
Abstract
Family caregivers play a vital role in supporting older adults, yet caregiving often brings persistent exposure to mortality, leading to heightened death anxiety and psychological distress. Applying terror management theory (TMT), this study explores how caregivers navigate death anxiety and maintain anxiety-buffering systems (cultural worldviews, self-esteem, and close relationships) while participating in a supportive intervention program. This qualitative study employed in-depth semi-structured interviews (approximately 90 min) with 17 family caregivers of older adults participating in a national caregiver intervention program in Israel. The interviews explored four key domains: (1) caregiving experience, (2) daily challenges, (3) program participation, and (4) program evaluation. Theory-driven deductive content analysis, guided by TMT’s framework, was used to identify patterns related to mortality awareness, psychological defenses, and intervention effects. The TMT-driven data analysis revealed three primary themes: (1) “This is death, it is hard, death, of course”: Heightened death anxiety in caregiving; (2) “You know there are things you don’t talk about, you don’t talk about death”: Disrupting of anxiety-buffering system due to caregiving; and (3) “You free the soul”: Intervention rebuilds anxiety-buffering system and balanced self. This study highlights the need for existentially informed caregiver support programs that integrate TMT principles to address the deeper emotional and philosophical challenges of caregiving. Implications for healthcare professionals, policymakers, and social workers emphasize the importance of developing interventions that not only alleviate caregiver burden but also strengthen resilience by addressing existential fears inherent in caregiving.
Introduction
The term “family caregiver” refers to an individual who provides necessary care, support, and assistance to family members who are ill, disabled, or older adults. Family caregivers typically play a critical role in the healthcare system, often serving as primary providers of care in community settings, while navigating the complexities of medical, emotional, and financial responsibilities associated with caregiving (National Alliance for Caregiving, 2020; Schulz et al., 2020; Sherman, 2019). While caregiving can foster a sense of purpose, strengthen family bonds, and elicit gratitude from care recipients (Edelstein et al., 2017), it also imposes significant burdens. Studies demostrated its long-term negative impact on physical, mental, social, and economic well-being (Amar et al., 2022; Bachner et al., 2011), accelerated biological aging, and the neglect of self-care (Allen et al., 2017), negative impact on professional life and financial security (Tur-Sinai et al., 2020, 2022), and elevated levels of stress, anxiety, and depression (Ünal & Ordu, 2023; Vrettos et al., 2023). The lack of formal and informal support exacerbates these difficulties, leaving caregivers unprepared for the multifaceted nature of their role (Or & Kartal, 2019; Park et al., 2018).
Recognizing the complexity of caregiving, a variety of intervention programs have been developed, that generally fall into two categories: practical support and psychosocial interventions. Practical interventions, such as financial assistance and respite care, aim to reduce the objective demands of caregiving, while psychosocial interventions focus on enhancing emotional resilience through support groups and psychoeducation (Leung et al., 2017). Multidimensional approaches that integrate education, skills training, and emotional support have shown promise in improving caregiver well-being (Calvó-Perxas et al., 2018). Individualized interventions have been particularly effective in enhancing social support, reducing depressive symptoms, and improving overall health outcomes (Elliott et al., 2010; Kusi et al., 2022).
However, many interventions have shown limited effectiveness, underscoring the need for a more comprehensive theoretical framework (Adelman et al., 2014; Northouse et al., 2012). The existential dimensions of caregiving remain relatively unexplored in intervention research, despite their significance for caregiver well-being. Family caregivers face constant exposure to mortality, challenging their psychological resilience beyond the practical demands of care. Applying terror management theory (TMT) provides insight into how this exposure shapes caregivers’ defense mechanisms and how interventions can address both existential concerns and practical needs. This perspective broadens traditional burden-focused research, uncovering critical but underexplored dimensions of caregiving.
Rooted in Becker’s work (1973) and expanded by Greenberg et al. (1986), TMT posits that humans uniquely recognize their own mortality, leading to death anxiety and the activation of psychological defense mechanisms aimed at mitigating existential distress (Helm et al., 2020). This anxiety-buffering system relies on three interrelated components. Cultural worldviews, including societal norms, moral values, religious beliefs, and ideological frameworks, provide meaning and impose order on human existence, offering a sense of continuity through literal (e.g., belief in an afterlife) or symbolic (e.g., legacy through achievements) immortality (Burke et al., 2022). When confronted with mortality, individuals often reinforce their worldviews, defending their beliefs and rejecting opposing perspectives (Pyszczynski et al., 2015). Self-esteem serves as another crucial buffer, fostering the perception of oneself as a valuable and competent individual within a meaningful universe (Pyszczynski et al., 2021). High self-esteem has been shown to reduce anxiety responses to mortality awareness, whereas threats to self-worth heighten death anxiety and defensive reactions. Close personal relationships further reinforce existential security by fostering belonging, emotional support, and shared purpose (Florian et al., 2002). Research suggests that mortality reminders increase the desire for interpersonal closeness, strengthen attachment behaviors, and enhance commitment to in-group relationships (Arrowood & Cox, 2020). Together, these mechanisms help individuals maintain psychological equilibrium in the face of death awareness, shaping behaviors and social interactions in profound ways.
Empirical studies have consistently supported these mechanisms, both in research with experimentally constructed reminders of mortality and in research in real-world events such as illness, natural disasters, and political instability (Horner et al., 2021). However, there are only few researchers applying TMT to the caregiving experience continually confronted with the reality of aging, illness, and death. In a study by Quevedo-Blasco et al. (2024), a notable positive association was identified between death anxiety and the duration of family caregiver experience. Additionally, death anxiety emerged as a significant negative predictor of coping among family caregivers (Semenova & Stadtlander, 2016). Similarly, a recent study on informal caregiving for older adults utilized TMT to explore dimensions of aging anxiety, revealing significant mediation in the associations between caregiving burden and negative affect (Hamama-Raz et al., 2023). Despite the growing recognition of existential challenges in caregiving, current interventions rarely address the terror management aspects of caregiver stress. This gap is particularly significant, as caregivers must navigate not only practical caregiving demands but also profound existential concerns about mortality, meaning, and human fragility.
The current study aimed to examine how family caregivers navigate death anxiety and maintain anxiety-buffering systems while participating in a supportive intervention program. Specifically, we ask: How do family caregivers manage death anxiety and maintain psychological equilibrium through cultural worldviews, self-esteem, and relationships while caring for aging relatives? How can the intervention program designed for family caregivers help manage death anxiety and maintain this anxiety-buffering system?
Design
This study utilized a qualitative research design to investigate the experiences of family caregivers participating in a national pilot intervention program. The Family Caregiver Support Program is a comprehensive intervention program designed to support family caregivers of elderly citizens within Israel’s welfare system. The program operates on three integrated levels of intervention: individual, group, and community-based services. At the individual level, social workers provide short-term counseling (three to six sessions), guidance, information provision, rights advocacy, and integration into existing programs through structured intake, intervention planning, documentation, and follow-up processes. The group-level component includes support groups, educational workshops, and respite activities designed to provide peer support and skill development. The community-level intervention focuses on raising awareness about family caregivers among professionals and the general public, developing partnerships with other organizations serving elderly populations and their families, building community processes for population identification and service accessibility, and establishing municipal round tables on aging that incorporate family caregiver issues. The program is implemented through a unified organizational model within welfare departments’ elderly divisions, with dedicated social workers responsible for the family caregiver domain alongside other departmental responsibilities. Supporting infrastructure includes structured learning and knowledge development processes, professional training programs, accompanying evaluation research, information management systems, and a theoretical and practical knowledge repository for ongoing professional development and updates for field workers (Resnizky & Cohen, 2020).
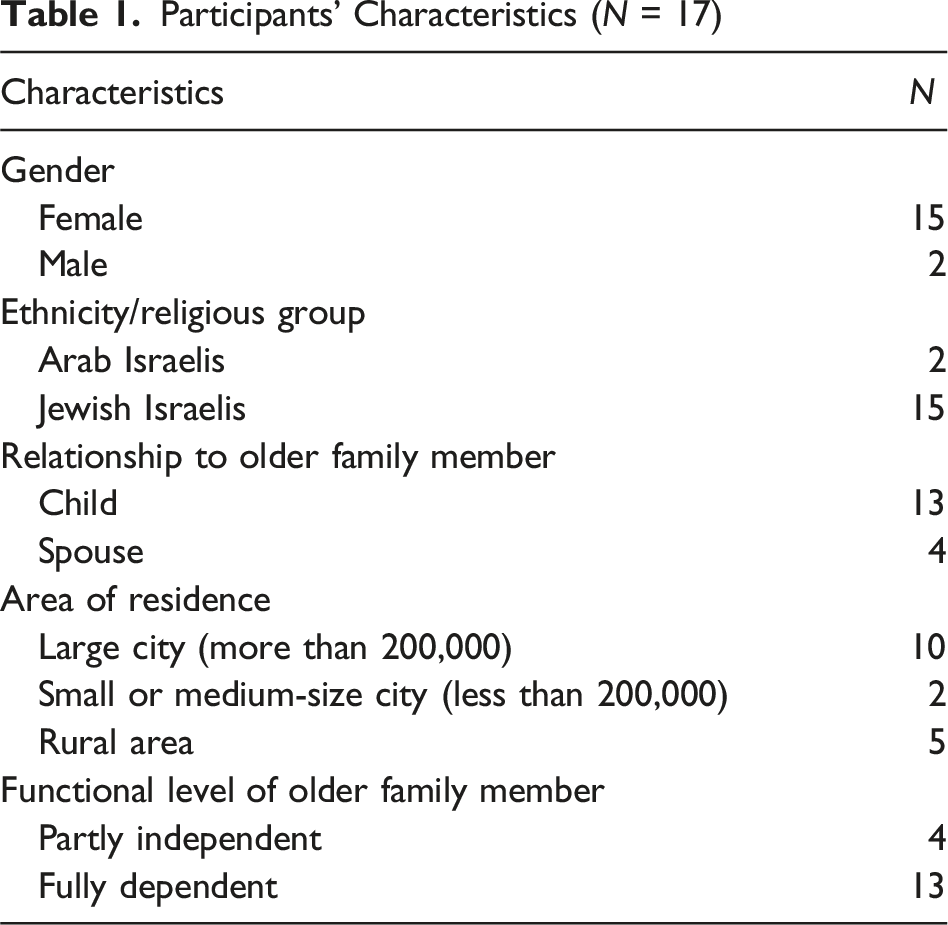
Participants’ Characteristics (N = 17)
Ethical Approval
This study was conducted in accordance with ethical guidelines and was approved by the Ethics Committee of Faculty of Social Welfare and Health Sciences, University of Haifa (Approval No. 018/22). All participants provided informed consent.
Materials and Methods
Participants
The study included 17 participants, who served as primary caregivers for older family members. The sample was predominantly female (n = 15, 88.2%) with only two male participants (11.8%). Most participants were Israelis Jews (n = 15, 88.2%), while two participants (11.8%) were Israeli Arabs. Regarding their relationship to the care recipient, the majority of participants were adult children caring for their parents (n = 13, 76.5%), while four participants (23.5%) were spouses providing care for their partners. Participants resided across different geographic areas, with the largest proportion living in large cities with populations exceeding 200,000 residents (n = 10, 58.8%), followed by those in rural areas (n = 5, 29.4%), and a smaller number in small to medium-sized cities with populations under 200,000 (n = 2, 11.8%). The functional status of the older family members varied considerably. The majority of care recipients were fully dependent (n = 13, 76.5%), requiring comprehensive assistance with daily activities, while four older adults (23.5%) maintained partial independence in their functioning. All participants received support from either an external caregiver or another family member in addition to their primary caregiving responsibilities. The duration of intervention participation ranged from two months to one and a half years, reflecting varying stages of caregiving experience and support service utilization among the study participants.
Data Collection
Experienced interviewers conducted individual interviews via Zoom, with each session lasting approximately 90 min. The interviews explored four key domains: (1) caregiving experience (e.g., “What does it mean for you to be a caregiver for an elderly parent/spouse?” and “What has changed in your life since becoming a caregiver?”); (2) daily challenges (e.g., “What are the health implications for you?” and “How has caregiving affected your relationships with other people?”); (3) program participation (e.g., “What services did you actually receive from the family caregiver support program?” and “What has changed in your life since you started receiving services?”); and (4) program evaluation (e.g., “What are the strengths and weaknesses of the service?” and “How could the service be improved?”).
The comprehensive interview guide offers optional questions for interviewers and is intended as a flexible framework rather than a rigid script, allowing adaptation to the flow of each interview. All interviews were audio-recorded and transcribed verbatim. For details, please see the English translation of the suggested interview guide in Appendix 1.
Data Analysis
We employed theory-based deductive content analysis, analyzing the qualitative data through a predetermined theoretical framework to identify, support, or challenge relevant constructs (Hsieh & Shannon, 2005). Our deductive content analysis followed these steps: (1) Initial coding: Identifying text segments related to TMT’s core constructs: death anxiety and anxiety-buffering system, for example, citation related to fear of aging and death such as “I have some anxiety about what will happen to me in old age.” (2) Secondary coding: Categorizing how caregiving experiences either challenged or reinforced the TMT constructs. For example, citations about fear of aging and about fear of death were coded as “caregiving-related growing fear of their own aging and mortality.” (3) Theme development: Grouping codes into broader themes reflecting patterns in how caregivers experience and managed mortality awareness; for example, the code “caregiving-related growing fear of their own aging and mortality” was united with category “distress when witnessing suffering of close one” and incorporated into the theme “This is death, it is hard, of course”: Heightened death anxiety in caregiving.
Researchers’ Background and Methodological Rigor
Data analysis was conducted by two experienced researchers with complementary expertise: a social worker and gerontologist (T.B.W.) and a social psychologist (K.S.), both with extensive experience in qualitative research and practice with older adults, intergenerational relationships, and family caregivers. Throughout the data analysis process, the researchers engaged in systematic self-reflection, discussing their personal perspectives on the issues under study and actively working to bracket out their personal values and potential biases (Braun & Clarke, 2019). Each researcher separately performed the initial coding process, followed by collaborative sessions to compare analyses, discuss differences, and seek agreement regarding theme content and interpretation of meaning. Regular reflexive discussions were conducted to ensure that emerging themes reflected participants’ experiences rather than researchers’ preconceived opinions.
Credibility (i.e., internal validity) was strengthened through systematic data analysis procedures grounded in rich descriptions of participants’ narratives, peer debriefing, and referential adequacy (Morse, 2015). Separating the researchers’ interpretive notes from descriptive narratives ensured that the themes identified authentically reflected participants’ experiences. Confirmability was established by maintaining detailed documentation of analytical decisions and coding processes, along with transparent reporting of the researchers’ reflexive discussions and bias management strategies.
Transferability was addressed through comprehensive characterization of study participants and detailed descriptions of the research context, enabling readers to assess the applicability of findings to similar populations and settings. The complementary expertise of the research team provided multiple analytical lenses, while maintaining systematic approaches to ensure methodological rigor throughout the research process.
Validation
To ensure methodological rigor (Cypress, 2017), we maintained detailed process documentation, engaged in researcher self-reflection, and cross-checked interpretations through peer debriefing with experts in qualitative research, gerontology, and TMT.
Results
The TMT-driven data analysis revealed three primary themes: (1) “This is death, it is hard, death, of course”: Heightened death anxiety in caregiving; (2) “You know there are things you don’t talk about, you don’t talk about death”: Disrupting of anxiety-buffering system due to caregiving; and (3) “You free the soul”: Intervention rebuilds anxiety-buffering system and balanced self.
“This Is Death, It Is Hard, Death, of Course”: Heightened Death Anxiety in Caregiving Mind
Mortality Awareness: Direct Confrontation With Death
The process of a relative’s dying creates a situation of ambiguous relations with death, involving both the acceptance of its inevitability and the fight for the loved one’s life. This duality reflects among the participants a complex emotional landscape where they simultaneously strive to prolong life while grappling with the natural progression toward death as illustrated by the following quote: You know you have to say goodbye and it’s also … frustrating, because … it’s a kind of fear of death. True, Mother is very old, death will come. But there is a dissonance. On one hand, I’ve had enough, I want her to go, I no longer have the strength. On the other, I want her to live … (Interview 9)
This quote highlights the internal conflict that the caregiver faced and shared during the initial steps of the intervention when managing end-of-life care. The caregiver experiences a profound dissonance: on the one hand, she desires relief from the exhaustion and emotional strain of caregiving, while on the other hand, she clings to the hope of her loved one’s survival. This tension highlights the deeply human struggle between the intellectual acceptance of death as a natural process and the emotional resistance to letting go.
The social worker’s support during the intervention helped participants articulate this ambivalence and face their fears of impending loss and mortality. It is hard, seeing this death, it’s crying, it’s a quarrel with God—what is this thing anyway, why is it necessary, it’s … it’s all day, you know, all day working on myself on how to release my desires and how to accept that this is the situation, this is death, it is hard, death, of course. (Interview 16)
This quote captures the existential and spiritual struggle of caregiving. The caregiver describes an emotional journey of grappling with the meaning of death, questioning its purpose, and striving to find peace with its inevitability. The “quarrel with God” reflects a broader confrontation with the caregiver’s own religious beliefs, cultural values, and expectations, as they attempt to reconcile the emotional pain of witnessing decline with the need to accept death as a part of life. The repeated acknowledgment that “this is death, it is hard” underscores the caregiver’s gradual, yet painful, process of coming to terms with mortality and that the “quarrel with God” is destined to fail. The intervention programs could provide a safe space in which to share such insights and be accepted and supported by other members undergoing similar experiences and feelings.
Anticipatory Death and Aging Anxiety
Witnessing the decline of a loved one becomes a mirror through which caregivers project their own fears of dependency and aging. The next quote reflects the caregiver’s existential struggle with their inevitability: It’s also frustrating to look at your parent and say: “What, will I do this to my children, as well? Will I be like this, too?” I don’t want to be like that. But I see it—there’s no control … at a certain age, a person crosses the line and becomes [dependent]. And this fear [of becoming like my aging mother] probably also creates this anger in me … I’m close to that age and I’m afraid that maybe I’ll also be like that. (Interview 9)
The proximity to death in the participant’s everyday experience of care reveals his own fears. They shared their concern and fear of becoming a burden to their children, mirroring the current caregiving dynamic, which reveals how caregiving forces individuals to confront their own mortality. It seems that the realization of the loss of control in old age amplifies feelings of anger and frustration, as caregiving becomes a painful reminder of their own future vulnerability. This issue becomes central during the meetings with the social worker and in discussions among the intervention participants addressing cultural perceptions, as well as norms and values relating to intergenerational reciprocity and expectations.
For caregivers without children, the lack of a support network for their own future intensifies anxieties about aging: Look, I … I don’t have children. So [after the complex process of receiving support for parents] I have some anxiety about what will happen to me in old age. (Interview 10)
Witnessing the complexity of caregiving tasks creates a heightened awareness of her own future dependence and raises concerns about who will fulfil that role for her. This concern enables the provision of an empathic response from the professional intervention and encourages participants to express how caregiving can transform one’s outlook on life and aging, triggering existential questions and anxieties.
Another caregiver’s narrative reflects the traumatic nature of witnessing a loved one’s suffering and death. My father’s death was very, very hard for me, He was taken care of for 12 years, clean, organized, if creams were needed then the best things and suddenly I reached a situation where I just had no control. It wasn’t under my control, no matter how much I tried and ran, and in the end, he died a very hard death, on my eyes … And I started to have anxiety that something is happening to me. (Interview 11)
Despite the best efforts to provide care, the lack of control over the outcome and the hardship of being there led to feelings of helplessness and deep anxiety. The caregiver’s subsequent fear for their own health and future mortality illustrates how caregiving, particularly in challenging circumstances, can leave long-lasting psychological scars and a heightened awareness of one’s vulnerability. Exposing this vulnerability created closeness and intimacy among the intervention group participants.
“You Know There Are Things You Don’t Talk About, You Don’t Talk About Death”: Disrupting of Anxiety-Buffering System due to Caregiving
Challenging Cultural Worldviews
The interviews revealed the cultural taboo surrounding discussions of death and planning for the end of life, and how in the caregiving context it became a part of everyday life. I really wanted [mother] to sign a lasting power of attorney. It was hard for her, it was really hard to talk about it. In the end, we signed, but it was hard because you don’t talk about anything, you know there are things you don’t talk about, you don’t talk about death. What will be, what will happen when you get sick, you don’t talk about it, so even when I tried to talk, it was really hard for me … (Interview 16)
The intervention participants shared their difficulties and found the legal issues as sensitive and even more as a taboo. The caregiver’s desire to address and formalize legal and medical arrangements underscores a practical response to the inevitability of decline and death. This avoidance creates barriers to communication and decision-making, intensifying the emotional burden on caregivers and in the same time raises the tension for the ambiguous future. During the intervention sessions, the participants were able to verbalize their deeply ingrained societal and personal discomfort, while discussing mortality.
The intervention participants refer to societal shifts toward institutional eldercare that challenge caregivers’ beliefs about familial reciprocity and intergenerational responsibility. Next quote reflects the contradiction of family caregivers with contemporary society’s relationship with aging and mortality, where the loss of personal control caused by caregiving directly contradicts the individualistic cultural belief that emphasizes independence and self-determination: “Today people put the elders in nursing homes and don’t visit them. They raised us, they gave everything to us, why don’t we give back to them?” (Interview 17). At the same time, the respondent herself shares social perception that moving to a nursing home is already “one foot in the grave,” accelerating the fear of approaching death.
Challenging Self-Esteem
The findings indicate that the caregiving role systematically undermines self-esteem by stripping the participants of their sense of agency and control—key components of positive self-regard. As one participant poignantly described: It started little by little … before she had a chance to recover from the [first] fall, she fell again … She broke her knee and shoulder and experienced delirium … then, I actually went to live in her home with the paid caregiver because she was no longer in a position where she could even understand what was happening. (Interview 16)
This narrative illustrates how caregiving progressively erodes one’s sense of self-determination, as life becomes increasingly dictated by external circumstances rather than personal choices. It appears that moving into the parent’s home forces the caregiver to give up other identities or roles. As a result, an imbalance arises in relation to the caregiver’s own needs, potentially triggering existential anxiety and the question: “So, who am I?”. This struggle was echoed by the intervention participants and was observed to elicit an emotional response.
The involuntary nature of the role further undermines self-esteem, as expressed by one participant: “There’s no choice … [the role of caregiving] becomes yours” (Interview 15). Another described it as “the role I was given in my life” (Interview 9). This passive language reflects how caregiving can overwhelm the participant’s life world and challenge one’s sense of being an active agent in her own life story. During the intervention, the social worker addressed the caregivers’ negative feelings such as helplessness, loss of self-control, and a sense of existential insecurity. As a result of capturing the relevant feelings of the other participants, caregivers were able to grapple with their own expectations for the future.
The potential futures they might experience as a caregiver and the possible future they once imagined had shifted since they became caregivers. This caregiver shared how her expectations and dreams for the future have been shattered; it seems that her own self-expression was prevented, and as a result she found herself neglected: We have a three-room apartment. There’s a study, a bedroom, a living room, and a [small, empty] room. I had a fantasy that when I retire, I would make [the empty room] into a studio and I would paint there. Well, now there’s a foreign worker in the studio. And the whole bedroom [is taken up by] my husband. [He] has a big bed and all that. At nine-thirty he goes to bed. It’s not possible [for me to stay] there, so my bedroom is the [empty] room. My apartment is now 12 meters … at first, I was depressed, the house felt, you know, “shut down” … (Interview 13)
The caregiving role further disrupts self-confidence by forcing the participants into situations where their previous competencies and knowledge become insufficient. This creates a profound sense of inadequacy that challenges their self-worth: I must arrange the foreign worker’s payments … the laws [around payments] have changed, and we weren’t informed. How was I supposed to know that? It’s so frustrating and there is no consistency … (Interview 13)
The primary motivation for participants in this intervention program was the need to address and navigate the legal and personal rights of their family members. This quote reveals how caregiving throws individuals into complex systems they feel ill-equipped to navigate, challenging their sense of competence and self-efficiency. This need has been given full attention during the intervention in order to help the participants gain back some self-worth. The all-consuming nature of caregiving further erodes self-esteem by limiting opportunities for other forms of self-validation: Sometimes, I feel like a woman after pregnancy. She gave birth to the baby and now she’s at home with him 24/7 and has no choice. He’s crying, and you have to go to him, he’s vomiting, and you have to take care of him. I mean it’s this kind of burden that sits on you. It’s yours. (Interview 15)
This comparison to new motherhood illustrates how caregiving can overwhelm one’s identity, leaving little room for other self-esteem-maintaining activities and roles. The constant state of reactive care undermines the sense of competence and control that typically buffers against existential anxiety. Such dedication to the current role possesses her everyday routine in a way that feels like a dead-end.
Challenging Close Relationships
In the next quotes, participants express their anger, frustration, and exhaustion, related particularly to how the burden of care is not equally shared across multiple family members: “It’s an extremely exhausting situation … It takes a toll on everyone … the whole family. There is a lot of frustration around the fact that my brother does not take part in this story, and that everything falls on us.” (Interview 16) “My brothers don’t know what meds [our mother] is on. I know what medicines I buy for her. She has narcotic back stickers for pain. I buy them for her, I put them on her. Apart from shopping, here and there, I do everything for her.” (Interview 12)
This issue elicits highly sensitive discussions during the intervention and reveals how unequal distribution of caregiving responsibilities can lead to conflict among family members, resulting in the feeling of extreme emotional strain.
Another form of close relationships between the caregivers and their aging relatives was expressed and shared by some of the intervention participants and is illustrated in the following quote: Before, I had a husband, and I was the wife. Now, I am the wife, but I am also the caregiver. And we have a foreign caregiver, but still … there were things [my husband] was responsible for [and] he no longer is. Now, everything is on me. Both managing him and managing the foreign caregiver. So, [life is] not the same. Life is really changing; I don’t have a husband I can go out with anymore. (Interview 13)
This process of changing role became significantly central and meaningful during the intervention session, particularly for participants who are caring for their spouse, and involved added layers of losses. This caregiver no longer has a husband to go out with. She feels that life is changing, both at the household management level and the personal-intimate level, as her spouse no longer functions in his role as her husband. Another quote reflected on similar difficulties in moving from the role that had been clear to her throughout her life (as a daughter) to a role that was still not completely clear to her: “It’s a very big problem … suddenly you become your mother’s mother. But you’re not exactly your mother’s mother” (Interview 9).
During the intervention program, the participants also discussed how the older adult’s declining health or behavioral changes can lead to their own social isolation, which in turn amplifies the caregiver’s feelings of loneliness: “There was a time when I really felt my mother’s loneliness. Because people ran away due to her behaviour” (Interview 16).
This dynamic, elaborated by the participants and the social worker, emphasizes the further isolation of the caregiver, who not only bears the emotional weight of caregiving but must also confront the loneliness and alienation resulting from the shrinking social network of their loved one.
“You Free the Soul”: Intervention Rebuilds Anxiety-Buffering System and Balanced Self
The findings show that participation in intervention programs strengthens the main components of anxiety-buffering mechanisms and allows the participants to maintain psychological equilibrium while facing regular mortality reminders in their caregiving role.
Strengthening Cultural Worldviews
Respondents share how participation in support programs for family caregivers helps normalize their experiences and emotions. It seems that they begin to feel validated, recognized, and empowered, enabling them to view caregiving as a natural, albeit challenging, part of life: You know you’re not alone. At meetings, you see other people and you learn, you always learn from each other … And we are seen … we are not transparent. (Interview 11)
This statement highlights how by interacting with others facing similar struggles, caregivers are reminded that their feelings are not unique but part of a broader shared experience. The acknowledgment that they are “seen” suggests the emotional validation they receive, which counteracts the common perception of invisibility that often accompanies caregiving.
Another caregiver emphasizes the need to address the cultural silence surrounding caregiving, aging, and mortality. I think it needs to be raised in awareness that aging and death and a sick parent and a family caregiver, think about it, talk about it, there’s no talk. It needs to be publicized, that someone who is aging and it’s okay to age, it’s part of life, not to be frightened of it, not to run away. (Interview 16)
This caregiver recognizes the transformative potential of open dialogue and awareness, both for caregivers and society at large. By normalizing aging as an inevitable part of life, the intervention not only provides emotional support but also equips caregivers to confront their own fears about aging and mortality, fostering a healthier acceptance of these realities that helps to overcome their own mortality anxiety.
Rebuilding Self-Esteem
The program addressed the feelings of anxiety and a lack of control that caregivers experienced when dealing with the new and unfamiliar processes by helping them understand what to expect, what services they might need, and how to navigate those services. The information and skills caregivers acquire through the program alleviate feelings of uncertainty and anxiety, empowering them with a sense of control and peace of mind. It’s very helpful. First, the fact that you know there’s someone behind you. We’re now more aware … before [the intervention] we weren’t aware of all these things regarding older and incapacitated people. The very fact that there is more awareness about the medical, physical, and mental matters [of older adults] … it’s very, very comforting first of all. (Interview 11)
This quote emphasizes how acquiring knowledge reduces the emotional burden of caregiving. Awareness of available resources and a better understanding of the aging process provide caregivers with reassurance, replacing uncertainty with clarity. The intervention creates a safety net, giving participants confidence that they are not navigating these challenges alone. I think I received knowledge and tools that I didn't have before. And I definitely think [that now] I know where to turn in case I need help, which I didn’t know before. Also, when I heard about the Welfare Department, I didn’t think they had [intervention programs for caregivers]. First of all, I was exposed to the program and the options, so yes, I agreed [to participate in the program]. And it helped, and I can also share my knowledge with others. (Interview 9)
This quote highlights the empowering effect of learning about resources and options. Beyond individual benefits, the caregiver’s ability to share this knowledge with others demonstrates how the intervention fosters a ripple effect, strengthening the broader caregiving community. This newfound awareness transforms uncertainty into proactive problem-solving, enhancing caregivers’ confidence and preparedness.
Fostering Close Relationships
Support meetings provide caregivers with opportunities to break free from isolation, establish new social connections, and share experiences that reduce feelings of loneliness. I look forward to the meeting every Tuesday. I think the meetings contribute something, they help me, bring me out of a certain loneliness. You learn there that you are not alone … I’m not saying that a sorrow shared is a sorrow halved, God forbid, but you learn that there is other [people in similar] situations. You can learn from the behavior of others … about how to do things in similar situations. (Interview 16)
The weekly meetings act as a lifeline, offering caregivers a space to connect with others and share their burdens. While caregiving remains challenging, knowing that others face similar struggles helps reduce feelings of isolation. The opportunity to observe and learn from others’ approaches also enhances caregivers’ coping strategies, fostering both emotional and practical growth. There’s an opportunity to go out for an hour…In the first meeting, I saw women who take care of their husbands by themselves. This hour or two meant a lot to them … for an hour or two, you free the soul. You’re in another place, which is very helpful. (Interview 11)
This quote highlights the rejuvenating effect of stepping away from caregiving responsibilities, even briefly. The meetings offer a physical and emotional escape, allowing caregivers to recharge and return to their roles with renewed energy. This “freedom for the soul” underscores the importance of creating moments of respite to prevent caregiver burnout.
Promoting Emotional Balance
The intervention facilitated caregivers’ development of more robust anxiety-buffering systems through the integration of caregiving into their cultural worldview and self-concept. This process involved reconstructing meaning around mortality awareness and strengthening psychological defenses against death anxiety. This is what there is. I won’t throw [my mother] away, I’ll take care of her. Even if I was angry with her yesterday, today I’ll be fine. She won’t change, the change that can happen is only within me. Not in her. I try to change myself, so that it will be easier for me. (Interview 9)
This quote demonstrates how the intervention helped caregivers develop more effective anxiety-buffering mechanisms. Rather than fighting against mortality reminders, the caregiver reconstructs their cultural worldview to incorporate caregiving as a meaningful response to human finitude. This internal transformation represents a strengthening of psychological defenses that helps manage death anxiety through meaning-making. I think that in some ways we did reach acceptance and balance and many other benefits, which we can’t define and are maybe unaware of. This intergenerational connection, this sharing, this responsibility, I think everyone benefits from it. [My mother] … us, the grandchildren, the great-grandchildren … I think it’s something for the short and long term … My children come to grandma with love and joy, and she cooks and prepares really tasty food … everyone’s favorites. And it’s not a burden. It’s fun … Overall, in the beginning, it was more difficult, but I think that at some point we reached a kind of balance and harmony. (Interview 7)
This narrative illustrates how caregivers can develop robust anxiety-buffering systems through what TMT calls symbolic immortality. By situating caregiving within intergenerational connections, the participant creates meaning that transcends individual mortality. The emphasis on family traditions (cooking), shared experiences, and long-term impact suggests the development of cultural continuity beliefs that help manage death anxiety. The transformation from burden to “harmony” indicates successful integration of mortality awareness into a meaningful worldview that provides psychological protection through cultural value systems and relational bonds.
Discussion
This study applied TMT to explore the lived experiences of family caregivers in a supportive intervention program. Findings reveal that caregiving brings mortality into daily consciousness, making death a persistent reality rather than an abstract concept. Prior research indicates that prolonged exposure to death-related experiences heightens death anxiety and reduces coping ability (Quevedo-Blasco et al., 2024; Semenova & Stadtlander, 2016). Our study supports this, showing that caregivers struggle with the tension between intellectually accepting death’s inevitability and emotionally resisting loss. Many participants experienced inner conflict—exhaustion from caregiving alongside the difficulty of letting go—aligning with TMT’s premise that direct confrontation with mortality disrupts psychological equilibrium and activates defense mechanisms (Solomon et al., 1991). Beyond concern for their loved ones, caregivers also face anticipatory death anxiety, internalizing fears about their own aging and future dependency. Witnessing a parent’s or spouse’s decline serves as a mirror for their own mortality, intensifying distress (Hamama-Raz et al., 2023). These psychological struggles contribute to increased anxiety, depression, and emotional distress (Bachner et al., 2011; Ünal & Ordu, 2023; Vrettos et al., 2023).
TMT suggests that cultural worldviews buffer existential anxiety by providing meaning and continuity (Burke et al., 2022). However, our findings indicate that caregiving can disrupt these worldviews, exacerbating distress. A key challenge was the cultural silence surrounding death, which hindered discussions on end-of-life planning—a phenomenon linked to modern society’s limited language for death beyond medical discourse (Bregman, 1999). Caregiving also intersects with cultural expectations of familial duty. While cultural norms may encourage caregiving roles (Xiao et al., 2024), they can also generate stress, guilt, and conflict (Edelstein et al., 2017; Gallego-Alberto et al., 2020). Caregivers navigate conflicting cultural narratives: modern values emphasizing autonomy (Pickard, 2010) and traditional norms framing caregiving as an obligation (Olagundoye & Alugo, 2018). Some mitigate this tension by reframing caregiving as a meaningful role, a perspective shown to reduce stress and enhance resilience (Ng & Indran, 2021).
Self-esteem plays a crucial role in buffering death anxiety, as it allows individuals to perceive themselves as competent, as valued, and in control (Pyszczynski et al., 2021). The empirical literature demonstrates unequivocal relationships between caregiving for older adults and self-esteem. Some studies found that informal caregiving positively correlates with self-esteem and might be linked with reward (Cheng et al., 2022; Jütten et al., 2018) and a sense of self-worth (Hajek & König, 2017). Conversely, feelings of being overwhelmed by care tasks (Pudelewicz et al., 2019) and a lack of reciprocity or appreciation (Reid et al., 2005) might often result in diminished self-esteem, especially in cases of lack of social support and financial strain (Cheng et al., 2022). Our findings align with this research, demonstrating that caregiving undermines self-esteem by diminishing caregivers’ autonomy, placing them in unfamiliar roles, and restricting their personal aspirations. Many participants described a gradual loss of identity, as caregiving duties consumed their time, energy, and emotional resources, sidelining personal and professional goals. The deterioration of self-esteem observed among caregivers represents a critical vulnerability in their anxiety-buffering system according to TMT. As caregivers lose their sense of competence, control, and personal achievement, they simultaneously lose a key psychological defense against mortality awareness.
TMT also suggests that close relationships act as a fundamental buffer against death anxiety, providing individuals with a sense of belonging and continuity (Florian et al., 2002). Social isolation, however, increases mortality anxiety (Cicirelli, 2002). Our findings support previous research indicating that caregiving may lead to negative changes in relationships with older family members, the extended family involved in caregiving, and the broader social circle (friends and neighbors). Caregiving reshapes emotional bonds with their older parents and spouses and involves role reversal with an added sense of loss (Enright et al., 2020; Monin et al., 2019). Findings demonstrate that caregiving increased family tensions in discussions related to end-of-life care and financial matters (Laryionava & Winkler, 2021; Monin et al., 2019) and distribution of responsibilities equally, leading to conflicts between siblings or extended relatives, and emotions of anger, frustration, and exhaustion (Brodaty & Donkin, 2009; Friedemann & Buckwalter, 2014). Conflicts may arise over the distribution of caregiving responsibilities, adding to the tension and impacting the caregiver’s mental health (Kayaalp et al., 2021). In these situations, caregivers may react defensively, potentially distancing themselves from the emotional needs of both the older adult and other family members (Maggio et al., 2024; Nardella et al., 2025) and hindering communication and support within families (Wittenberg et al., 2021). As an older adult’s health declines or their behavior changes, they may become socially isolated, causing the caregiver to feel increasingly alone, that is in line with systematic review findings of higher levels of loneliness among caregivers (Hajek et al., 2021).
Intervention programs can help restore caregivers’ disrupted anxiety-buffering systems by reinforcing cultural worldviews, self-esteem, and social connections—key protective mechanisms in TMT. Group discussions and psychoeducational sessions enabled caregivers to see their role not as an individual burden but as a socially meaningful responsibility. This reframing, supported by research on caregiving as interdependence rather than sacrifice, reduces stress and enhances resilience (Ng & Indran, 2021). Validating caregiving as a vital contribution to family and community strengthens cultural worldviews, providing existential meaning and continuity (Burke et al., 2022).
Findings from a recent study within the framework of TMT suggest that caregivers’ experiences may often involve an initial breakdown of defensive buffers before more adaptive systems can emerge (Taubman-Ben-Ari et al., 2025). Conceptually reframing this within the context of our study, this process may unfold in two phases: first, the collapse of existing anxiety-buffering systems under the stress of caregiving; and second, their reconstruction through intervention. Such reconstruction may involve the development of new coping strategies, reframing of the caregiving role, and strengthened sources of meaning. Over time, these adaptive mechanisms can enhance resilience and improve psychological well-being despite the ongoing challenges of caregiving.
The intervention also helped rebuild self-esteem by equipping caregivers with knowledge, coping strategies, and decision-making skills, fostering a renewed sense of competence and control. This aligns with findings that education and structured guidance enhance self-efficacy, transforming helplessness into mastery (Cheng et al., 2022). From a TMT perspective, self-esteem serves as a psychological shield against death anxiety, enabling caregivers to maintain a positive self-concept despite ongoing exposure to mortality reminders (Pyszczynski et al., 2021; Zhao et al., 2022).
A key benefit of the intervention was fostering social connections. Group meetings provided emotional validation and a shared sense of purpose, reinforcing caregivers’ sense of belonging (Florian et al., 2002). By creating “communities of meaning,” caregivers constructed narratives that redefined their experiences, countering isolation and existential distress. This collective meaning-making process transformed caregiving from a burden into a meaningful contribution, highlighting the social dimension of terror management. Strengthening social bonds, worldview stability, and self-esteem, the intervention helped caregivers develop a more adaptive anxiety-buffering system in the face of mortality reminders.
Conclusions
Our findings reveal a paradox: caregiving increases mortality awareness while simultaneously weakening the psychological resources needed to manage it. However, intervention can restore these defenses by strengthening self-esteem, social bonds, and meaning-making. The application of TMT to caregiver intervention demonstrates how existential frameworks can transform our understanding of caregiver distress and support needs. While conventional caregiver interventions focus primarily on reducing objective burden and teaching practical skills, a TMT-informed approach addresses the deeper psychological processes that maintain well-being in the face of mortality awareness. This dual focus—acknowledging both practical needs and existential concerns—offers a more holistic and integrative model for caregiver support. By explicitly addressing the terror management dimensions of caregiving, interventions can help caregivers develop more robust psychological defenses against death anxiety while simultaneously improving their practical caregiving capabilities. This integrated approach may yield more sustainable improvements in caregiver well-being than interventions focused solely on burden reduction.
This study has several limitations. The sample consisted of caregivers participating in a structured intervention, potentially limiting the generalizability of the findings. Recruitment through WhatsApp groups may have introduced selection bias, as caregivers who were not members of these groups for various reasons were excluded from participation in the study.
Future research should include a more diverse caregiver population, particularly those not enrolled in formal support programs, to capture a wider range of experiences. Additionally, while this study highlights TMT’s relevance to caregiving distress, further research is needed to empirically test TMT’s specific mechanisms within this context.
Despite its limitations, this study advances our understanding of the existential dimensions of caregiver distress and the potential of psychosocial interventions to mitigate these challenges. While prior research has primarily focused on alleviating practical burdens, our findings underscore that existential anxieties—particularly those related to death, identity loss, and meaning—are equally critical in shaping caregivers’ psychological well-being. By applying TMT, we demonstrate that caregiver distress is not solely a response to workload but also a reaction to the profound confrontation with mortality and loss of self. This framing has practical implications: interventions designed with TMT in mind can better equip caregivers to sustain their role over time by reinforcing psychological defenses such as meaning-making, self-worth, and relational belonging. From a policy perspective, integrating existential components into caregiver support frameworks offers a more holistic model of care—one that recognizes and validates the emotional, philosophical, and symbolic dimensions of caregiving. Doing so can enhance not only caregiver resilience but also long-term engagement and reduced attrition from caregiving responsibilities. In this sense, TMT offers more than a theoretical lens—it is a guide for designing interventions and policies that attend to address the core of human vulnerability.
Supplemental Material
Supplemental Material - Balancing the Self: Intervention For Family Caregivers Through the Lens of Terror Management Theory
Supplemental Material for Balancing the Self: Intervention For Family Caregivers Through the Lens of Terror Management Theory by Ksenya Shulyaev, Offer E. Edelstein, Aviad Tur-Sinai, Yaacov G. Bachner, Abby King, and Tova Band-Winterstein in Qualitative Health Research
Footnotes
Ethical Considerations
This study was conducted in accordance with ethical guidelines and was approved by the Ethics Committee of the University of Haifa (Approval No. 018/22). All participants provided informed consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research was funded by JDC Israel.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the sensitive nature of the data collected in this study, including transcripts of in-depth interviews with family caregivers, the data cannot be publicly shared to protect participants’ privacy and confidentiality. Access to anonymized excerpts may be considered upon reasonable request and subject to ethical approval.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.