advanced cancer, there is a living with uncertainty: When death will occur? What death will look like? What will the future hold? Discussing palliative care can bring to the forefront of a young adult’s mind existential thoughts, questions, and reflections concerning the likelihood of their survival and longevity: “I’m like, I’m not stable. I’m not. It’s not shrinking, it’s progressing. Let’s be realistic here and let’s plan for the for the worst as years to come.” I was in my apartment. I was probably sitting on my bed, I think. So, that was sort of my first interaction with palliative care was my doctor just sort of off-handedly saying something like, “All your care is palliative now.” And me … I didn’t realize that at that point. It was like, “What? What do you mean it’s palliative now? Like, I don’t want that. That means I’m gonna die. I don’t wanna die!”
For a young adult, a conversation about palliative care may confront the meaningfulness of a life lived and a life ending. So, in this lived world of dying and death, we need to consider how to support young adults in their living and their dying with metastatic/advanced cancers.
Discussion
Our research with young adults living with metastatic/advanced cancers shows the meaningful significance of engaging in conversations with healthcare providers about palliative care. It specifically addresses lacunae in our understanding of the experiences of young adults living with metastatic/advanced cancer accessing palliative care in the adult healthcare system. To be clear, the aim was not to draw empirical claims or generalizations of all conversational experiences. Instead, we offer possible understandings regarding the meaningfulness of this experience for a young person living with metastatic/advanced cancer, a perspective that had not yet been explored in the literature (Drake et al., 2021, 2023). From reflecting on this work and the existing literature, we can draw considerations for practice.
Considerations for Practice
Considering Timing
From understanding a conversation as an opening for talk, these conversations about palliative care may provide opportunities to discuss timelines, worries and concerns, goals of care, and other aspects that may be important for a young person. North American guidelines for adolescents and young adults recommend that these young people receive the early integration of palliative care with their standard oncological care (Abdelaal et al., 2021). To begin such conversations at the time of diagnosis may help ensure that these discussions take place in a timely manner (Sansom-Daly et al., 2020; Wiener et al., 2015), thus aligning with the import of creating an opening for conversations to address unique challenges the young person may be experiencing. We would be amiss not to acknowledge that some participants described needing to advocate for these conversations with their healthcare providers, and that, at times, these conversations were not supported despite being desired. The literature highlights how poor psychosocial care at the end-of-life can have a negative impact on the young person (Sansom-Daly et al., 2020). Additionally, the impact on a young person of having to advocate for their own access to palliative care needs to be thought of when considering the timing of these conversations.
Supporting Hope and Control
In comparison, from understanding conversation as an experience of need and relief, we may realize the importance of supporting young people’s need for hope and sense of control. Acknowledging this can help one understand the import of anticipating, identifying, and addressing physical, relational, and existential needs of individuals living with their metastatic/advanced cancer. This may include a plan for care that supports young people having hope and control over their illness to ensure their care aligns with their values to live well through the time they have left. From the broader palliative care literature, we can understand that hope plays a pivotal role in how families cope with challenging events (Laranjeira et al., 2022). The literature on adolescents and young adults living with advanced cancer has found that the role of hope may change for the young person throughout the trajectory of their cancer experience (Bennett et al., 2022). This couples with our understanding of the need for communication to be honest regarding prognosis and decision-making (Sansom-Daly et al., 2020), acknowledging that hope may be influenced by information provided and available supports (Laranjeira et al., 2022). Attentiveness to experiences of need, the language in conversations, and the hope that young people may live with and how this may vary over time, are key considerations.
Exploring Complex Topics
From understanding conversation as an experience of reflection, we may appreciate the significance of the support that these young people may need to be afforded. It is also important to acknowledge that when providing this support, a dichotomy may exist between a conversation serving as a source of hope and also a moment to reflect on their fear of dying or death. Being categorized as “palliative” can present an omnipresence of thoughts around disease progression and dying young (Avery et al., 2020a). We may appreciate that when these conversations are shut down, which may happen for a variety of reasons, the young adult may experience distress over their concerns not being addressed (Sansom-Daly et al., 2020) or otherwise unwelcomed. Our work may be read as supportive of research that highlights the importance of these conversations to be delivered by a member of the team with a strong rapport with the young person, who is comfortable exploring and navigating such complex topics (Sansom-Daly et al., 2020).
Seeking Support
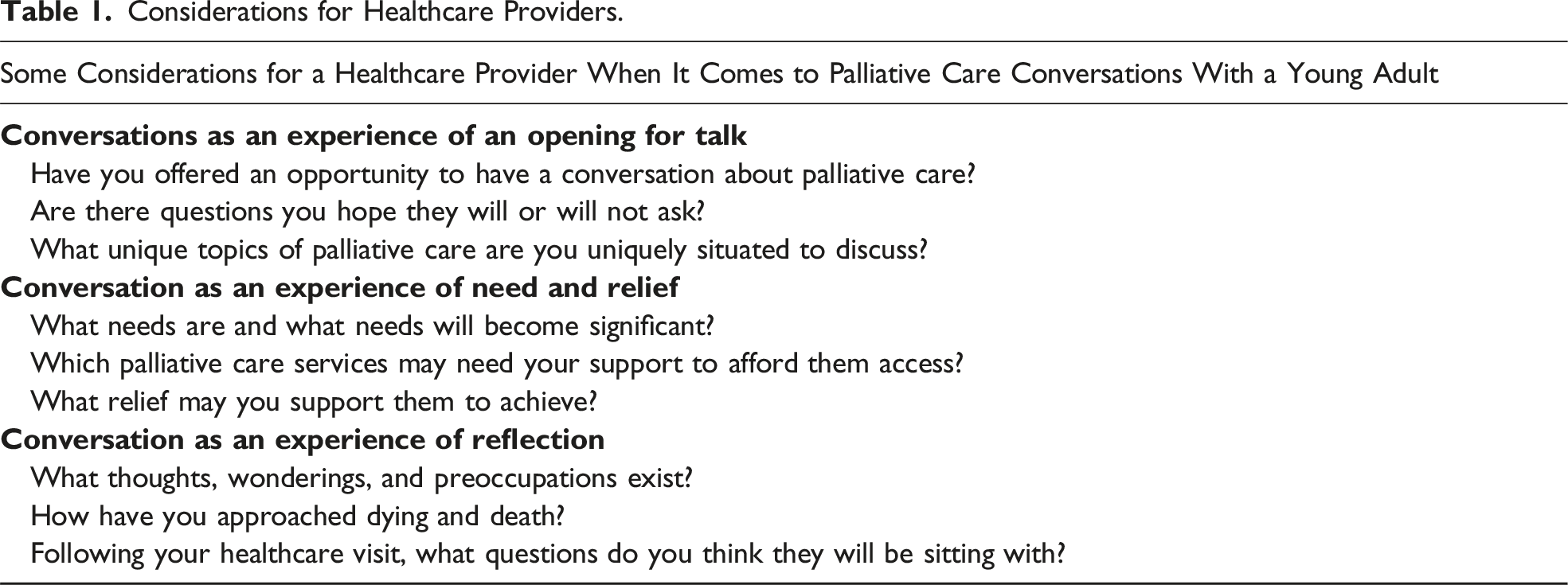
Considerations for Healthcare Providers.
Considerations for Future Work
It is important to acknowledge that the focus of this study was on young adults living with metastatic/advanced cancer engaging in conversations about palliative care with their healthcare providers. This is only a small part of the larger and varied palliative care journey for young adults living with these difficult diagnoses (Rosenberg & Wolfe, 2013). The experiential material collected was limited to the stories of those who felt comfortable recounting their experiences and included several participants who advocated or attempted to advocate for their access to this care. It was not required that participants were accessing palliative care services to take part in our study. Experiences related to the referral process beyond initial conversations, the receipt of palliative care services, pursuing experimental medical interventions, and other phenomena that compose the broader experience of advanced/metastatic cancer were beyond the focus of this study yet may nonetheless be deeply significant (Drake et al., 2023; Lockwood et al., 2021; Rosenberg & Wolfe, 2013). These topics would benefit from research and foreseeably resource, guideline, and policy-development (Drake et al., 2023; Sansom-Daly et al., 2020). Finally, it was clear from speaking with the young adults how emotionally challenging and taxing it may be for them to navigate adult health services and information about their conditions, in addition to the daily symptoms that they live with. Further research into how we can better support young people living with advanced cancers and their access to care could help alleviate some of the suffering that they experience through the necessity of frequent and intense self-advocacy efforts. Consistent with this is the need for future research that attends to supporting their partners, children, and other family members (Drake et al., 2023; Tutelman et al., 2019). In consideration of these efforts, understanding how gender, race, and other social constructions impact the receipt of care and self-advocacy efforts should be explored from a social justice perspective (Cheung et al., 2021).
Conclusion
Understanding the conversational experiences of young adults living with metastatic/advanced cancers is pertinent for young adult health researchers and the tapestry of understanding in this research area. This knowledge provides understandings necessary for those who provide care for these individuals and are able to offer or refer them to palliative care services, so that they can act with tact to provide young adults support, access, and dignity in their care.
Footnotes
Acknowledgments
[Emily K. Drake] is a Killam Laureate whose doctoral work is supported by the Canadian Cancer Society, Nova Scotia Research and Innovation Graduate Scholarship, and the Faculties of Health and Graduate Studies at Dalhousie University. She is a trainee in the Cancer Research Training Program of the Beatrice Hunter Cancer Research Institute, with funds provided by the QEII Foundation. This original study will contribute toward [Emily K. Drake]’s doctoral degree. We thank the young people who took part in this study for sharing their experiences with us.
Author Contributions
This original study will contribute toward Emily K. Drake’s doctoral degree. She contributed to the conception of the study, development of the study protocol, data collection, production of the phenomenological text, and led the preparation of the article. L.E.W., M.v.M., D.T., I.R., and J.C. contributed to the conception of the study and the study protocol. All authors provided feedback on the interpretation of the findings and read and approved the final article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michael van Manen is a Deputy Editor of Qualitative Health Research. He was not involved in any part of the peer-review process, and the manuscript was subject to the same standard of peer-review as others submitted to the journal. This includes the input of two or more independent peer-reviewers who were blinded to the author’s editorial association with Qualitative Health Research. All other authors report no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: [Emily K. Drake] was supported in this study by doctoral funding from the Killam Trust, the Canadian Cancer Society, the Nova Scotia Research and Innovation Graduate Scholarship, Dalhousie University, and the Beatrice Hunter Cancer Research Institute, with funds provided by the QEII Foundation [grant numbers not applicable].