
Abstract
Care-experienced mothers represent a vulnerable population at the intersection of complex childhood adversity and the challenges of parenthood, making them a crucial focus for research on mental health. The current study aimed to explore how care-experienced women perceive and manage the impact of motherhood on their mental health. Using interpretative phenomenological analysis, we examined how care-experienced mothers interpret and make sense of motherhood and mental health in their specific contexts. Through the analysis of five mothers’ interviews, four superordinate themes were identified: (1) The value and fragile benefits of motherhood; (2) When the past and present collide; (3) The value and power of identities; and (4) Engagement with services: the push and pull. The findings suggest that care-experienced mothers are more vulnerable to distress when their identities are solely tied to motherhood and when they experience power imbalance in support services. This highlights the importance of fostering self-worth beyond the maternal role and the need to provide accessible non-stigmatizing services. It is therefore important for policymakers and health professionals to work in collaboration with care-experienced mothers to establish compassionate, tailored, and ongoing support beyond statutory care. This support will be crucial in helping mothers with care histories maintain better mental health and consequently equip them to develop healthier relationships with their children and themselves.
Introduction
Getting It Right For Every Child (GIRFEC) is a Scottish framework policy that supports and safeguards the well-being of children and young people (Scottish Government, 2022). In conjunction with the policy, the Scottish Government commissioned the Independent Care Review with its findings leading to a commitment to bring change for all care-experienced children and to make sure that every care-experienced child and young person in Scotland is safe, loved, and respected (The Promise, Independent Care Review, 2020). More importantly, the care review also highlighted the need for increasing ongoing support to those moving out of the care system into adult life, with the aim to reduce inequalities in health outcomes across Scotland for care-leavers. Understanding the experiences of care-experienced mothers, particularly with respect to their mental health, has an important role to play in advancing this aim. Care-experienced individuals, especially mothers, face unique challenges rooted in their histories of adversity, family instability, and systemic intervention. These experiences often intersect with critical aspects of their adult lives, including parenthood, mental health, and socio-economic stability. Despite these vulnerabilities, research on care-leavers, particularly women who become mothers, remains limited. This gap in the literature leaves crucial questions unanswered regarding how these women navigate the emotional and psychological demands of motherhood and how their care experiences influence their mental health. The current study seeks to address these gaps, synthesizing existing knowledge on the interplay between care experience, motherhood, and mental health. We employed an interpretative phenomenological analysis (IPA) to explore how care-leaver women perceive and manage the impact of motherhood on their mental health.
Children and young people entering the care system are overwhelmingly removed from their family of origin to ensure their safety, meaning their childhoods are often marred by abuse, neglect, and family difficulties (Barnes et al., 2017). These adverse childhood experiences increase the risk of poorer outcomes across virtually all developmental domains (Hughes et al., 2017). As a result, international research highlights that care-leavers are more likely to experience homelessness (Picker et al., 2024), unemployment (Furey & Evans, 2021), physical health problems (e.g., Batty et al., 2024; Zlotnick et al., 2012), and mental health problems (Seker et al., 2022). They are also more likely to engage in offending behavior (Summerfield, 2011), use alcohol and drugs (Aparicio et al., 2015), and underachieve academically (Rees, 2013). Of particular relevance to this study, care-leavers are also more likely to become young parents (Eastman et al., 2019), and their children are more likely to be placed in out-of-home care with prevalence rates of 8%–19% compared to 1% in the general population (Jäggi et al., 2022). Out-of-home placement (OHP) is also more likely to occur if the care-experienced parent experiences mental health difficulties (Straatmann et al., 2021), and if the mother versus the father is care-experienced (Wall-Wieler et al., 2018).
Research shows that levels of parental involvement between care-experienced mothers and fathers differ markedly (Roberts, 2021). Care-experienced mothers are twice as likely as care-experienced fathers to live with their children (Eastman et al., 2019). They are also twice as likely as their non-experienced peers to parent alone and without help or involvement from the father (Botchway et al., 2014; Radey et al., 2016; Schelbe & Geiger, 2017). In contrast, children of care-experienced fathers are more likely to live with their biological mother, whereas children of care-experienced mothers who are not living with their parents are more likely to be placed in foster or adoptive care (Eastman et al., 2019). The reasons for care-experienced fathers’ lack of involvement are multifaceted, involving structural barriers such as limited access to suitable accommodation and the failure of services to recognize fathers’ contributions. Recent qualitative work also highlights how these fathers may carry deep-seated mistrust toward professionals and fear judgment or child removal, leading to guardedness and reduced help-seeking (Dandy et al., 2020).
While it is important to understand barriers to father involvement, the higher rates for solo parenting among care-experienced mothers (Eastman et al., 2019) place them at the center of caregiving responsibilities, underscoring the need to explore their experiences more closely. Given that there is also a greater risk of intergenerational transmission for OHP among mothers (Wall-Wieler et al., 2018) and that mental health difficulties are also associated with a higher risk of OHP (Straatmann et al., 2021), it is crucial to understand their experience of motherhood, its potential impact on their mental health, and their support needs. Maternal mental health challenges are not only significant for the mothers themselves but also have important implications for their children. Research has shown that maternal mental health difficulties are associated with adverse effects on child development (Kingston & Tough, 2014). Thus, research on maternal mental health also contributes to the broader child health agenda (World Health Organization [WHO], 2021) and is also consistent with the Scottish Government’s GIRFEC policy (Scottish Government, 2022) and their ambition to make Scotland the best place in the world to grow up (The Promise, Independent Care Review, 2020).
For care-experienced women, vulnerability to mental health difficulties in motherhood appears to be heightened. By the very nature of being care-experienced, these mothers are less likely to benefit from family support (Botchway et al., 2014), which, combined with an increased likelihood of single parenthood, may exacerbate feelings of isolation. There is substantial empirical evidence linking social isolation with poorer mental health outcomes (Rohde et al., 2016). Moreover, care-experienced mothers are also likely to face greater economic and social disadvantages during their child’s first year of life compared to their non-care-experienced peers (Botchway et al., 2014), factors that are strongly associated with poorer mental health (e.g., WHO, 2013). For instance, data from the Millennium Cohort Study (MCS) indicate that care-experienced mothers were twice as likely to report symptoms of depression, with over half reporting a formal diagnosis, compared to under a third of their non-care-experienced counterparts. They also reported higher levels of life dissatisfaction and a perceived lack of control over their circumstances (Botchway et al., 2014).
The MCS provides valuable population-level data, but qualitative research is needed to understand the lived experiences of care-experienced mothers in depth, particularly since most existing studies have focused on young mothers who were still in care, became parents while in care, or were transitioning out of care (e.g., Crous et al., 2021; Radey et al., 2016; Schelbe & Geiger, 2017). For example, Aparicio and colleagues (2018) used IPA to examine teenage mothers living in foster care, highlighting the complex emotional transitions and the need for mental health support. More recently, Walsh and colleagues (2023) employed IPA to explore the experiences of mothers who grew up without a mother themselves, finding that mental health struggles were central to their early mothering of children under the age of two. There remains, however, a need to understand how care-experienced mothers more broadly, across different care settings and ages, experience and manage the impact of motherhood on their mental health after leaving care.
The Current Study
The current study aims to explore how care-leaver women perceive and manage the impact of motherhood on their mental health. By focusing exclusively on mothers who have already left care and directly addressing their mental health experiences, this study addresses important gaps in the literature. Existing research on this topic is largely based on population-level data and incidental findings from qualitative studies that explore the broader experience of motherhood among care-experienced women. Furthermore, most qualitative studies have focused on mothers still in care, those transitioning out of care, and teenage mothers. It offers new insights into the unique mental health challenges faced by care-experienced mothers post-care, an area that has received relatively little attention in research. As this study is concerned with the individual lived experiences of care-experienced mothers, and how they create meaning from these experiences and interpret events and people, we selected IPA as the most suitable methodology. This approach allows for an in-depth exploration of the personal and psychological significance of motherhood for care-leaver mothers, centering their voices and ensuring that their perspectives are at the foreground, and thus aligns with the commitment made by the Scottish Government to care-experienced people (The Promise, Independent Care Review, 2020). Ultimately, this study aims to answer the following question: “How do care-experienced mothers perceive and manage the impact of motherhood on their mental health?”
Methods
Design
This qualitative study employed the phenomenological principles of IPA (Smith et al., 2021), utilizing semi-structured interviews to generate in-depth, experiential data. IPA is a phenomenological, hermeneutic, and idiographic approach that examines how people experience a phenomenon and how they make sense of that experience in context (Smith et al., 2021). In this study, we adopt a contextualist position that recognizes that events and circumstances are real for participants, while focusing our analysis on the meanings that individuals ascribe to those events. Experience is therefore treated as subjective and shaped by each person’s historical, cultural, social, and economic context. Meaning-making is interpretative and socially mediated. The task of IPA is to offer a carefully argued account of this sense-making rather than to adjudicate on the objective status of the underlying phenomena.
Phenomenology is concerned with studying and understanding everyday human lived experiences, and it positions participants as the experts of their own personal worlds seeking to establish a common voice between researchers and participants. Idiography in IPA operates at two different levels. First, it requires researchers’ commitment to the particular detail of case-by-case experiences and in-depth analysis of each mother’s account before any cross-case comparison. Second, claims are offered at the level of the specific group/context (i.e., experiences of mental health as a care-leaver mother) rather than at population level. Our analytic sequence followed this idiographic pattern by completing and documenting full individual analyses prior to developing group-level themes. Hermeneutics is concerned with interpretation and involves a “double hermeneutic” process, which requires researchers to attempt to make sense of the participants’ own meaning-making. The principles and underlying assumptions of IPA align well with the current study’s aim of understanding how care-experienced mothers make sense of their lived experiences of motherhood and mental health in the context of their care histories, and it also aligns with the Scottish Government’s Promise (The Promise, Independent Care Review, 2020) of providing a voice to care-experienced people.
Sampling and Recruitment
We used purposive sampling to achieve experiential homogeneity on the core phenomenon, namely, being a care-experienced woman and also a mother. Within this shared experience, we anticipated and accepted variation in age and care history as context that could shed light on nuances in meaning-making. This study reports on data from five care-experienced mothers. Smith and colleagues (2021) suggest that for an IPA study, a sample size of between four and ten is sufficient. The aim is not to achieve saturation of themes but to represent the richness of individual accounts (van Manen et al., 2016). The mothers were recruited via social media and third sector organizations operating in Scotland, namely, through children’s charities Barnardo’s and Aberlour. Invitations for recruitment were also sent to residential childcare homes in Scotland to be possibly distributed to care-leavers.
Participants
To be eligible for inclusion, mothers were required to be “care-experienced” and residing in Scotland. The researcher adopted a broad definition of the term to represent the range of care settings a person may have experienced. National Guidance from the Scottish Government defines this as “anyone who has been or is currently in care or from a looked-after background at any stage in their life, no matter how short, including adopted children who were previously looked after” (Scottish Government, 2021). Eligible participants were mothers who had experienced care, including foster, kinship, or residential care. Kinship care refers to when a child is unable to live with their birth parents and lives instead with a relative or other adult with whom they have a pre-existing relationship. When kinship care is not available, children may also be looked after by an approved foster carer or live with other children in residential childcare provision (Scottish Government, n.d.). Participants were required to be over 18 years old and to have aged out of the care system, with English as their first language. Two of the mothers were between 35 and 40 years old, one mother was between 45 and 50 years old, and two of the mothers were below 30 years of age (one between 20 and 25 and another one between 25 and 30). Three out of the five mothers were from an English background but were currently residing in Scotland. Individuals with a formal diagnosis of moderate to severe intellectual disability or current psychotic illness were excluded due to concerns regarding their ability to participate and to give informed consent. Mothers were also required to have at least one biological child, with their youngest being at least six months old. Four of the five mothers had full custody of their children. One mother had a child in kinship care and two children in temporary respite foster care. However, she had been the primary caregiver for these two youngest children for approximately 5 and 7 years. As such, she was considered able to provide insights broadly consistent with those of the other participants. Consistent with IPA, the sample is homogeneous with respect to the phenomenon under study while retaining natural variability in life course and service contact that is typical of this population.
Procedure
Data Collection
All interviews were conducted remotely, either by telephone or via Microsoft Teams. Interviews with mothers lasted an average of 90 minutes (range: 34:49–124:40 min). All interviews were digitally recorded using an encrypted dictation device or Microsoft Teams. Interviews began with a brief rapport-building chat which was not recorded. Participants were reminded of what the interview would generally entail, their right to terminate or take a break at any time, and consent to record the session, and how data would be used was discussed a final time. Once interviews were concluded, time was provided to reflect on participants’ emotional well-being, and they were reminded of the information sheet provided prior to interviews detailing various avenues of support should it be required. Time was also provided for participants to ask any additional questions about the study, and all were thanked for their contribution. The recordings were transcribed verbatim by the lead researcher, and all identifying information was pseudonymized.
Interview Schedule Development
A semi-structured interview guide was developed in line with IPA guidelines, using open-ended questions to encourage participants to discuss the phenomenon of interest (Smith et al., 2021). As part of this process, an initial interview schedule was piloted with three Experts by Experience. Following discussion and reflection with an Expert by Research, the interview schedule was modified to invite further exploration of participants’ experiences (e.g., broader questions and more prompts). A further two pilot interviews were conducted with the new revised interview schedule. Feedback from participants suggested the revised schedule provided sufficient scope for deep exploration of personal experiences, and for this reason, the latter two pilot interviews were kept as part of the final sample. Examples of questions are: Tell me your story of becoming a mum. Can you describe your mental health to me since you’ve become a mum? Can you tell me about how you manage your mental health?
Ethics
This study received favorable opinion granted by the Ethics Committee at The University of Edinburgh, School of Health in Social Science, Clinical and Health Psychology, on 23 July 2020. The study was carried out in line with the British Psychological Society’s (BPS, 2021) Code for Ethics and Conduct. Given that the study explored sensitive topics in a potentially vulnerable population, relevant ethical risks were considered part of the study’s risk analysis. Participant data were collected, stored, and processed in compliance with the General Data Protection Regulation. Ethical approval to recruit care-experienced participants was also obtained from Barnardo’s Research Ethics Committee on 7 June 2022.
Analysis
The IPA in this study followed the procedure and the six steps outlined in Smith et al. (2021). The analysis was conducted at the individual case level before moving to broader thematic synthesis. Each transcript was first read multiple times to ensure familiarity with the mothers’ narratives. Initial exploratory notes were made, capturing descriptive, linguistic, and conceptual comments. These notes informed the identification of emerging themes, which were subsequently examined for patterns and associations within each mother’s account. Once individual analyses were completed, themes across mothers were compared to identify recurring patterns as well as points of divergence. The process was iterative, with themes refined through ongoing engagement with the data. This led to the development of superordinate themes that captured key aspects of mothers’ experiences, supported by subordinate themes that reflected nuances within these overarching categories. To enhance the credibility of the findings, mothers were invited to review the thematic structure, and one mother provided feedback, confirming that the final themes resonated with her lived experiences.
Reflexivity
Interviews and analysis were carried out by the first author, who engaged in a variety of different reflexive processes (sensu Berger, 2015; Smith et al., 2021). For instance, a bracketing interview was conducted with an experienced IPA researcher prior to participant interviews. This interview revealed several factors with the potential to shape both the researcher’s interpretative lens as well as how participants engaged with the researcher and interview process. The lead author acknowledged her position as a young, white, middle-class female of child-bearing age, and as a Trainee Clinical Psychologist, and that her professional, social, and economic status may have influenced interviews in a unique way, perhaps altering how participants wished to be perceived or how comfortable they felt discussing personal aspects of mental health. The main researcher herself is also the daughter of a care-experienced mother, fell pregnant with her first child during the recruitment and data-collection phase of the study, and is a “professional” with experience of supporting care-experienced mothers. This may have influenced which parts of the interviews the researcher interpreted as being most salient, perhaps because they identified strongly with them (e.g., the challenges of pregnancy). Ongoing use of researcher discussion with the co-authors, ethical considerations in line with the BPS Code of Ethics and Conduct (2021), and a reflective journal were essential components of the research process to ensure researcher influence at all stages of the study was adequately accounted for.
Results
Interviews with the mothers were analyzed, leading to the identification of four superordinate themes: The value and fragile benefits of motherhood; When the past and present collide; The value and power of identities; and Engagement with services: the push and pull. Six subordinate themes also arose within these (see Figure 1 for thematic map). Each theme is illustrated with extracts from at least two participants. Quotes for each theme are presented below. IPA Themes and Sub-Themes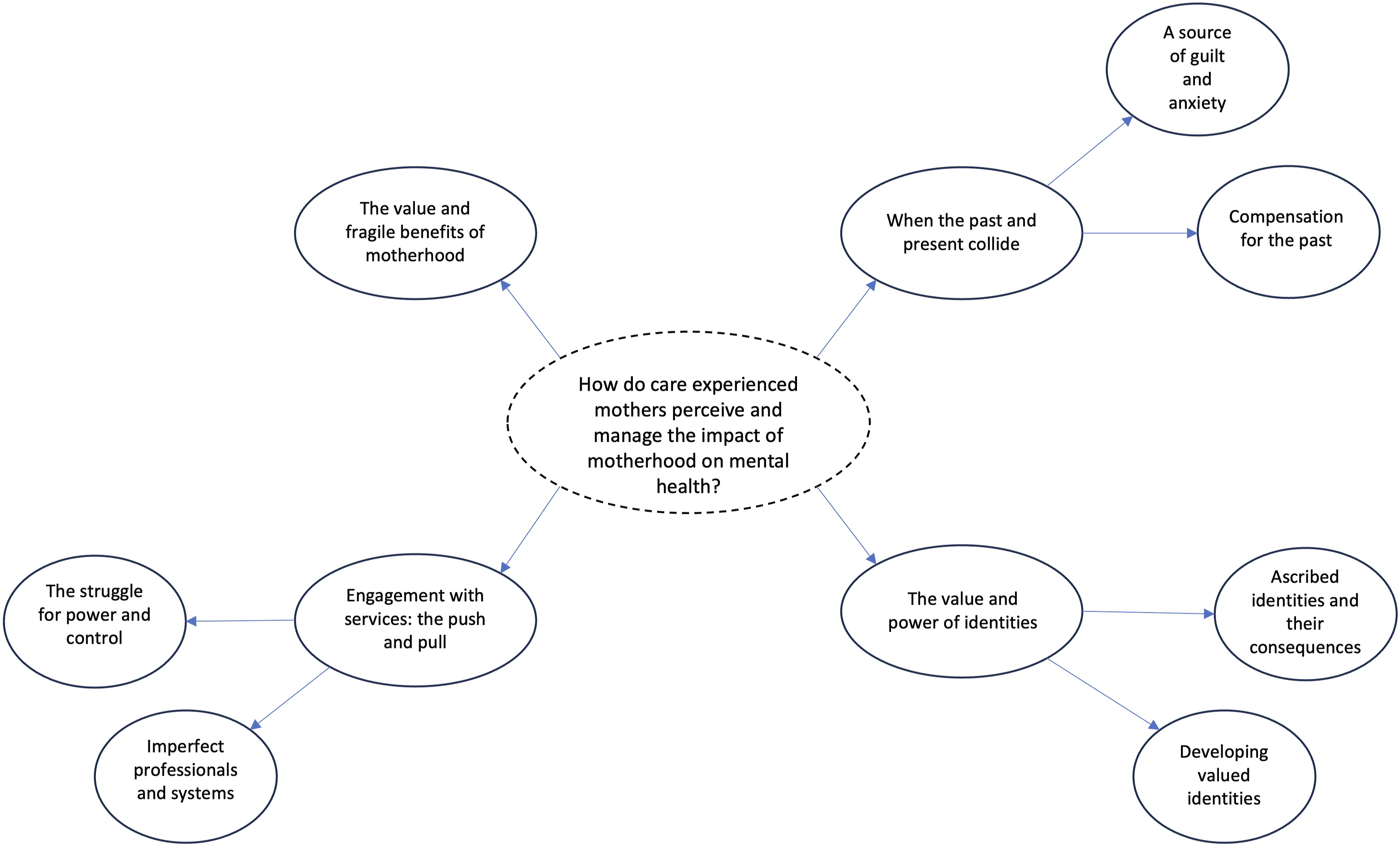
Superordinate Theme: The Value and Fragile Benefits of Motherhood
Mothers highlighted that while motherhood for care-experienced women could be immensely challenging and pose a threat to mental health, it was also perceived as valuable, offering significant rewards. They reported that most pregnancies were unplanned and largely a surprise: “He wasn’t planned. But we wouldn’t change it now, right enough!” (Miranda, 20). Aileen expressed joy at discovering she was pregnant, despite acknowledging the hardship of pregnancy: I was like “oh my gosh!”. And obviously it was like, really joyful and it was nice to know that it could happen. And obviously I wanted to keep him … But, em, it was horrible in some ways because pregnancies are difficult, but it was nice because I got him at the end of it. (Aileen, 15–18)
Motherhood justified significant sacrifices: “I just thought ‘No, I’m keeping this baby’ and basically said to my husband ‘It’s up to you how much you want to be involved’” (Cristina, 17–18). The perception of motherhood as something worth sacrificing for was a significant shift for Cristina who “had such a negative experience of having a mum it was never something that I aspired to be” (Cristina, 231–232). Aileen, similarly, reflected on her unexpected embrace of motherhood, despite initially feeling “totally against” it due to the perceived complexity: “When it happened it was kind of like, oh god. I can’t, this can’t not happen” (Aileen, 26–27). Both women had believed motherhood was impossible due to past health issues and experiences, yet their unexpected pregnancies prompted a re-evaluation of what motherhood could mean for them, as opposed to what it had represented in the past.
The early post-partum period brought new challenges. Cristina described the “enormity of the responsibility” (Cristina, 430–431) as a potential threat to mothers’ mental health, while Aileen reflected on the early days of motherhood as “quite a dark time” (Aileen, 90) suggesting an experience which was perhaps overwhelming or frightening. However, motherhood also offered moments of bonding, as Kerri highlighted: “Breastfeeding … it was a lovely bonding experience” (Kerri, 227). Children soon became a source of pride and joy, helping some mothers protect against mental health challenges or aiding their recovery: She always makes me wee things, like, and is always saying nice wee things to me. I think they really are … they make my day every day. That’s what I get up for in the morning every day. So I don’t know where I’d be without them. That’s what I’ve said, I wouldn’t be here anyway. … That’s what keeps me going in life definitely. (Kayleigh, 589–592)
Kayleigh’s positive interactions with her children seemed to boost her self-esteem, even when her mental health was poor. The pleasure she experienced in the company of her children was the motivation she needed to tolerate it and face each day. However, Kayleigh also implied that her children were her sole motivation, raising concerns about the potential risk to her mental health should this source of motivation wane.
Superordinate Theme: When the Past and Present Collide
This superordinate theme synthesizes mothers’ perceptions on how their childhood experiences shaped their self-perception as parents, their concern about how others might view them, and the difficult emotions this elicited. It also highlights coping strategies employed by the mothers to manage these feelings.
Subtheme: A Source of Guilt and Anxiety
Mothers suggested that motherhood for care-leaver women was often accompanied by guilt and anxiety. These emotions frequently stemmed from their adverse childhood experiences. Mothers expressed concerns about their parenting abilities and worries about how others might perceive them. When they felt they were falling short of either their own or external standards of “good enough” parenting, guilt was identified in participants’ accounts. Aileen reflected: Yeah, I think I was reflecting a little bit about … this week is a great example of like, I’ve come away (on holiday) on my own, which as a mum, all the guilt about … But I think I question my choices like 10 times more because I, I’m like, am I like my birth mum? (Aileen, 584–587)
Aileen’s narrative filled with references to “mother guilt” highlights the internal conflict between attending to her own needs and caring for her son. While guilt seemed a normal part of motherhood, Aileen felt more vulnerable due to fears of repeating her own mother’s abusive behavior. There was a sense that Aileen often coped with these feelings by monitoring herself closely but also recognized the importance of sometimes prioritizing her emotional well-being. To manage their anxieties, some mothers strove to be the “perfect” parents, as Aileen explained: “I try and like do the most fun things with him all the time because I want him to have all these fun, fun experiences” (Aileen, 836–837).
The mothers connected mental health struggles which they associated with their adverse childhood experiences with heightened feelings of guilt and anxiety about their parenting. Kerri shared her concerns about how her own anxiety might have affected her son: And it’s more to do with decision making and you know, that, that, that eh, that eh, that freeze response which happens when you’re sexually abused. … that’s where the anxiety comes from. … I do think I’ve passed some of my anxiety on to [my son], and I have incredible guilt with regards to that. (Kerri, 321–325)
Similarly, Kayleigh feared how her children might one day perceive her due to her mental health struggles and past substance use: “So I don’t want them to look back and think, … my mum’s mental health was bad, and addiction and … I don’t want them ever thinking like that or knowing that stuff” (Kayleigh, 609–612).
Kerri’s hesitation as she expressed her concerns hinted at the emotional difficulty of verbalizing these feelings, suggesting deeper shame. Kayleigh, similarly, worried about her children’s perception of her own mental health and how this may affect them in the future. Both mothers’ narratives illustrate how guilt was closely intertwined with shame, as they feared negative evaluations not only from others but also from themselves. This fear of being judged as inadequate was captured poignantly by another mother’s candid rhetorical question: “Like, do they think I’m a shit mum?” (Aileen, 871).
Subtheme: Compensation for the Past
Motherhood often triggered difficult emotions, particularly anxiety, as many care-experienced mothers worried about being “good enough” parents and about replicating the behaviors of their own abusive caregivers. Mothers reflected on how they attempted to mitigate these feelings by compensating for their negative childhood experiences through their parenting. The experiences of Cristina, Aileen, and Kerri illustrate the range of compensatory parenting behaviors and how the intensity of a mother’s anxiety influenced the extent to which she engaged in these behaviors. Cristina, for example, reflected on how her own childhood experiences influenced her approach to supporting her son through his autism assessment: … with my youngest, with him having his autism assessment that has been a real fight and I’ve had to really advocate for him at school. And I know that a lot of that is borne from my parents not supporting me and not advocating for me when I, you know, had difficulties. … I’m very focussed on making sure that [son’s] views are central. Cause I didn’t have that. (Cristina, 491–496)
Unlike other mothers, Cristina did not express feelings of guilt or anxiety about her parenting. Instead, she seemed to draw strength from her childhood experiences, using them as a source of determination and strength. Her focus was on ensuring that her son had the support she lacked, and her parenting appeared to be informed by her past rather than compensating for it.
In contrast, other mothers found it more difficult to separate their adverse childhood experiences from their parenting. Aileen, for instance, recalled advice from a professional about the dangers of compensatory parenting: I remember someone from the perinatal team saying to me, “Try not to compensate, because you’ll smother him. Because you’re so conscious of not feeling loved, you’ll smother him.” And I was like, “I won’t do that.” And I’m like, “Yeah” I say like, “I love you, [son]. I love you so much. I love you the most ever.” … And he’s like, “Yeah. Shut up, mom.” I’m like, “I love you.” Em, and I do that all the time. But I feel guilty for doing it. Like I’m harming him. (Aileen, 831–835)
Despite being aware of the risks, Aileen felt compelled to engage in compensatory behaviors because of the pain she experienced from feeling unloved as a child. This led to feelings of guilt, as she feared that her attempts to overcompensate may negatively affect her son. Similarly, Kerri was determined that her son would be loved to an extreme degree: “My son would be loved and protected to, to, to the end of my, you know, whatever extreme I had” (Kerri, 401–402). Kerri compared her parenting to her own childhood, noting how different her approach was: “sort of one extreme to the other, isn’t it” (Kerri, 405).
Both Aileen and Kerri feared that their compensatory behaviors, driven by their own distress, may harm their children. Kerri reflected on how her over-protectiveness may have hindered her son’s development: “Maybe I didn’t allow him to develop some of his own abilities” (Kerri, 403–404). She also acknowledged how pervasive guilt was in her life: “Guilt is my, is my, is my, you know, constant companion” (Kerri, 414).
Superordinate Theme: The Value and Power of Identities
Mothers’ accounts revealed identity as a lens through which they made sense of their experiences of motherhood and care experience. Identities were sometimes difficult to define or resist when imposed by others, but they were powerful in shaping access to support, opportunities, and decision-making. These identities played a significant role in how mothers managed their mental health.
Subtheme: Developing Valued Identities
Many mothers in the sample experienced uncertainty about their identity before becoming a mother. Motherhood provided an opportunity to make sense of themselves and their histories, conferring a renewed sense of purpose. Mothers varied in how strongly they identified with being a mother and how they integrated their care experiences into their sense of self. This process of identity formation appeared to have a positive impact on their mental health. Kayleigh articulated how her identity as a mother was still evolving, shaped by her past and current experiences: Like, even now, I feel like I’m still, I’m just learning who I am, if you know what I mean? I’m still, I don’t know. … when I became a mum, … then domestic abuse. And then I couldn’t be who I was for years with him, because I didn’t even know who I was. …. (Kayleigh, 598–602)
For Kayleigh, the formation of her identity had been disrupted by her experiences of abuse both in and following care. Though she identified strongly as a mother, she still felt uncertain about who she was outside of this role. However, she described a growing sense of self-discovery and reflected on how this had improved her coping abilities: “I feel like I’m still just getting to know me. … But, I’ve got a better way of thinking now than I did before. Definitely. I can, I think about things before I do them now” (Kayleigh, 605–607). Kayleigh’s narrative suggested that she developed a clearer sense of her identity and she became better equipped to handle challenges, making more deliberate, reflective decisions.
For other mothers, like Aileen, embracing multiple identities was protective. Aileen frequently worried about being, or being perceived as, a “shit mum” (Aileen, 865). However, having a professional identity alongside her role as a mother helped bolster her self-esteem. Aileen also embraced the identity of being care-experienced, which she had once hidden but now saw as a source of strength: “I went from being a young person who was, like, would hide my care experience to being someone as an adult who utilizes that appropriately” (Aileen, 318).
Aileen’s narrative reflected a broader shift in how care experience was perceived, not just by herself but also in the professional realm of social work. This transformation from shame to pride contributed positively to her self-esteem. Aileen and Cristina, both in professional training at the time of interview, saw their care experiences as providing them with unique insights that benefited their role as both mothers and professionals: Cristina shared how her experience helped her become empathic: “Being in care, it’s a very niche experience to have, but there’s things that it opens your eyes to, can make you, you know, a much more understanding person” (Cristina, 316–318). Both women found value in using their care experience to “give back” to the care-experienced community, aligning with their personal values and further enhancing their sense of self-worth: “That’s a strong value that I have in me, kind of striving for social justice for people” (Cristina, 145–146).
Subtheme: Ascribed Identities and Their Consequences
This theme captures the experiences of labelling, particularly how care-experienced mothers and those with mental health struggles felt that professionals and systems assigned them identities that were silencing and limiting. These labels often ignored the complexity of their individual experiences and shaped the care they received.
Miranda highlighted how her care experience was not equal to that of others, yet she felt labelled in ways that erased these distinctions: I was taken into foster care with my brother and sister. … We were in the same house until we were like, 18. … I had a special [maternity] team that deals with people who have been in care before, but it’s also the same level as like, junkies. … I did feel kinda like, I think, labelled in a way. If that makes any sense? (Miranda, 52–57)
Despite having a relatively stable care experience, Miranda felt that her treatment by maternity services lumped her together with people facing very different challenges. The label “care-experienced” seemed to override other aspects of her identity, including her role as a temporary carer for her sister’s children. Based on Miranda’s account, her midwife dismissed her past caregiving experience, saying, “it’s your own child now, and you know, it’s different” (Miranda, 244). Miranda reflected her regret at not advocating more strongly for herself: “I just feel like I wish that I had said that really, that I knew what I was doing and whatever else” (Miranda, 241). This sense of being reduced to a label was further reinforced in public settings, where she felt “othered,” such as within a mother and baby groups, where she had to explain why she was receiving specialized care: “It wasn’t very nice, you know, having to explain, like, why. Cause it does feel like, that’s coming into like, labels again” (132–133).
The issue of labelling also extended into mental health services. Aileen shared her concerns about diagnostic labels, especially the label “Personality Disorder,” which she narrowly avoided as a teenager: “… 15-year-olds who are in care …. you’re labelling them … we know there’s an aspect there of self-fulfilling prophecy … we’re giving them a life of that, .. We’re not offering them the opportunity to live a life without that label”. (Aileen, 1428–1434). Aileen’s narrative revealed her fear of how labels could permanently shape someone’s identity. The label of personality disorder, in her view, carried a sense of hopelessness that trapped people in their childhood trauma without offering a path to recovery. She criticized how medical professionals sometimes applied such diagnoses to care-experienced teenagers and young mothers which she perceived to suggest a lack of professionalism: “They love to throw personality disorder diagnoses at teenagers and young mums” (Aileen, 1406–1407). Cristina, too, experienced the power of labelling in mental health services, finding that her history of childhood trauma was disregarded in favor of a simplistic diagnosis of post-natal depression: I really didn’t like the fact that doctors were calling it post-natal depression. … that’s very different to being confronted with childhood trauma. … I wasn’t being listened to. … they probably just thought, she’s had a baby, we see this often, you know, symptoms of depression. (Cristina, 72–74, 439–441)
Like Miranda, Cristina felt that her personal history was reduced to a label that failed to capture the complexity of her experiences. Despite seeking help, the inaccurate diagnosis caused her additional distress, leaving her feeling silenced and misunderstood.
Superordinate Theme: Engagement With Services: The Push and Pull
This superordinate theme reflects the complex dynamics between mothers and the professional services they engaged with. Mothers described power imbalances, with professionals often holding control over decisions affecting the mothers’ lives. These dynamics sometimes replicated the mothers’ earlier experiences of feeling powerless, creating further distress. The interactions between mothers and services, compounded by systemic shortcomings, impacted mothers’ mental health and their willingness to engage with services. Mothers highlighted examples of health and social care systems failing to meet mothers’ needs, often due to these imbalances.
Subtheme: The Struggle for Power and Control
This subtheme captures how mothers perceived the balance of power as weighted toward professionals, often leaving mothers feeling controlled and silenced. For many mothers, this experience of being overpowered was distressing, as it mirrored feelings from their childhood. Power dynamics also influenced the type and quality of care mothers received. Miranda’s account highlighted how she felt she had to negotiate her care preferences with professionals: … I did like, voice that to them, that I would prefer that [talking therapy]. I agreed to take the medication as long as, like, I was referred to that. But then I ended up taking the medication … it just made me feel a wee bit numb. … But I still heard nothing as I say. Now he’s two [laughs]. So, it’s quite bad to be honest. That’s a year and nine months. (Miranda, 320–324)
Despite clearly articulating her preference for talking therapy, Miranda felt that accessing this care required bargaining. The power seemed to rest with the professionals, and ultimately, her preference was not honored. For Kerri, the feeling of being overpowered dissuaded her from seeking help, as she avoided engaging with services for fear of losing control: “I don’t think I actually went to one of the clinics until he was, maybe not a year, maybe 8 months/9 months old” (Kerri, 836–838).
While some mothers like Miranda appeared more willing to accept the power dynamics imposed by services, others like Cristina challenged them. Cristina described how, during her second pregnancy, she became more assertive, disclosing her care-leaver status despite her concerns about how it might be used against her: … I made a mental note not to speak about my care experience. … The second time round when … I was feeling comfortable in who I was, I remember sitting there like waiting for the question and then very confidently, like, looking at her and going “yeah, I was [in care]. And you know, what you gonna do? Are you gonna refer me? Are you gonna judge me?” (Cristina, 116–121)
Cristina’s willingness to challenge authority developed through her counselling, where she learned to “hold [her] power” (Cristina, 257). However, even with this new confidence, Cristina recognized the risks associated with asserting control. She carefully weighed when and how to challenge professionals, dependent on whether she felt safe in doing so: “I think if I felt safe, I would think of how to word it and speak out” (Cristina, 418).
Mothers employed various strategies to retain some sense of control, ranging from complete disengagement to selective involvement. Kayleigh, for instance, retreated from any contact: “I wasn’t talking to anybody. I was just living in this wee cave” (Kayleigh, 479). Kerri, on the other hand, chose to limit her engagement by opting for a home birth: “I wanted to have a home birth because I didn’t want, you know, it was that whole lack of control” (Kerri, 801–802). Others, like Aileen, confronted the power imbalance directly: “And yeah, I put a complaint in” (Aileen, 440).
Subtheme: Imperfect Professionals and Systems
This subtheme highlights how mothers perceived failures in the systems and individuals meant to support care-experienced mothers. These failures, whether due to professional incompetence, lack of understanding, or systemic inflexibility, were perceived to be significant barriers to meeting mothers’ parenting and mental health needs. Kayleigh shared her frustrations with an unreliable social worker, who, according to her, failed to fulfil basic responsibilities: … everybody had complained. It wasn’t just me. Like, she wasn’t getting in touch with people and she wasn’t arranging meetings, and ignoring phone calls and like, making up like lies as well. And I’d, em, just had enough. So now I’ve got an amazing social worker. She’s lovely. She’s so nice, so things are on the right track now. (Kayleigh, 624–627)
For Kayleigh, the ineffectiveness of her previous social worker had caused frustration. Her needing to emphasize that “it wasn’t just [her]” suggests that she felt her concerns would not be taken seriously on their own, highlighting how care-experienced mothers may feel disempowered within the system. Her positive shift in well-being following the appointment of a new, competent social worker further highlights how fragile her mental health was, heavily dependent on the quality of professional support.
Similarly, Aileen described an encounter with a mental health worker, whose approach she perceived as unprofessional: He was like, “You, you were in care weren’t you? So like, ah, you know we maybe need to think of a safeguarding referral for this child” and I was like you wouldn’t do, you wouldn’t do a safeguarding referral for a prebirth just because I’ve been in care. That’s not appropriate (…) And he was like, why not? And I’m like, why? I’m a service user. Why am I telling you this? (Aileen, 375–386)
Aileen’s account reveals her frustration with professionals making assumptions about her parenting based solely on her care experience. She noted how this mental health professional overstepped his boundaries, which she found both offensive and odd, calling him a “weirdo.” This remark captures her incredulity at being subjected to a safeguarding referral for reasons she felt unjustified. Her emphasis on understanding her rights reflects the survival strategies Aileen has developed, drawing on her childhood experiences of navigating a non-ideal systems: “I’ve always took pride and like knowing the law and stuff and my, my rights around stuff because when I was a kid I felt like I had no rights” (Aileen, 397–398).
Discussion
This study explored how care-leaver mothers experience and manage the impact of motherhood on their mental health, providing a much-needed platform for their voices to be heard. Care-experienced mothers often navigate motherhood against a backdrop of childhood adversity, systemic involvement, and societal stigma. In line with the Scottish Government’s Promise (Independent Care Review, 2020) to bring change to all care-experienced people by listening and focusing on their experiences, this study sheds light on the complex emotional landscape of motherhood for care-leavers, including challenges, strengths, and strategies they employ to protect both their mental health and their children’s well-being. Through our interpretative engagement with the accounts of five participants, we developed four superordinate themes: The value and benefits of motherhood; When the past and present collide; The value and power of identities; and Engagement with services: the push and pull. These themes reveal how motherhood can be both a profound source of fulfilment and trigger for distress linked to past experiences, highlighting the need for more tailored and compassionate support for care-experienced mothers.
In relation to “The value and benefits of motherhood,” the findings suggest that while motherhood posed significant challenges to mental health, it was also perceived as valuable and rewarding. These findings align with previous research that shows motherhood, for women in the general population, can be marked by disruption, emotional and physical exhaustion, and oscillation between happiness and loneliness (Miller, 2007). In the context of care-leavers, motherhood has been similarly framed as a source of joy, love, and connectedness, providing a sense of future orientation and motivation to improve lifestyle choices (Aparicio et al., 2015; Bermea et al., 2019). While concerns about “cycles of care” repeating are commonly reported in the literature (Haight et al., 2009), the current study suggests that for some mothers, the experience of motherhood can instead be stabilizing and a positive turning.
Under the theme “When the past and present collide: Motherhood as a source of guilt and anxiety,” mothers frequently expressed anxiety regarding their ability to parent and fears of negative judgment by others. The concern about having children removed from their care or of replicating their own abusive/neglectful childhood experiences is well documented (Haight et al., 2009; Maxwell et al., 2011; Pryce & Samuels, 2010). The sense of “maternal guilt” interpreted in these narratives reflects wider research findings, where guilt is understood as a common, almost inevitable, feature of motherhood, shaped by societal expectations and cultural ideals of the “intensive mother” (Hays, 1996; Williamson et al., 2023). The pressure to meet the ideal of the “ever giving” and “self-sacrificing” mother (Bassin et al., 1994, p. 2) may exacerbate feelings of inadequacy, particularly when mothers lack positive parenting role models, as was evident among many participants in this study. This aligns with findings from Walsh et al. (2023), who highlighted how mothers who grew up without meaningful maternal relationships described heightened anxiety about acknowledging normal ambivalent feelings in motherhood, fear of repeating harmful patterns, and the struggle to develop a “good enough” mothering identity without clear models to follow.
Many mothers in the current study seemed to experience guilt when they perceived themselves to fall short of this intensive mothering ideal, contributing to heightened anxiety and, in some cases, perfectionism tendencies. These findings are consistent with research demonstrating that striving for perfect parenting can increase maternal guilt and stress (Henderson et al., 2016; Rotkirch & Janhunen, 2010). However, while guilt is often associated with specific behaviors, some mothers in this study found it difficult to express these feelings and instead related them to their self-worth, indicative of shame rather than guilt. The distinction between guilt and shame is significant, as shame tends to promote avoidance and withdrawal, while guilt may lead to reparative actions (Smith et al., 2002). This is particularly important given research suggesting that maternal shame can be a barrier to seeking help for mental health difficulties (Dunford & Granger, 2017). Support interventions promoting self-compassion, such as mindfulness-based therapies, have shown promise in mitigating shame and post-natal depression (Perez-Blasco et al., 2013), and these may also be helpful for care-experienced mothers.
Compensatory parenting, captured under the theme “When the past and present collide: Compensating for the past,” was a strategy several mothers used to manage difficult emotions. While compensatory parenting has been noted in other studies on care-experienced and incarcerated mothers (Pryce & Samuels, 2010), it has rarely been explored in depth. In this study, compensatory behaviors ranged from over-protectiveness to over-permissiveness, driven by fears of being rejected by their children or repeating the past patterns of their upbringing. Some mothers struggled with setting boundaries, which may stem from associating authority and limit-setting with the abuse they experienced as children (Greene et al., 2020). The fear of repeating cycles of care likely intensified this overcompensation, with some mothers striving to be the “perfect” parent as a way to avoid past mistakes. Interventions like Mellow Bumps, which help mothers reflect on how their past experiences influence their parenting, may offer a useful framework for addressing these patterns (Breustedt & Puckering, 2013). Such fears of repeating past patterns were also highlighted by Walsh et al. (2023), where the mothers described anxiety about replicating their own mothers’ behaviors and strong desire to “break the cycle” of harmful parenting.
Identity was a recurring concept in the mothers’ narratives, as highlighted in the theme “Developing valued identities.” The acquisition of the identity of “mother” provided many women with a sense of purpose and a way to understand themselves. This mirrors findings from other research showing that motherhood can help care-leaver women cast off unwanted identities and assume a socially valued role (Luyten et al., 2017; Pryce & Samuels, 2010). However, the current study also found that tying self-worth exclusively to motherhood could leave women vulnerable when faced with parenting challenges. Supporting care-experienced mothers to cultivate a broader sense of identity beyond motherhood may therefore be important in fostering well-being. For two mothers in the study, who were in professional training, their care experiences were reframed as a valuable asset, both in their personal and professional lives. As research has suggested, roles that position care-leavers as experts by experience or role models can foster positive identity development (Luyten et al., 2017).
In the subtheme “Ascribed identities and their consequences,” mothers reflected on the impact of being labelled in healthcare settings, where care-experienced mothers often felt stigmatized and misunderstood. Misdiagnosis of mental health difficulties was particularly distressing, as it felt dismissive of mothers’ complex histories. This finding aligns with research suggesting that misdiagnosis can lead to increased distress and potentially inaccurate treatment (Perkins et al., 2018). Mothers in the current study stressed the importance of being seen as individuals rather than being reduced to their care histories. More concerning was that their mental health struggles were often misdiagnosed, overlooking the deeper impact of their earlier experiences and the ways these continued to shape their well-being.
Finally, the theme “Engagement with services: the push and pull” captured the complex dynamics between mothers and support services. Many mothers described feeling scrutinized or judged, echoing their earlier experiences of being monitored and controlled within the care system. This sense of power imbalance made it difficult for some to trust professionals, leading to reluctance to seek support. Some mothers expressed frustration at being treated as inherently “high risk” due to their care histories rather than being seen as individuals with strengths and capabilities. This sense of being pre-judged seemed to reflect earlier experiences of surveillance and control within the care system, contributing to mistrust and avoidance.
To interpret these dynamics, recent child-protection literature has highlighted how such interactions can disrupt relational safety and emotional engagement. For example, Sleed and colleagues (2024) describe how the high-pressure nature of child-protection contexts may undermine parents’ capacity to mentalize, that is, to reflect on and respond to their child’s internal states. In such contexts, parents can struggle to stay reflective, particularly when interactions with professionals feel threatening or emotionally overwhelming. Although not their focus, these findings resonate with broader research suggesting that heightened emotional arousal, including stress and anxiety, can disrupt reflective functioning (e.g., Luyten et al., 2020). Saar-Heiman (2023) further draws attention to how the use of power by professionals can either foster or erode trust depending on whether it is experienced as “power with” or “power over” parents. Together, these insights suggest that supporting meaningful engagement may require not only accessible and non-stigmatizing services but also relational approaches that foster psychological safety and affirm mothers’ experiences.
These dynamics may also help explain why some mothers in our study voiced concerns about being misjudged or having their children removed, and consequently led some to withhold information about their struggles, further distancing them from available support. While services increasingly adopt approaches, such as trauma-informed practice, aimed at being sensitive to adversity, mothers in this study suggested these were not always applied meaningfully. For older care-leaver mothers who are no longer eligible for statutory support beyond age 25, significant gaps remain (MacAlister, 2022). Ensuring that services are accessible, not-stigmatizing, and informed by care-experienced mothers’ lived realities may help foster trust and engagement.
These risks may be part of a broader pattern as recent UK research has highlighted how repeated child removals often stem from intersecting challenges such as abuse, mental health difficulties, and substance use (Russell et al., 2022). These removals, in turn, can compound distress and instability, making it even harder for parents to access or benefit from support (Broadhurst & Mason, 2020; Devaney et al., 2024). While our study did not focus on this group, some mothers’ fears of removal and being labelled “high risk” parallel patterns seen in these contexts. These findings underscore the importance of relational, non-stigmatizing services that recognize and respond to cumulative adversity.
The current study, while offering significant insights, is not without limitations. In line with the Scottish National Guidance (Scottish Government, 2021), this study adopted a broad definition of the term “care experience.” A key aim in IPA is experiential homogeneity rather than demographic uniformity. Our sample was homogeneous regarding the focal phenomenon of being a care-experienced mother living post-care in Scotland. However, there was variation in age and care histories, which we treated as contextual features that shaped meaning-making. Future work could take a more narrowly focused approach, for example, by recruiting mothers from a single care setting or age band, to explore whether specific contexts shape experiences differently, particularly as there is a dearth of research in this area. Another limitation was that there was potential for volunteer bias, which may have restricted the range of perspectives captured. While for the purpose of this study, the focus was intentionally placed on mothers to ensure their voices are prioritized and their unique experiences explored in depth, the exclusion of fathers highlights a research gap. Future research could build on this study by considering the perspectives of fathers, as well as older care-leavers.
Despite these limitations, the study provides valuable contributions to understanding the experiences of motherhood and mental health challenges faced by care-leaver mothers. By centering the voices of care-leaver mothers, this study provides a nuanced and in-depth exploration of their lived realities, offering practical implications for policy and practice.
Conclusion
This study demonstrates that care-leaver mothers perceive motherhood as both deeply meaningful and very challenging, with the role often serving as a source of purpose while also triggering feelings of guilt, shame, anxiety, and self-doubt. The coping strategies mothers in this study employed, including compensatory parenting, were influenced by both personal histories and interactions with services. The findings suggest that care-leaver mothers are particularly vulnerable to distress when their identity is solely tied to motherhood and when they experience power imbalance in support services. This highlights the importance of fostering both self-worth beyond the maternal role and trust in accessible, non-stigmatizing services.
The study underscores the need for tailored, ongoing support that extends beyond statutory care, especially for older care-leaver mothers who may fall outside eligibility criteria. Ensuring that interventions are informed by the lived experiences of care-leaver mothers is crucial to bridging the gaps in service provision. Approaches that promote self-compassion, such as mindfulness-based interventions, may help mitigate feelings of shame and perfectionism, supporting mothers in developing healthier relationships with both their children and themselves.
Finally, routine collection of data on care-leaver mothers, co-produced with those who have lived experiences, would be a valuable step toward shaping policies and practices that directly affect them. By amplifying their voices, challenging stigma, and improving access to mental health and parenting support, future efforts can contribute to a more equitable landscape in which care-leaver mothers feel seen, heard, and supported.
Footnotes
Acknowledgements
We extend our gratitude to the care-experienced mothers and their support workers who generously shared their time, perspectives, and experiences. Your invaluable insights have been instrumental in conducting this study, and this work would not have been possible without your courage and openness.
Ethical Considerations
Our study was approved by the Clinical Psychology, School of Health in Social Sciences Research Ethics Committee at the University of Edinburgh (approval no. CLIN789).
Consent to Participate
All participants provided written informed consent prior to enrolment in the study.
Author Contributions
Brodie McGougan: data collection, initial data analyses, and write up. Monja Knoll: secondary data analyses and oversight of methodology, feedback, and editing. Ingrid Obsuth: supervision of all aspects of the project, conceptualization, writing, and re-drafting of drafts.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.