
Abstract
This study explores the practice of healthcare support workers (HCSWs) working with people with dementia on mental health wards for older people within the National Health Service in the United Kingdom. People with dementia in these settings have complex physical and mental health needs with significant behaviors that challenge and therefore require high levels of staff expertise to meet their needs. Underpinned by the theory of care aesthetics, our primary aim was to raise the visibility of HCSWs’ everyday practice in this under-researched area of dementia. Working with three mental health wards over two sites, we used an exploratory, participatory action research methodology with qualitative and ethnographic methods to refine and clarify our understanding of care aesthetics in this practice setting. Over the course of the study, and through a series of collaborative learning groups in each site, we developed an explanatory practice model applying constant comparative analysis to the data to ensure that each stage of the model was iteratively developed and refined with the participating HCSWs. The model demonstrates how HCSWs use sensory, embodied, and relational practice to effectively “tune in” to the person with dementia, to the ward and their colleagues, to themselves and their values, to their craft, and to ward visitors. Being co-present was a resulting linking schema that demonstrated high-quality in-the-moment person-centered care. The model illustrates the range of everyday practices delivered by HCSWs and how care aesthetics has the potential to inform and develop the language of person-centered dementia care.
Keywords
Introduction
In the United Kingdom (UK), it is estimated that around 1 million people live with dementia, with that figure set to rise to 1.2 million by the year 2040 (Livingston et al., 2020). As the literature and demographic trends suggest, most people with dementia prefer to remain at home and in a familiar neighborhood network (Alzheimer’s Society, 2014; Keady, 2024). However, as the disease progresses to its more advanced stages, additional care is needed and some people with dementia move into a care home or other assisted living environment (Alzheimer’s Society, 2014). A smaller number of people with dementia are compulsorily admitted into National Health Service (NHS) mental health wards for older people, often under a section of the Mental Health Act (1983), for an assessment of their dementia because of the complexity of its presentation and the potential risk to the person or to others (Edmans et al., 2022; Jones et al., 2023a, 2023b). These specialist wards are usually located in NHS Mental Health Trusts and operate as locked environments of care, with entry and exit to the ward secured and under the control of ward staff. Wards may be structured either as “dementia-only” or “mixed,” with the latter also providing care to those with functional mental health conditions, such as late-life psychosis (Pinner et al., 2011). Admissions to mental wards for older people come from general hospital wards, care homes, and domestic homes (Edmans et al., 2022). Following a period of assessment and intervention, and an associated reduction in risk, patients are discharged to the most appropriate location; this is most often a long-term care setting, but for a smaller proportion of patients, this could be a return to the domestic home (Edmans et al., 2022).
The literature also reveals that such compulsory admissions result in a high level of stress for family members who undergo a transition of role identity from that of primary carer to ward visitor (Partridge et al., 2025; Wolverson et al., 2023). As Partridge et al. (2025) go on to suggest, for family carers of people with dementia, this abrupt change requires additional understanding and support as families are often undergoing traumatic pre- and post-admission experiences and uncertainty over where their relative will be discharged to. Despite the complexity and vulnerability of people with dementia admitted to these wards, and the impact on family carers, these environments of care have largely been overlooked in research practice (Jones et al., 2024; Partridge et al., 2025; Ross & Dexter-Smith, 2017; Wolverson et al., 2022).
Mental health wards for older people are staffed by ward-based staff, such as mental health nurses and healthcare support workers, as well as a broader multidisciplinary team (Edmans et al., 2022). In the UK, the term “healthcare support worker” (hereafter HCSW) is an umbrella term used to represent a range of “unregistered” healthcare support roles, including healthcare assistant, nursing auxiliary, and occupational therapy assistant, who work under the supervision of “registered” staff such as mental health nurses and allied health professionals (Griffin, 2023). HCSWs account for nearly 28% of the NHS workforce and are notable for the high-patient-facing nature of their roles (Griffin et al., 2024). On mental health wards for older people, HCSWs represent the largest staff group, with more HCSWs on a given shift than mental health nurses (Edmans et al., 2022).
In terms of training in the United Kingdom, while “registered” staff are taught on university courses adhering to national regulator guidance (e.g., Nursing & Midwifery Council, 2023), HCSWs as “unregistered” staff have no mandatory and standardized training, with most learning on-the-job from working alongside role models, by attending in house training, and through supervision from registered staff (Griffin, 2023). Several influential reports have highlighted that regulation, training, and development of HCSWs needs to be improved (Cavendish, 2013; Francis, 2013) but also that this staff group has significant untapped potential (Palmer et al., 2021). The Care Certificate was launched in 2015 to provide minimum standards for training, supervision, and assessment for staff new to health and social care (Skills for Care, 2025), and this includes standards relevant to mental health and dementia (Peate, 2016). While many NHS Mental Health Trusts have adopted the Care Certificate, this remains voluntary and inconsistencies in support and training remain for HCSWs (Palmer et al., 2021).
Given their high rate of patient-facing duties and the associated impact on the patient experience, there is a surprising lack of research exploring the training, skills, and roles of HCSWs in mental health wards for older people. For example, a recent qualitative systematic review of the literature on HCSW practice with patients with dementia on NHS acute and mental health wards for older people (Kindell et al., 2025) found only 19 published articles, with many studies stemming from the same data set(s). The review highlighted the crucial role that HCSWs have with personal care, such as washing, dressing, and feeding people with dementia. While there were similarities in HCSW everyday caring practices between the acute and mental health wards for older people, Kindell et al. (2025) drew the conclusion that, owing to the level of risk and behaviors that challenge experienced by people with dementia on the mental health wards, HCSWs required: A high degree of skill in communication, including verbal skills as well as embodied interactional skills such as facial expression, movement, touch etc., to maintain a person with dementia’s dignity and cleanliness and to provide for their physiological and safety needs. (p. 11)
Although the Care Certificate identifies standards for communication, we would suggest, this lacks a focus on the higher levels of interactional expertise needed for frontline practice with people with dementia admitted to mental health wards for older people.
Focusing on the sensory, embodied, and relational practices required within personal care and other health-related tasks aligns closely to the field of care aesthetics (Thompson, 2022), which draws on feminist care ethics to shine the brightest of spotlights on the importance of the micro-practices of care, such as touch, tone of voice, and bodywork. Here, “aesthetics” is used to refer to the experience of all the senses within the care relationship, not a narrow idea of how something looks (for an exploratory application of care aesthetics to dementia care practice, see Campbell et al. (2024) and Jones et al. (2024)). Care aesthetics, therefore, builds on the care ethics literature exploring the broader field of care (e.g., Mol et al., 2010) and the sociology literature that addresses the place of bodywork in health and social care (e.g., Twigg et al., 2011), with an aim to draw out and study in detail the sensory, embodied, and relational aspects described within these fields. In terms of HCSWs, this allows for exploration of skills that have been learnt and crafted over time through on-the-job experience in direct patient contact, a lens that is outside of the traditional NHS hierarchy in terms of qualifications and pay grades.
At present, there is no model of care that captures HCSW practice for people with dementia on the mental health wards for older people or positions their work within a theoretical and/or relational framework. This study therefore aims to provide a first step in this direction by (i) making visible the invisible aspects of HCSW care practice through the detailed lens of care aesthetics and (ii) inductively generating a practice development model that focuses on everyday HCSW care practices in this specific ward setting.
Methods
Interdisciplinary Research Team
Before further outlining our methods of study, it is important for us to share two positions. First, this reported NHS case study is one of four nested within a wider, three-year Arts and Humanities Research Council–funded research project called The Care Aesthetics Research Exploration (CARE) project, drawing together researchers from the arts and health with an overarching aim to integrate their complementary expertise across the project; see https://www.creative.manchester.ac.uk/research/creativity-health-wellbeing/care-aesthetics-research-project/. The other case studies on CARE are (i) arts-informed care home work for people with dementia, (ii) homecare workers visiting older people at home, and (iii) the aesthetic practices involved in the distribution of food to excluded communities. Second, this NHS case study was conducted by a multidisciplinary team that brought together theatre and arts practitioners (KM-R; RP; and JT); academic clinicians with experience in working with people with dementia admitted to mental health wards for older people (JK and JDK); clinicians specializing in dementia care (RE and RW); and academic and applied expertise in care aesthetics (JT).
We wanted to explore how HCSWs used their bodies and communication skills in their everyday practices with a curious and open mind. Importantly, the two full-time researchers employed to conduct the data collection with the HCSWs were post-doctoral performing arts specialists in dance (KM-R) and theatre (RP) practice, respectively, with skills in studying embodied and sensory practice. This allowed for detailed, open, and non-judgmental documentation of practice, not anchored to a certain positionality on the meaning and application of “health.” Data analysis throughout was conducted by the full research team drawing from both the arts and health.
Study Recruitment and Sample
This 20-week study took place between March 12 and June 12, 2024, and across two identified NHS Mental Health Trust sites in the North of England. Three separate mental health wards for older people took part in the study: site 1 comprised one “dementia-only” ward and one “mixed” ward; site 2 comprised a “dementia-only” ward. Inclusion criteria for HCSWs to take part in the study were (i) HCSWs with active support worker roles on the ward, including nursing assistants, occupational therapy assistants, and activity coordinators; (ii) those employed in a substantive or casual post in the participating NHS Mental Health Trust (i.e., full time, part time, or regular agency role); and (iii) those with an ability to attend a minimum of three collaborative learning groups (CLGs; Clarke et al., 2011). There were two routes into the study for HCSWs, either by face-to-face contact from the researchers (i.e., KM-R and RP) or by invitation from clinical staff who had agreed to support the study. Following this, five experienced HCSWs in site 1 were consented into the study and four at site 2, all of whom attended and contributed toward the arranged CLGs. There was a higher proportion of male HCSWs at site 2. To ensure patients were not disadvantaged by the research taking place, “backfill” monies were provided by the study budget to pay for HCSW staff replacement costs on the participating wards.
Data Collection
Summary of Methods of Data Collection
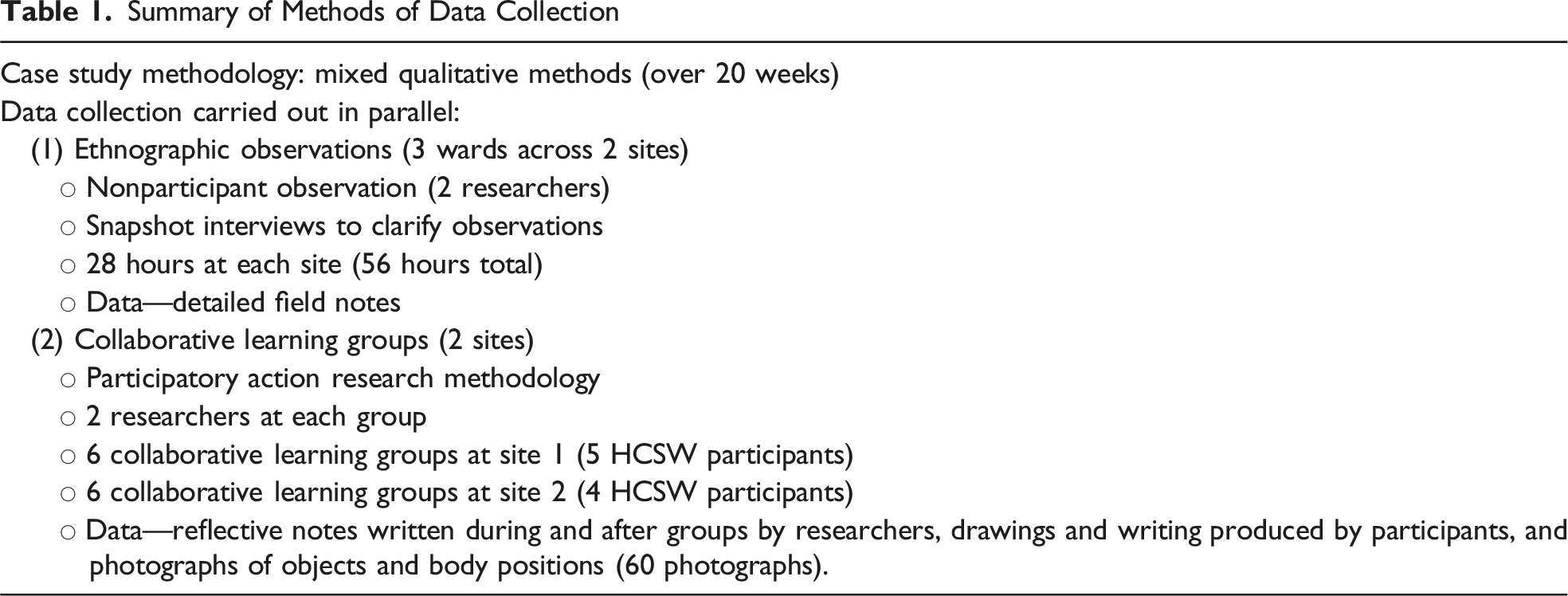
In total, and outside of the CLG activities, the researchers conducted 28 hours of HCSW observation at site 1 and 28 hours at site 2. The ethnographic observations were further enhanced in the form of snapshot interviews conducted by the researchers during real-time situations on the ward to clarify and better understand what was being seen at the time (should the conditions and patient care priorities allow). Observation notes were used as the basis of activities for the planned CLG sessions.
HCSW Collaborative Learning Groups: Structure and Activities
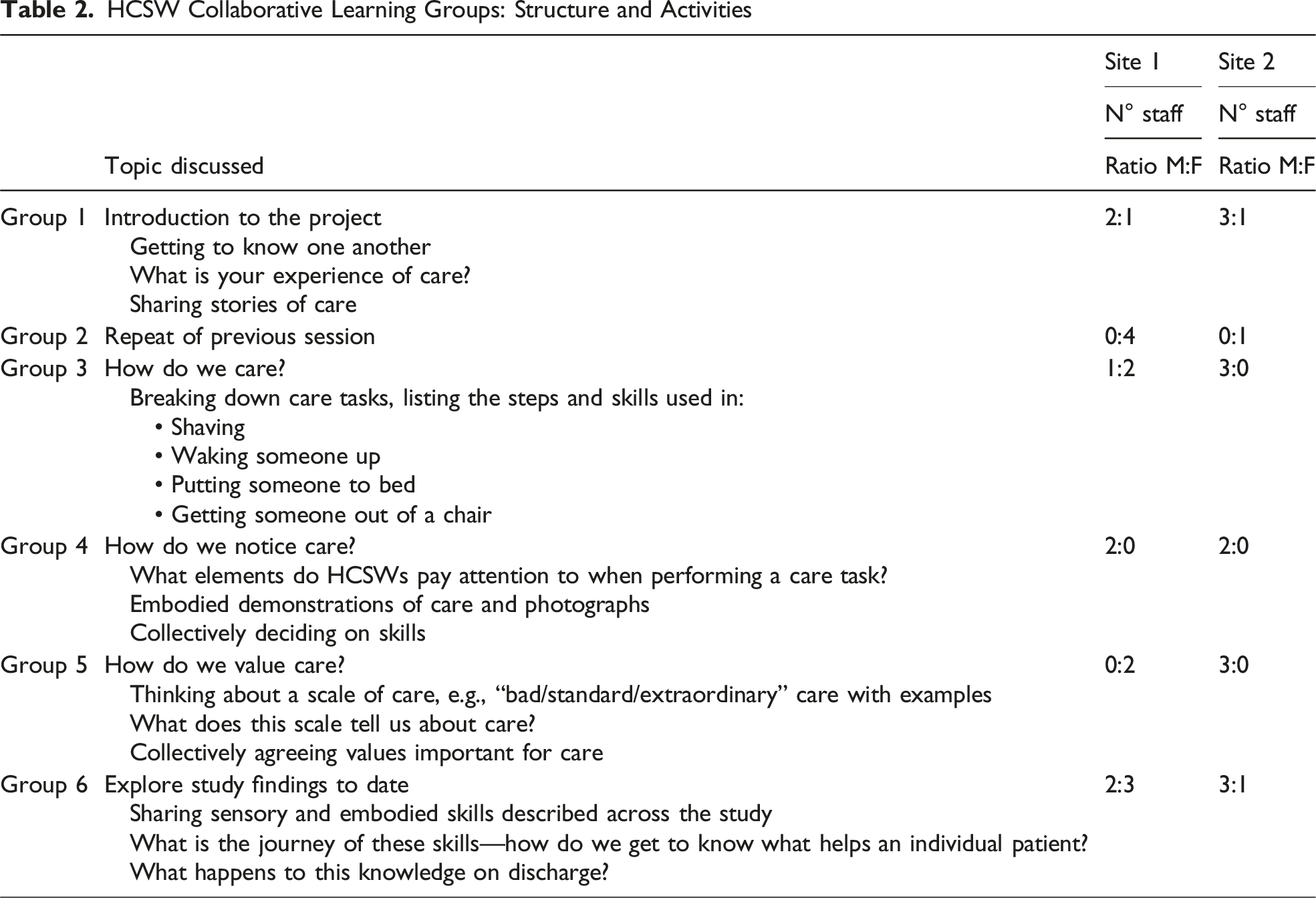
Both researchers kept reflective notes during and following each CLG, and these notes were used as data. All CLG outputs produced by the HCSWs and the researchers were collected at the end of each session and transcribed. Summaries of these transcriptions were used at the start of the next CLG session as a reminder of previously undertaken work and as part of the data set for constant comparative analysis (Glaser, 1978; Glaser & Strauss, 1967).
The two researchers engaged in reflective sessions after each ward visit, to sense check the data and gather any additional insights. Members of the research team met weekly across the 20-week study to discuss any issues arising from the research work, including the experiences of the two researchers on the mental health wards for older people, and conduct emergent data analysis.
Data Analysis
All data were transcribed together with the narrative descriptions of the photographs. Over the course of the study and led by the method advocated by Glaser (1978) to produce an explanatory model that had the potential to move over time, constant comparative analysis was applied to the data set to ensure that each stage of the model was iteratively developed and tested/refined at subsequent points of contact with the HCSWs. Data analysis was initially undertaken through a team approach at each of our weekly in-person meetings so that the emergent findings could be taken back to the CLG for agreement and refinement at the start of the next session. Figure 1 outlines this cyclical process. Cycle of Data Collection and Analysis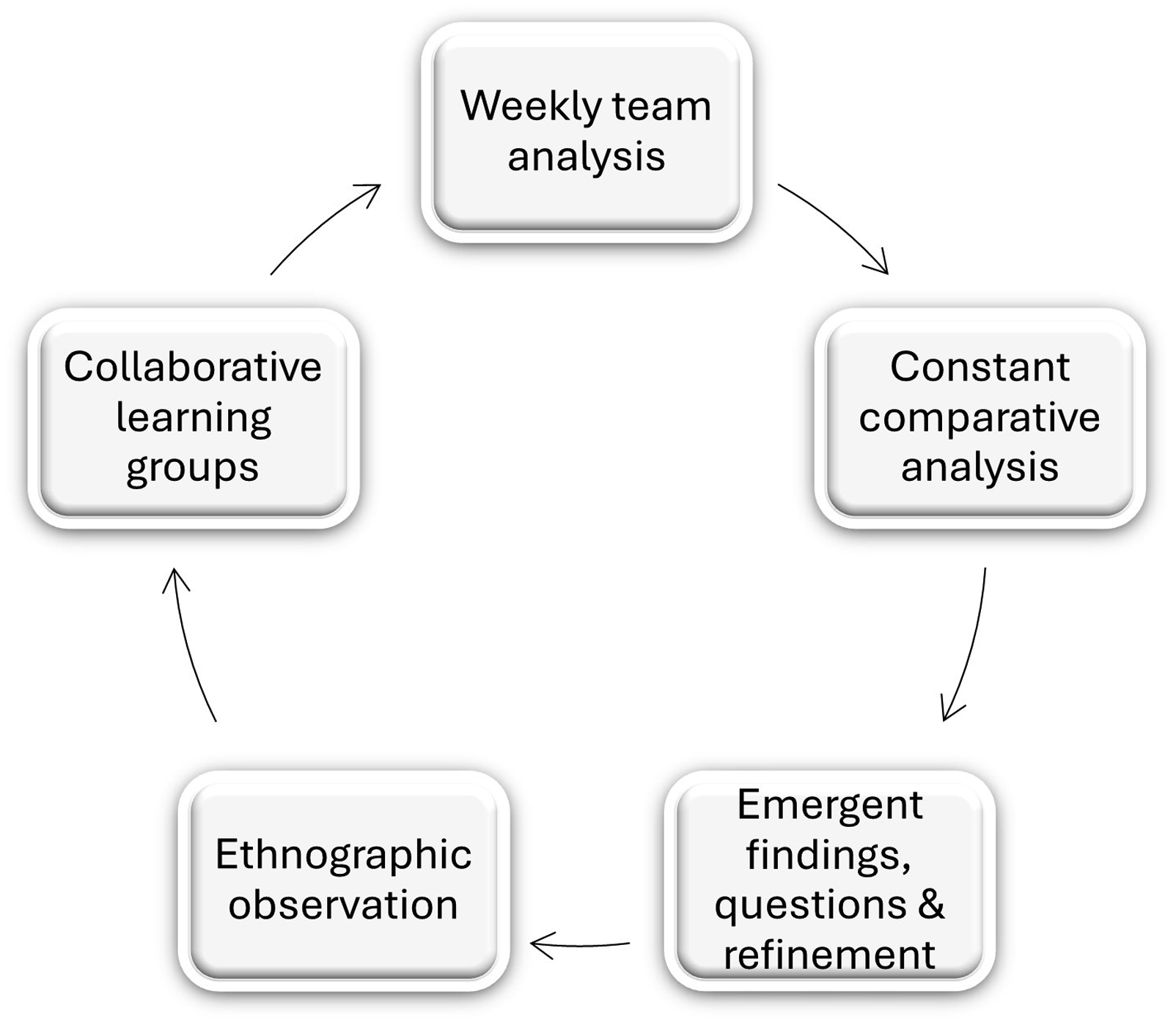
The team approach to analysis also enabled clarification of any points of (mis)understanding of what was being seen and coded in the data from our different professional perspectives and professional/clinical/academic languages. This team approach to analysis continued from sessions 2 to 6 (see Table 2). The HCSW practice development model that emerged from this process is shared in Figure 2 at the start of the Findings section. Healthcare Support Worker Practice Development Model: Everyday Care Practices for People With Dementia on NHS Mental Health Wards for Older People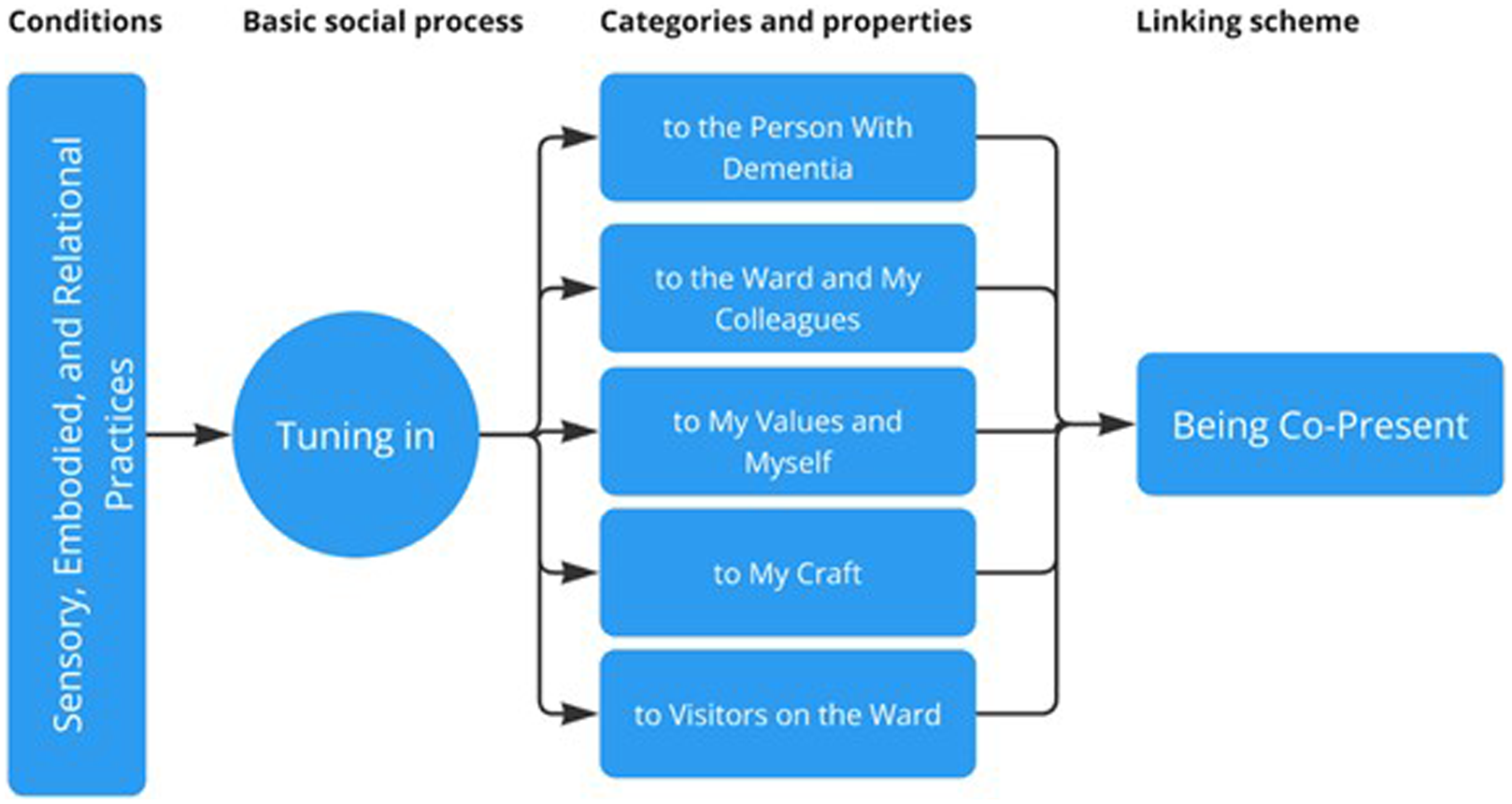
Ethics
This study was approved by NHS Health Research Authority and Health and Care Research Wales (reference number 23/NW/0335). All ward and participant names are anonymized in this article in line with research protocol and ethics permission. All participants provided written informed consent prior to enrolment in the study.
Findings
Figure 2 shares the HCSW practice development model that emerged to define everyday practices with people with dementia admitted to NHS mental health wards for older people. Each of these separate but interconnected stages will be defined and explored in turn, starting on the left of Figure 2 with “sensory, embodied, and relational practices” and then moving across the figure to “being co-present.” In our model, and with all the stages in the model working in harmony, “being co-present” is the descriptive meaning and practice outcome that HCSWs strive to achieve in their everyday work with people with dementia admitted to NHS mental health wards for older people.
In the supporting writing in the Findings section, a key relating to the data strands is provided along with the date this was collected; for reference, this is: S1 (site 1), S2 (site 2), Ob (observation data), CLG (data from CLG), and Rf (reflection sessions). Both main researchers will be referred to by their initials, and, at times, we refer to the CLG number (1–6) where the data strand was located. We will also use the terminology “person with dementia,” “people with dementia,” and “patient with dementia” depending on the situational context and shorten the location of the site of the research to the “ward.”
Sensory, Embodied, and Relational Practices
As we saw throughout the duration of the research and the final data set, the sensory, embodied, and relational practices of HCSWs with people with dementia on the mental health wards for older people have their roots deeply embedded in care aesthetics (Thompson, 2022). These attributes are positioned in Figure 2 as the foundational conditions of HCSW practice and are the building blocks upon which all other components of the model are built, interact, and intersect. These sensory, embodied, and relational practices included examples of HCSWs: observing and responding to the subtle changes in the facial expression of the person with dementia; using touch to soothe and/or feel if a person with dementia is cold or requiring additional help with personal care needs; and bending their head to make eye contact with the person with dementia. HCSWs were also seen to use their bodies in various ways, for instance, by kneeling down to be on the same level as the person with dementia; shielding others on the ward; linking arms together; stroking or rubbing shoulders; and holding hands with the person with dementia.
As seen in the data and in discussion, some movements were to do with conducting personal care tasks, such as feeding, shaving, and dressing the person with dementia, or helping the person with dementia to the toilet, while others were used to brighten someone’s mood, to be alongside the person with dementia, or to support the safety of others. Voice was also used in different ways by HCSWs, most notably through verbal communication, but also by humming and singing, responding to changes required for those on the ward with a hearing loss, and calming someone with dementia who was distressed. These practices were not performed in isolation of one another and were accomplished through a dynamic sensory register that was grounded in interaction with others.
Tuning in
Using the language of Glaser’s (1978) approach to mid-range theory building, “tuning in” is a basic social process that represents the continuing ability of HCSWs to use all their senses [hearing, touch, smell, taste, sight], intuition, experience, and accumulated knowledge, to tailor care and decision-making to a range of stakeholders on the ward, including to the person with dementia. This innate ability for HCSWs to “tune in” is present both “in the moment” and through planned activities of care. “Tuning in” also exists within and across each of the categories identified in Figure 2, as we will now further illustrate.
Tuning in … to the Person With Dementia
Within this first category, there were multiple and overlapping properties that supported HCSWs “tuning in” to a particular person with dementia on the ward, including understanding their experience “in the moment”; making sense of information from their life story; reading and responding to behavior; and communicating and connecting with the person’s everyday lives. In their ability to “tune in” to the person with dementia, HCSWs displayed a practical and empathetic stance that took account of how the lived experience of dementia affected that person’s quality of life and well-being, as this exchange between two HCSWs demonstrates: Mike: It’s frightening for patients having two to three people changing your pad [continence aid]. Claudia: Yeah … you’re going to be thinking, “I’m going to be raped.” (S1.CLG. April 30, 2024)
In this quote, Claudia demonstrates how a person with dementia may misinterpret the situation within such an intimate care task. Moreover, her reference to rape indicates the depth of fear that may be experienced by the person with dementia in that care moment because of this misidentification, and the need, therefore, for HCSWs to take this into account.
“Tuning in” to the person with dementia on the ward also included playful encounters and the everyday use of banter and jokes designed to make the person with dementia laugh. In addition, as delivering personal care and dealing with behaviors that challenge on the ward were daily occurrences for HCSW, they often spoke about the risks involved in undertaking their role, such as being unexpectantly hit by a patient and/or subjected to verbal abuse. “Tuning in” was therefore considered integral to the HCSW role and knowing when to step forward, or step back, during interactions with the person with dementia on the ward.
HCSWs often spoke about the importance of respecting the person with dementia’s experience of lived time and their belief that they were elsewhere and fully engaged in (past) everyday tasks and activities. On one occasion after concluding a CLG (number 4; see Table 2) in site 1, the researchers reflected on the improvisational and performative nature of this “tuning in” process: KM-R: During the CLG today, a HCSW gave such a beautiful example of a patient on the ward handing them [the HCSW] a fish while the patient was “fishing” by embodying those actions as if he were sitting on a riverbank casting off. In our reality, it was an invisible fish that he [the patient] handed to the HCSW, but the important point was that the person with dementia then expected the HCSW to do something with that invisible fish. But the patient made sure the HCSW didn’t just throw the invisible fish away because, of course, it was not invisible to the person with dementia, and he was “fishing.” The HCSW then had to interact and improvise a performance with the person with dementia with this little invisible fish in their hands.
As well as previous hobbies and pastimes, HCSWs also spoke about the need for “tuning in” to the past occupation of the person with dementia on the ward—what the HCSWs in our study called the patient’s “work mode.” To illustrate this further, Claudia, an HCSW, gave an example of a female patient on the ward who used to be an office cleaner, and that she [Claudia] would acquire products from the ward cleaner’s trolley to enable the patient to have her own bucket and cleaning products. Claudia went on to explain that when the patient was cleaning, she [Claudia] would say “Oh, you missed a spot there … Better go back to that or it might be noticed” (S1.CLG. March 26, 2024). For HCSWs, working with people with dementia whose life stories moved in and across place and time, “tuning in” to the person with dementia required sensitive and detailed observation of behavior, alongside knowledge of the person’s life story to understand the perspective of the person with dementia in that moment in time and then how best to respond.
Tuning in … to the Ward and My Colleagues
The category of “tuning in to the ward and my colleagues” groups together practices that relate to the broader ward context, including knowing the physical layout and routine of the ward; noticing changes in the ward atmosphere; working as part of a team; and educating others about the HCSW role and their practice. As HCSWs are required to manage the needs of multiple patients on the ward, “tuning in” to knowledge about the ward layout and its everyday routines was crucial in maximizing caring practices and patient well-being, as this researcher observation highlights: Food is arriving on the ward in a big metal block on wheels. Suppertime is early. Kevin [HCSW] walks by, points to a person with dementia in the dayroom, and says to a colleague: “He likes milky coffee.” Kevin then disappears down the hall. Behind me, the living room fills with chatter. A patient’s cheery voice cuts over the television. The chatter echoes down the hall, where I sit. I move to the lounge. HCSWs and other staff buzz around patients who are sitting quietly at tables. Trays are checked, folders are scrolled through. Kevin is handling utensils and trays with a kitchen towel; they must be hot. (S2.Ob. June 5, 2024; RP)
HCSWs were frequently seen to support each other, including those with different roles on the ward, and had a strong sense of teamwork. Similarly, during their periods of observation, the researchers noticed more experienced HCSWs “tuning in” to help less experienced colleagues perform personal care, as this example illustrates: She [experienced HCSW] is looking on and working in tandem with the new HCSW at the table who is feeding a patient. She is overseeing, instructing and advising like the coach on the sidelines during a football training session. (S2.Ob. April 30, 2024; KM-R)
HCSWs were also observed to be highly adept at “tuning in” to the ward atmosphere and being able to tailor their care to account for any “felt” changes in it. For instance, during a music-making session with people with dementia on the ward which had seemingly rendered it “calm,” an HCSW took advantage of this atmospheric shift to feed a participant with dementia who had shown little interest in eating for several days, as this observational record reveals: She [HCSW] leaves the music group and then returns holding a cup and a spoon. She stands in front of the patient, swaying to the new tune, and brings the spoon to his lips. The patient is grinning up at her. The HCSW continues to sway to the music, feeding him a spoonful of food every 30 seconds or so, taking her time, singing along, until the cup was empty. (S1.Ob. April 23, 2024; RP)
Such anticipatory care demonstrates the importance of relational practices and the personal knowledge that HCSWs need to “tune in” to different sensory registers to meet the specific needs of patients with dementia on the ward.
Tuning in … to My Values and Myself
During the CLG sessions across both sites, HCSWs often discussed the importance of “tuning in” to [their] personal values, with a need to maintain respect for, and the preservation of, the patient’s well-being, quality of life, and dignity. These personal values were seen as quality indicators of HCSW practice, as these examples from the data show: A female HCSW adjusts the glasses on a man with dementia on the ward. She pulls down the bottom of his top over his trackpants, stretches her arm around his shoulders and tilts her head slightly to get a better look at him next to her. (S1.Ob. April 16, 2024; KM-R) Providing constant reassurance was vital in bringing [the person with dementia] around and into the present moment in time. (S2.CLG. April 24, 2024) Patients are humans. The respect you give to your parents should be the same you give to patients. (S1.CLG. April 30, 2024)
Moreover, acting like a friend, establishing trust, giving choices, not rushing with care tasks, helping patients make decisions, and making things fun were also seen to be important personal values that were carried through into everyday practice.
Throughout the 20-week contact with HCSWs on this study, it was clear that the completion of personal care tasks to a high standard was a source of significant pride and a further quality indicator of a “job well done.” As one HCSW shared with the researchers: I want them [patients on the ward] to be clean and I want their room to be tidy. I love it when they’re eating. I want them to eat something, drink something. (S2.CLG. April 10, 2024)
Showing that you care was extended to everyday tasks such as shaving male patients with dementia on the ward. In developing this point, one HCSW spoke about the importance of “tuning in” to share that moment and time together, and at the end of a shave, one HCSW shared that it was important “not to simply reach for the towel and walk away” but, instead “to take the time to look in the mirror together and to ask the person with dementia if they were satisfied with the shave” (S1.CLG. April 30, 2024).
However high the personal values and standards of the HCSWs, shift work can be tiring, and this was complicated at times by staffing on the ward being sub-optimal or experienced HCSWs being required to mentor new HCSWs (or agency staff) brought onto the ward to make-up the staffing numbers. To help minimize “burn-out” on the ward, HCSWs discussed the importance of “tuning in” to yourself to unload some of the tensions that can arise, but as Mike shared, “We [HCSWs] don’t have time to sit down with staff and ask ‘how do you feel about doing this?’” (S1.CLG. April 30, 2024). It would appear, therefore, that for HCSWs to meaningfully “tune in” to yourself required ongoing and structured support and supervision. However, from our in-contact experience, this did not appear to be a regular feature of caring routines or in shared examples of HCSW practice during the CLGs.
Tuning in … to My Craft
Alongside personal care needs and to their own values, HCSWs spoke about refining their practice of responding directly to the sensory, social, and emotional needs of patients, what we are referring to here as the “craft” of HCSW care. While HCSWs were required to follow care plans and instructions delegated from registered staff on the ward, delivering care in a person-centered and flexible manner meant they also made many decisions on their own, sometimes rapidly if situations on the ward changed, or if the person with dementia’s personal care needs had not been met at one time of the day but needed to be completed before the end of a shift. During a period of observation, one of the researchers noted the multiple demands and decisions required of HCSWs on daily basis: They [HCSWs] are checking a folder to see who they’re “on” next [i.e., one-to-one observation]. There is so much work to do, and it is hard work. Hands to be held, shoulders patted. Their effort in checking documents, monitoring, observing, feeding, holding (always holding), talking, occupying the time and space here, now. I also feel quite moved by the enormous efforts and constant actions of the staff in asking about me and my wellbeing. (S2.Ob. May 1, 2024; KM-R)
It was also clear that “meeting needs” in the ward environment was not easy, requiring patience and expertise and a need to “tune in” to the embodied actions of the person with dementia, as this exchange between KM-R and Bob [an HCSW] demonstrates: KM-R: How do you help [patient’s name] to drink as [patient’s name] continually walks up and down the ward corridor with a glass of juice in his hand, but he does not seem to recognize that as a drink? Bob: Sometimes [patient’s name] signals to me that he is thirsty. Other times, I simply ask. Or I place a hand on his shoulder or lower back and lift the glass to his lips.
Within their everyday work, HCSWs were required to balance care, safety, and risk on the ward. The researchers noted that “keeping an eye” [on patients] was a core part of the HCSW role and one where they were highly skilled at “tuning in” to, and this included circumstances when the person with dementia was “dozing on the couch or sitting or walking around” (S2.Rf. May 15, 2024; KM-R). Indeed, during one observation session, the researchers noted how suddenly the situation on the ward could change, recording how an HCSW quickly intervened to stop an altercation between two patients: Kane [HCSW] reacts quickly by standing in between two male patients. Kane puts up a hand, palm up (in peace) toward a patient (P1) who has jumped out of his seat after being touched suddenly by another patient (P2) from behind. Kane says “sorry” to P1 and guides P2 away. P1 suddenly kicks his foot out toward P2 but Kane just manages to stop it connecting with P1. He then moves P2 swiftly out of the room and then returns to calm P1 down. (S2.Ob. May 1, 2024; RP)
Within their reflections of this encounter, the researchers noted the subtle skills that were required to diffuse this situation, including the HCSW’s use of body language, communication skills, and tone of voice. Interestingly, HCSWs were clear that it was through “tuning in” to their craft of care that [any] training was best situated and that classroom teaching did not always best reflect their ways of learning and doing.
Tuning in … to Visitors on the Ward
It was evident from the different data strands on this study that HCSWs had a central role in “tuning in” to the visitors on the ward (i.e., the family members, friends, and relations who were attending the ward to visit the person with dementia). This “tuning in” process required HCSWs to be skilled at remembering relationships that mattered to the person with dementia including, whenever possible, the names of the visitors. As admission to the ward for a person with dementia could be over a period of several months, and that as HCSWs were ever-present on the ward, these visiting relationships were often positioned as being “friendly” and HCSWs seen as a “friendly face.” Indeed, from the researcher observations of such interactions on the ward, it was evident that visiting family also appreciated the familiarity and care that was shown to them when they attended the ward.
On the other hand, the ward could be a busy and, at times, a volatile and unpredictable environment. HCSWs therefore also needed to consider the safety of visitors to/on the ward. Managing this protective and proactive element to their work was highlighted by an observation made by the researchers and then discussed at the next CLG which the HCSWs attended (S1.CLG. April 30, 2024), as this revealing, but lengthy, extract suggests: The context for this example occurred during one observation period when a HCSW shared with the researcher (RP) that a particular patient could be “very confused” when woken up in the lounge. Consequently, the patient would not recognize his visiting relatives when they arrived to see him, which the relatives found very upsetting. As a way of managing this process, at the next visit, a HCSW was observed meeting the visiting family members at the entrance to the ward and instead of taking them to the lounge, the HCSW took the family members to their relatives’ bedroom and were asked to wait there for a short while. Two HCSWs were then observed to wake the person with dementia gently in the lounge and then saying to him, “Come with me, I’ve got a surprise … you are going to love it.” The person with dementia was then walked between the two HCSWs to his bedroom so that the visit could go ahead with the minimum of distress to all those concerned. When asked about this plan of care and interaction in the next CLG, the HCSWs shared that this was a strategy that they had worked out together (i.e., between the HCSWs) rather than being told to do it by the registered staff or following a care plan in the patient notes. This ability to “tune in” to the needs of the visitors was seen to be extremely skilled and yet invisible to those outside of the HCSW workforce on the ward.
In developing this skill at “tuning in” to the safety of visitors on the ward, HCSWs also took care to protect the safety of visitors by making them aware that a particular patient [not related to the visitors] was upset and/or to avoid a certain area on the ward because of the potential for an incident to occur. As previously shared, this care was also extended to the researchers during their time on the ward.
Being Co-Present
Lastly, and depicted to the right of Figure 2, the data highlight the importance of “being co-present,” which, in our model, is a theoretical abstraction and linking scheme that acts as the descriptive meaning and practice outcome of everyday HCSWs work with people with dementia admitted to NHS mental health wards for older people. “Being co-present” is attended to in the “here and now,” and it is a vital aspect of quality, person-centered dementia care. These connections are fully embodied, are situated in the present, and have the potential to enhance well-being. As we have seen in the data, these moments of connection are not solely a facet of communication but can occur at other times, such as when interaction is subtle or seen to be mundane, for example, when HCSWs sit quietly with a patient with dementia on a settee holding their hand or when they sit closely together watching television.
Being co-present does not diminish the importance of planning for activities or assessing need, or for accounting for what has been done, and the impact of care after it has been completed. Indeed, the model outlined in Figure 2 and in the supporting text includes both preparation aspects of quality care and a practice of reflection and learning. However, the argument we advance here is that being co-present and attending to the demands of a moment is a vital aspect of care and one that HCSWs are especially adept at “tuning in” to.
Discussion
This article has drawn on mixed qualitative methods to deliver an in-depth understanding of the everyday care practices carried out by HCSWs working with people with dementia admitted to NHS mental health wards for older people. Despite the important patient-facing nature of their role, to date there is a paucity of studies exploring the practice of this group. Analysis has provided an explanatory and dynamic model of HCSW practice grounded in the direct experiences of this staff group and underpinned with the language and relational concepts of care aesthetics (Thompson, 2022). A previous review has described the presence of HCSWs on hospital wards with a key theme of “always being front and center” (Kindell et al., 2025), which details the continual physical presence of HCSWs out on the ward floor and their crucial role in meeting personal and healthcare needs. The analysis here takes this a step further in terms of considering “being co-present” as a theoretical abstraction and linking scheme that describes the meaning and outcome of HCSW practice with people with dementia on NHS mental health wards for older people. As we define it, “being co-present” is both a spatial and temporal idea that suggests that attending to the “here and now” is a vital aspect of quality, person-centered dementia care orientated to the “in-the-moment” well-being of the person with dementia.
This alignment is pertinent for the physical location of the study as patients with dementia on the NHS mental health wards for older people had significant difficulties with communication and were reliant upon additional non-verbal support for interaction, including the use of touch, facial expression, and body movements. Additionally, patients with dementia were admitted to the ward because of their considerable challenges with behavior and/or pronounced levels of risk, and this meant that mood, interaction, and/or the ward atmosphere could change rapidly, requiring appropriate supportive action from the ward team, including HCSWs. Moreover, as a locked environment of care, HCSWs needed to support all of those within the ward space (i.e., patients, colleagues, and visitors) and to quickly “tune in” to any shifts in the ward atmosphere, such as a sudden increase in noise and movement, to engage with people with dementia who may be unable to feel, or relay, this experience themselves (see also: Richardson & Campbell, 2024; Sumartojo et al., 2020). It was this rapid ability to “tune in” and attend to the sensory attributes of the ward that operationalized and applied the values and principles of care aesthetics and helped to articulate the skilled care practices of HCSWs.
As seen throughout the study findings, and in Figure 2 especially, care aesthetics also provides a framework to analyze the micro-practices of care, including the expertise required to deliver person-centered care (Kitwood, 1997), and respond to the values of “positive person work” which includes recognition, negotiation, collaboration, and facilitation. Two areas within Kitwood’s (1997) original formulation of “positive person work” are a focus on “play” and “timalation,” both of which, we would suggest, have received limited attention in the literature or practice context since the publication of Kitwood’s seminal text. However, “play” is described by Kitwood (1997) as an exercise in spontaneity and self-expression and an experience that has value in, and of, itself. In our data, this can be seen within the formalized activity sessions conducted by HCSWs on the ward, but also, crucially, in spontaneous interactions that are a part of everyday care practices, such as using banter, dancing, and singing with patients with dementia on the ward. Furthermore, “timalation” refers to forms of interaction which target the senses and provides contact, reassurance, and pleasure (Kitwood, 1997). During observations, HCSWs were regularly seen to rub shoulders, stroke and hold hands, or sit closely alongside the person with dementia to provide reassurance. Attention to the sensory experiences was not just to complete care tasks; these acts of “timalation” often occurred outside of such a setting and provided important embodied and relational experiences in themselves. Person-centered care also extended to “tuning in” to the needs of family members on the ward, as evidenced by the support provided around visiting in the example above. Given the significant emotional challenges for carers in this setting (Partridge et al., 2025; Wolverson et al., 2023), this would appear to be a vital aspect of the HCSW role.
The model in Figure 2 also highlights how the senses and the body are used within a care relationship and explores how both participants, that is, in this context the HCSW delivering the care and the person with dementia receiving it, are experiencing the encounter on a sensory level. There were numerous examples in the data where care was not just delivered; it was embellished using thought and foresight and to consider the person with dementia’s experience “in the moment” (Keady et al., 2022). For example, as theatre scholars, the researchers on this study (KM-R; RP; and JT) were continually struck by the performative nature of the care work that was on show on the ward and the ability of HCSWs to spontaneously, and creatively, improvise in the moment. As an illustration, and as shared in the article under the “Tuning in … to the person with dementia” category heading, when a person with dementia was embodying the actions of “fishing” on the ward, the person then handed an imaginary [to us] “fish” to the HCSW who then chose to carefully take the “fish” and enter the person’s world. What followed was a sustained interactive performance by the HCSW that upheld the self-esteem and embodied actions of the person with dementia on the ward who was, indeed, “fishing.” Interestingly, this decision by the HCSW to accept and go along with a situation of altered reality (rather than challenge it with the “truth”) is currently conceptualized in the dementia studies literature as entering a state of “therapeutic lying,” an area that presents as potentially contentious in healthcare (see Elvish et al., 2010; Murray et al., 2025), as well as difficult to define, due to the nuances of non-truth telling in daily life (see Williamson & Kirtley, 2016). The interactive choices inherent in such encounters have most often been explored with respect to managing a person with dementia’s distress and what to say in response to repetitive questions (see Pilnick et al., 2025). However, if we stand back and view the interaction with the “invisible” fish through the lens of theatre performance, this could be framed as a linked association between “play” and “improvisation” (Dowler, 2013), both of which have a long history in theatre studies (Spolin, 1963). The actions used by the HCSW represent not just verbal responses but, arguably, also responsive embodied acts which layer the interaction with creative improvisation. Such a performative and descriptive lens engenders a more sensitive and relational way of describing these everyday supportive acts and caring moments.
A lens of improvisation can help important questions to be surfaced to underpin reflective practice, such as “if you do step into someone else’s reality, what part will you choose to play?” So, for example, in terms of supporting the person with dementia who, in our study, was in “work mode” as a cleaner, an HCSW could choose to become a co-worker and enhance camaraderie or instead become a supervisor and ask the person with dementia to make sure they have not “missed a spot there”—as played out in Claudia’s example, with potential for either stance. Further research is required to explore this area, but performance practice could provide an opportunity to reposition these interactions as creative holistic encounters where the skills are in “tuning in” to the person with dementia and their experience of lived time.
The contextualized nature of care experiences also demonstrates the numerous choices and decisions that HCSWs are required to make throughout their day, such as how best to attain cooperation when communication and consent is significantly compromised, and manage refusals to engage and other challenges with behavior. HCSWs spoke about prioritizing the patient’s well-being within their decision-making rather than focusing on completing the task by, for example, leaving a person who might be refusing to get dressed and returning a little later to try again when the person with dementia may be in a different frame of mind. However, HCSWs are faced with considerable ethical complexity within their work, including the issues discussed above in terms of altered reality and practical challenges, such as how often or how long to postpone a personal care task during instances of refusal and the consequences of this in terms of dignity and needs, and how this might then impact personal well-being. The high frequency of these ethical issues in the everyday care of people with dementia and the associated training needs has been recognized in other work (Kindell et al., 2025; Nuffield Council on Bioethics, 2009). In this sense, while the overall frame of HCSW work was delegated by the registered staff on the ward, within their everyday care practice, HCSWs were required to make numerous “in-the-moment” decisions on how best to deliver care which, we would suggest, are aligned to their intuitive and skilled ability at “tuning in” to a situation.
Finally, care aesthetics offers a language that might contest the well-established hierarchy of NHS staffing, with HCSWs currently at the bottom of that ladder because of their lack of recognized professional qualifications. Care aesthetics draws attention to the “craft of care,” and this means that staff with few formal qualifications can be actively celebrated as highly skilled experts in their craft, contributing to high-quality care and, potentially, to the development of other workers. There is debate on how these skills are acquired, for example, whether the skills represent an innate part of the worker (Smythe et al., 2015) or if they are acquired via informal ways of learning (see chapter 3 in Surr et al. (2023) for further discussion of this area). While care aesthetic theory would argue skills are honed over many years of personal and vocational experience (Harman, 2021; Thompson, 2022), further research is needed to explore how HCSWs can be supported to more effectively “tune in” to themselves, their values, and their craft. This has significant implications for staff training, well-being, and retention, areas all recognized as requiring further and urgent attention in the NHS (Griffin et al., 2024; Hall et al., 2024).
Strengths and Limitations
To the best of our knowledge, this is the first inductively generated model of everyday HCSW practice with people with dementia admitted to NHS mental health wards for older people. Further research is needed to explore this in additional settings to see how the model might contribute to supporting HCSWs and their mentors to further understand and develop their practice and its subsequent impact on people with dementia in their care. The interdisciplinary nature of the research team was also another strength as it enabled different perspectives to contribute toward what was being seen and described in an everyday care context, albeit one that has been rarely studied. A limitation of the work is that it only involved three wards drawn from one area of the North of England. A larger and more culturally diverse sample would help to provide additional authenticity to the HCSW structures and processes described in this article. In addition, more explicit consideration of care delivery in situations where an HCSW is of a different ethnic and cultural background to the patients they are caring for is warranted, including where language and cultural differences exist, and how this manifests itself in terms of “tuning in” to the person with dementia, making sense of their life story and responding to behavior and communication. For example, the HCSWs’ use of banter and jokes, described in this study, may be different, or could even be misinterpreted, in a cross-cultural context.
Conclusion
HCSWs represent the largest staff group on mental health wards for older people, and this, along with the amount of time they spend in direct patient facing duties, means understanding and enhancing their practice could have a significant impact on the care of patients with dementia and their family members. This article has presented a data-driven dynamic model for HCSW practice that draws insights from the field of care aesthetics. A core aspect of care aesthetics is consideration of sensory, embodied, and relational skills, with the data indicating that this is central to the work of HCSWs, whether this is within the delivery of personal care, recreational activities, or in supporting the social interaction and behavior of people with dementia. HCSW practice entailed numerous in-the-moment decisions where staff were required to “tune in” to the person with dementia, visitors, the ward, and their colleagues, as well as themselves, their values, and their craft. Being co-present was a vital aspect of person-centered care orientated to the “in-the-moment” quality of life of the person with dementia on the ward. Care aesthetics provides an important lens to consider the craft of care for HCSWs and to act as an applied learning opportunity across all strata of care provision for people with dementia in the NHS workforce, and beyond. Lastly, this study also contributes to the development of the field of care aesthetics, exploring the practical application of this theory in a real-world context.
Footnotes
Acknowledgements
Ethical Considerations
This study was approved by the NHS Health Research Authority and Health and Care Research Wales (HCRW; reference number 23/NW/0335).
Consent to Participate
All participants provided written informed consent prior to enrolment in the study. All ward and participant names are anonymized in this article in line with research protocol and ethics permission.
Author Contributions
JT, JDK, and JK contributed through the conceptualizing and design of project. JT, JDK, JK, KM-R, RP, RC, and RW refined research methods, ethical issues, and practical delivery. KM-R and RP carried out the fieldwork. All authors took part in writing, review, and editing of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Arts and Humanities Research Council of the United Kingdom under grand number AH/W003104/1.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.